Article Text

Abstract
Background The reported prevalence of chronic pain after spinal cord injury (SCI) varies widely due, in part, to differences in the taxonomy of chronic pain. A widely used classification system is available to describe subcategories of chronic pain in SCI, but the prevalence of chronic pain in SCI based on this system is unknown.
Objective The primary objective of this systematic review and meta-analysis is to determine the prevalence of chronic pain after SCI based on the International Spinal Cord Injury Pain (ISCIP) classification system.
Evidence review A comprehensive search of databases from January 1980 to August 2019 was conducted. The risk of bias was assessed using a modified tool developed for uncontrolled studies. The Grading of Recommendations, Assessment, Development and Evaluation approach was used to assess certainty in prevalence estimates.
Findings A total of 1305 records were screened, and 37 studies met inclusion criteria. The pooled prevalence of overall chronic pain was 68% (95% CI 63% to 73%). The pooled prevalence of neuropathic pain in 13 studies was 58% (95% CI 49% to 68%); the pooled prevalence of musculoskeletal pain in 11 studies was 56% (95% CI 41% to 70%); the pooled prevalence of visceral pain in 8 studies was 20% (95% CI 11% to 29%) and the pooled prevalence of nociceptive pain in 2 studies was 45% (95% CI 13% to 78%). Meta-regression of risk of bias (p=0.20), traumatic versus non-traumatic etiology of injury (p=0.59), and studies where pain was a primary outcome (p=0.32) demonstrated that these factors were not significant moderators of heterogeneity. Certainty in prevalence estimates was judged to be low due to unexplained heterogeneity.
Conclusion This systematic review and meta-analysis extends the findings of previous studies by reporting the prevalence of chronic pain after SCI based on the ISCIP classification system, thereby reducing clinical heterogeneity in the reporting of pain prevalence related to SCI.
- chronic pain
- epidemiology
- neuralgia
Statistics from Altmetric.com
Introduction
Chronic pain after spinal cord injury (SCI) diminishes physical and psychosocial functioning.1 2 The reported prevalence of chronic pain after SCI varies considerably due, in part, to differences in the taxonomy of chronic pain.3 4 The International Spinal Cord Injury Pain (ISCIP) classification system is widely recognized and the first universal classification tool in SCI-related chronic pain, combining the International Association for the Study of Pain and Bryce-Ragnarsson taxonomies specific to SCI-related pain conditions.5–7 The ISCIP classification system is used internationally in research and clinical settings to categorize the complex symptom burden commonly presenting in patients with SCI,8–12 mitigating the considerable clinical heterogeneity that often complicates accurate and complete diagnosis and treatment of chronic pain in SCI. The ISCIP classification system organizes chronic pain hierarchically into three tiers. The first tier is comprised of four broad categories of chronic pain (neuropathic, nociceptive, other pain and unknown pain), the second tier is comprised of subcategories of neuropathic and nociceptive pain, and the third tier specifies the anatomical source of pain. The neuropathic pain second tier subcategories include at-level pain, below-level pain (occurring at least three levels below the level of injury) and other neuropathic pain diagnoses. Second tier subcategories of nociceptive pain include musculoskeletal, visceral and other nociceptive pain diagnoses. The ‘other’ pain and ‘unknown’ pain first tier categories do not have second tier subcategories. Examples of third tier sources of neuropathic pain include spinal cord or nerve root injury and syringomyelia. Tendinopathy, abdominal or genitourinary dysfunction, and pressure ulcerations are examples of nociceptive pain. Examples of third tier sources of other pain include complex regional pain syndrome and fibromyalgia, and no third tier sources of pain are identifiable for the unknown pain category.5 6
The prevalence of chronic pain after SCI based on the ISCIP classification system has not been previously reported. This is important because although the ISCIP classification system is widely used in research and data collection with respect to SCI-related pain, the prevalence of the subcategories of pain according to the ISCIP classification system is unknown. Detailed knowledge about the prevalence of SCI-related chronic pain could help investigators design appropriately powered clinical trials and enhance the accurate deployment of pain therapies based on the rate of anticipated need.13 14 Thus, the primary objective of this systematic review and meta-analysis is to determine the overall prevalence of chronic pain after SCI based on the ISCIP pain classification system.
Methods
Study protocol
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed,15 and an a priori protocol was followed. The review was registered in the PROSPERO database (CRD42020147090). The investigative process began after the protocol was submitted, but prior to completion of registration.
Search strategy
A comprehensive search of several databases from January 1, 1980 to August 20, 2019 was conducted. The databases included Ovid MEDLINE, MEDLINE Epub Ahead of Print, MEDLINE In-Process and Other Non-Indexed Citations, Daily, Ovid EMBASE, Ovid Cochrane Central Register of Controlled Trials, Ovid Cochrane Database of Systematic Reviews and Scopus. The search strategy was designed and conducted by an experienced librarian with input from the principle investigator. Language was restricted to English, and controlled vocabulary supplemented with keywords was used to search for studies of the prevalence of chronic pain in individuals with SCI. The actual strategy listing all search terms used and how they are combined is available in online supplemental appendix A.
Supplemental material
Eligibility criteria
Study inclusion criteria included (1) randomized-designed, crossover-designed and parallel-designed clinical trials; (2) prospective and retrospective longitudinal studies; (3) cross-sectional studies; (4) age 18 years or older; and (5) publication years 1980 to present. Exclusion criteria included (1) studies that involved adults with SCI without chronic pain; (2) studies that involved adults with SCI with pain of less than 3 months’ duration and (3) non-English-language studies.
The primary objective of the literature search was to determine the prevalence at time of injury, 1 year and lifetime prevalence of chronic pain in adults with SCI. The secondary objective was to determine the prevalence at time of injury, 1 year and lifetime prevalence of diagnostic subgroups of chronic pain in adults with SCI based on the ISCIP classification system.
Study selection process
Two independent pairs of reviewers screened all titles and abstracts included in the search results. These reviewers then screened full-text articles for inclusion and exclusion criteria, and the reason for exclusion of each full text was recorded.
Data extraction
Four reviewers abstracted data from the full-text articles using a templated computer database. Based on the a priori protocol, abstracted data included study design, sample size, cohort demographics (eg, mean age, sex), traumatic versus non-traumatic cause of SCI, level of injury, completeness of injury and years since SCI. The ISCIP criteria for chronic neuropathic, nociceptive, other pain and unknown pain were applied to studies that reported sufficient details about specific types of chronic pain.
Risk of bias assessment
The risk of bias was assessed using a tool specifically designed for assessing bias in uncontrolled studies.16 This tool consisted of four questions: (1) Do(es) the patient(s) represent the whole experience of the investigator (center) or is the selection method unclear to the extent that other patients with similar presentation may not have been reported? (2) Was the exposure adequately ascertained? (3) Was the outcome adequately ascertained? (4) Is the case(s) described with sufficient details to allow other investigators to replicate the research or to allow practitioners make inferences related to their own practice? The risk of bias was reported for each of four questions relating to selection, ascertainment and reporting for each study. Reviewer discrepancy was resolved by consensus or by a third reviewer.
Evidence synthesis
When reported, the overall prevalence of chronic pain and prevalence of chronic pain based on the ISCIP classification system were reported for each study. Results were pooled with random-effects models using the DerSimonian and Laird method and were reported with 95% CIs. Meta-regression with a mixed-effects model was selected to investigate potential moderators of heterogeneity. Statistical analyses were performed using R V.3.5.0 (R Core Team, 2018).
We investigated several potential moderators of heterogeneity including etiology of injury (traumatic or non-traumatic), risk of bias and pain as the primary outcome by performing meta-regression with subgroup analysis. The third characteristic was based on van Gorp et al’s findings in a previously published systematic review.4
Certainty in prevalence estimates
The GRADE approach (Grading of Recommendations, Assessment, Development and Evaluation)17 is a comprehensive and transparent process of evaluating the certainty of evidence (previously called quality of evidence) in interventional and diagnostic systematic reviews. The approach has been extended to prevalence studies. We applied GRADE domains of risk of bias, inconsistency or heterogeneity, indirectness, publication bias and imprecision.18 We considered studies with a small sample size (under 1000) to provide imprecise prevalence estimates and wide CIs.
Results
Characteristics of included studies
The PRISMA flow diagram of the study selection process is depicted in figure 1. Thirty-seven studies met inclusion and exclusion criteria (table 1).19–55 The survey conducted by Warms et al53 included two separate cohorts, and the results are presented separately as v1 and v2. When studies included multiple follow-up time points, the results reported for the longest follow-up time point were recorded. Despite our stated outcome of reporting pain prevalence at 1 year following injury, due to inconsistency in reporting of time points of pain following initial injury, we were unable to reliably aggregate 1-year pain prevalence across studies. Thirty-four studies used a cross-sectional design19–21 23–29 31 33–55 and four studies used a prospective cohort design.22 30 32 54 Mixed cohorts of traumatic and non-traumatic causes of SCI were used in 25 studies19 20 22–24 26–29 31 33–36 40 41 43–46 49 51–53 55 and traumatic only cohorts were used in 12 studies.21 25 30 32 37–39 42 47 48 50 54 Although most studies reported the proportion of their population who had sustained a traumatic injury, those with a mixed cohort did not separately report the prevalence of pain in subjects who had sustained traumatic versus non-traumatic injuries. Among the 34 studies reporting level of injury,19–40 42 43 45–47 49–55 3589 patients were tetraplegic and 7048 were paraplegic. Table 2 summarizes the number of patients with each subcategory of pain according to ISCIP criteria.
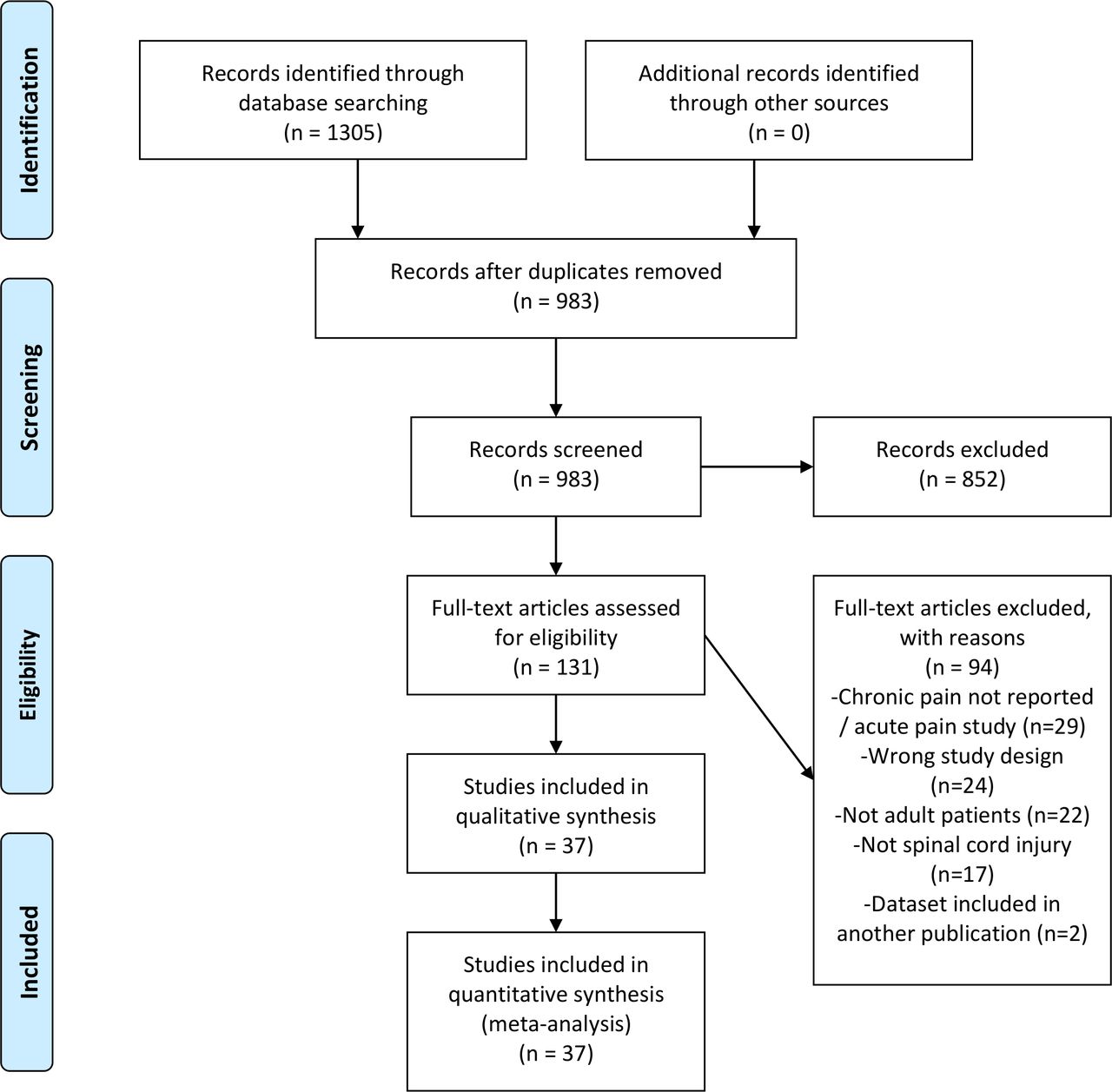
Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram of study selection process. Adapted from: Moher et al.15
Studies reporting prevalence of chronic pain in spinal cord injury (SCI)
Categories of reported pain according to ISCIP classification criteria
Table 3 summarizes the results including quality assessment according to GRADE criteria, pooled prevalence estimates and certainty in the estimates based on GRADE analysis. Certainty across all pain categories and subtypes is rated as low to very low due to inconsistency resulting from unexplained statistical heterogeneity.
GRADE analysis including quality assessment, summary of findings and certainty in estimates of prevalence of chronic pain in spinal cord injury
Risk of bias assessment
The risk of bias summary and the entire risk assessment is contained in online supplemental appendix B. Common sources of bias included selection bias in 27% (N=10) of studies, ascertainment of outcome in 19% (N=7) of studies and ascertainment of exposure in 16% (N=6) of studies. To investigate risk of bias as a source of heterogeneity, we performed subgroup analysis based on whether risk of bias was judged to be high (based on a cut-off of ‘no’ to two of our questions) (online supplemental appendix C). Seven studies were deemed to have a high risk of bias.23 26 28–31 40 The prevalence of pain in these seven studies ranged from 44% to 77%. The pooled prevalence of pain among studies with high risk of bias was 62% (95% CI 51% to 73%) with high heterogeneity (I2=94%). The pooled prevalence of pain among studies with low risk of bias was 69% (95% CI 64% to 74%) with high heterogeneity (I2=97%). Risk of bias was not found to be a significant moderator of heterogeneity.
Supplemental material
Supplemental material
Prevalence of all chronic pain types
All 37 studies (n=11 351) reported chronic pain prevalence and the prevalence of all chronic pain types ranged from 33% to 100% (figure 2). The pooled prevalence of all chronic pain types was 68% (95% CI 63% to 73%) with high heterogeneity (I2=97%).
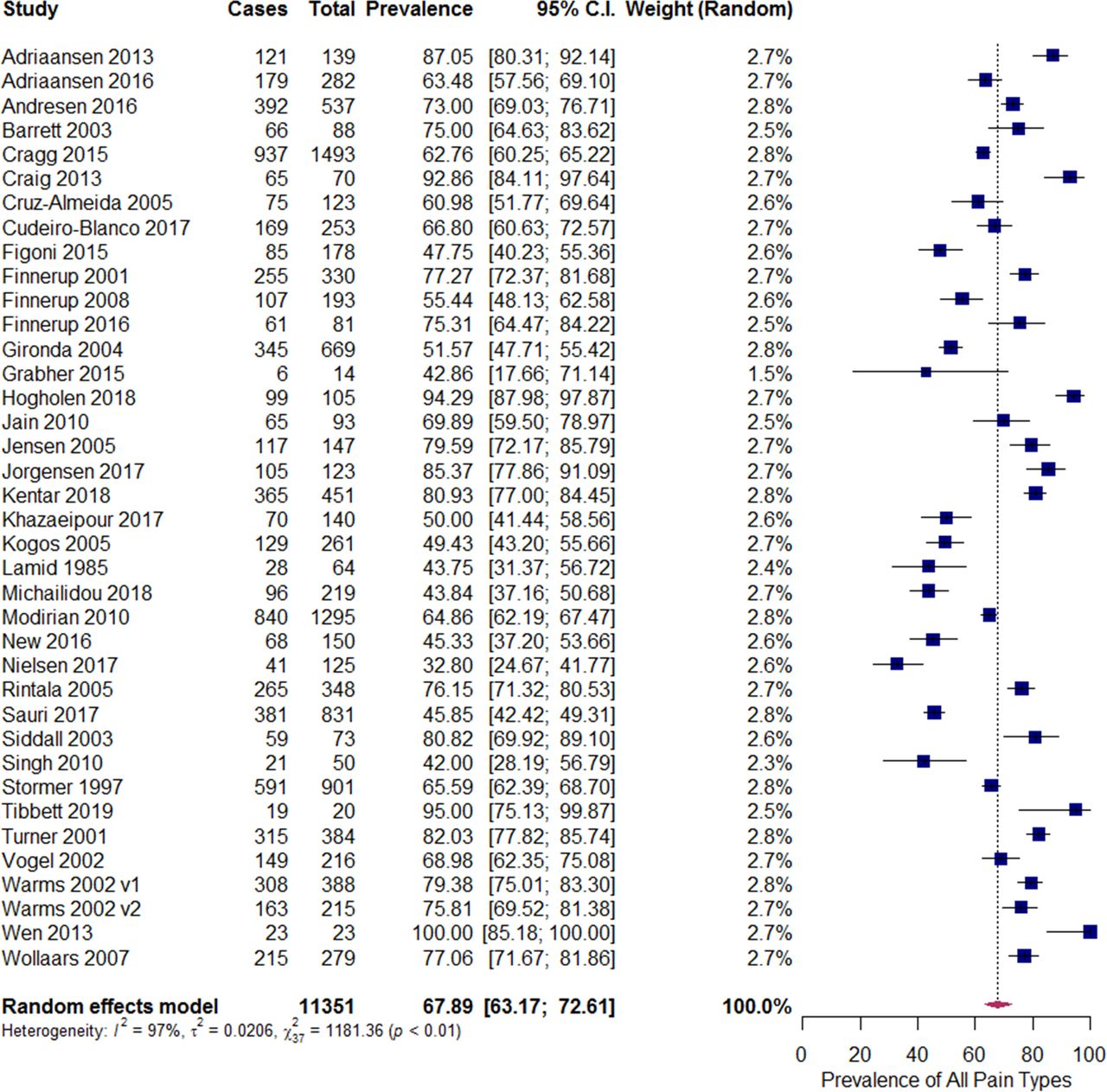
Pooled prevalence of chronic pain in spinal cord injury, all pain types.
Meta-regression performed with individual covariates including risk of bias (p=0.20), traumatic versus non-traumatic amputation (p=0.59), and studies where SCI pain was a primary outcome (p=0.32) demonstrated that these individual factors were not significant moderators of heterogeneity. Meta-regression with these three factors combined as a single covariate resulted in significant residual heterogeneity signifying that this combined factor was not a significant moderator of heterogeneity (p=0.44). The results of this meta-regression can be viewed in online supplemental appendix C.
Prevalence of chronic pain based on subgroup analyses of ISCIP categories
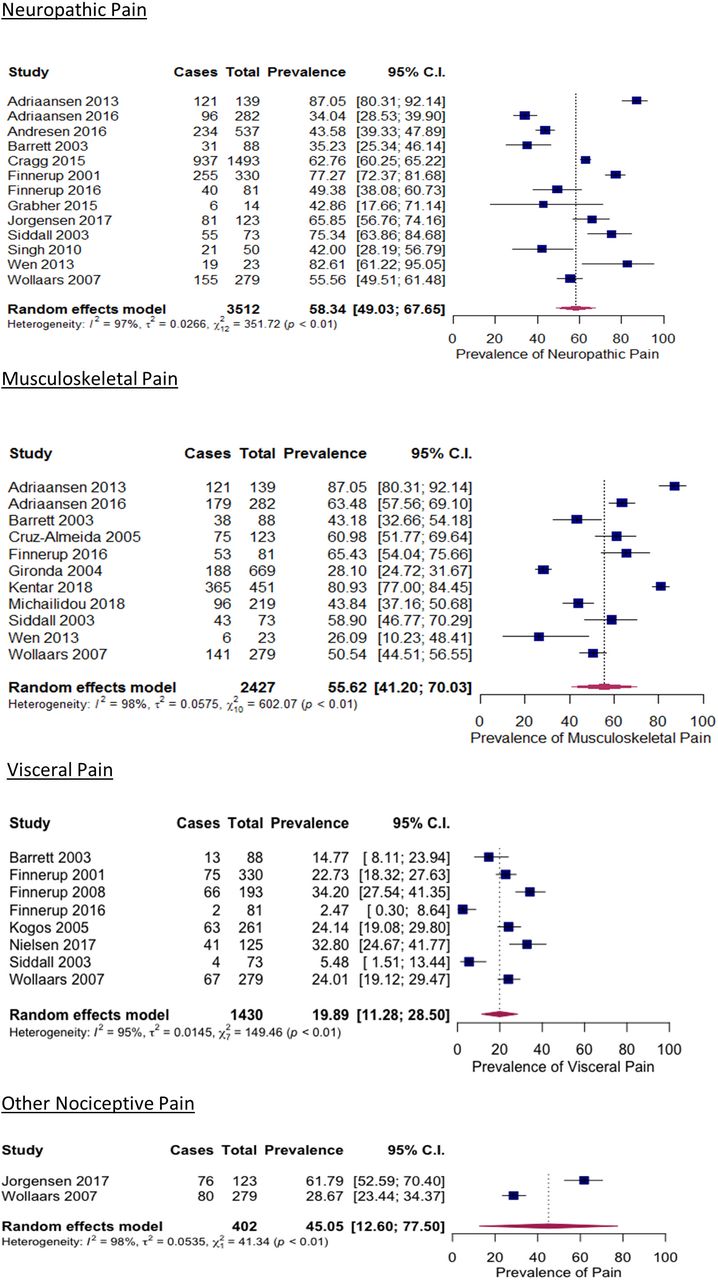
Twenty of 37 studies reported chronic pain that could be classified using the ISCIP classification system. The prevalence of chronic neuropathic pain in 13 studies (n=3512) ranged from 34% to 83% (figure 3). The pooled prevalence of neuropathic pain was 58% (95% CI 49% to 68%) with high heterogeneity (I2=97%). Inadequate data were available to further subclassify neuropathic pain as at-level or below-level, and other neuropathic pain diagnoses were not reported.

{kind=link}
{kind=link}
{kind=link}
Pooled prevalence of chronic pain in spinal cord injury, subgroup analysis based on ISCIP categories. ISCIP, International Spinal Cord Injury Pain.
The prevalence of chronic nociceptive musculoskeletal pain in 11 studies (n=2427) ranged from 26% to 87% (figure 3). The pooled prevalence of musculoskeletal pain was 56% (95% CI 41% to 70%) with high heterogeneity (I2=98%).
The prevalence of chronic visceral pain in eight studies ranged from 2% to 34% (figure 3). The pooled prevalence of chronic visceral pain was 20% (95% CI 11% to 29%) with high heterogeneity (I2=95%).
The prevalence of other chronic nociceptive pain in two studies ranged from 29% to 62% (figure 3). The pooled prevalence of other chronic nociceptive pain was 45% (95% CI 13% to 78%) with high heterogeneity (I2=98%).
The occurrence of unknown pain was not reported in any study.
Prevalence of all chronic pain types in traumatic injuries
To assess for possible sources of heterogeneity, we performed subgroup analysis based on etiology of injury (traumatic vs non-traumatic). Twelve21 25 30 32 37–39 42 47 48 50 54 of 37 studies included only subjects with traumatic injuries. The prevalence of pain in these 12 studies ranged from 42% to 100%. The pooled prevalence of pain among studies of patients with traumatic injuries was 69% (95% CI 60% to 78%) with high heterogeneity (I2=96%). Etiology of injury was not found to be a significant moderator of heterogeneity.
Certainty of prevalence estimates
Using the GRADE approach, the certainty in the prevalence estimates is judged to be low, primarily due to the high degree of heterogeneity (inconsistency). Performance of subgroup analysis according to pain category mitigated indirectness derived from differences in patient population. Given the variety of included study design and study design, we did not downgrade quality of evidence based on publication bias.
Discussion
The main finding of this systematic review and meta-analysis was that the pooled prevalence of SCI-related chronic pain type overall was 68%. When the meta-analysis was performed for each ISCIP category, the prevalence rates of chronic neuropathic pain and musculoskeletal pain were 58% and 56%, respectively. The prevalence of other chronic pain was 45%, and the prevalence of visceral pain was the lowest at 20%.
This is the first time that a systematic review has evaluated prevalence of chronic pain according to all categories of SCI-related pain, using the widely accepted ISCIP criteria. The overall prevalence of chronic pain after SCI in this review is consistent with the findings of previous systematic reviews.
At least two previous systematic reviews have reported the prevalence of chronic pain based on two of the subcategories. The prevalence of chronic neuropathic pain was reported in a systematic review that involved 17 studies.56 Criteria for study inclusion required evidence that a working definition of neuropathic pain was used which encompassed use of the ISCIP classification system. The overall point prevalence of neuropathic pain was 53% (95% CI 39% to 67%).56 The 58% prevalence of neuropathic pain reported in our study is within the 95% CI of the Burke et al study.56 For the ISCIP subcategories of at-level and below-level neuropathic pain, the prevalence rates were 19% (95% CI 13% to 26%) and 27% (95% CI 20% to 35%), respectively. High levels of heterogeneity (I2=84%–93%) were reported for all prevalence calculations.56 In a separate systematic review that involved eight studies, the prevalence of chronic musculoskeletal pain was 49% (95% CI 44% to 55%).57 The prevalence of chronic back pain was 47% (95% CI 43% to 50%) and the prevalence of chronic low back pain was 49% (95% CI 44% to 55%).57 The type of back and low back pain could not be further differentiated due to insufficient evidence.57 These prevalence rates are lower than the 56% prevalence identified herein, but our review included information from an additional five studies.
Assessment of heterogeneity
All pooled prevalence rates were confounded by high levels of heterogeneity. Despite use of subgroup and meta-regression analyses, which are recommended approaches for identifying sources of heterogeneity,58 59 high levels of heterogeneity remained unexplained. High levels of heterogeneity have been reported in systematic reviews of prevalence studies.60 Although a computational analysis of the I2 statistic is beyond the scope of this review, it may be described as a measure of inconsistency among included studies, and not necessarily as a threshold tool for conduction of meta-analysis. The value of I2 increases with the number of subjects in the studies comprising the meta-analysis.61 62 If the underlying eligibility criteria are considered to be sound, restricting studies based on statistical heterogeneity introduces bias. The decision to conduct a meta-analysis should not be solely based on the I2 statistic; rather, the decision to pool studies should also incorporate an assessment of other relevant sources of heterogeneity.62 Other potential sources of heterogeneity were considered but inadequate data were available to conduct subgroup analyses based on pain intensity, temporal changes in pain, cervical versus lumbar SCI or duration of injury.
Other systematic reviews of SCI-related pain prevalence have also found high degrees of statistical heterogeneity. The primary aim of a systematic review that involved 82 studies was to identify sources of heterogeneity in pain prevalence studies.4 In this particular review, the precision of clinical criteria used to diagnose chronic pain (mild, moderate or high) was reported to be an important source of heterogeneity. Another reported source of heterogeneity included whether a study was primarily focused on pain; the prevalence of chronic pain was 14%–25% higher in studies that had a primary pain focus. The higher prevalence among pain-focused studies was postulated to be due to (1) selection bias (patients without pain less likely to participate); (2) publication bias (studies reporting high prevalence rates more likely to be published) and (3) higher sensitivity of diagnostic tools in pain-focused studies.4 In a second systematic review that involved 42 studies, the prevalence of chronic pain ranged from 26% to 96%.3 Although a formal meta-analysis was not performed due to high levels of heterogeneity, the mean prevalence rate was reported to be 62%.3 In both reviews,3 4 the use of uniform research methods for conducting prevalence studies of SCI pain was recommended as an approach to reduce heterogeneity in future studies. Although improved methodological heterogeneity will not necessarily improve the I2 statistic, this is a laudable goal for conduction of further prevalence studies.
Based on the finding that whether a study’s primary focus was on pain was a significant moderator of heterogeneity, we also performed subgroup analysis based on this characteristic. Thirty-two20–25 28–31 34–45 47–55 63 of 37 studies had a primary pain focus. The prevalence of pain in these 32 studies ranged from 33% to 100%. The pooled prevalence of pain in pain-focused studies was 68% (95% CI 63% to 73%) with high heterogeneity (I2=97%). Pain as the primary study focus was not found to be a significant moderator of heterogeneity.
In summary, we have reported the I2 statistic as a measure of statistical heterogeneity, which was high across all subgroups as has been observed in other systematic review of prevalence studies. Three study design characteristics including risk of bias, etiology of injury and whether pain was the primary focus of the study were all considered, and none were found to be significant moderators of statistical heterogeneity. Other systematic reviews have highlighted the importance of methodological heterogeneity as contributing to variability across studies. We have endeavored to address the problem of clinical heterogeneity through study design stratifying chronic SCI-related pain according to type of pain as defined by the ISCIP categories.
Limitations
This systematic review has limitations. By restricting our search to English language only, we may have excluded prevalence studies relevant to our objective. This introduces intrinsic bias to our results against manuscripts not published in English. There is also the question of appropriateness of meta-analysis given the statistical heterogeneity of the data. Although our preceding discussion addressed our rationale for conducting meta-analysis despite high levels of statistical heterogeneity in the meta-regression, there is a reasonable argument to be made that qualitative analysis would be sufficient for presentation of results. Given the known high degrees of statistical heterogeneity among prevalence studies in general, we felt that proceeding with meta-analysis was reasonable given the reported data among the identified studies. We felt that our results were sufficiently comparable to justify calculation of pooled prevalence of chronic SCI-related pain stratified according to the ISCIP categories, thereby decreasing the problem of clinical heterogeneity among this complex patient population.
Conclusion
This systematic review and meta-analysis extends the findings of previous studies by reporting the prevalence of chronic pain after SCI based on the ISCIP classification system. Pain is common after SCI and ongoing population-based prevalence studies using the ISCIP classification system are needed to accurately determine the prevalence of chronic pain in this important patient population.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @RajMoman
Contributors All authors have made substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data; and have participated in drafting the work or revising it critically for important intellectual content. All have submitted final approval of the version published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplemental information.