Article Text

Abstract
Background and objectives Several studies have evaluated the effect of pectoral nerve blocks to improve postoperative analgesia following breast cancer surgery resulting in contradictory findings. The aim of this study was to examine the effect of Pecs blocks on postoperative analgesia in women following mastectomies.
Methods We performed a quantitative systematic review in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. Articles of randomized controlled trials that compared Pecs block (types I and II) to a control group in patients undergoing mastectomy were included. The primary outcome was total opioid consumption 24 hours after surgery. Secondary outcomes included pain scores and side effects. Meta-analysis was performed using the random effect model.
Results 7 randomized controlled trials with 458 patients were included in the analysis. The effect of pectoral nerve blocks on postoperative opioid consumption compared with control revealed a significant effect, weighted mean difference (WMD) (95% CI) of -−4.99 (−7.90 to −2.08) mg intravenous morphine equivalents (p=0.001). In addition, postoperative pain compared with control was reduced at 6 hours after surgery: WMD (95% CI) of −0.72 (−1.37 to −0.07), p=0.03, and at 24 hours after surgery: WMD (95% CI) of −0.91 (−1.81 to −0.02), p=0.04.
Discussion This quantitative analysis of randomized controlled trials demonstrates that the Pecs block is effective for reducing postoperative opioid consumption and pain in patients undergoing mastectomy. The Pecs block should be considered as an effective strategy to improve analgesic outcomes in patients undergoing mastectomies for breast cancer treatment.
- pre-emptive analgesia
- opioids, adverse effects
- regional anesthesia
- acute pain
- postoperative pain
Statistics from Altmetric.com
Introduction
Women electing to pursue surgical interventions for breast cancer (eg, mastectomies) often experience moderate to severe postoperative pain and opioid-related side effects such as nausea and vomiting.1–3 These side effects frequently result in patient discomfort and increased hospital stay.4 5 In addition, poorly controlled postoperative pain may lead to a decrease in quality of recovery and the development of persistent postsurgical pain.6–8
Over the past few years, several studies have evaluated the ability of two novel techniques targeting nerves of the thoracic wall (pectoral nerve blocks: Pecs type I and type II blocks) to improve postoperative analgesia following breast cancer surgery. Nonetheless, many of these studies have resulted in contradictory findings. A quantitative analysis of this literature examining the effectiveness and safety of these newer regional anesthetic techniques for patients undergoing breast cancer surgery has not yet been performed.
The aim of this systematic review was to examine the ability of pectoral nerve (Pecs) blocks type I and/or II to improve postoperative analgesia in women following mastectomies. We also aimed to summarize complications associated with these regional anesthesia techniques.
Methods
The review was performed in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.9 Institutional review board approval was not required.
Systematic strategy
Articles of randomized controlled trials exploring pectoral nerve blocks on postoperative pain following breast cancer surgery were identified by searching electronic databases (PubMed, Embase, Cochrane and Google Scholar) up to December 2018. Key words and Medical Subject Headings (MeSH) descriptor terms were: ‘interfascial plane’, ‘regional’, ‘peripheral’, ‘pectoral’, ‘pecs’, ‘breast surgery’, ‘nerve blocks’ and ‘mastectomy’ were used in a variety of sequences. The search was restricted to adults 18 years of age or older. In addition to the primary search methods, the bibliographies from the identified articles were also reviewed for additional studies. Language restrictions were not used. Unpublished studies were not investigated. There was no limitation on sample size.
Inclusion and exclusion criteria
The inclusion and exclusion criteria were defined prior to the commencement of the systematic review. Articles of randomized controlled trials that compared interfascial plane techniques (pectoral nerve block; Pecs type I, modified pectoral nerve block; Pecs type II) with local anesthetics to a control group (ie, no block or sham block) in patients undergoing mastectomy with or without lymph node dissection were included. Articles had to describe postoperative outcomes of pain scores or opioid consumption. We included studies involving Pecs blocks type I and type II.
Selection of included articles and data extraction
According to the search strategy, two investigators (DL-C and MCK) individually assessed the abstracts and trial outcomes retrieved by the initial query. Articles that did not fulfill the inclusion criteria or met the exclusion criteria were omitted. Disputes between the reviewers were finalized by discussion and if a resolution was not met, the final decision was determined by an additional investigator (ADC) who was incognizant of the discussion by the previous investigators.
Two investigators (DL-C and MCK) individually evaluated the full text of all included randomized control trials and extracted data from each individual trial using a predesignated collection form. Disputes between reviewers were finalized by discussion and if a resolution was not met, the final decision was determined by an additional investigator (ADC). The data extracted from the randomized controlled trials included type of nerve block, use of ultrasound guidance, choice of local anesthetic and dose, surgery description, choice of anesthesia, number of patients in treatment and control groups, postoperative opioid consumption, postoperative pain scores (≤6 hour and 24 hours) at rest and adverse events (eg, local anesthetic toxicity, hypotension and pneumothorax) associated with block placement. Numerical rating scale of pain or visual analog scale were adapted to an 11-point numeric rating scale (0=no pain, 10=extreme pain). Postoperative opioids were transformed to equianalgesic dose of intravenous morphine assuming no cross-tolerance.10
The data were obtained from the text or tables of the selected articles, and when data were not available, it was obtained directly from the figures. Continuous outcomes were recorded using mean and SD. Data that were reported as median, IQR, or mean±95% CI were transformed to mean and SD using the method of Hozo et al.11 The SD for postoperative pain scores was approximated using the most extreme values. When the same outcomes were reported more than once, the most conservative value was used.
Methodological quality of clinical research trials
Two investigators (DL-C and MCK) individually assessed the included articles for their quality using the Jadad scale.12 The modified Jadad assessment tool is used to evaluate the methodological quality of a clinical trial using the following elements: randomization, blinding and masking of patients and completeness of data at follow-up including patient withdrawal. Disputes between reviewers were finalized by discussion and if a resolution was not met, the final decision on scores was determined by an additional investigator (ADC). The overall score of clinical trial quality ranges from 0 to 5, with 0–2 indicating low quality, while 3–5 signifies high quality.
Outcomes
Primary outcome included total opioid consumption in the postoperative period 24 hours after surgery. Secondary outcomes were pain scores in the postoperative period (≤6 and 24 hours after surgery), incidence of postoperative nausea and vomiting (up to 24 hours) and adverse outcomes (ie, postoperative hypotension, pneumothorax and local anesthetic toxicity).
Bias assessment
The Cochrane Risk-of-Bias Tool was used to evaluate the potential risk of bias in the included randomized trials. The risk bias tool involves six specific domains involving selection bias, detection bias, performance bias, attrition bias, reporting bias and other potential source of bias.13 Two investigators (DL-C and MCK) individually evaluated the risk of bias of the included studies. An additional investigator was involved in the assessment if there was a discrepancy among the previous two investigators (ADC). The assessment of each domain was recorded either as low risk, high risk or unclear risk indicating that there was inconclusive information or unknown risk of bias.
Statistical analysis
A meta-analysis was performed for studies that had similar comparision outcomes if the total number of included studies was not less than three studies. The pooled data consisting of continuous variables (total opioid consumption at 24 hours, pain score at 6 hours and at 24 hours) was calculated and expressed as weighted mean differences (WMDs) with 95% CIs.
A significant effect compared with control required that the 95% CI for continuous data did not include zero, and for dichotomous data, the 95% CI did not include 1.0. Due to the the limited amount of randomized trials identified, we elected to use the random-effects model in an attempt to generalize our findings to trials not included in our meta-analysis.14
A funnel plot was used to investigate publication bias and further analyzed using Egger’s regression test.15 A one-sided p<0.05 was considered as an indication of an asymmetric funnel plot. Heterogenity between studies was assumed to be statiscally significant if the I2 statisic was greater than 50% or P<0.05. If heterogeneity was high, we perfromed a senistivity analysis by removing individual studies and examing its effect on the overall heterogenity. A two-sided p value<0.05 was considered statistcally significant. All statistical analyses were performed using the Comprehensive Meta-Analysis software Version 3 (Biostat, Englewood, New Jersey, USA).
Results
The primary search yielded 681 studies, and after screening and removing article duplications, 110 potential articles were identified. Articles that did not meet eligibility on further review of full texts were excluded. The specific reasons for exclusion of articles are depicted in figure 1. A total of seven randomized controlled trials with 458 patients were eligible and included in the analysis. The median (IQR) sample size for included studies was 60 (52–73) and the median Jadad score was 5 (4.5–5). The demographic characteristics of the included trials are summarized in table 1.16–22 All seven randomized controlled trials reported on postoperative opioid consumption and/or pain scores.

Flow chart of selected studies.
Included studies
Quality assessment
All trials reported inclusion and exclusion criteria and described baseline characteristics. Randomized treatment allocation sequences were created with number generator computer software program or random number tables in all studies. Randomized controlled trials describing proper concealment of treatment allocation were described in three trials.17 18 20 All studies described study personnel and outcome assessors as blinded to treatment allocation. The description of patient blinding was not clear in one study.16 The methodological quality and judgements about each risk of bias domain as a percentage across all included studies is presented in table 2.
Methodological quality and risk bias summary
Postoperative opioid consumption at 24 hours
The pooled data of five clinical trials16 18 19 21 22 investigating the effect of pectoral nerve blocks on postoperative opioid consumption compared with control revealed a significant effect, WMD (95% CI) of −4.99 (−7.90 to −2.08) mg intravenous morphine equivalents (p=0.001) (figure 2). Heterogeneity was high, I2=91. A visualization of the funnel plot did not reveal asymmetry; Eggers regression test did reveal asymmetry (ie, a one-sided p=0.48). A sensitivity analysis by removing individual studies did not substantially reduce heterogeneity.

Meta-analysis evaluating the effect of Pecs blocks with local anesthetic on postoperative opioid consumption compared with control at 24 hours after surgery. The overall effect of Pecs blocks versus control was estimated as a random effect. The point estimate (95% CI) for the overall effect was −4.99 (−7.90 to −2.08) (p=0.001) mg intravenous morphine equivalents.
Postoperative pain ≤6 hours after surgery
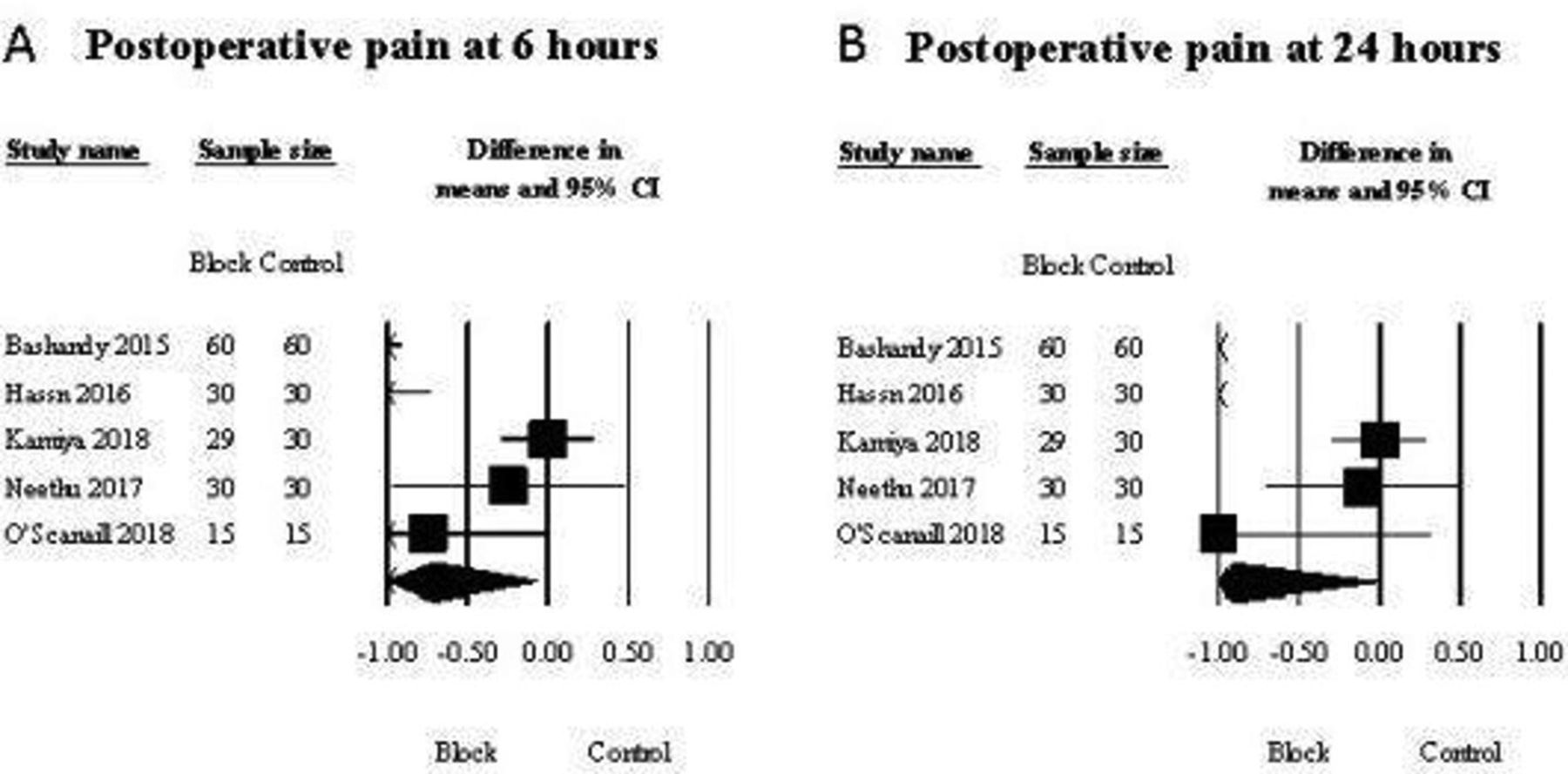
The pooled data of five studies16 18–21 examining the result of pectoral nerve blocks on postoperative pain compared with control at 6 hours after surgery revealed a statistically significant effect: WMD (95% CI) of −0.72 (−1.37 to −0.07); p=0.03 (figure 3). Statistical heterogeneity was high, I2=88. An examination of the funnel plot did not reveal asymmetry (ie, Eggers regression test revealed a one-sided p=0.21). A sensitivity analysis by deleting individual studies did not substantially reduce heterogeneity.

{kind=link}
{kind=link}
{kind=link}
Meta-analysis evaluating the effect of Pecs blocks on postoperative pain to control at (A) 6 hours and (B) 24 hours after surgery. The overall effect of Pecs blocks with local anesthetic versus control was estimated as a random effect. In part A, the point estimate (95% CI) for the overall effect was −0.72 (−1.37 to −0.07) (p=0.03) (0–10 numerical scale). In part B, the point estimate (95% CI) for the overall effect was −0.91 (−1.81 to −0.02) (p=0.04) (0–10 numerical scale). The weighted mean difference for individual studies is represented by the square symbol on Forrest plot, with 95% CI of the differences shown as a solid line. The size of the square and the thickness of the 95% CI line resemble the sample size.
Postoperative pain at 24 hours after surgery
The pooled data of five studies16 18–21 examining the result of pectoral nerve blocks compared with control on pain at 24 hours after surgery revealed a statistically significant effect: WMD (95% CI) of −0.91 (−1.81 to −0.02); p=0.04 (figure 3). Statistical heterogeneity was high, I2=95. An exploration of the funnel plot did not reveal asymmetry (ie, Eggers regression test revealed a one-sided p=0.43). A sensitivity analysis by deleting individual studies did not substantially reduce heterogeneity.
Safety analysis
Block complications
One study reported that three patients experienced hematoma and/or bleeding following needle placmement of the pectoral nerve blocks.17 This would translate to an incidence (95% CI) of 0.7% (0.1% to 2.0%) when considering the aggregate number of patients.
Postoperative side effects
The pooled data of four studies17–19 21did not suggest that pectoral nerve blocks had a significant effect on postoperative nausea and vomiting compared with control at 24 hours after surgery OR (95% CI) of 0.80 (0.44 to 1.48), p=0.48. Heterogeneity was not observed (I2=0).
Discussion
The most important finding of the current study revealed that the use of pectoral nerve blocks reduced total opioid consumption in the postoperative period for women undergoing breast cancer surgery. Moreover, the use of pectoral nerve blocks reduced postoperative pain at 6 and 24 hours following surgery. Taken together, our results suggest that pectoral nerve blocks are an effective analgesic option for acute postoperative period pain management in women undergoing mastectomy surgeries.
Our results are clinically important since poor postoperative pain control is common in patients having breast cancer surgery. In addition, the development of persistent postsurgical pain has been associated with inadequate pain control immediately after the surgery.23 24 It is, therefore, possible that the use of the pectoral nerve blocks can ameliorate acute pain after surgery and subsequently reduce the development of persistent postsurgical pain.
Another important finding of our study was the low incidence of complications due to pectoral nerve blocks (eg, systemic toxicity or pneumothorax). One clinical trial included in our analysis reported the occurrence of a hematoma and/or bleeding in three patients (2.3%); however, the authors were uncertain if they were related to the placement of the block or due to a surgery complication.17 Our finding is similar to previous reports that pectoral nerve blocks appear to cause less postprocedural complications than neuraxial blocks.25–27
The use of pectoral nerve blocks can be used as an alternative to other more technically advanced analgesic blocks such as thoracic epidural analgesia and thoracic paravertebral blocks.28 29 Recently, Versyck et al performed a systematic review and concluded that the analgesic effect of the Pecs II block was comparable with the paravertebral block.30 Nonetheless, the authors included multiple types of surgery (eg, breast conserving surgery, breast reconstruction surgery and mastectomies) and the analgesic effect of the Pecs block on mastectomy surgery alone was not estimated. Future studies to determine the analgesic effect of the Pecs block compared with paravertebral blocks for mastectomy surgeries are still warranted.
It was also interesting to note that we did not observe an overall effect of the Pecs block on opioid-related side effects (eg, nausea and vomiting) despite detecting a reduction on opioid consumption and pain scores. If both comparisons groups had a targeted goal for reduction of pain, it is plausible that the control group would have required more opioids and patients would have experienced more postoperative nausea and vomiting. In addition, all patients received robust antiemetic prophylactic medication that may explain why we could not detect a difference.
Zhao et al performed a prior quantitative analysis to estimate the analgesic effects of Pecs blocks on patients undergoing mastectomy surgeries.31 There are several substantial differences between the prior meta-analysis and the current one. First, the quantitative analysis was done by combining randomized trials and cohort studies which may not be methodologically acceptable. This is likely the reason why they detected an enormous opioid sparing effect of Pecs Blocks ((SMD (95% CI) of 1.37 (2.12 to 0.63)) compared with the modest opioid sparing effects that we detected in the current study. In addition, Zhao et al included studies with catheters and other blocks (eg, serratus block), therefore their results cannot be attributed to the Pecs blocks alone.32
Our study can only be understood when taken into consideration its limitations. In order to minimize clinical heterogeneity, we only examined the effect of pectoral nerve blocks for patients undergoing mastectomies. We cannot, therefore, generalize our findings to other types of breast surgery (eg, cosmetic, breast conserving and reconstruction). We did not compare the effect of Pecs blocks to other regional anesthesia techniques (eg, erector spinae block, serratus and paravertebral blocks) given the low number of studies proving direct comparisons between these techniques.33–36 Sena et al has demonstrated that quantitative analysis should be discouraged when less than four comparisons are available.37 Lastly, we did not examine a dose response effect of the Pecs blocks since the dosage used in the included studies did not provide enough variability.
In conclusion, this quantitative analysis of randomized controlled trials demonstrates that the use of the Pecs block is mildly effective for reducing opioid consumption and pain in the acute postoperative period for patients undergoing mastectomy. Improving pain control in the acute recovery period may decrease the occurrence of chronic pain in patients undergoing breast cancer surgery. The Pecs blocks should be considered as an effective strategy to ameliorate analgesic outcomes of patients undergoing mastectomies for the treatment of breast cancer.
References
Footnotes
Contributors All the authors listed qualifies to authorship.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement There are no data in this work.