Article Text

Abstract
Introduction Interscalene brachial plexus blocks are a commonly performed procedure to reduce pain following total shoulder arthroplasty. Liposomal bupivacaine has been purported to prolong the duration of brachial plexus blocks for up to 72 hours; however, there has been controversy surrounding the analgesic benefits of this drug. Our hypothesis was that an interscalene block performed with bupivacaine alone would be non-inferior to a combination of liposomal bupivacaine and bupivacaine with respect to opioid consumption following total shoulder arthroplasty.
Methods Subjects presenting for primary total shoulder arthroplasty were randomized in a 1:1 ratio to an ultrasound-guided, single-injection interscalene block with either a combination of liposomal bupivacaine and bupivacaine (LB group) or bupivacaine without additive (Bupi group). The primary outcome of this study was 72-hour postoperative cumulative opioid consumption (in oral morphine equivalents) with a non-inferiority margin of 22.5 mg. Secondary outcomes included pain scores, patient satisfaction with analgesia and patient reported duration of sensory block.
Results Seventy-six subjects, 38 from the Bupi group and 38 from the LB group, completed the study. Analysis of the primary outcome showed a 72-hour cumulative geometric mean oral morphine equivalent consumption difference of 11.9 mg (95% CI −6.9 to 30.8) between groups (calculated on the log scale). This difference constitutes approximately 1.5 tablets of oxycodone over 3 days. No secondary outcomes showed meaningful differences between groups.
Discussion Interscalene brachial plexus blocks performed with bupivacaine alone did not demonstrate non-inferiority compared to a mixture of liposomal bupivacaine plus bupivacaine with regards to 72-hour cumulative opioid consumption following total shoulder arthroplasty. However, the difference between groups did not appear to be clinically meaningful.
- Ultrasonography
- Acute Pain
- Brachial Plexus
Data availability statement
Data are available upon reasonable request.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Extending the duration of a single-injection peripheral nerve blocks may improve analgesia and reduce postoperative opioid consumption following total shoulder arthroplasty.
WHAT THIS STUDY ADDS
Interscalene brachial plexus blocks performed with bupivacaine alone did not demonstrate non-inferiority compared to liposomal bupivacaine plus bupivacaine with respect to 72-hour postoperative opioid consumption following total shoulder arthroplasty.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Despite a prolonged block duration, an interscalene brachial plexus block performed with liposomal bupivacaine plus bupivacaine did not appear to improve postoperative analgesia in a clinically meaningful fashion when compared with bupivacaine alone following total shoulder arthroplasty.
Introduction
Total shoulder arthroplasty can be associated with severe pain in the perioperative period.1 The interscalene brachial plexus block is a commonly performed technique to improve postoperative pain and reduce opioid consumption following this surgery. However, the duration of analgesia for this procedure following single injection technique is limited,2 3 even when adjuvants are added to the local anesthetic.4 Continuous brachial plexus blocks have been successfully used to prolong effective analgesia,5 but require specialized expertise and are resource intensive.6
In 2018, the FDA approved liposomal bupivacaine (LB) for use in interscalene brachial plexus blocks for postoperative analgesia following shoulder surgery. LB is an encapsulated formulation of bupivacaine designed to slowly release local anesthetic over 72 hours.7 While there are numerous studies demonstrating the benefits of LB in shoulder surgery,8 9 many of them are sponsored by the manufacturer of the drug. Conversely, much of the contemporary and independent analysis of LB has brought into question the clinical value of this drug.10–12 Given the subsequent controversial nature of LB use in brachial plexus blocks, it remains unclear if an admixture of LB with bupivacaine provides benefit over standard bupivacaine with regard to reducing opioid usage following total shoulder arthroplasty.
The objective of this study was to evaluate the addition of LB to bupivacaine in interscalene brachial plexus blocks for patients undergoing total shoulder arthroplasty. The primary outcome was defined a priori as 72-hour postoperative cumulative opioid consumption. Secondary outcomes included: block-related adverse events, verbal Numeric Rating Scale (NRS) pain scores, unanticipated inpatient admissions following surgery, patient-reported duration of sensory block, patient satisfaction with postoperative analgesia, and frequency of persistent opioid use at 1 week from day of surgery. We hypothesized that interscalene brachial plexus blocks performed with bupivacaine alone would be non-inferior to those performed with a combination of LB plus bupivacaine.
Methods
Study design
This randomized trial was prospectively registered at clinicaltrials.gov (NCT04974385) by DAE (principal investigator) on July 3, 2021 (https://clinicaltrials.gov/ct2/show/NCT04974385). The study was conducted at the University of Virginia Health System, Charlottesville, Virginia from August 4, 2021 to April 27, 2022. Adult subjects (≥18 years old) scheduled for primary total shoulder arthroplasty, including anatomic total shoulder or reverse shoulder replacement, were screened and approached for inclusion. Patients with a history of chronic opioid use, pregnancy, pre-existing lung disease, allergies to local anesthetics, pre-existing neuropathy of the surgical limb, or patient refusal were excluded from participation. Written informed consent was obtained from all enrolled subjects.
Using a 1:1 ratio with a computer-generated simple randomization obscured in sealed envelopes, each subject was randomized to receive an ultrasound-guided, single-injection interscalene block with either: a combination of LB plus bupivacaine (LB group) or bupivacaine without additive (Bupi group).
Perioperative management
In the absence of contraindication, all subjects received a preoperative oral analgesic regimen consisting of acetaminophen (975 mg) and celecoxib (200 mg). Peripheral nerve block placement occurred in the preoperative holding area, as is institutional practice, prior to proceeding to the operating room (OR). Once in the OR, general anesthesia was induced with propofol (1–2 mg/kg) and tracheal intubation was facilitated with 0.6 mg/kg rocuronium at the treating anesthesia team’s discretion. Intraoperatively, all subjects received 8 mg of intravenous dexamethasone and 0.5 mg/kg of intravenous ketamine. No intraoperative opioids were administered.
Block placement
Following verification of informed consent, subjects were offered procedural sedation of up to 2 mg of intravenous midazolam for the nerve block procedure. They were then placed in a semirecumbent position, with the brachial plexus identified using a high-frequency linear array transducer (Sonosite, Bothell, Washington) in the supraclavicular fossa, where the subclavian artery is visible in short axis. The transducer was then moved in a cephalad direction until the upper trunk could be identified in a stacked trifascicular pattern between the anterior and middle scalene muscles.13 The skin was cleaned with chlorhexidine gluconate and 1–2 mL of 1% lidocaine was used to anesthetize the skin. A 22-gauge echogenic needle was then advanced through the middle scalene muscle until it was within the subepimyseal compartment. Subjects randomized to the LB group then received an injection of 10 mL of 0.5% bupivacaine with 10 mL of 133 mg LB, for a total volume of 20 mL.
Alternatively, subjects randomized to the Bupi group were similarly positioned and the same procedural sedation offered. Following a similar protocol for localization of the brachial plexus, a 22-gauge echogenic needle was used to inject 20 mL of 0.5% bupivacaine without additive.
Recordings and measurements
Data collection was performed by personnel blinded to the block procedure type. Subjects were evaluated in the post anesthesia care unit (PACU) pending their discharge, and then via telephone evaluation at home. All study patients remained blinded for the duration of evaluation and wore identical identifying arm bands stating they received LB as a safety precaution to prevent further administration of local anesthetic.
PACU assessment, opioid consumption and pain
Upon arrival to the PACU, both intravenous and oral opioids were made available to all subjects at the discretion of the attending anesthesiologist. Time to PACU discharge readiness was recorded by nursing staff and retrieved from the EMR by study personnel. Subjects were instructed to take standardized oral postoperative multimodal analgesics with alternating doses of oral acetaminophen 650 mg and ketorolac 10 mg every 3 hours. Prescription of outpatient opioids consisted of oxycodone 5–10 mg every 4 hours, as needed for discomfort not relieved by the combination of acetaminophen and ketorolac. All opioid consumption in the PACU, at 24 hours, 48 hours and 72 hours postoperatively was recorded and converted to oral morphine equivalents (MME) for statistical analysis.14 The primary outcome was defined as 72-hour postoperative cumulative opioid consumption. Verbal NRS pain scores at rest, with activity, and worst were also recorded by investigators as reported by the subject. Subjects were asked to rate their pain from 0 to 10; with 0 representing ‘no pain’ and 10 representing the ‘worst pain imaginable’.
Block-related adverse events, duration of sensory block and patient satisfaction with analgesia
As part of the postoperative assessments in PACU, 24 hours, 48 hours, 72 hours and 1 week postoperatively, subjects were asked to report any block-related adverse effects, which included: symptoms of local anesthetic systemic toxicity, injection site inflammation, shortness of breath and persistent sensory or motor block>72 hours in the blocked extremity. Subjects were asked to give a verbal assessment representative of the quality of analgesia at these time intervals. Response to these assessments were recorded dichotomously as ‘satisfied’ or ‘unsatisfied’. Subjects were also asked to note the time they perceived the return of sensation to their surgical extremity as a surrogate for block duration.
Unanticipated admissions
As part of the 24-hour, 48-hour, 72-hour and 1-week postoperative assessments, electronic medical records were reviewed for any new hospital admission encounters. Patients were also asked during each assessment period if they needed to return to a hospital for any reason. Any new hospital admissions following surgical discharge were recorded.
Statistical analysis
The sample size was calculated assuming a mean 72-hour MME utilization rate of 45.6 mg with an SD of 37.6 mg based on prior studies.15 Our non-inferiority margin, 22.5 mg, was chosen in an attempt to ensure a clinically relevant difference.16 17 A smaller non-inferiority margin would have limited clinical consequence over a 72-hour timeframe. To have a significance level of 0.05 and a power of 0.8, 35 subjects were required in each arm. Additional subjects per group (for a total of 80 subjects) were recruited to prevent loss of power due to early withdrawal or protocol violations.
Categorical variables were compared using the χ2 test or Fisher’s exact test as appropriate. Evidence of departure from a normal distribution was detected for continuous variables presented in this analysis18; thus, all continuous variables were analyzed as geometric means using the natural log transformation.16 The delta method19 was used to calculate the variance of functions of parameters from the variance/covariance matrix, was used to calculate 95% CIs and p values for the difference in geometric means. The difference in medians and the 95% CI was calculated using a bootstrap algorithm with 10 000 replications.20 SAS V.9.4 was used for analysis. The non-inferiority test for the primary endpoint was tested using a one-sided threshold of 0.025 as the criterion for significance. Two-sided p values<0.05 were considered statistically important; however, no adjustments were made for multiple testing and thus these values should be considered descriptive.
Results
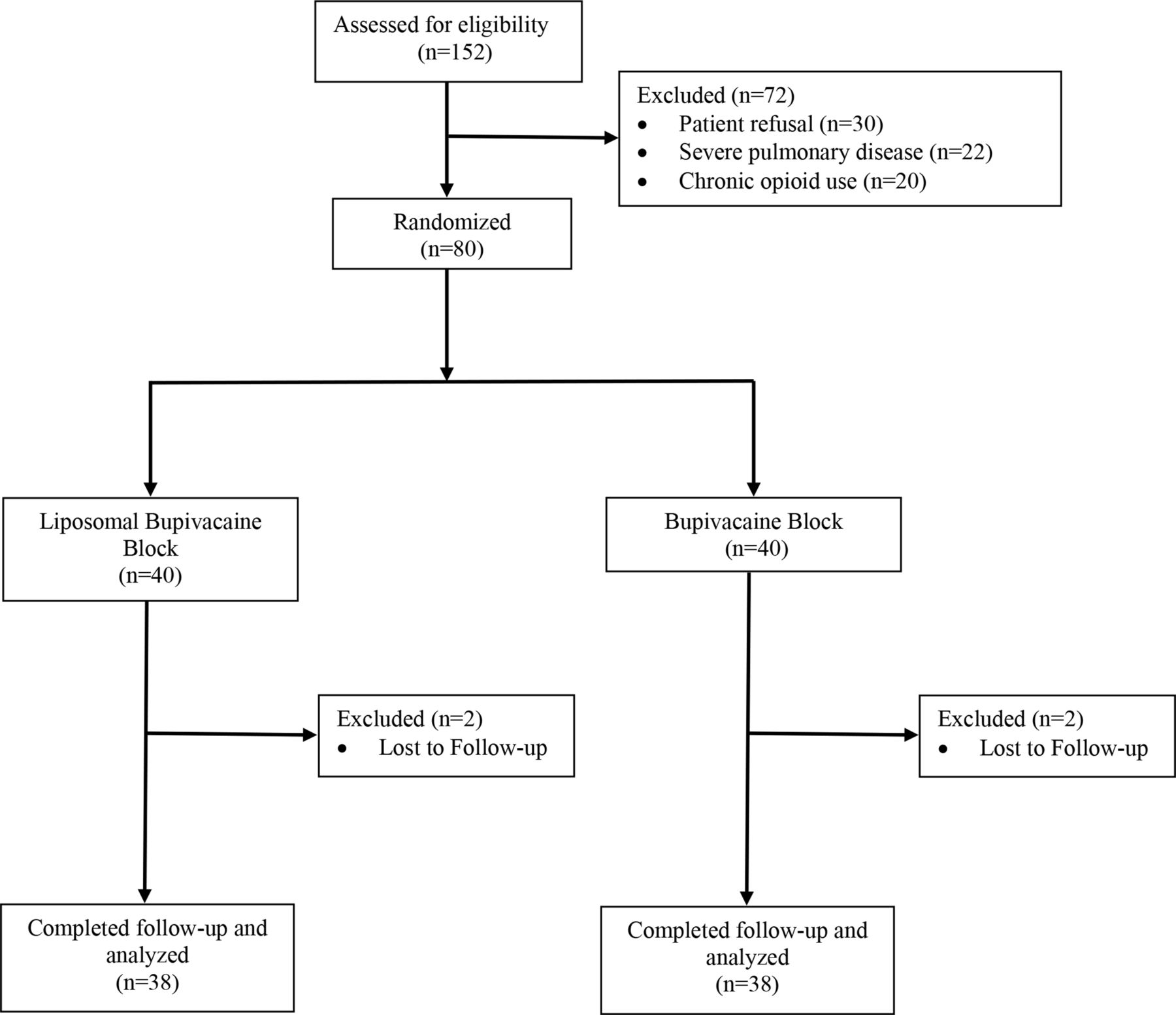
Eighty subjects provided written informed consent to participate in this study. Seventy-six completed the study, thirty-eight from both the LB and Bupi groups. Four subjects were excluded from primary analysis due to missing primary outcome data, two from both the LB and Bupi groups (figure 1). Demographic data and perioperative characteristics were similar between groups (table 1).
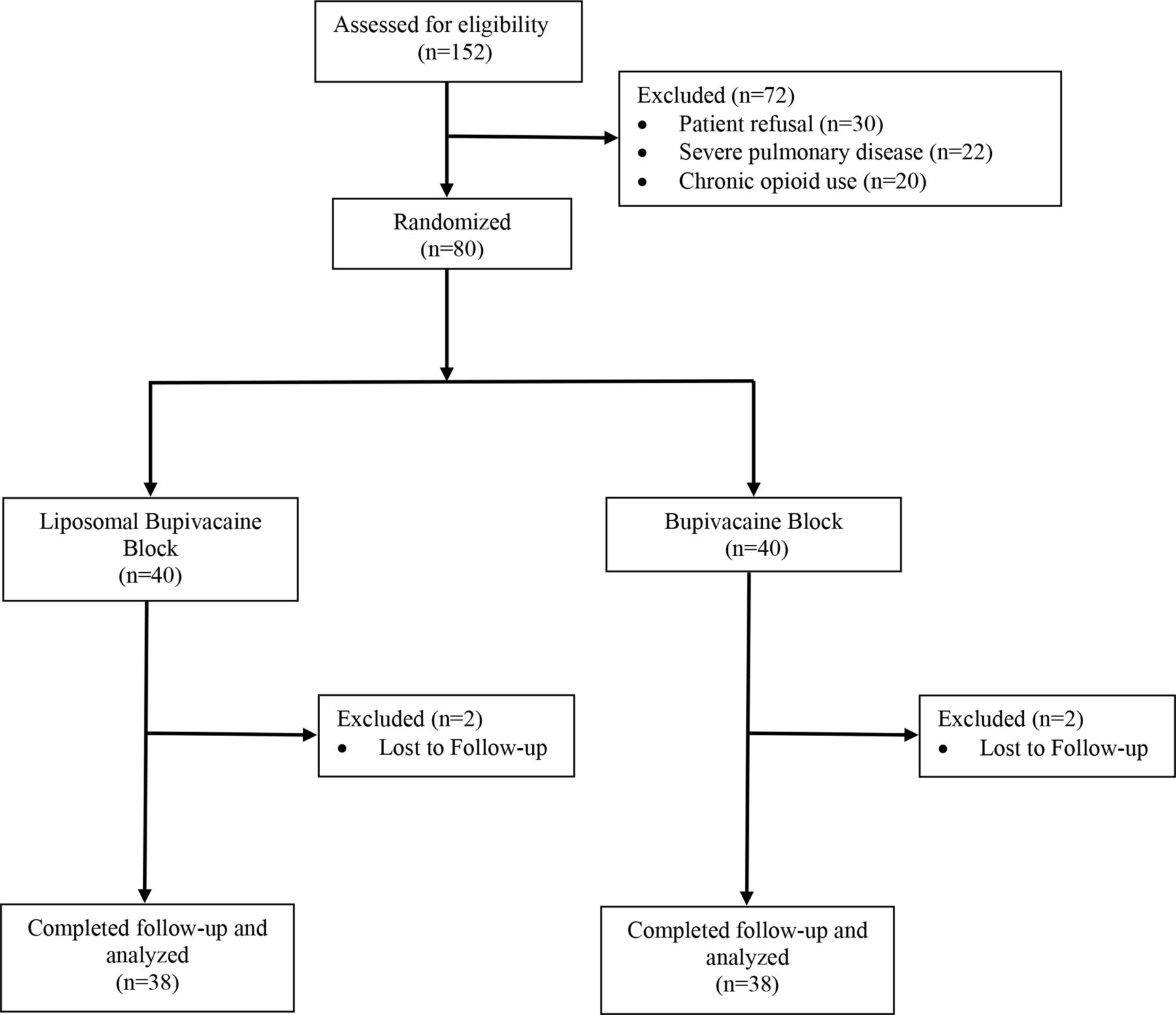
Consolidated Standards of Reporting Trials statement flow diagram.
Demographic data and perioperative characteristics
Primary outcome: 0–72 hours opioid consumption non-inferiority
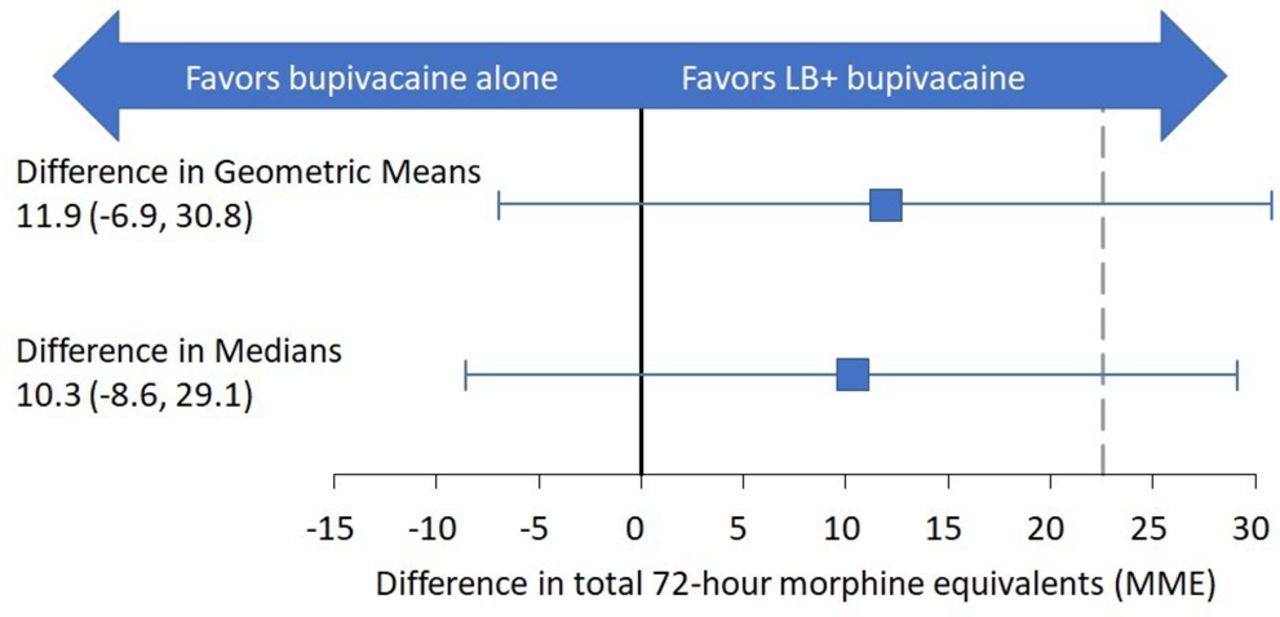
Analysis of the primary outcome of this study showed 72-hour cumulative geometric mean MME consumption for the LB group of 19.3±4.0 mg and for the Bupi group of 31.1±3.5 mg. The geometric mean difference between groups (calculated on the log scale) was 11.9 mg (95% CI −6.9 to 30.8). The 95% CI includes the non-inferiority margin of 22.5; thus, non-inferiority was not demonstrated (figure 2). Median 72-hour cumulative morphine equivalent consumption for the LB group was 36.3 mg (IQR: 7.5–64) and for the Bupi group was 46.5 mg (IQR: 26.3–67.5). The difference in medians was 10.3 mg (95% CI −8.6 to 29.1) (p=0.3).
{kind=link}
{kind=link}
Non-inferiority diagram with observed difference between liposomal bupivacaine (LB) and Bupi groups in geometric mean cumulative 72-hour oral morphine equivalent consumption. The difference in medians and 95% CI is shown for comparison. The dashed line designates the non-inferiority margin (Δ). The horizontal bars designate the 95% CI of the difference between LB and Bupi groups.
Individual time-point comparisons of opioid consumption
There was a statistically significant difference in geometric mean opioid consumption at 72 hours between the Bupi (6.1±3.0 mg) and LB (2.7±3.4) groups (p=0.045). No other statistically significant differences were observed (tables 2 and 3).
Secondary outcomes in PACU following surgery
Secondary outcomes PACU to 1 week following surgery
Pain scores and patient satisfaction
There was a statistically significant difference in resting geometric mean NRS pain scores at 48 hours between the Bupi (1.9±0.8) and LB (1±1) groups (p=0.03). Otherwise, there were no statistically significant differences in all other NRS pain scores or satisfaction with analgesia between groups (tables 2 and 3).
Duration of sensory block and block-related adverse events
Geometric mean perceived sensory block duration was 24.3±0.9 hours in the Bupi group compared with 39.9±0.6 hours in the LB group (p<0.001). There were two unanticipated admissions for shortness of breath following surgery in the Bupi group and one in the LB group within the first 24 hours following surgery (p=0.6). No other block-related adverse events were reported.
1-week outcomes
There were no statistically significant differences in NRS pain scores, patient satisfaction (table 3), or persistent opioid use between the Bupi (50%) and LB (50%) groups (p=0.9).
Discussion
This study did not demonstrate non-inferiority between an interscalene brachial plexus block using bupivacaine alone and a combination of LB plus bupivacaine, with regards to 72-hour cumulative opioid consumption following total shoulder arthroplasty. However, the point estimates for the total difference in opioid consumption, approximately 12 mg MME, equates to one and a half tablets of oxycodone over 3 days. Given the 10 mL of LB used in our study, the differential in cost associated with LB use is more than two orders of magnitude greater than conventional parenteral opioids without any clinically meaningful improvement in analgesia (133 mg of LB: US$198.84 vs a single 5 mg tablet of oxycodone: US$0.62).21 22 Other studies evaluating the efficacy of LB in interscalene block for shoulder surgery have similarly demonstrated clinically unimportant reductions in either pain scores or opioid consumption.9 15 23 When an additive such as dexamethasone is added to bupivacaine for interscalene block, the small reduction afforded by LB may become even smaller.24 25
While subjects in the LB group reported an increased perceived sensory block duration when compared with the Bupi group, this difference did not translate into a relevant improvement in analgesia. Both opioid consumption at 72 hours and resting pain scores at 48 hours showed statistically significant reduction in the LB group when compared with the Bupi group; however, these differences were not clinically meaningful. All other secondary outcomes were similar between groups, including satisfaction with analgesia and unanticipated inpatient admissions following surgery. Despite a prolonged blockade of diaphragmatic function with the use of LB,26 we did not observe an increased number of admissions for shortness of breath. This might have been due to subject selection, as we excluded patients with pre-existing pulmonary disease. Thus, our results cannot be extrapolated to this surgical entire cohort.
Currently, continuous brachial plexus nerve blocks appear to be a reliable method by which prolonged postoperative analgesia in total shoulder arthroplasty can be provided.5 13 These perineural catheters also have the added advantage of rapid discontinuation in the setting of block-related adverse events and replacement in the event of block failure, an option which does not exist in single-injection blocks. However, continuous catheters are not without their own challenges. Placement of continuous nerve blocks requires a higher level of expertise, longer procedural time, and has associated increased costs versus single injection techniques.6
Our study has a number of limitations. First, given that our outcomes relied on subject reporting in an outpatient setting, there may have been inaccuracies in how subjects recall their experiences following discharge. While these data are potentially less accurate than similar outcomes in an inpatient setting, due to the nature of the surgery, it would be unethical to retain subjects in the hospital simply to perform more accurate data collection.
Second, our study was designed assuming a relatively normal distribution of cumulative MME between groups 72 hours following surgery. However, we found substantial skew due to outliers in the distribution. As a result, this study may have been relatively underpowered for the non-inferiority comparison.
Third, although we did not find non-inferiority between the two treatment groups, the resultant difference in geometric means for opioid consumption was small enough to be clinically unimportant. Our margin was based on prior research studies and expert recommendation.16 17 27 It is possible that the use of our standardized multimodal analgesia protocol was highly effective in lowering opioid consumption within this surgical cohort in such a way that made comparison of any intervention challenging to assess. While testing these interventions independently from the use of multimodal analgesia may have yielded alternative results, we feel that it would be both unethical and clinically irrelevant to do so.
Finally, in the absence of guidance regarding important magnitudes of opioid reduction, correlates are often used such as opioid-related adverse events. Our study was not exhaustive in this regard (ie, nausea, vomiting and pruritus). While these are often collected in conjunction with opioid consumption and pain scores, there is often no context in terms of more globally relevant data points, such as unanticipated admissions. Our investigators tracked any such utilization of healthcare resources over the 1 week following surgery to determine if either block-related adverse events or opioid-related adverse events showed difference between groups. However, as the results indicated there were no clinically meaningful differences in any outcome.
In summary, an interscalene brachial plexus block performed with bupivacaine alone did not demonstrate non-inferiority compared to a mixture of LB plus bupivacaine with regards to 72-hour cumulative opioid consumption following total shoulder arthroplasty. However, the difference between groups did not appear to be clinically meaningful. Further studies are warranted to contextualize the value of LB in this setting.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by University of Virginia Institutional Review Board, Charlottesville, Virginia (HSR210190). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to recognize the contributions of regional anesthesia fellows Federico Jimenez-Ruiz, MD and Michael Glick, MD who worked to recruit study patients, coordinate study blocks and performed data collection. We would also like to thank faculty members of the regional anesthesia and acute pain division at the University of Virginia who assisted in supervision of the study blocks. Finally, the authors would like to recognize a shining light which was lost to the opioid epidemic: Jessica Marie Hammons (July 24, 1977 – August 31, 2015). This research is done in her memory.
References
Footnotes
Contributors DAE, BCW, SFB and NAH: this author helped design the study, conduct the study, analyze the data and write the manuscript. JRC: this author helped conduct the study, analyze the data, and write the manuscript. CMR, PEA and AES: this author helped analyze the data and write the manuscript. DAE is responsible for the overall content and acted as the guarantor for this study.
Funding Department of Anesthesiology, University of Virginia, Charlottesville, VA, USA.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.