Article Text

Statistics from Altmetric.com
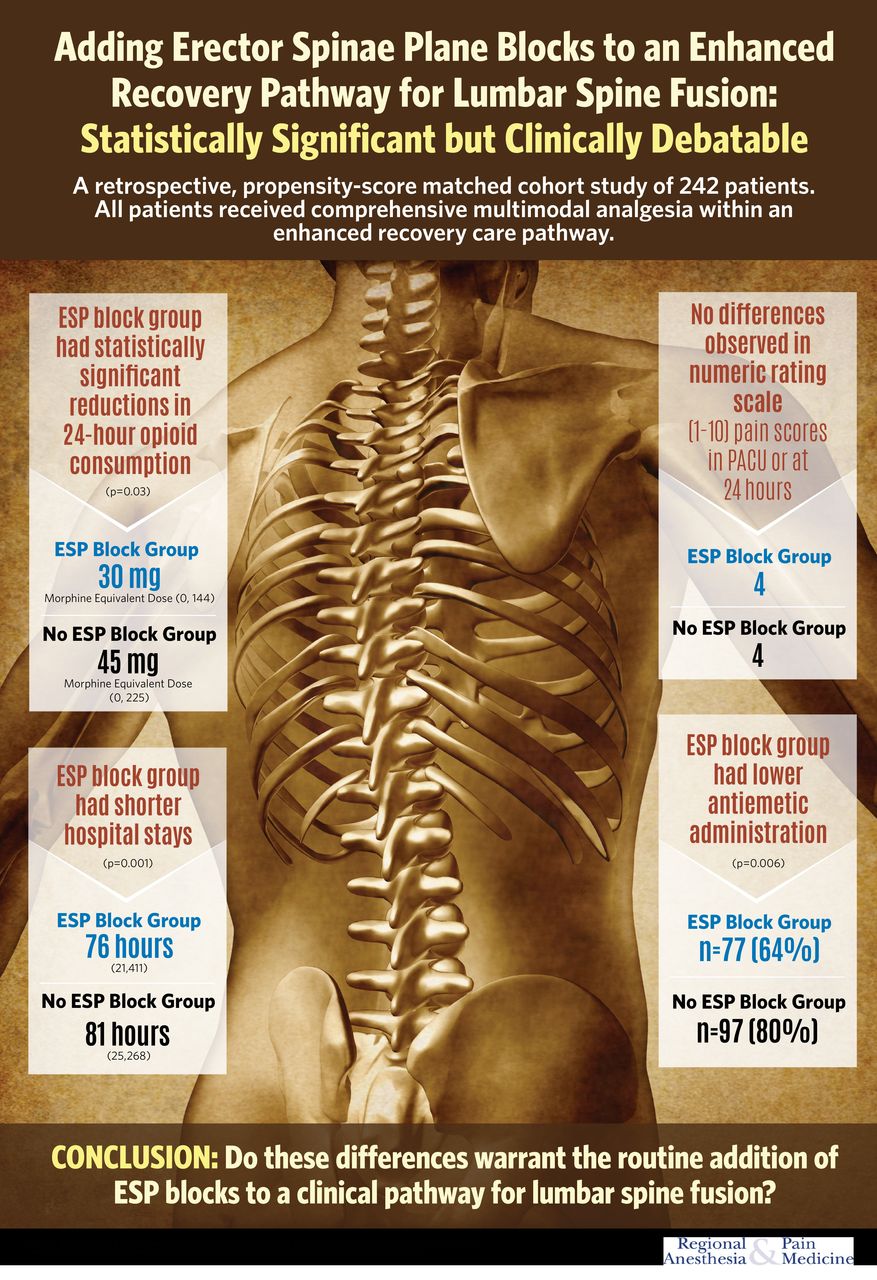
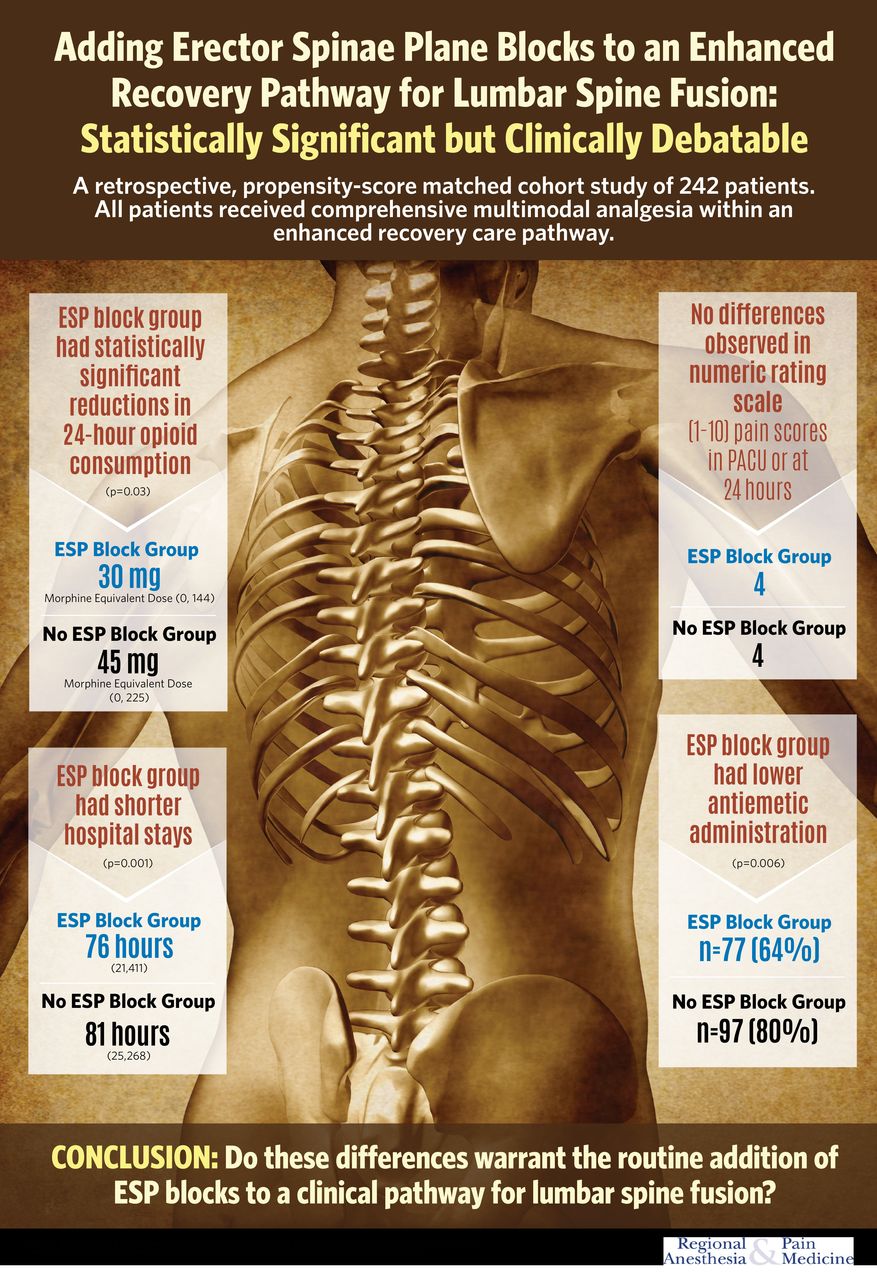
Erector spinae plane (ESP) blocks have been described as useful for multiple types of operations in recent years. Soffin et al explore the value of bilateral ultrasound-guided ESP blocks on pain and opioid-related outcomes when they are utilized in combination with a standardized multimodal analgesia care pathway for lumbar fusion.1 The authors used a retrospective propensity score-matched cohort study design to compare patients who did or did not receive ESP blocks. After matching, 242 patients were matched and compared. They did discover a significantly lower 24-hour opioid consumption in the ESP group (30 mg (0.144) vs 45 mg (0.225)). They did not note a significant difference in pain scores in the Post Anesthesia Care Unit (PACU) or on the floor. Length of stay was noted to be about 5 hours shorter in the block group, and fewer patients in the block group required postoperative antiemetics. However, the authors question whether the small reduction in morphine equivalent dose of opioids, the small change in length of stay and the small reduction in postoperative antiemetic use is clinically relevant enough to justify the added effort and risk of erector spinae blocks for lumbar spine surgery when a standard care pathway is employed.
{kind=link}
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Acknowledgments
We would like to acknowledge Jim Snively, artist, of Pittsburgh, PA, for graphic design of this infographic.
Reference
Footnotes
Twitter @dr_rajgupta, @ESoffin, @ESchwenkMD
Contributors All authors participated in preparation of this infographic, either with editing, design, or finalization.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests RKG and EMS are co-associate editors of Regional Anesthesia and Pain Medicine.
Provenance and peer review Commissioned; internally peer reviewed.