Article Text

Abstract
Background/Importance Liposomal bupivacaine (LB) is a prolonged release formulation of conventional bupivacaine designed for prolonging local or peripheral regional single injection anesthesia. To this day, the benefit of the new substance on relevant end points is discussed controversial.
Objective The objective was to determine whether there is a difference in postoperative pain scores and morphine consumption between patients treated with LB and bupivacaine hydrochloride in a systematic review and meta-analysis.
Evidence review Randomized controlled trials (RCT) were identified in Embase, CENTRAL, MEDLINE and Web of Science up to May 2020. Risk of bias was assessed using Cochrane methodology. Primary end points were the mean pain score difference and the relative morphine equivalent (MEQ) consumption expressed as the ratio of means (ROM) 24 and 72 hours postoperatively.
Findings 23 RCTs including 1867 patients were eligible for meta-analysis. The mean pain score difference at 24 hours postoperatively was significantly lower in the LB group, at −0.37 (95% CI −0.56 to −0.19). The relative MEQ consumption after 24 hours was also significantly lower in the LB group, at 0.85 (0.82 to 0.89). At 72 hours, the pain score difference was not significant at −0.25 (−0.71 to 0.20) and the MEQ ratio was 0.85 (0.77 to 0.95).
Conclusion The beneficial effect on pain scores and opioid consumption was small but not clinically relevant, despite statistical significance. The effect was stable among all studies, indicating that it is independent of the application modality.
- analgesia
- nerve block
- pain
- postoperative
- pain management
- pharmacology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All relevant data are included in this review and/or supplements.
Statistics from Altmetric.com
Introduction
Two demands to regional anesthesia have been rising over the last couple of years, one being a need for faster mobilization after surgery, the other an analgesia concept with less opioids being used and prescribed. Catheter techniques are left for single injection analgesia wherever possible to achieve the goal of faster mobilization and discharge. Many adjuvants to local anesthetics have been tested to increase the effective duration of a single injection anesthesia. Another promising candidate in this development is liposomal bupivacaine (LB), an extended release formulation of bupivacaine indicated for single-dose administration. In LB, the drug bupivacaine is encapsulated into multivesicular liposomes resulting in prolonged release for up to 72 hours after injection.1 LB is approved by the Food and Drug Administration for infiltration at the surgical site, transversus abdominis plane block (2011) and for interscalene brachial plexus block (2018). Since 2020, it is approved by the European Medicines Agency for field block infiltration, brachial plexus block and femoral nerve block.
Thus, the shortcomings of a single injection of plain bupivacaine hydrochloride (PB) for nerve blockades or local infiltration (duration of analgesic effect typically <24 hours) may be overcome by the new formulation.1 It has been suggested that LB may be an effective alternative for delivering prolonged postoperative anesthesia when compared with continuous nerve blockade techniques (catheters), as technical and personal demands are substantially lower in single injection blockades.2
Since its approval in 2011 in the USA, several studies have investigated LB for a variety of indications, including nerve blockades in arthroscopic surgery, wound infiltration after laparoscopic surgery and nerve blockades or periarticular infiltration in total joint arthroplasty. The ensuing results were heterogeneous regarding potentially beneficial effects on pain scores and opioid consumption. Previous meta-analyses regarding this topic are not conclusive, as they either focus on specific anesthesia techniques (eg, local or regional), or on specific surgical procedures such as shoulder surgery, joint replacement surgery or laparoscopic,3–6 although some of the existing meta-analyses had wide inclusion criteria, such as non-randomized or cohort studies.4 5 7 8
Of course, the gold standard to evaluate an intervention like LB is to measure it in randomized controlled trials of high quality under strictly defined conditions, for example, shoulder replacement and interscalene plexus block only. Thus, when there is a lack of data, extending the inclusion criteria does not necessarily help finding the true effect, but increases bias in all kinds of directions. Pooling different uses of LB on the other hand is also problematic. The analgesic duration and effectiveness of a local anesthetic depends on factors like the blood circulation of the tissue it is used in and the proximity and number of neurons reached by it. These confounders are so important that comparing the absolute effect of LB in regional and local infiltration analgesia is most likely pointless. However, if there is a difference in the analgetic duration or effectiveness of LB compared with PB, it is a pharmacological effect. And despite the many confounders on the absolute difference regarding duration and effectiveness of both, we assume that the relative difference between the two should be stable among all uses of it.
The objective of our meta-analysis is to compare the analgesic efficacy and the relative, pharmacological differences between liposomal and plain bupivacaine from randomized controlled trials to give an understanding of what can be expected of LB in the future.
Methods
Study registration
The present study was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement9 and prospectively registered on 7 August 2019 in the PROSPERO registry (International Prospective Register of Systematic Reviews, PROSPERO CRD42019135615).
Search strategy
Potentially relevant studies were identified through a comprehensive literature search of the MEDLINE, CENTRAL, Embase and Web of Science electronic databases. To prevent publication bias the search strategy was as extensive as possible. The databases were searched for randomized controlled clinical trials comparing LB and PB in adult patients undergoing peripheral nerve block or local infiltration analgesia (such as wound infiltration or periarticular approaches) from the earliest records. The last search update was performed in May 2020. The PICOS scheme was applied as follows: P (patients) was defined as adult patients receiving local or peripheral regional anesthesia. P was left unrestricted in the search term to maximize the sensitivity of the search. I (intervention) was defined as local, regional or infiltration anesthesia with LB, searching for the terms (liposomal bupivacaine) OR (liposome bupivacaine) OR (depofoam) OR (exparel) OR (extended release bupivacaine). C (comparison/control) was defined as regional, local or infiltration anesthesia with PB searching for the terms (bupivacaine) OR (bupivacaine hydrochloride) OR (plain bupivacaine) OR (standard bupivacaine) OR (bupivacaine HCl). O (outcome) was defined as pain reduction, analgesic effect, duration of analgesia and adverse events incidence. O was left unrestricted in the search terms for the same reason as for P. S (study design): only randomized controlled trials were eligible for inclusion. RCT filters were not used in the search strategy to prevent the exclusion of relevant results due to higher precision of the search.
The detailed search terms for each database are provided in the online supplemental files.
Supplemental material
Funnel plot analysis was conducted to identify possible publication bias.
Inclusion and exclusion criteria
The included study types were restricted to RCTs comparing LB with PB in local anesthesia, infiltration or regional anesthesia. Conference abstracts or meeting abstracts were not excluded a priori. We made no language restrictions.
Data extraction
At least two reviewers (A-KS, BO and H-CD) screened the studies and performed the data extraction. They also investigated the full-text versions of the included studies independently. The reviewers collected data containing relevant information concerning the predefined primary end point parameters, that is, pain scores and opioid consumption, as well as concerning secondary end point parameters, including adverse effects. All studies included in this review were characterized in regard to their patient collective, demographic characteristics, type of surgery and anesthesia, methods, setting, groups, length, interventions and end points.
The methodological quality of the eligible RCTs was assessed using the Cochrane Tool for the Risk of Bias Assessment,10 and included the items randomization, allocation concealment, participant blinding, outcome assessment blinding, incomplete outcome data, intention-to-treat analysis, selective bias and other bias.
Discrepancies and disagreements were resolved by discussion and under the supervision of a third author (TW). Engauge Digitizer 10.411 was used for extraction if data were presented graphically only. If different doses of either substance were used, data were pooled for analysis.
Risk of bias assessment
The assessment for the risk of bias (RoB) followed the recommendations supplied by the Cochrane handbook10 where applicable. In addition, an eighth RoB category was introduced, which provided a third category describing the process of blinding in an individual study more precisely. The standard seven-item RoB evaluation provides two categories for blinding (performance and assessment). For this meta-analysis, we split the performance blinding into patient blinding and performer blinding, resulting in the mentioned eighth RoB item.
The RoB table was created using Microsoft Excel for Mac, V.16.33.
Data synthesis and analysis
Data for pain scores and morphine equivalents (MEQ) were recorded as the mean±SD. If not available, the mean and SD were estimated from the median and range as described by Hozo et al 12 and for median and IQR as described by Luo et al and Wan et al.13 14
The SD was obtained from the SE by multiplying by the square root of the sample size (according to the Cochrane handbook).10
If not available, SD was imputed as average SD from similar studies according to the Cochrane handbook.10
Data for adverse events were extracted as dichotomous events for both groups.
All statistical meta-analyses were performed with R package meta (R Development Core Team, Vienna, Austria). Meta-analysis was performed calculating the weighted mean difference (MD) for pain scores and ratio of means (ROM) for MEQ for comparisons of continuous data. For dichotomous data, meta-analysis was performed calculating the risk ratio (RR). All calculations are stated with the 95% CI. Statistical significance was defined as p values ≤0.05. Statistical heterogeneity was assessed using the χ2 test and I2 values.15 As the chosen end points are likely to depend on modalities that vary between the individual studies, some heterogeneity was expected to occur. Accordingly, a random effect model was applied.
A pain score difference of >1.5 on a 0–10 scale was considered to be clinically relevant according to Cepeda et al and Farrar et al.16 17 According to clinical experience, a morphine-sparing effect of >30% was considered to be clinically relevant.
For missing or incomplete data, we contacted the corresponding authors of the included studies twice to obtain the additional information.
Trial sequential analysis
Trial sequential analysis (TSA) was performed to assess whether the primary end point results of the analysis are conclusive. As repeated significance testing of accumulating data increases the possibility of type 1 error, a TSA was performed to assess the strength and maturity of available evidence. The strength of the evidence can be considered by determining the required information size for a conclusive meta-analysis. In order to control the type 1 error, the alpha-spending function was used to adjust the threshold for statistical significance to account for the elevated risk of random error before the meta-analysis has reached its required information size.
We performed TSA using the software distributed by the Copenhagen Trial Unit, Center for Clinical Intervention Research, Rigshospitalet, Copenhagen, Denmark.18–20 A DerSimonian-Laird random effects model was applied. We assumed a two-sided α of 0.05 and β of 0.2, resulting in a power of 0.80.
End points
The primary end points were the reported pain scores (converted to a numeric rating scale from 0 to 10) at 24 hours and 72 hours after surgery, and the total postoperative cumulative opioid consumption in intravenous MEQ over 24 and 72 hours, because 24 hours is the most relevant timepoint for single injection anesthesia and 72 hours is stated to be the prolonged duration of LB.
Data on adverse events were extracted as secondary end points.
Results
Comprehensive literature search
Due to the novelty of the topic, the amount of literature on the field was not exceedingly high, therefore it was possible to conduct a comprehensive search strategy with a manageable amount of studies. The literature search identified 2718 studies, 1368 titles and abstracts were screened after duplicate removal. Twenty-three full-text articles21–43 were included in this systematic review. The study inclusion process is shown in figure 1. The detailed search term is provided in the online supplemental content 1.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of literature search and study inclusion.
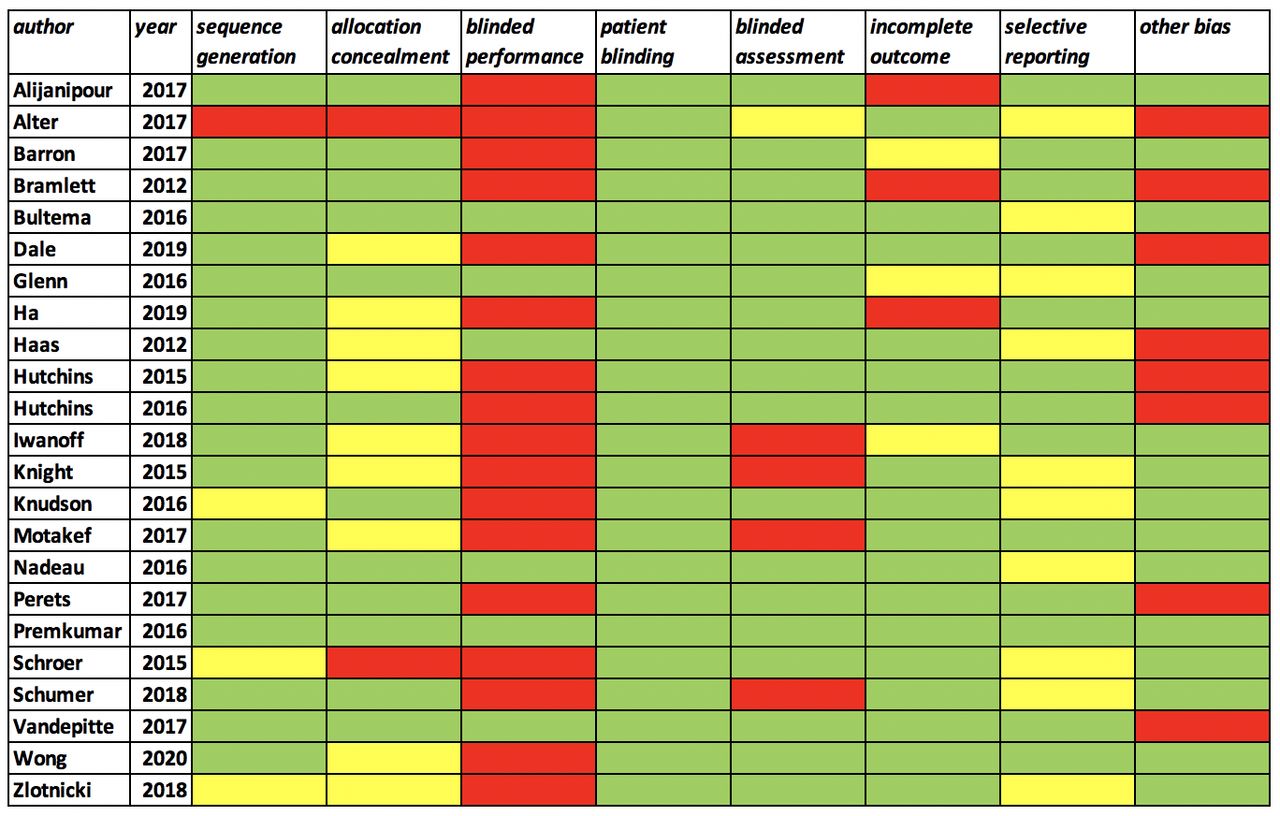
Risk of bias assessment
With 23 included studies in 8 categories for RoB, the total number of items was 184. A high RoB was given 35 times. Seventeen of the high-risk items were allocated for study conduction with an unblinded performer of the intervention. The patient was blinded in all included studies, while the assessment was blinded in 18 or 19 studies (1 unclear risk). The only high-risk items occurring in the ‘other bias’ category addressed third-party (pharmaceutical industry) funding by the pharmaceutical distributor of LB (figure 2).

Risk of bias summary of included studies.
The demographic characteristics of the included RCTs are presented in the online supplemental content. Study characteristics of the included RCTs are shown in table 1.
Details of included studies
Details of RoB assessment are presented in online supplemental content.
The analysis of funnel plots showed no publication bias for mean pain score difference 72 hours and for ratio of MEQ at 24 and 72 hours. For mean pain score at 24 hours, a potential publication bias was detected. The funnel plots are provided in the online supplemental content.
High certainty: we are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: we are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different
Primary end points
Pain scores 24 hours
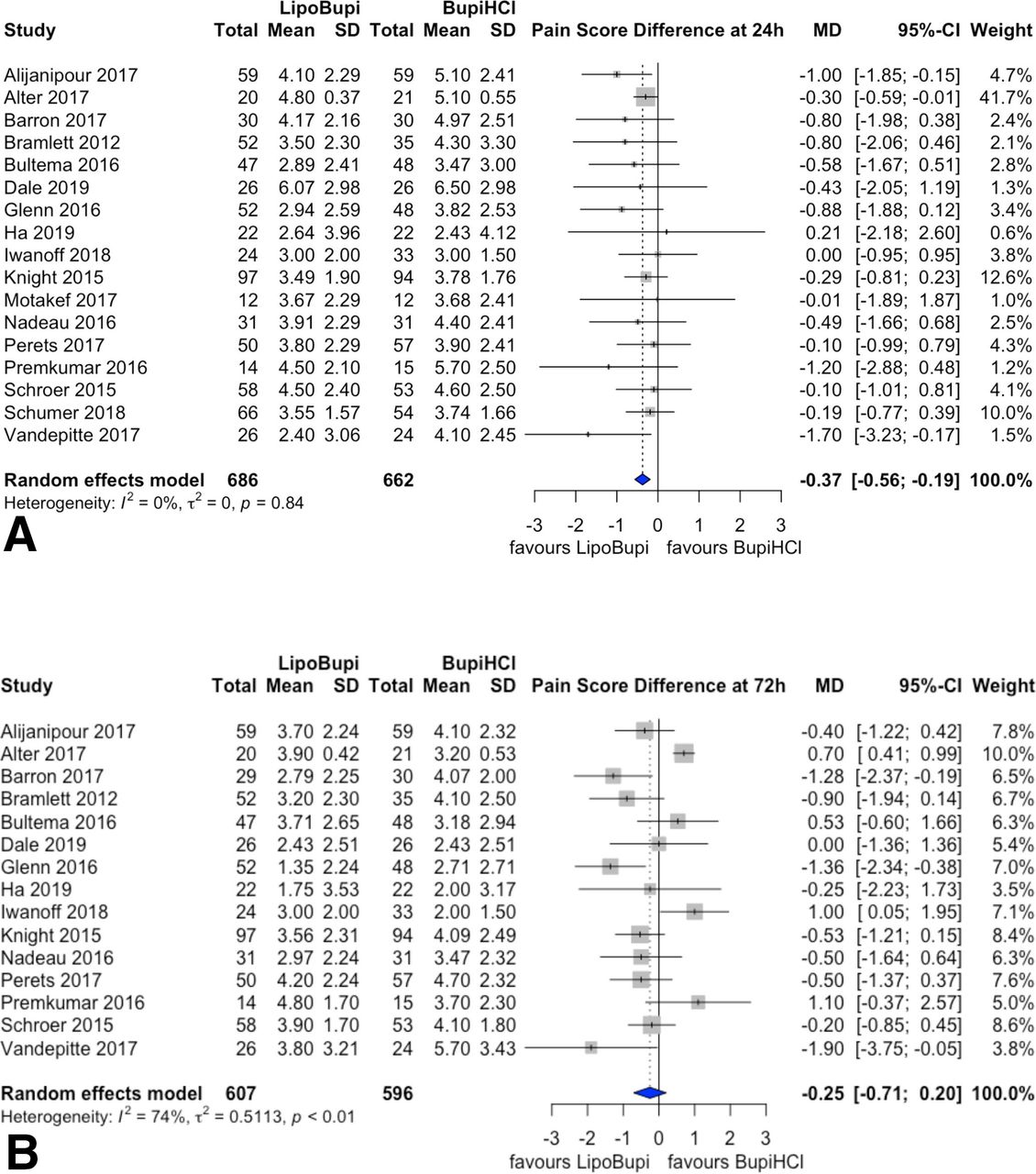
Seventeen studies reported the pain scores at 24 hours postoperatively. The overall effect estimator was −0.37 (95% CI −0.56 to −0.19). The heterogeneity was low with an I2 of 0%. The forest plot summarizing the pain scores at 24 hours postoperatively can be seen in figure 3. Cumulative pain scores or short-term pain score trends were not reported sufficiently, therefore an area under the curve analysis could not be conducted.
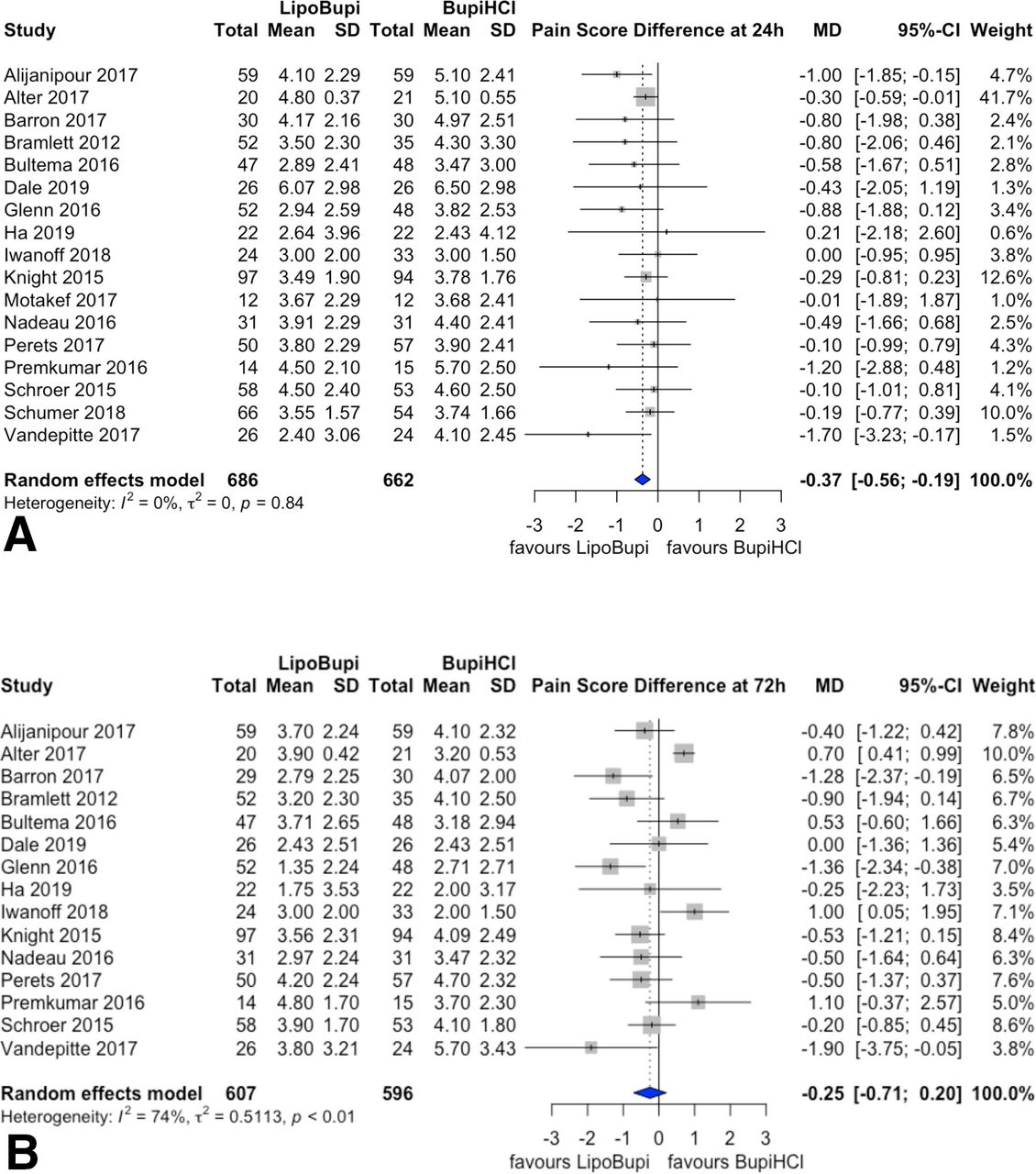
Forest plot of mean pain scores after 24 hours (A) and after 72 hours (B). Mean pain score differences between liposomal bupivacaine and plain bupivacaine. Pooled estimates of the weighted mean difference are shown with 95% CIs. Pooled effect estimates are presented as diamonds and lines depict the 95% CIs.
Pain scores 72 hours
Fifteen studies reported the pain scores at 72 hours postoperatively. The overall effect estimator was −0.25 (95% CI −0.71 to 0.20). The heterogeneity was high with an I2 of 74%. The forest plot summarizing the pain scores at 72 hours postoperatively is shown in figure 3.
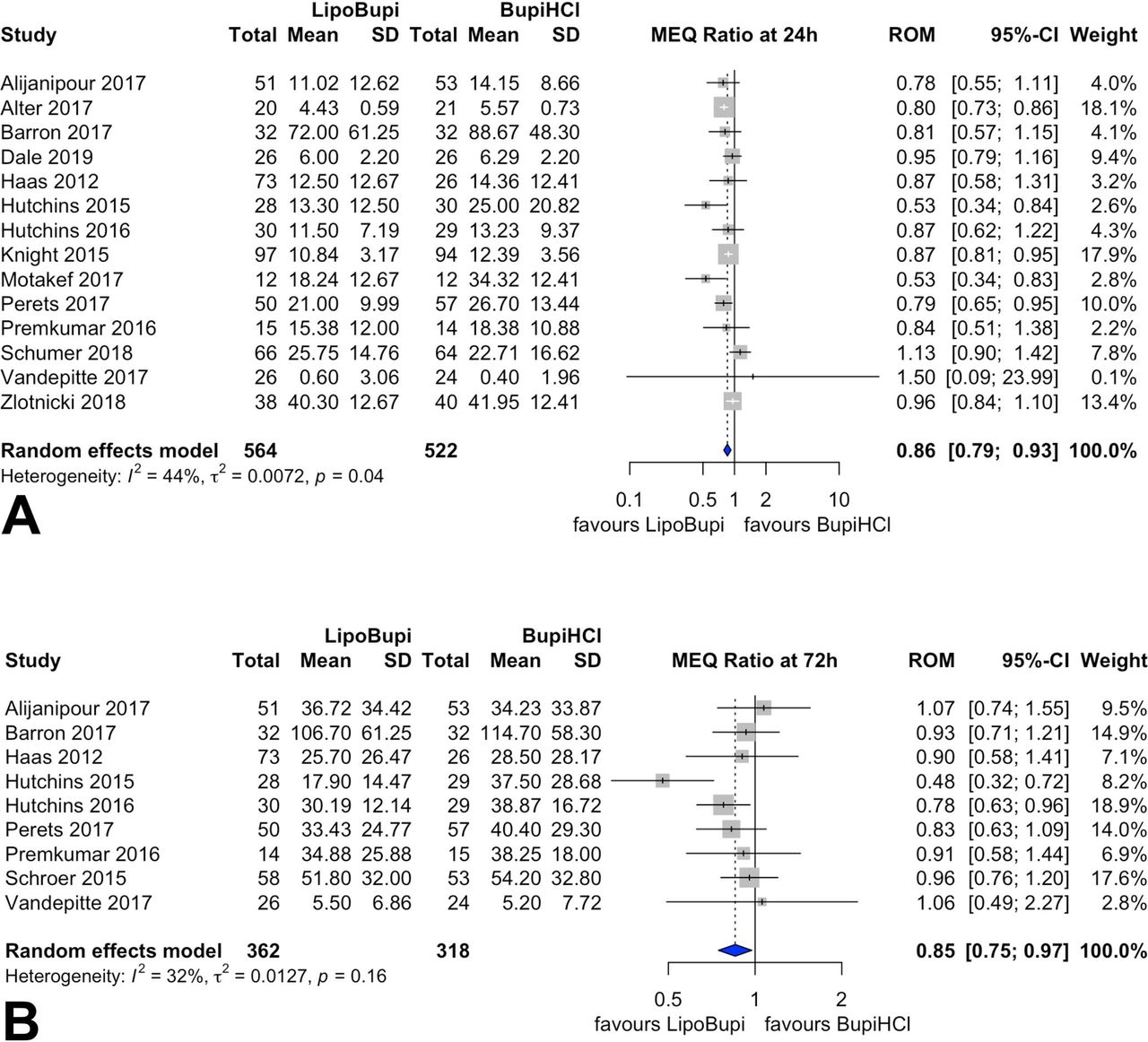
MEQ 24 hours
Fourteen studies reported the total MEQs consumed at 24 hours postoperatively. The overall effect estimator for the ROM was 0.85 (95% CI 0.82 to 0.89). The heterogeneity was low with an I2 of 44%. The forest plot summarizing the MEQs consumed at 24 hours is shown in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of cumulative morphine equivalents after 24 hours (A) and after 72 hours (B). Ratio of means for cumulative morphine equivalents. Liposomal bupivacaine compared with plain bupivacaine. Pooled estimates of the ratio of means are shown with 95% CIs. Pooled effect estimates are presented as diamonds and lines depict the 95% CIs.
MEQ 72 hours
Nine studies reported the consumed cumulative MEQs at 72 hours. The overall effect estimator for the ROM was 0.85 (95% CI 0.77 to 0.95). The heterogeneity was low with an I2 of 32%. The forest plot summarizing the MEQs consumed at 72 hours is reported in figure 4.
Time to first analgesic request
The time to first analgesic request was reported in only three studies.31 33 41 Vandepitte et al 41 reported a time to first analgesic request of 2598 (LB) vs 2778 (PB) min, Knight et al 33 of 271.9 (LB) vs 248.3 (PB) min and Hutchins et al 31 of 20 (LB) vs 23 (PB) min, respectively. Meta-analysis was not conducted for this end point.
Secondary end points
The reported number of adverse events associated with the intervention was low. Eleven studies with a number of 853 patients reported adverse events. From most to least frequent, the following adverse events were observed: nausea and vomiting (106 (LB) vs 137 (PB) cases), dizziness (14 vs 4 cases), pruritus (15 vs 13 cases). Only one study41 observed serious adverse events (symptoms of systemic toxicity like ear ringing or metallic taste) in four (LB) versus three (PB) cases. Alijanipour et al 21 observed neurological complications twice and a wound healing complication once in patients receiving LB (vs none with PB).
No allergic reactions or deaths were reported. Details of adverse events and side effects rates are presented in the online supplemental digital content 3.
The summary of findings and GRADE results are reported in table 2.
Summary of findings
Sensitivity/Subgroup analysis
A sensitivity analysis regarding the effect of blinding, funding and general methodological quality was initially planned but not done as due to the low amount of inconsistency a substantial change in the effect estimator is statistically not possible.
Trial sequential analysis
Pain scores 24 hours
The results for TSA for pain scores after 24 hours are shown in the online supplemental content 4. The estimated required information size of 1063 patients was achieved (1348 patients were included in this meta-analysis). The cumulative Z-curve crossed the conventional boundary (Z=1.96; p=0.05) as well as the O’Brien-Fleming boundary (alpha spending function).
MEQ 24 hours
The results for TSA for cumulative MEQ after 24 hours are shown in the online supplemental content 5. The estimated required information size of 1267 patients was not achieved (1086 patients were included in this meta-analysis). The cumulative Z-curve crossed the conventional boundary (Z=1.96; p=0.05) as well as the O’Brien-Fleming boundary (alpha spending function).
Discussion
The comprehensive systematic review and meta-analysis presented here is based exclusively on randomized controlled trials comparing the efficacy and safety of LB with PB in patients receiving local infiltration analgesia or peripheral regional anesthesia.
The results show small differences in pain scores between both drug formulations at 24 and 72 hours after surgery. Despite the statistical significance of some of the results, the effect sizes are considered clinically not relevant in concordance to pain score cut-offs that are proposed by Cepeda et al 16 and Farrar et al 17 as a clinically detectable pain score difference needs to be 1.3–2 points on a scale of 0–10 in order to be objectively and subjectively noticeable.
Furthermore, this meta-analysis shows a statistically significant reduction of MEQs consumed over 24 and 72 hours, respectively. The observed opioid-sparing effect of 15% in MEQs is arguably clinically relevant, especially since the overall rate of opioid-related side effects was low and the dose reduction did not alter the rate of adverse events (supplemental digital content).
The literature research conducted was exhaustive, as it was not restricted to English language publications and included published manuscripts as well as conference abstracts. Any further restrictions in the PICO scheme could potentially have led to the exclusion of relevant results and were therefore avoided. Our eligibility criteria were restricted to RCTs in order to aim for high evidence.
To detect a possible publication bias in the literature on LB, we provided the funnel plots for all primary end points (online supplemental files). The analysis showed a homogenous distribution of studies (effect measures with respect to study size) for mean pain score difference at 72 hours and for ratio of MEQ at 24 and 72 hours, implying a low risk of publication bias. For the end point mean pain score at 24 hours postoperatively, a small publication bias is likely to exist. In a normal distribution of effect estimates dependent on study size, some smaller studies would be expected that actually show a higher pain score with LB due to chances. Since the distribution is slightly asymmetric, the potential publication bias may lead to overestimation of the analgesic effect of LB at 24 hours.
The chosen end points pain scores and MEQ consumption are the most common and valid measures to estimate the effectiveness of an anesthetic or analgesic intervention. The chosen time intervals are the most informative and important when investigating the potential of prolonged single injection local or regional anesthesia. At 24 hours, the analgesic effect of traditional single injection anesthesia is limited and an improvement at this timepoint is of high clinical relevance. The 72 hours timepoint was chosen as it is the claimed pharmacological active duration of the slow release formulation.
We pooled different application modalities (local infiltration, regional anesthesia, field blocks) to characterize the relative pharmacological effect of LB compared with PB that is independent of the application modality. The limitation to this is that the relative measures are more difficult to interpret as, for example, an absolute block prolongation in minutes or hours. Of course, comparing absolute time measure in a pooled analysis of local and regional application modalities is obsolete, but the relative effect of a pharmacological substance should be stable among all interventions. And the fact that the heterogeneity in our results was so low indicates the correctness of this assumption and the pharmacological stability of the observed effect in this analysis. Furthermore, due to the low heterogeneity the results are likely to be applicable to other clinical situations.
Very recently, a comparable systematic review on LB has been conducted by Hussain et al.44 According to the results presented here, the authors did not detect a statistically or clinically relevant benefit of LB. Apart from that, the approach of Hussain et al was different regarding their restriction to periarticular infiltration analgesia after total knee arthroplasty, while being rather unrestricted concerning control group. This led to a different set of included studies, which may explain the slightly increased heterogeneity in the review of the study by Hussain et al.44
As there were large differences in the painful surgical stimulus ranging from less painful interventions (soft tissue surgery) to painful and major surgery (endoprosthetic surgery), the differences in MEQs consumption had to be calculated and interpreted as a relative measure (ratio of the mean) instead of absolute difference. The underlying assumption is that LB has a relative morphine-sparing effect in general. The absolute morphine-sparing effect will be larger after painful surgery than in less painful interventions.
Subgroup analysis with the purpose of identifying potential confounders or explanations for bias was considered ahead of and during the course of this study. A large number of studies was expected to show biased results due to pharmaceutical sponsoring. Another potential confounder was considered to result from pooling different application modalities.
In meta-analyses with high heterogeneity, sensitivity analysis can help to explain the observed heterogeneity and can generate hypothesis which subgroups of patient could benefit or get harmed by the intervention of interest. Subgroup can further identify confounders or bias. Subgroup analysis of high-quality studies sometimes allows to clarify if an effect is overestimated or underestimated.
However, if heterogeneity is low or not existing the analysis of any possible combination of studies analyzed in a subgroup is statistically futile and cannot possibly change the estimated effect, at least not substantially. As this was the case in this study, no subgroup analysis was conducted.
The low heterogeneity indicates that the estimated treatment effects of LB are independent of the application modality (local infiltration, regional anesthesia) and that the relative effect on MEQs consumption is independent of the type of pain.
This argumentation also applies to the question whether blinding substantially biased the presented results. We conclude that performer blinding as well as funding did not influence the outcome of this study as otherwise methodologically well-performed studies were included.
Regarding the forest plot for mean pain scores after 24 hours postoperatively, the study performed by Alter et al was weighted with 41.7% due to its small SD. Compared with the other studies in this review, the distribution of data is statistically difficult to explain and can result from an extremely unlikely event or flawed data.
To verify if the exclusion of the study by Alter et al 22 leads to a significant bias of the effect estimator, we excluded this study once. However, excluding this study from meta-analysis does not change the effect estimator (−0.43 (95% CI −0.67 to −0.19)) (forest plot not shown).
According to the TSA, the meta-analysis for pain scores at 24 hours is conclusive, as the estimated required information size was achieved. The meta-analysis for cumulative MEQ at 24 hours is not conclusive, as the required information size was not achieved. However, the cumulative Z-curve crosses the alpha spending boundary, indicating that the effect estimator is likely to stay significant.
Conclusion
In conclusion, the meta-analysis shows no clinically relevant analgesic benefit of LB. The observed effect was stable among all application modalities and is therefore assumed to be independent of the application modality. The TSA showed that future studies are unlikely to change the effect estimator.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All relevant data are included in this review and/or supplements.
Acknowledgments
The authors would like to thank Tilo Koch, Gesa Kix, Ruzica Axt of the institutional study office and Veronika Straka and Marion Riehl of the medicinal library for their help with obtaining the articles. The authors would also like to thank Gertrude Duncan for proofreading the manuscript as a native speaker.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors A-KS: helped with substantial contributions to the conception and design of systematic review, data collection and acquisition, analysis and interpretation of data, drafting the article, final approval of the version to be published, agreement to be accountable for all aspects of the work. H-CD: helped with substantial contributions to the conception and design of systematic review, data collection and acquisition, analysis and interpretation of data, drafting the article, final approval of the version to be published, agreement to be accountable for all aspects of the work. BO: helped with substantial contributions to the conception and design of systematic review, data collection and acquisition, analysis and interpretation of data, drafting the article, final approval of the version to be published, agreement to be accountable for all aspects of the work. TW: helped with substantial contributions to the conception and design of systematic review, data collection and acquisition, analysis and interpretation of data, revising the article critically, final approval of the version to be published, agreement to be accountable for all aspects of the work. LE: helped with substantial contributions to the conception and design of systematic review, data collection and acquisition, analysis and interpretation of data, revising the article critically, final approval of the version to be published, agreement to be accountable for all aspects of the work. HW: helped with substantial contributions to the conception and design of systematic review, data collection and acquisition, analysis and interpretation of data, revising the article critically, final approval of the version to be published, agreement to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests TW: receives consultancy fees from Teva Pharmaceuticals.; HW: receives speaker’s fees from B. Braun, Vygon and Sintetica
Provenance and peer review Not commissioned; externally peer reviewed.