Article Text

Abstract
Background Radiofrequency (RF) treatment of the genicular nerves has the potential to reduce chronic knee pain due to osteoarthritis or persistent postsurgical pain, however, a direct comparison between the two main modalities used, conventional and cooled, is lacking.
Methods This double blind, non-inferiority, pilot, randomized controlled trial compared the effects of cooled and conventional RF in chronic knee pain patients suffering from osteoarthritis or persistent postsurgical pain after total knee arthroplasty. Patients were randomized following a 1:1 rate. The primary outcome was the proportion of patients with ≥50% pain reduction at 3 months postintervention. Other outcomes were knee pain, functionality, quality of life, emotional health, and adverse events up to 6 months postintervention. Conventional RF treatment was tested for non-inferiority to cooled in reducing knee pain at 3 months follow-up.
Results Forty-nine of 70 patients were included, of which 47 completed a 3-month follow-up. The primary outcome was achieved in 4 of 23 patients treated with conventional RF (17%) vs in 8 of 24 with cooled (33%) (p=0,21). Results from the non-inferiority comparison were inconclusive in relation to the non-inferiority margin. There was no statistically significant difference between secondary outcomes. There were no serious adverse events.
Conclusions Both conventional and cooled RF treatment reduced pain in the osteoarthritis and persistent postsurgical pain population. This pilot study did not demonstrate statistically significant differences in the proportion of patients experiencing ≥50% pain reduction between techniques. The non-inferiority analysis was inconclusive. These results warrant further research.
Trial registration number NCT03865849.
- CHRONIC PAIN
- Pain, Postoperative
- Neuralgia
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Conventional and cooled radiofrequency of the genicular nerves are safe procedures that reduce therapy resistant chronic knee pain due to osteoarthritis and persistent postsurgical pain.
WHAT THIS STUDY ADDS
This pilot randomized controlled trial comparing cooled and conventional radiofrequency modalities suggests that pain reduction is higher in the cooled radiofrequency group, however, the analysis is inconclusive due to the small number of patients included.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Cooled radiofrequency of the genicular nerves might lead to better symptom reduction in chronic knee pain patients compared with conventional radiofrequency. However, the results in this study were not statistical significant, therefore, a large, powered randomized controlled trial is necessary to prove statistical significance.
Introduction
Chronic knee pain is most often caused by osteoarthritis (OA) of the knee, a degenerative process that affects joint cartilage and the subchondral bone.1 OA causes pain, stiffness and loss of function leading to psychological and sleeping disorders, and a diminished quality of life. Worldwide, the prevalence of knee OA is increasing reflecting the aging population and the increasing prevalence of obesity, a well-known risk factor.2 Non-surgical treatment options, including pharmacological therapy, physiotherapy and lifestyle changes, are often insufficient and frequently associated with side effects. Consequently, many OA patients undergo a total knee arthroplasty (TKA).3
Unfortunately, a TKA is not a guarantee of success, given that the incidence of persistent postsurgical pain (PPSP) and functional limitation after TKA is as high as 53%.4 Patients suffering from OA that have exhausted conservative treatments and are not surgical candidates (eg, due to comorbidities or very young age) and PPSP patients only have few therapeutical options.5 Radiofrequency (RF) treatment of the genicular nerves might be a viable treatment option.
RF treatment of the genicular nerves is a minimally invasive treatment that reduces pain by interrupting the conduction of nociceptive stimuli through the application of a radiofrequent current adjacent to the responsible nerves. Recent systematic reviews indicate that RF is a safe and effective treatment in patients with OA of the knee, and to a lesser extent, in PPSP patients after TKA.6–8 Two RF modalities, conventional and cooled RF, are commonly used to target the superomedial, the superolateral and the inferomedial genicular nerve. Prior studies suggest a higher success rate and a longer effect of cooled compared with conventional RF due to an increased lesion size, however, until present, no direct comparative studies have been performed in an randomised controlled trial (RCT).6 9 This knowledge gap warrants further comparative studies. This is the first prospective study to directly compare the effectiveness of conventional and cooled RF in patients with chronic knee pain due to OA or PPSP after TKA. The primary goal was to provide an estimate of clinical treatment effects (pain, physical functioning, mental health, medication use, quality of life and adverse events, (AE)). A pilot design was chosen for the following reasons. First, to assess the feasibility of conducting a sufficiently powered randomized controlled trial in the future. Second, to evaluate the study design and thirdly to calculate a sample size more accurately. We hypothesize that in both patient groups (OA and PPSP), knee pain relief after conventional RF treatment is not inferior to cooled RF. In this article, only the effectivity outcomes will be discussed.
Methods
Trial design
The COCOGEN trial is a prospective, double-blind, randomized, non-inferiority, pilot trial conducted in three participating centers (Hospital Oost-Limburg, Belgium; Maastricht UMC+, The Netherlands; Rijnstate, The Netherlands). Total follow-up time was 6 months. Patients were enrolled from February 10, 2020 to April 28, 2021.
Randomization, allocation, and blinding
Participants were randomly allocated to one of two parallel groups, conventional or cooled RF, with an allocation ratio of 1:1, and variable block size of 2 or 4 after stratification per etiology of pain (OA and PPSP) using the online CASTOR EDC application. The study was double-blinded: both the patient and the outcome assessor were blinded to treatment allocation. The treating pain physician was unblinded. The blinding of patients was tested approximately 30 min after the treatment by asking the patient which intervention they thought they received with the following possible answers: ‘Conventional RF’, ‘Cooled RF’, and ‘I don’t know’. All patients were systematically unblinded 6 months after treatment.
Participants
Patients were recruited by their treating pain physician. Adult subjects were included if they suffered from moderate to severe (Numeric Rating Scale (NRS) >4) chronic anterior knee pain (> 12 months) due to OA or PPSP after TKA that was unresponsive to conventional treatments (physiotherapy, analgesics, or intra-articular infiltrations). For OA patients, a radiologic confirmation of Kellgren-Lawrence (KL) grades II–IV on X-ray or MRI was required.10 For PPSP after TKA patients, a negative orthopedic workout was required.11 Informed consent was obtained in all patients before participation. Exclusion criteria were: body mass index >40 kg/m2; chronic widespread pain; untreated psychosocial disease; radicular pain in index leg; local or systemic infection (bacteremia); uncontrolled immune suppression; uncontrolled coagulopathy (defined as supratherapeutic dose of anticoagulation medication); currently implanted with a defibrillator, neuromodulator or other electrical devices; allergies to products used during the intervention; evidence of inflammatory arthritis or an inflammatory systemic disease responsible for knee pain; intra-articular injections (eg, steroids, hyaluronic acid, platelet enriched plasma) in the index knee during the 3 months prior to start study; previous conventional or cooled RF of the index knee; pregnant, nursing or planning to become pregnant before the treatment; participation in another clinical trial/investigation within 30 days prior to signing informed consent and patients who refused to comply to protocol procedure.
Study procedures and data collection
The study data were collected from the medical patient record, questionnaires, and functionality tests at baseline, 1, 3 and 6 months after the procedure in an online patient case report form in the Castor data management tool. Data collection at baseline included: demographic data, NRS, KL grade of OA, results of goniometry, and results of the timed-up-and-go test (TUG). Data collected at the follow-up visits were: NRS, Oxford knee score (OKS), patient’s self-reported impression of change measured by the Patient’s Global Impression of Change (PGIC), health-related quality of life expressed in EuroQol-5 Dimension- 3 Level (EQ-5D-3L), mental health measured by Hospital Anxiety and Depression Scale (HADS) and in the Pain Catastrophizing Scale (PCS), medication use measured by the change in Medication Quantification Scale III (MQS III), knee functionality measured using goniometry and the TUG test, and AE. The OKS, HADS, PCS and functionality tests were only collected at the 3-month and 6-month follow-up visit. The NRS score at each time point was calculated as the mean score of the previous 4 days, collected using a pain diary.
Intervention
An RF treatment of the superomedial, superolateral, and inferomedial genicular nerves was performed in a standardized manner in both treatment groups using a Halyard/Coolief RF generator.12 A prognostic block prior to the treatment was not performed as a recent study showed no benefit of prior prognostic blocks.13 All patients were monitored. No sedation was used. Patients were positioned in a supine position on a fluoroscopy table with the index knee flexed 10°–15°. The procedure was performed under sterile conditions. For each nerve, the needle was placed guided by ultrasound in the proximity of the genicular nerve at the junction of the shaft and condyle of the femur and tibia. After identifying the target point, the skin and subcutaneous tissues were anesthetized with 1 mL lidocaine 2% at estimated entry point. The needle was advanced using an anterior to posterior ‘in plane’ approach until contact is made with the bony cortex at the center between anterior and posterior of the femur and tibia. If ultrasound guided needle tip position was final a control fluoroscopy image was made to confirm the final needle tip position in AP and lateral view. A sensory threshold (50 Hz) of ≤0.5V and an absent response to motor stimulation (2 Hz) of 1.0V was obtained for each genicular nerve. Consequently, 1 mL of lidocaine 2% was injected at each genicular nerve before RF treatment. The conventional RF was performed using for each nerve a 100 mm, 18-gage, straight RF introducer and a 10 mm active tip RF probe set at a temperature of 80°C at the tip for 90 s. The cooled RF was performed with a 100 mm long, 17-gage, straight RF introducer and a 4 mm active tip, 18-gage cooled RF probe generating a temperature of 60°C at the tip of the probe for 150 s.
Outcomes
Endpoints were chosen following the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) guidelines.14 The primary endpoint is the proportion of patients with a pain reduction of at least 50% at 3 months postintervention. Pain intensity is expressed using the 11-point NRS. The NRS is a unidimensional, subjective measurement of pain intensity, expressed by the patient as a number between 0 and 10, ranging from no pain to maximal pain. A pain dairy containing 3 NRS recordings per day for 4 days prior to each visit during the active hours of the day was collected. The NRS was not specified to be evaluated in rest or in movement, thus aiming to reflect the pain the patient experienced during normal daily activities. We used a threshold of 50% pain decrease, despite the IMMPACT guidelines recommending a threshold of 30%. We chose for 50% as this threshold is most often used in the clinic, as well in previous studies, making comparisons later on easier. In addition, we also collected data on at least 30% pain reduction.
The secondary endpoints were NRS, OKS, PGIC, EQ-5D-3L, HADS, PCS, MQS III, goniometry, TUG test, and AEs.15–23 PGIC was measured using a 7-point Likert scale ranging from ‘0’ meaning ‘Much worse’ to 7 meaning ‘Extremely improved’. Patients scoring 6 and 7 were considered having a significant improvement. Success of blinding was also tested as mentioned previously.
Statistical methods
The rule-of-thumb of Julious suggested including 12 patients per group in case of a pilot study, so that preliminary data on effect sizes, measures of spread, and feasibility can be obtained.24 As this study is stratified by indication (OA and PPSP after TKA), we aimed to include a total of 48 patients.
The clinical outcomes were analyzed according to the intention-to-treat principle. Patient baseline characteristics were described for both knee pain groups separately and stratified by treatment allocation using mean and SD for continuous variables, and count and percentage for categorical variables.
The primary outcome, the proportion of patients achieving treatment success at 3 months after treatment, was computed as percentage and was tested between groups using Pearson’s χ2 test. To test for non-inferiority, mean NRS change from baseline and between group difference in change score, including 95% CI, were calculated at 3 months. The lower bound of the 95% CI of the difference was compared with the non-inferiority limit of 0.75 NRS points.25 26 Other secondary study parameters were reported as mean or percentage difference including 95% CI. All hypothesis testing was considered explorative.
Results
Participants
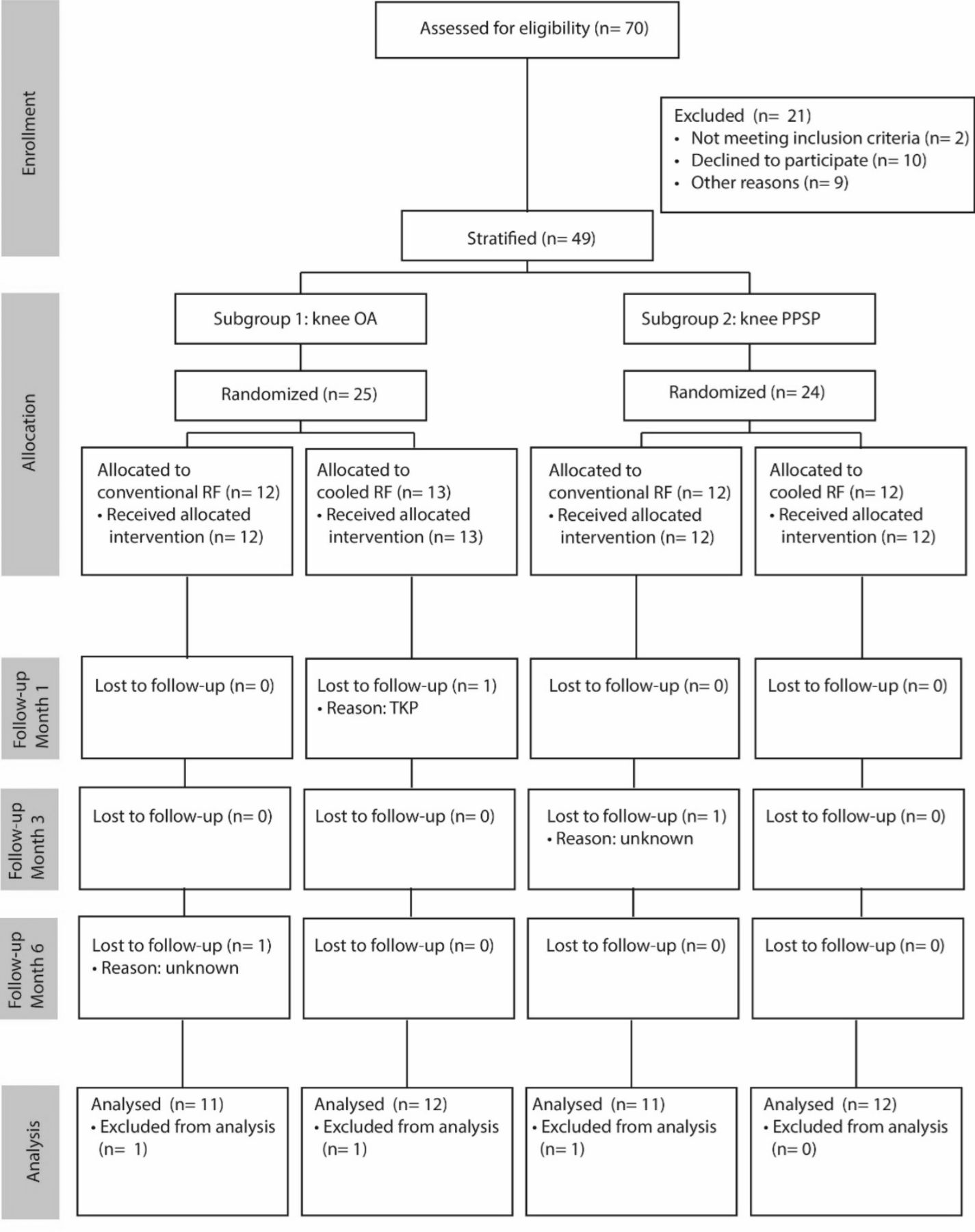
Seventy patients were screened for eligibility, of which 49 were included. One additional patient was included due to a small lag in registration in the database as the last two patients were recruited approximately at the same time in different centers. Figure 1 depicts the Consolidated Standards of Reporting Trials flow chart of participants during the trial. Three patients dropped out, one of which received a TKA. There were further no missing data for the primary endpoint and there were no cross overs between the groups. Table 1 presents the baseline patient characteristics.
Baseline demographic characteristics of patients per stratification group

Participant flow chart during the study. All allocated participants received the planned treatment and were analyzed according to the intention-to-treat principle. OA, osteoarthritis; PPSP, persistent postsurgical pain; TKP, total knee prothesis; RF, radiofrequency.
The primary outcome
There were more patients who achieved the primary endpoint after a cooled RF in comparison with conventional RF as described in table 2. Similarly, a higher percentage of patients reached ≥50% pain reduction after a cooled RF in comparison with conventional RF at all other time points. However, these differences were not statistically significant at each time point.
Percentage of patients with ≥30% and ≥50% pain reduction after conventional and cooled RF treatment
The ORs of ≥50% pain reduction after a cooled versus conventional RF treatment were 1.46 (95% CI 0.44 to 4.87), 2.38 (95% CI 0.60 to 9.38) and 2.7 (95% CI 0.69 to 10.55), respectively at 1, 3 and 6 months after treatment in the whole group, independent of the indication.
The differences between the proportion of patients with ≥50% pain reduction after an RF treatment (conventional and cooled combined) between OA and PPSP were also not statistically significant at each time point, although absolute numbers where at each time point higher in the OA group.
Secondary outcomes
Numerical Rating Scale
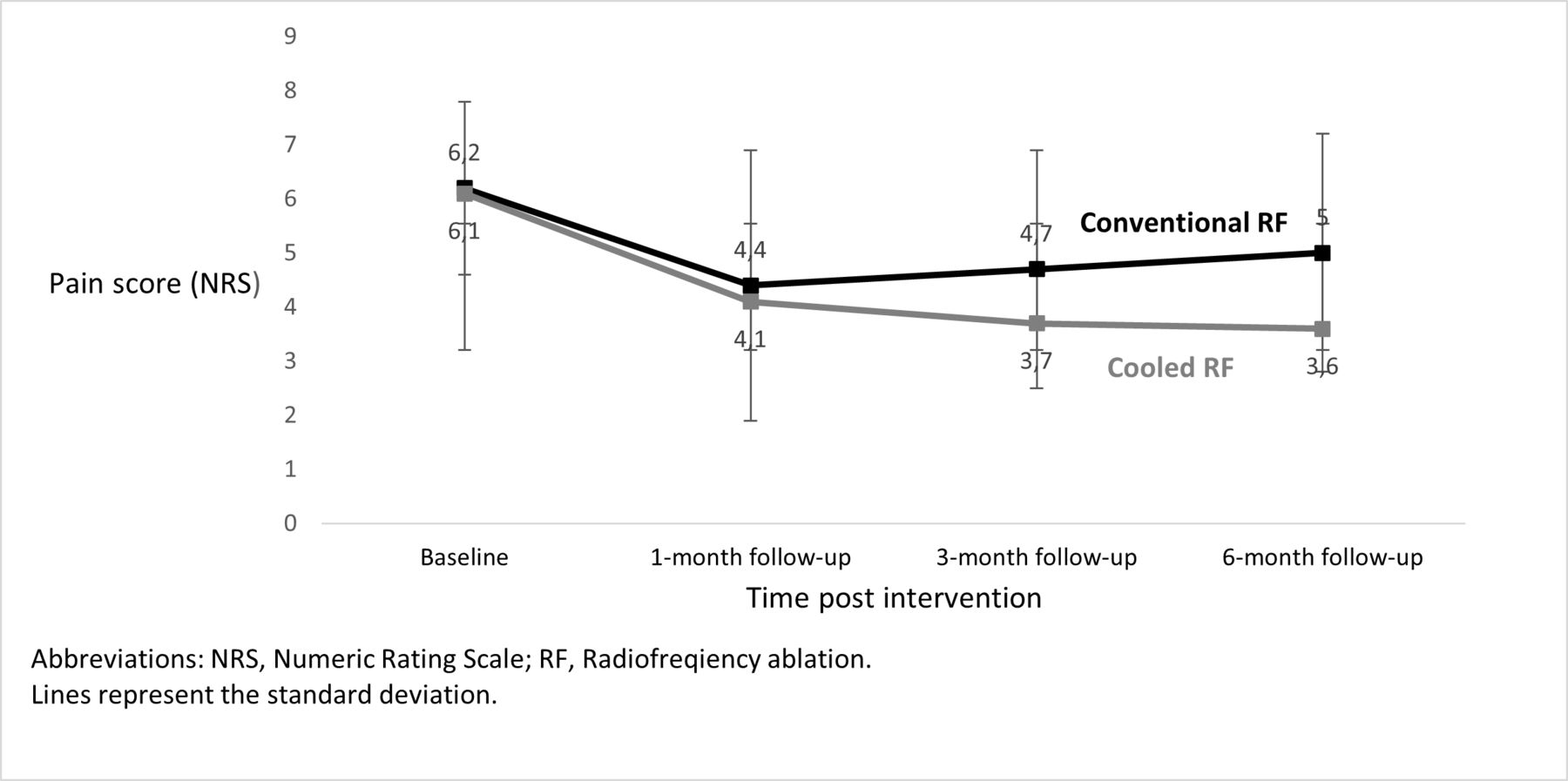
At each time point, the mean NRS score of the OA subgroup, PPSP subgroup and the whole population decreased in a statistically significant manner (p<0.05) compared with baseline after both conventional and cooled RF treatment (figure 2). The mean pain reduction (ΔNRS) (95% CI) at 3 months compared with baseline was –2.0 (−3.2 to −0.9) for OA, −2.0 (−2.8 to –1.1) for PPSP and −2.0 (−2.7 to −1.3) for the whole population. In patients treated with cooled RF, the mean pain reduction (ΔNRS) (95% CI) at 3 months compared with baseline was –2.2 (−4.2 to −0.1) for OA, −2.5 (−3.8 to –1.2) for PPSP and −2.3 (−3.5 to −1.2) for the whole population. In patients treated with conventional RF, the mean pain reduction (ΔNRS) (95% CI) at 3 months compared with baseline was –1.9 (−3.3 to −0.5) for OA, −1.5 (−2.6 to –0.3) for PPSP and −1.7 (−2.5 to −0.8) for the whole population. The mean ΔNRS of the OA and PPSP subgroup was statistically significant at each follow-up point compared with baseline, but the mean ΔNRS was not significantly different between the OA and PPSP subgroups at each follow-up moment. When analyzing both the OA an PPSP population together, at each follow-up point, the ΔNRS of cooled RF compared with baseline was not significantly different to the ΔNRS of conventional RF compared with baseline. There was, however, an increase of the ΔNRS over time in the whole cooled RF group compared with a decrease in the whole conventional RF group.

Mean NRS at each time point compared between conventional and cooled RF in the whole group.
The non-inferiority outcome
The non-inferiority comparison between conventional and cooled RF was performed on the combined OA and PPSP population due to the limited number of patients included in this trial. The point estimate difference in NRS was 1 at 3 months but as the 95% CI (−0.6 to 2.7) includes the non-inferiority margin of 0.75, it is inconclusive at this point (figure 3).

{kind=link}
{kind=link}
{kind=link}
Non-inferiority graphic. RF, radiofrequency ablation.
Patient’s Global Impression of Change, OKS, EQ-5D-3L, HADS, PCS, MQSIII, Goniometry, and TUG test.
Table 3 describes the evolution of the secondary outcomes at different time points compared between conventional and cooled RF treatment of the genicular nerves in the whole population.
The evolution of secondary outcomes at different time points compared between conventional and cooled RF treatment of the genicular nerves
Adverse events
There were no serious AE. There were no significant differences in prevalence of AE between conventional and cooled RF, respectively, 5 and 6 cases. After conventional RF, five patients reported a transient increase in pain. After cooled RF, three patients developed a subcutaneous hematoma which resolved spontaneously, one patient developed infrapatellar hypoesthesia, and two patients reported a transient increase in pain.
Blinding
Data from two participants were missing. Thirty-nine patients (83%) reported that they did not know which treatment they received. Five patients (11%) guessed the wrong allocation and three (6%) guessed right.
Discussion
As this is a pilot trial with inherent low statistical power, the primary goal was to estimate and compare the treatment effect size of conventional and cooled RF of the genicular nerves. This study showed that the proportion of patients with at least 50% pain reduction was higher, although not significantly, after a cooled RF treatment of the genicular nerves in comparison with a conventional RF treatment in patients with chronic knee pain due to OA, PPSP and the whole population at each time point up to 6 months after the procedure. Mainly, in the PPSP group cooled RF led to higher proportion of patients with ≥50% pain reduction in comparison with conventional RF. The differences were not statistically significant reflecting among others the insufficient sample size of this pilot trial. Despite this, we found a statistically significant pain reduction after both conventional and cooled RF treatment of the genicular nerves up to 6 months postprocedure. The point estimate of the difference in mean pain reduction from baseline between conventional and cooled RF at 3 months was one which could indicate inferiority of conventional RF, nevertheless, these results are inconclusive as the 95% CI included the non-inferiority margin of 0.75. At 6 months, the mean pain reduction of the patients treated with cooled RF was 2.5 point, which is above the clinically relevant margin of 2 points according to the IMMPACT guidelines. This was not the case with conventional RF. The proportion of patients with ≥50% pain reduction and the absolute pain reduction, although both higher in the OA group, did not differ statistically significant between OA or PPSP. Most secondary outcomes improved in time after both conventional and cooled RF. We found no statistically significant difference in secondary outcomes between both RF treatments. There were no serious AE reported, indicating that both RF modalities are safe. Results of the blinding analysis also indicate that the blinding process was adequate. In a large retrospective study by Kapural et al cooled RF also resulted in a higher chance of treatment success and a longer duration of effect in comparison with conventional RF in OA patients.27
When comparing the findings of this trial with the literature, we remark that treatment success in this study is lower. Earlier studies demonstrate treatment success (proportion ≥50% pain reduction) of a conventional RF between 32% and 59% at 3 months and after a cooled RF between 61% and 74% at 6 months.12 13 28 29 First, this difference could be explained by the fact that no prognostic block was used in this trial. We did not include a prognostic block as we considered that its possible benefit did not outweigh the risks. The possible benefit is a better patient selection and by this better treatment outcomes. However, the randomized controlled trial by McCormick et al showed that a prognostic block with 1 mL of local anesthetic and a 50% threshold did not lead to improved pain and knee function outcomes in comparison with not performing a prognostic block.13 At the moment, there are no prospective studies showing a better outcome with the use of prognostic genicular nerves blocks prior to RF. The main drawback of using prognostic blocks, is that patients with a false-negative block are refused a potentially safe and effective treatment. Furthermore, there are also other downsides and risks associated with the use of prognostic blocks such as an increased cost, patient discomfort and especially in the group of patients post-TKA the risk of infection. Moody et al reported two cases of patients with PPSP suffering a knee infection after a prognostic genicular nerve block.30 Also, there are other studies where investigators have decided to not perform a prognostic block.31–33 Second, most published studies include only OA patients, whereas in this study both OA and PPSP patients were included. To our knowledge, this is the first RCT that investigated the effects of cooled RF in PPSP patients. In operated patients, anatomy can be even more variable and causes of pain can be plural resulting in diminished treatment success. As this study found an effect size of the primary endpoint of 18.7% and 37.5%, respectively, for conventional and cooled RF at 6 months in the whole population, it is of utmost importance that future studies also include a sham procedure to evaluate the possible placebo effect.
The prevalence of knee OA is rising and subsequently also the prevalence of total knee replacement and that of PPSP after TKA. As these conditions have a high impact on the patients’ health-related quality of life and a high societal cost, there is a need for minimally invasive alternative treatments.27 As cooled RF is associated with a higher product cost it is important to determine not only its effectiveness but also the cost-effectiveness.34
This study has several limitations. First, as this is a pilot trial sample size is, inherent to the design, too low to draw conclusions. Nevertheless, as this is the first trial to directly compare conventional and cooled RF of the genicular nerves in an RCT, results remain important to guide future research. Second, there was no prognostic block used prior to the RF treatment in both OA and PPSP patients which could have influenced our results. Third, this study was designed to target only three genicular nerves. In the literature, there is an ongoing discussion on possible strategies to increase treatment success, for example, by targeting more nerves or targeting nerves at different locations as cadaveric studies demonstrate significant anatomical variability.35 36 Fonkoue et al performed a study that compared an injection of 5 vs 3 nerves with LA and steroid in OA patients with a follow-up of 12 months.37 They found in both groups a significant reduction in pain intensity but only a significant greater pain reduction in the group with 5 nerves 1-hour postoperative. All the other time points showed no significant difference. Furthermore, the study performed by Chen et al targeted four nerves with cooled RF and found that 71% of patients report ≥50% pain reduction at 6 months.38 These results are comparable (74.1% of patients reported ≥50% pain reduction) with the study of Davis et al with a similar design with the exception that they only targeted three genicular nerves.39 The retrospective analysis of Chen et al found that targeting more than three nerves increased treatment success (Global Perceived Effect >30%) from 57.5% (126/219) to 80% (36/45), although there are inherent limitations due to the retrospective design.40 The editorial of Kim and Cohen advocates that ablation of up to ten genicular nerves could improve outcomes of this treatment.36 However, this hypothesis is also based in ex vivo studies and prospective clinical trials on patients comparing the number of genicular nerves targeted are lacking. It is at this time unknown whether denervation of all nerves, which innervate the anterior knee, is necessary for adequate analgesia.36 On the other hand, increasing the number of lesions, also increase the risk of complications, therefore each intervention should be a balance between possible clinical benefits and risk of complications. At the time this study was conducted, most studies performed an RF treatment of the genicular nerves on three nerves. Nevertheless, targeting more than three nerves theoretically could lead to better outcomes and should be focus of future research.
Conclusions
In conclusion, both conventional and cooled RF of the genicular nerves reduced pain in the OA and PPSP population. The explorative results of this pilot study showed that a not statistically significant higher proportion of patient experienced ≥50% pain reduction from baseline after cooled RF compared with conventional RF. The non-inferiority analysis was inconclusive. Further research in the form of a powered comparative RCT is warranted.
Supplemental material
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval was granted from the ethical committees of Hospital Oost-Limburg (19/0038U) and Maastricht UMC+ (NL69877.068.19/METC 19-031). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors wish to thank Nelleke De Meij and Philma Beijers for their assistance in coordination and patient data gathering for the COCOGEN study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors have contributed substantially to the manuscript and agree with the content. Thibaut Vanneste acts as guarantor of overall content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.