Article Text

Abstract
Objective To investigate the cost-effectiveness of exercise therapy in the treatment of patients with non-specific neck pain and low back pain.
Design Systematic review of economic evaluations.
Data sources The search was performed in 5 clinical and 3 economic electronic databases.
Eligibility criteria for selecting studies We included economic evaluations performed alongside randomised controlled trials. Differences in costs and effects were pooled in a meta-analysis, if possible, and incremental cost-utility ratios (ICUR) were descriptively analysed.
Results Twenty-two studies were included. On average, exercise therapy was associated with lower costs and larger effects for quality-adjusted life-year (QALY) in comparison with usual care for subacute and chronic low back pain from a healthcare perspective (based on ICUR). Exercise therapy had similar costs and effect for QALY in comparison with other interventions for neck pain from a societal perspective, and subacute and chronic low back pain from a healthcare perspective. There was limited or inconsistent evidence on the cost-effectiveness of exercise therapy compared with usual care for neck pain and acute low back pain, other interventions for acute low back pain and different types of exercise therapy for neck pain and low back pain.
Conclusions Exercise therapy seems to be cost-effective compared with usual care for subacute and chronic low back pain. Exercise therapy was not (more) cost-effective compared with other interventions for neck pain and low back pain. The cost-utility estimates are rather uncertain, indicating that more economic evaluations are needed.
Registration PROSPERO, CRD42017059025.
- rehabilitation
- systematic review
- exercise
- lower back
- neck
Statistics from Altmetric.com
Background
Neck pain and low back pain are common conditions, associated with high levels of disability, absenteeism and high socioeconomic costs.1–5 Neck pain and low back pain are leading causes of years lived with disability.3 Total annual expenses related to low back pain alone in the UK are about £12 billion, and in the USA indirect costs are US$7.4 billion.6 In the Netherlands, total annual societal costs of neck pain were estimated at US$686 million.7
As neck pain and low back pain are important global health problems, there is a need to consider the effectiveness of treatments for improving symptoms. Clinical practice guidelines recommend exercise therapy in the treatment of patients with neck pain and low back pain.8–11 Exercise therapy may reduce pain and increase flexibility, strength, endurance and cardiovascular conditioning.12–15
Given limited financial resources, knowledge regarding the relative efficiency of treatments would help decision makers prioritise resources. Economic evaluations, in which the incremental effects and incremental costs of two or more interventions are compared,16 can inform resource decision-making. The European Union’s ‘Research Agenda for Health Economic Evaluation’ (RAHEE) project examined evidence gaps about the cost-effectiveness of treatments for the 10 highest burden conditions in Europe.17 18 The RAHEE project identified the need for further high-quality economic evaluations about cost-effectiveness of exercise therapy for patients with neck pain and low back pain due to the lack of evidence.17 18 Therefore, the present study aimed to analyse current evidence to identify if exercise therapy is a cost-effective treatment for non-specific neck pain and low back pain.
Methods
Inclusion criteria
We included economic evaluations (including cost-effectiveness, cost-utility, cost-minimisation and cost-benefit analysis) performed alongside randomised controlled trials. Patients with non-specific neck pain (ie, pain in the cervical region, with or without radiation to the shoulder region or upper extremities, including whiplash disorders)19 and low back pain (ie, pain in the region between the costal margins and the inferior gluteal fold, with or without radiation to the lower extremities)20 21 were included. Studies including multiple pain locations without separately reporting results for neck pain and low back pain were excluded.
We considered any type of exercise therapy (eg, strengthening, endurance, aerobic, stretching, stabilisation, coordination, functional and neuromuscular exercises) performed individually or in a group. The exercise therapy could be supervised or unsupervised. Studies evaluating exercise therapy combined with other treatments were excluded unless exercise therapy was evaluated separately or was the main treatment. The comparator was no treatment, usual care, other types of intervention (manual therapy, physiotherapy, cognitive behavioural approach) and different types of exercise.
The primary outcome was the incremental cost-utility ratio (ie, cost per quality-adjusted life-year (QALY)) and the secondary outcomes were incremental cost-effectiveness ratios including any type of clinically relevant outcome measure reported in the studies (eg, pain intensity, disability, global perceived effect/recovery). We also included studies that measured effects and costs, but did not calculate an incremental cost-effectiveness ratio.
Search methods
The search was conducted in the following electronic databases: PUBMED, EMBASE, CINAHL, Cochrane Central Register of Controlled Trials, PEDro, EconLit, British National Health Services Economic Evaluation Database (NHSEED) and HTA. Thus, the protocol of this study registered previously (PROSPERO registration: CRD42017059025) was slightly modified. The clinical database CINAHL and the economic database HTA were added to the search strategy, and the economic database EURONHEED was excluded because it is not updated anymore. The electronic search terms were derived from the search strategies of the Cochrane Back and Neck Group22 and NHSEED.23 The complete EMBASE search strategy is presented in online supplementary appendix 1. We searched all databases from inception to 12 April 2017. In addition to the electronic search, we searched reference lists of relevant systematic reviews and included studies.
Supplementary file 1
Data collection
Selection of studies
Two reviewers (GCM and MvT) independently conducted the study selection process, first considering title and abstract, and then the full paper. Disagreements between reviewers were resolved first by discussion and then by arbitration of a third reviewer (JvD), if disagreements persisted. We included only full-text papers, and there was no restriction for date of publication and language.
Data extraction and management
Data were extracted by two independent authors (GCM and MvT/JvD). A customised data extraction sheet was used to extract bibliometric data (ie, author, year of publication and language), characteristics of participants (ie, location of pain, age and sample size), description of the interventions (ie, types of interventions, comparisons, frequency, intensity and duration), details of the economic evaluation (ie, country, currency, type and perspective of the economic evaluation, time horizon, willingness to pay, reference year and discounting), outcomes assessed (ie, clinical outcomes, instruments, duration of follow-up assessments, type of direct and indirect costs) and study results (ie, cost-effectiveness: differences in clinical and costs outcomes and incremental cost-effectiveness ratios).
Assessment of the risk of bias of the included studies
Two review authors (GCM and MvT/CL) independently conducted the assessment of the risk of bias. Disagreements were solved first by discussion and then by arbitration of a third reviewer (JvD), if disagreements persisted. The assessment of the risk of bias of the randomised controlled trial design was evaluated using the criteria from the Cochrane Back and Neck Group with 13 items.22 24 25 Each item was scored as ‘yes’, ‘no’ or ‘unclear’. Studies that met at least 6 or more of the 13 criteria were considered as having a low risk of bias.24 26 We opted to use the Consolidated Health Economic Evaluation Reporting Standards statement with 24 items, which is a report checklist developed to assess methodological quality, to evaluate risk of bias of economic evaluations.27 However, items 15 (choice of model), 16 (assumptions) and 18 (study parameters) that evaluate studies with modelling methods were excluded. The possible answer to each item was ‘yes’, ‘no’ or ‘not applicable’. Items 4 (target population and subgroups), 7 (comparators), 8 (time horizon) and 11 (measurement of effectiveness) were scored ‘yes’ even if the studies did not include information on why population and comparators were chosen, why time horizon was appropriate, and why the single study was a sufficient source of clinical effectiveness data. We judged studies that fulfilled at least 14 of the 21 items as being at low risk of bias.
All publications related to the included studies (published protocols or clinical studies) were used to inform the risk of bias assessment and data extraction.
Data synthesis
Pain intensity and disability data were recorded, in which lower scores indicate improved effects. Differences in costs and effects were pooled in a meta-analysis, if possible, and incremental cost-effectiveness ratios were descriptively analysed. Results of the studies conducted with different times (eg, 6 months vs 1 year) were not combined in the meta-analysis. We used a random effect meta-analysis model. The assessment of heterogeneity was based on the I2 statistic.28 If substantial heterogeneity was present (I2>50%), we tried to find an explanation for this heterogeneity. If we did not find an explanation for this statistical heterogeneity, we pooled the data, but were careful with interpretation of the results.
All costs were converted to Euros and Pound Sterling using purchasing power parities.29 Furthermore, all monetary values were converted to the same reference year (2017) using consumer price indices for Euros30 and for Pound Sterling.31 We used the threshold set by the UK’s National Institute for Health and Clinical Excellence (NICE) as an indicator for cost-effectiveness.32 33 That is, if an intervention had an incremental cost-effectiveness ratio lower than £20 000 (€22 852) per QALY gained, the intervention was deemed as cost-effective compared with a comparator treatment. The intervention was also considered cost-effective when it was more effective and less costly compared with a comparator treatment. The intervention was not considered cost-effective when it was less effective and more costly compared with a comparator treatment or had an incremental cost-effectiveness ratio above £20 000 (€22 852) per QALY gained.
Results
Characteristics of included studies
After screening the 9158 unique records found in the search, a total of 22 studies were included in the review (figure 1). Characteristics of included studies are described in online supplementary appendix 2. Five studies included participants with neck pain,34–38 16 studies included participants with low back pain39–54 and 1 study included participants with neck pain and low back pain.55 The number of participants included in the studies varied from 80 to 1287. Eight studies included acute (<6 weeks),35 38 39 42 49 51 54 55 and 16 studies subacute (6–12 weeks) and chronic (>12 weeks)34–36 38 40 41 43–48 50 52 53 55 neck pain and low back pain. Most studies were conducted in Europe.34 35 37–39 41 43–55 One study was conducted in Switzerland,45 one study in Norway,52 three studies in Sweden,37 39 49 six studies in the Netherlands,34 35 38 46 50 53 eight studies in the UK,41 43 44 47 48 51 54 55 one study in Ghana40 and two studies in the USA.36 42
Supplementary file 2

Flow of systematic review.
Five studies36 37 43 47 55 applied the healthcare and societal perspective, one study39 applied the societal and employer perspective, one study46 applied the healthcare and employer perspective, six studies34 35 38 45 50 53 applied the societal perspective only and three studies44 48 51 applied the healthcare perspective only. Six studies40–42 49 52 54 did not report the perspective. If the applied perspective was not specifically mentioned, we assumed that studies that reported direct healthcare costs only were conducted from a healthcare perspective,40–42 and studies that also reported indirect costs were conducted from a societal perspective.49 52 54 Five studies37 40–42 54 did not calculate an incremental cost-effectiveness or cost-utility ratios.
Fifteen studies conducted a cost-utility analysis34–36 38 39 41 43–45 47 48 50 51 53 55; utilities were measured in terms of QALYs. Nine of these studies also conducted a cost-effectiveness analysis34–36 38 41 47 48 50 53 and clinical outcomes were measured in terms of pain intensity,34–36 41 48 53 number of days in pain,47 disability34–36 38 41 47 48 50 53 and global perceived recovery.34 35 38 53 Four studies37 40 44 54 conducted a cost-effectiveness analysis only and three studies46 49 52 conducted a cost-benefit analysis only.
Quality assessment
Risk of bias of the trial design
Five studies39 41 49 52 54 were at high risk of bias. None of the studies34–55 blinded assessors, patients or care providers. Four studies39 49 51 52 did not adequately report randomisation procedures, six studies37 39 41 42 49 52 did not have an adequate allocation concealment and nine studies38–41 44 45 47 49 51 had a high drop-out rate. In three studies,39 49 54 groups were not similar at baseline. Eight studies39–41 47 49 51 52 54 did not report information on cointerventions and in two35 37 studies cointerventions were different between groups. Five studies39 44 51 52 54 did not report on intervention compliance and in eight studies34 40 41 43 45 48 50 53 compliance was not acceptable (table 1).
Risk of bias assessment using the criteria from the Cochrane Back Review Group
Risk of bias in the economic evaluation
Eight studies37 40–42 48 49 52 54 were at high risk of bias. Items 1 (title),40–43 46 48 54 2 (abstract),35 37 39–42 44 46 48–50 52 54 55 6 (perspective),37 40 42 46 49 52 54 12 (measurement and valuation of preference-based),35 41 44 48 50 13 (estimating recourses and costs),37 40–42 45 49 52 54 14 (currency, price date and conversion),35 37 40 41 46 48 52 54 17 (analytical methods),37 40 42 44 48 49 52 54 19 (incremental costs and outcomes),37 40–42 44 49 52 54 and 20 (characteristics uncertainty)39 44 45 were most frequently failed. Five studies37 42 44 46 52 used a follow-up duration longer than 12 months, but only one of those studies44 reported using discounting (table 2).
Risk of bias assessment using the Consolidated Health Economic Evaluation Reporting Standards statement
Cost-effectiveness of exercise therapy
The results of the included studies for the cost-utility analysis are described in this session. The results of the included studies for cost-effectiveness analysis are presented in online supplementary appendix 3.
Supplementary file 3
Exercise therapy compared with usual care
Neck pain
Two studies were identified.35 37 A meta-analysis could not be performed, because the studies evaluated different time horizons.
Based on cost-utility analysis from a societal perspective, exercise therapy was associated with a cost of £−3421 (€−3840) per QALY gained (ie, cost-effective).35
Rosenfeld et al 37 did not perform a cost-utility analysis.
Acute low back pain
Four studies were identified.39 42 49 54 A meta-analysis could not be performed, because the studies evaluated different clinical outcomes and did not present mean or SD for costs.
Based on cost-utility analysis, exercise therapy was not significantly more effective than usual care for QALYs.39 The mean total societal cost was £1779 (€1969) for exercise therapy and £3787 (€4191) for usual care.39 The incremental cost-utility ratio was £4712 (€5214) per QALY gained from the employer’s perspective and £−10 874 (€−12 032) per QALY gained from the societal perspective (ie, cost-effective).39
Seferlis et al,49 Cherkin et al 42 and Wright et al 54 did not perform a cost-utility analysis.
Subacute and chronic low back pain
Five studies compared exercise therapy with usual care.43 45–47 51
Meta-analyses were conducted for QALY,43 45 51 and healthcare costs43 46 47 51 at 12 months (figure 2). There was no statistically significant difference in QALYs (mean difference: 0.03, 95% CI −0.01 to 0.06). From a healthcare perspective, the costs of exercise therapy were significantly higher than usual care (mean difference: £168, 95% CI 61 to 275; or mean difference: €176, 95% CI 64 to 288).

Forest plots of comparison: exercise therapy vs usual care for subacute and chronic low back pain.
Based on cost-utility ratio from a societal perspective, there was £82 657 (€88 965) per QALY gained for the comparison between exercise therapy and usual care (ie, not cost-effective).45
Based on cost-utility ratio from a healthcare perspective, there was £3760 (€3874) per QALY gained for the comparison between exercise therapy and usual care (ie, cost-effective).47 Based on cost-utility ratio from a healthcare perspective, there was an incremental increase of £11 649 (€12 293) per QALY gained (ie, cost-effective) for exercise therapy plus usual care compared with usual care alone.51
Based on cost-utility ratio from the healthcare perspective, there was £16 267 (€17 447) per QALY gained and exercise therapy was dominant from the societal perspective (ie, less costly and more effective).43
Hlobil et al 46 did not perform a cost-utility analysis.
Exercise therapy compared with other type of intervention
Exercise therapy versus manual therapy
Neck pain >2 weeks
Four studies34–36 38 compared exercise therapy with manual therapy (manipulation and mobilisation).
Meta-analyses were conducted for QALY,34–36 38 and societal costs34–36 38 at 12 months (figure 3). There were no significant differences in QALY (mean difference: −0.02; 95% CI −0.04 to 0.00) and costs (mean difference: £963, 95% CI −79 to 2005; €1023, 95% CI −86 to 2132). A sensitivity analysis was performed to identify if studies conducted in different countries could influence the results. Including only three studies conducted in the Netherlands34–36 38 resulted in smaller differences (mean difference: £427, 95% CI −39 to 894; €434, 95% CI −51 to 920), but these were also not statistically significant. Meta-analyses for other clinical outcomes are described in online supplementary appendix 3.

Forest plots of comparison: exercise therapy vs manual therapy for neck pain >2 weeks.
From a societal perspective, there was an incremental cost-utility ratio of £39 655 (€44 493) per QALY lost (ie, not cost-effective).35
From a societal perspective, exercise therapy had higher costs and smaller effects for QALY compared with manual therapy (ie, not cost-effective).34 Exercise therapy was associated with a cost of £14 740 (€16 138) per QALY lost in favour of manual therapy (ie, not cost-effective).38
From both the healthcare and societal perspective, exercise therapy was associated with higher costs and smaller effects for QALY in comparison with manual therapy.36
Acute low back pain
Two studies42 49 compared exercise therapy with manual therapy and performed only cost-effectiveness analysis (see online supplementary appendix 3 for results). A meta-analysis could not be performed, because the studies evaluated different time horizons, different clinical outcomes and did not present mean or SD for costs.
Subacute and chronic low back pain
The mean QALY was 0.63 for exercise therapy and 0.66 for manual therapy.51 The mean cost from the healthcare perspective was £682 (€719) for exercise therapy and £759 (€801) for manual therapy.51 The difference in costs and effects was not tested statistically, and an incremental cost-utility ratio was not presented.
Exercise therapy versus physiotherapy
Subacute and chronic low back pain
Five studies41 44 48 52 53 compared exercise therapy with physiotherapy among patients with subacute and chronic low back pain.
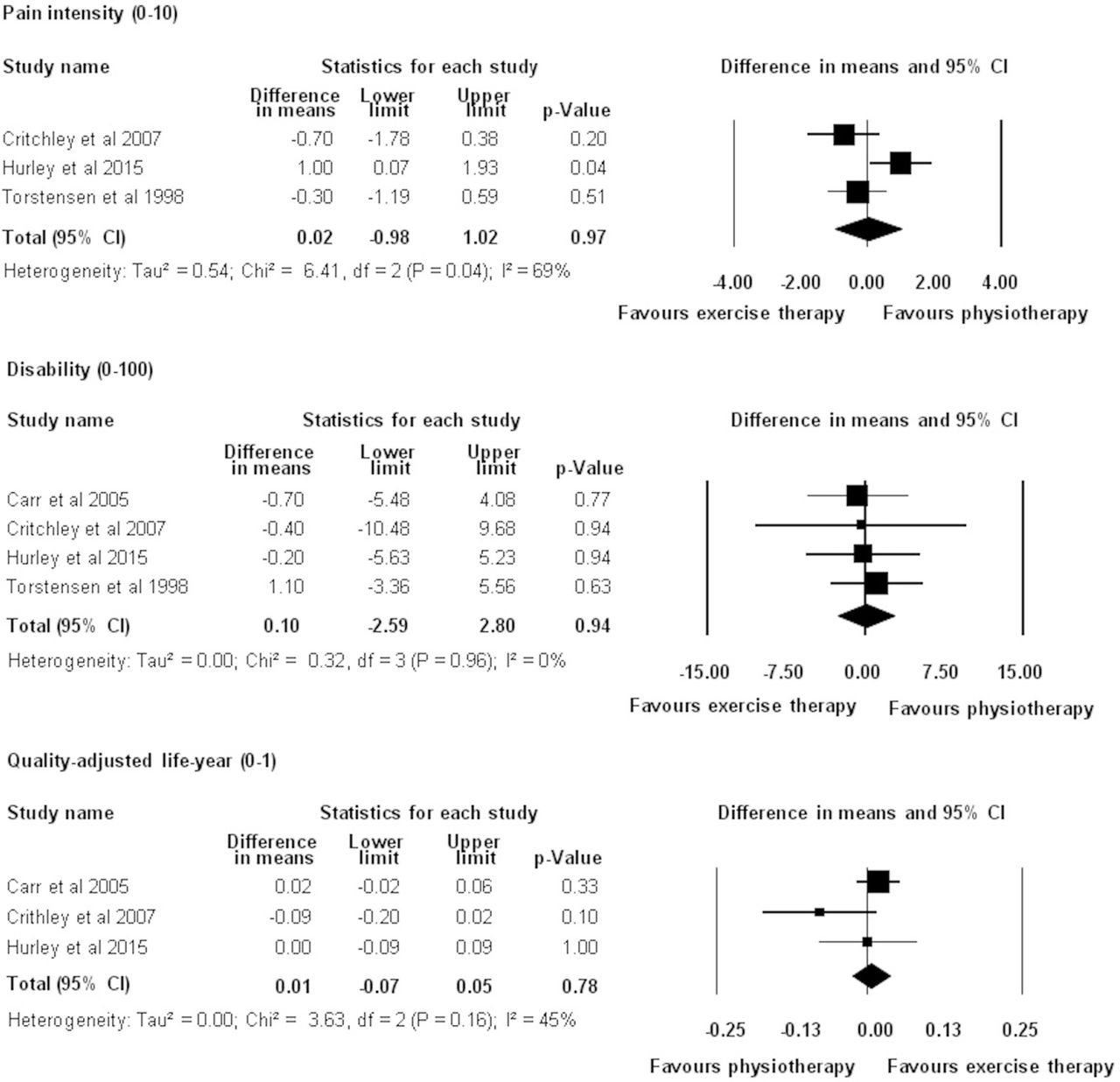
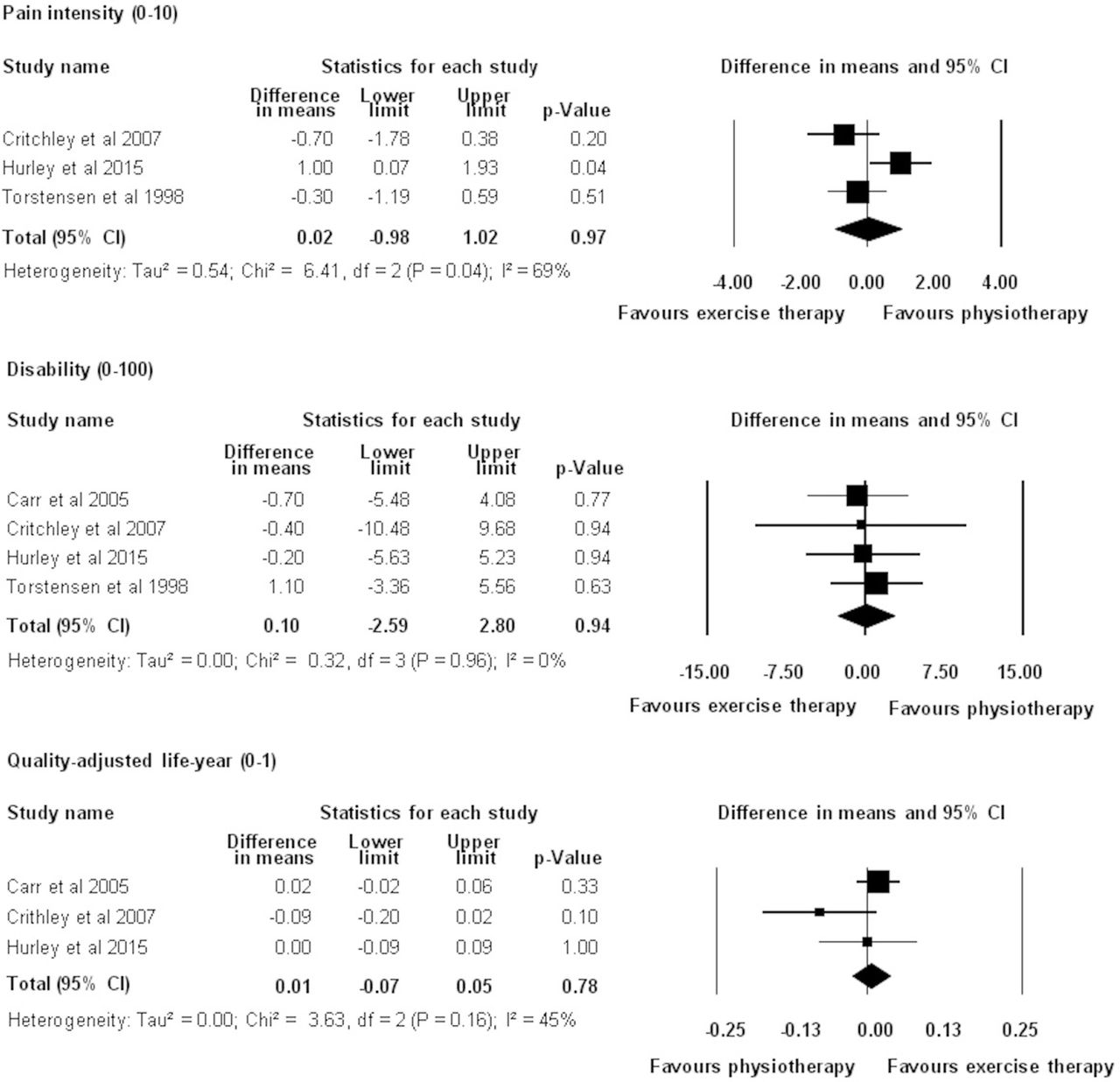
A meta-analysis was performed for this comparison (figure 4). We pooled data from three studies for QALY.41 44 48 Exercise therapy had similar improvements to physiotherapy (QALY: 0.01, 95% CI −0.07 to 0.05). The results for other clinical outcomes are described in online supplementary appendix 3. A meta-analysis for costs could not be performed, because studies evaluated different time horizons.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plots of comparison: exercise therapy vs physiotherapy for subacute and chronic low back pain.
From the healthcare perspective, exercise therapy had similar effect compared with physiotherapy for QALY. There were no significant differences in costs (£273 or €298 for exercise therapy and £480 or €525 for physiotherapy).41 There was an incremental cost-utility ratio of £−1416 (€−1456) per QALY lost for exercise therapy compared with physiotherapy (ie, less costly and less effective).44 There were no differences in QALY at 12 months.48 Total mean costs were £1875 (€2053) for exercise therapy and £1426 (€1561) for physiotherapy.48
From the societal perspective, there was an incremental cost-utility ratio of £6759 (€6213) per QALY gained (ie, cost-effective).53
Torstensen et al 52 did not perform a cost-utility analysis.
Exercise therapy versus cognitive behavioural approach
Neck pain and low back pain >2 weeks
Exercise therapy generated, on average, larger effects and higher costs compared with cognitive behavioural approach, but these differences were not statistically significant.55 The incremental cost-utility ratio was £1649 (€1683) per QALY gained from the healthcare perspective, and £7909 (€8078) per QALY gained from the societal perspective (ie, cost-effective).55 Exercise therapy had a probability of being cost-effective in comparison with cognitive behavioural of approximately 80% at a willingness to pay of £1000 (€1142) per QALY gained.55
Chronic low back pain
Two studies were identified.44 50 A meta-analysis could not be performed, because the studies evaluated different time horizons, different clinical outcomes and did not present mean or SD for costs.
There were no significant differences in effects of exercise therapy compared with cognitive behavioural approach and costs from a healthcare perspective. Based on the cost-utility ratio, exercise therapy was associated with higher costs and smaller effects than cognitive behavioural approach.44 Societal costs were £24 029 (23 621) or €24 488 (23 999) and mean QALY was 0.69 for exercise therapy, and £17 761 (20 661) or €18 100 (21 055) and mean QALY was 0.72 for cognitive behavioural approach.50 There was no statistical analysis for the societal costs and QALY, there was no cost-utility ratio for the comparison of exercise therapy and cognitive behavioural approach.50
Exercise therapy versus different type of exercises
Chronic neck pain
Exercise therapy was associated with higher costs and smaller effects than home exercise alone.36 The incremental cost-utility ratio value was not reported.36
Acute low back pain
There was no difference between general exercises and yoga exercises for QALYs.39 On average, general exercises generated higher costs than yoga from the employer (£194 or €215) and societal perspective (£1436 or €1589), but these differences were not statistically tested.39
Subacute and chronic low back pain
Three studies were identified.40 48 52 A meta-analysis could not be performed, because the studies evaluated different time horizons, different clinical outcomes and did not present mean or SD for costs.
From the healthcare perspective, there were no significant differences between stretching, aerobic and strengthening exercises compared with walking at 12 months for QALYs.48 Total mean costs for exercise therapy were £1875 (€2053), and for walking were £1090 (€1194). No incremental cost-effectiveness ratios were presented, and the difference in cost was not statistically tested.
Bello et al 40 and Torstensen et al 52 did not perform a cost-utility analysis.
Discussion
Main findings
The aim of this systematic review was to investigate the cost-effectiveness of exercise therapy in the treatment of patients with non-specific neck pain and low back pain. We found 22 economic evaluations conducted alongside randomised controlled trials. No studies investigated the cost-effectiveness of exercise therapy in comparison with no treatment. This is not surprising, as no treatment is not considered a realistic option in clinical guidelines. Findings were limited or inconsistent for comparisons between exercise therapy with usual care for neck pain and acute low back pain, other types of interventions for acute low back pain and different types of exercise in patients with neck pain or low back pain. Individual cost-utility ratios showed that exercise therapy was on average associated with lower costs and larger effects in comparison with usual care in patients with subacute and chronic low back pain from a healthcare perspective. In our meta-analyses, there were higher costs from a healthcare perspective for exercise therapy compared with usual care in patients with subacute and chronic low back pain. However, in the meta-analyses we were unable to examine uncertainty concerning data. When we pooled the data, there were also no differences for costs and effects between exercise therapy and manual therapy for neck pain.
Strengths and weaknesses of the review
We conducted meta-analyses for clinical and costs outcomes. Many studies included in this systematic review did not report SD or SEs of the mean effects and costs, although this did not affect the primary outcome, the incremental cost-utility ratio. In addition, many studies did not statistically test cost and/or effect differences, preventing statistical pooling. Studies also evaluated different time horizons and clinical outcomes. Considering these issues, the main limitation of our meta-analyses was the small number of studies per comparison. Although there are many randomised controlled trials investigating effectiveness of exercise therapy in the treatment of patients with neck pain and low back pain,56–58 there are only few economic evaluations conducted alongside randomised controlled trials.
We combined results of a relatively small number of all available trials on exercise therapy. Thus, the results may not represent the real effects of exercise therapy. This is underscored by the fact that various systematic reviews56 58 59 of randomised controlled trials suggested that exercise therapy was more effective than usual care for pain intensity and disability at long-term in patients with chronic neck and low back pain. We did not find significant differences for this comparison in the meta-analyses of the subset of trials that also included an economic evaluation. It was not possible to conduct a meta-analysis for all comparisons and perspectives due to heterogeneity between the studies, lack of information and uncertainty surrounding costs or effects.
The number of economic evaluations was limited, which could introduce publication bias. Cost-effectiveness analysis might be only conducted if there is a difference in effects. Therefore, studies included in this systematic review could report an overestimation of the real effect. However, we did not find any differences in effects in the meta-analyses.
We assumed that costs in different countries are generalisable to a similar population. We applied a sensitivity analysis in which we included only three studies conducted in the Netherlands.34 35 38 The sensitivity analysis did not influence the results of meta-analysis.
A strength of this systematic review is that there were no restrictions for studies that did not include cost-effectiveness or cost-utility ratios (ie, incomplete economic evaluations), date of publication and language. We judged that most studies with incomplete economic evaluations37 40–42 54 were at high risk of bias. In future research, it would be prudent to only perform full economic evaluations to expand the evidence on cost-effectiveness of exercise therapy for neck pain and low back pain.
Little evidence for the cost-effectiveness of exercise therapy
Exercise therapy is a common intervention recommended by clinical practice guidelines for neck pain and low back pain,8 9 11 but there is still little evidence of its cost-effectiveness. As evidence for exercise therapy suggests that differences in effects compared with other interventions are small or moderate for patients with neck pain and low back pain,56 58 59 cost-effectiveness of treatments becomes more important in making decisions due to limited healthcare resources. There are two systematic reviews that investigated the cost-effectiveness of conservative interventions for neck pain60 61 and three systematic reviews for low back pain.62–64 However, none of these conducted a meta-analysis to compare results of costs and effects of the studies included. Furthermore, these systematic reviews did not include studies with incomplete economic evaluation.40–42 46 49 52 54 Present review included all economic evaluations (complete and incomplete analyses) and also included recently published studies.36 38 48 Thus, it was possible to pool data and analyse all published economic evaluations.
Our results correspond with those of other systematic reviews60 61 on neck pain. Behavioural graded activity was not cost-effective (ie, similar costs and effects) compared with manual therapy for neck pain, and combined treatment (consisting of advice, exercise therapy and manual therapy) was not cost-effective compared with usual care plus exercise therapy for neck pain.60 Exercise therapy was cost-effective compared with usual care for neck pain, but combined treatment (consisting of exercise therapy and manual therapy) was not.61 We found that home exercises plus manual therapy had lower costs and larger effects in comparison with home exercises alone.
There is inconsistent and heterogeneous evidence,62 64 although, exercise therapy may be a cost-effective intervention compared with usual care for chronic low back pain.63 We found that exercise therapy seems to be cost-effective compared with usual care, but the cost-effectiveness is similar in comparison with physiotherapy for subacute and chronic low back pain.
Future directions and implications
There remains a need for more high-quality economic evaluations alongside randomised controlled trials to evaluate the cost-effectiveness of exercise therapy compared with usual care and other types of interventions for patients with acute, subacute and chronic neck pain and low back pain. Economic evaluations comparing exercise therapy with drugs and surgery for patients with neck and low back pain are urgently needed. We recommend adding an economic evaluation to any future randomised controlled trial. Collaboration with health economists or other researchers with expertise in the field of health economics/health technology assessment is beneficial. Researchers must also report on the uncertainty surrounding the estimates and statistically test cost and effect differences. These steps may also help guideline developers when they consider cost-effectiveness in treatment recommendations.
Conclusions
Exercise therapy seems to be cost-effective compared with usual care for subacute and chronic low back pain. Exercise therapy was not (more) cost-effective, and had similar costs and effects compared with other type of interventions for neck pain, and subacute and chronic low back pain.
What is already known?
Neck pain and low back pain are leading causes of years lived with disability.
Exercise therapy may reduce pain and disability of patients with neck pain and low back pain.
What are the findings?
Exercise therapy seems to be cost-effective compared with usual care for subacute and chronic low back pain.
Exercise therapy had similar costs and effects related to other interventions.
Evidence around exercise therapy compared with usual care for neck pain and acute low back pain, other interventions for acute low back pain, and different types for neck pain and low back pain are still inconclusive.
Acknowledgments
The authors would like to thank the São Paulo Research Foundation (FAPESP) for financial support and Australian National Health and Medical Research Council for a Careers Development Fellowship.
References
Footnotes
Contributors GCM drafted the manuscript and conducted meta-analyses. GCM, MvT and JvD screened titles, abstracts and full paper for inclusion. GCM, MvT and JvD were involved in data extraction. GCM, MvT and CL conducted the assessment of the risk of bias and conducted meta-analyses. All authors contributed with research question, critically reviewed the manuscript and approved the manuscript prior to submission.
Funding GCM had her PhD scholarship supported by São Paulo Research Foundation (FAPESP (process: 2013/26321-8 and 2016/07915-2)). CL was supported by a fellowship from the National Health and Medical Research Council, Australia.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.