Article Text

Statistics from Altmetric.com
Introduction
During the first wave of the COVID-19 pandemic in the USA (March and April 2020) various organizations—including the American Academy of Orthopaedic Surgeons1—provided guidance on postponement or cancelation of elective and non-urgent surgeries to conserve healthcare resources. However, as these guidelines left the interpretation of “elective” and “non-urgent” largely to local healthcare delivery systems, it remains unknown how elective orthopedic surgeries and outcomes were affected.
We hypothesized that patients undergoing elective orthopedic surgery during the COVID-19 outbreak (compared with the previous year) would differ in terms of patient outcomes, specifically 30-day readmission given restraint healthcare resources during the COVID-19 outbreak.
Methods
We retrospectively analyzed patients captured in the Premier Healthcare database who underwent common elective orthopedic procedures during March and April of 2019 (“pre-COVID-19”) and 2020 (during the first COVID-19 wave in the USA). Premier Healthcare Database is a Health Insurance Portability and Accountability Act (HIPAA)-compliant administrative database providing information from over 700 US hospitals with comprehensive billing, cost, device, medication, and procedure information. Premier Healthcare Database is the largest acute care database in the USA, accounting for 20% of inpatient discharges. Procedures included foot and ankle surgery, primary and revision total hip arthroplasty or total knee arthroplasty, laminectomy, spine fusion, and shoulder and elbow arthroplasty (see online supplemental appendix 1 for definitions). Of note, we appreciate that revision surgery may be classified as elective or non-elective based on the indication; we only focused on surgeries labeled as elective in this dataset.
Supplemental material
Our primary outcome of interest was 30-day hospital readmission. Other outcomes included intensive care unit (ICU) admission, length of ICU (and hospital), length of stay (LOS), use of invasive ventilation, composite complication (online supplemental appendix 2) and in-hospital mortality. Covariates of interests included age, sex, race, comorbidity burden as measured by the Charlson-Deyo index,2 hospital location, bed size, teaching status, region, hospital LOS, and discharge disposition.
Supplemental material
Wilcoxon rank-sum tests and χ2 tests were applied as well as a multivariable logistic regression measuring the association between year and specifically 30-day readmission while adjusting for covariates. Covariates in the model were a priori determined based on clinical relevance; here, hospital LOS was treated as both an outcome in univariable comparisons as well as a covariate in our multivariable model with 30-day readmission. ORs and 95% CIs were reported. A p value <0.05 was determined as statistically significant.
Results
Overall, 38,741 and 12,245 elective orthopedic surgeries were included reflecting March/April 2019 and 2020, respectively. Compared to 2019, procedures in the March/April 2020 period reflected somewhat younger, more frequently women, non-white, and more comorbid patients while they were more commonly performed in teaching and larger hospitals. The distribution of surgeries performed in different regions was relatively skewed during the COVID-19 outbreak as the percentage of cases performed in the south increased, while percentage of cases done in other regions remained relatively stable, which may reflect the degree of spread of the first wave of COVID-19 in different parts of the country (table 1).
Patient and healthcare characteristics before and during COVID-19
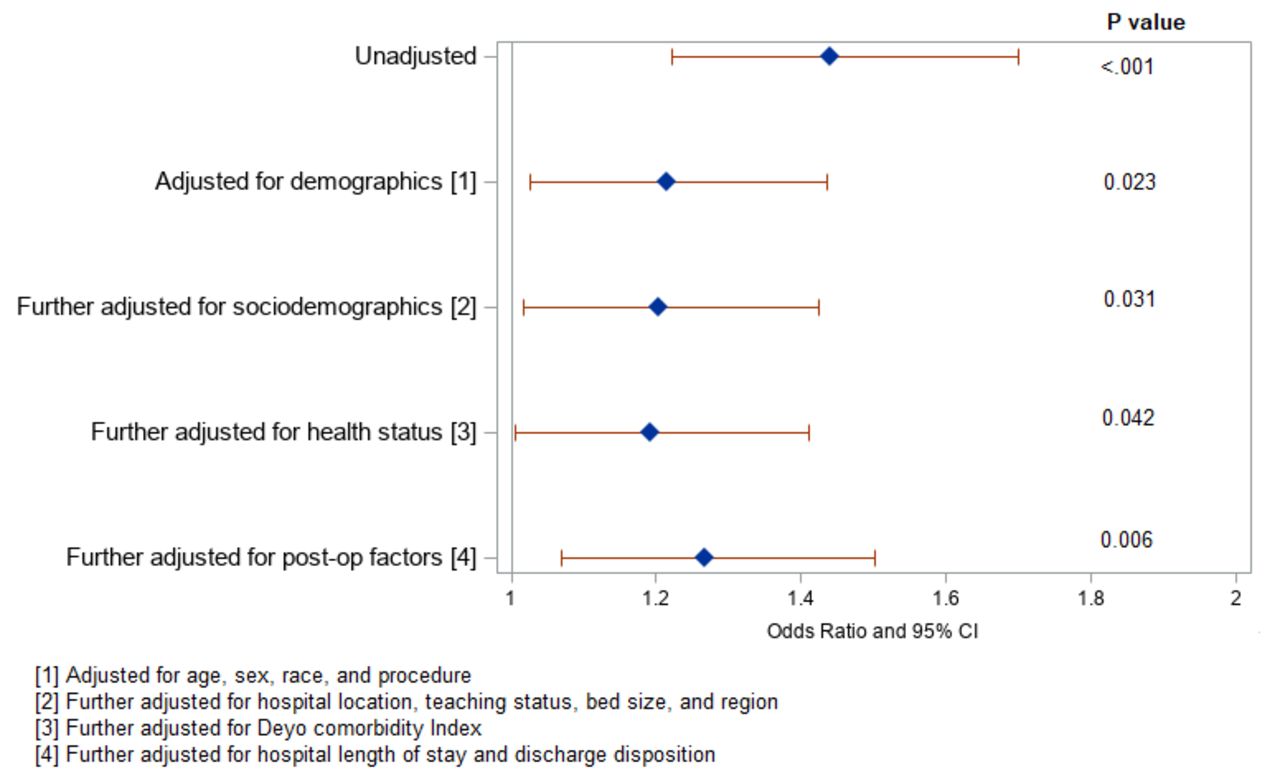
The crude readmission rate increased from 1.2% in 2019 to 1.7% in 2020. After adjustment for relevant covariates, there was 27% increase in the likelihood of readmission during COVID-19 period (adjusted OR: 1.27, 95% CI 1.07 to 1.5, p=0.006) (figure 1).
{kind=link}
ORs for the associations between time (during COIVD-19 vs pre-COVID-19) and 30-day readmission.
Further, patients were more frequently admitted to ICU (crude rate 2.7% in 2019 vs 3.4% in 2020, p<0.001), discharged home (crude rate 84.3% in 2019 vs 87.8% in 2020, p<0.001), experienced higher composite complication rates (crude rate 4.8% in 2019 vs 5.5% in 2020, p=0.002), and had higher cost (median (IQR): 16,686 (13,237, 23,181) in 2019 vs 18,441 (13,655, 27,040) in 2020, p<0.001) during the COVID-19 period. There were no significant group differences in terms of mechanical ventilation use, and ICU LOS (table 2).
Secondary patient outcomes before and during COVID-19
Discussion
In this analysis, patients admitted for elective orthopedic surgery during the COVID-19 period were younger, with higher comorbidity burden, and more likely re-admitted within 30 days of discharge (in the presence of a somewhat higher home discharge rate), compared with the same time period in the previous year.
These observations bring up various questions, including those related to elective hospital stays and subsequent COVID-19 exposure risks and related ethical concerns about performing elective surgery during a time with limited resources, especially if they are associated with worse outcomes. While younger patients are less likely to require ICU admission and/or mechanical ventilation,3 their initial prioritization for surgery during the COVID-19 period makes intuitive sense. However, a higher hospital readmission rate was noticed among this younger patient cohort during the COVID-19 period after controlling for sociodemographic factors, health status, and postoperative factors. It is possible that medical or staff resources were strained during the COVID-19 period and treatment might have been hindered.4 Additionally, risks of COVID-19 transmission during institutionalized care were likely to be weighed carefully against risks of suboptimal rehabilitation (which may in turn have led to higher readmission risks) at home. The presence of higher readmission risks in 2020 alongside somewhat higher home discharge suggests that this mechanism may have played a role in our observations.
Importantly, we were not able to identify “hotspots” during the COVID-19 period given the missing granularity of geographic data. Additionally, the Premier dataset does not yet contain long-term follow-up information of the COVID-19 cohort. Finally, there may be an underestimate of readmission rate, as our data were limited to readmissions to Premier hospitals only. Without being able to draw causal inferences from our data further research is warranted.
In conclusion, despite younger patients being prioritized for elective surgery during the COVID-19 period of March/April 2020, patient outcomes were worse. This questions the decision to perform elective orthopedic surgeries during pandemic without first understanding the drivers for these outcomes.
Ethics statements
Ethics approval
This study was approved by Institutional Review Board (IRB#2016-436).
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @jashvant_p, @jbLiujb, @sites_brian, @sgmemtsoudis
Correction notice This article has been corrected since it published Online First. The author order and affiliations have been updated.
Contributors HZ: this author helped in study design/planning, data analysis, interpretation of results, manuscript preparation, and review. LAW: this author helped in study design/planning, data analysis, interpretation of results, manuscript preparation, and review. JL: this author helped in study design/planning, interpretation of results, and manuscript review. JP: this author helped in study design/planning, interpretation of results, manuscript preparation, and review. BDS: this author helped in study design/planning, interpretation of results, manuscript preparation, and review. SGM: this author helped in study design/planning, interpretation of results, manuscript preparation, and review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.