Article Text

Abstract
Objective To determine the effect of prescription opioid use in the year before surgery on opioid consumption after surgery.
Background Recently developed postoperative opioid prescribing guidelines rely on data from opioid-naïve patients. However, opioid use in the USA is common, and the impact of prior opioid exposure on the consumption of opioids after surgery is unclear.
Methods Population-based cohort study of 26,001 adults 18 years of age and older who underwent one of nine elective general or gynecologic surgical procedures between January 1, 2017 and October 31, 2019, with prospectively collected patient-reported data from the Michigan Surgical Quality Collaborative (MSQC) linked to state prescription drug monitoring program at 70 MSQC-participating hospitals on 30-day patient-reported opioid consumption in oral morphine equivalents (OME) (primary outcome).
Results Compared with opioid-naïve participants, opioid-exposed participants (26% of sample) consumed more prescription opioids after surgery (adjusted OME difference 12, 95% CI 10 to 14). Greater opioid exposure was associated with higher postoperative consumption in a dose-dependent manner, with chronic users reporting the greatest consumption (additional OMEs 32, 95% CI 21 to 42). However, for eight of nine procedures, 90% of opioid-exposed participants consumed ≤150 OMEs. Among those receiving perioperative prescriptions, opioid-exposed participants had higher likelihood of refill (adjusted OR 4.7, 95% CI 4.4 to 5.1), number of refills (adjusted incidence rate ratio 4.0, 95% CI 3.7 to 4.3), and average refill amount (adjusted OME difference 333, 95% CI 292 to 374)).
Conclusions Preoperative opioid use is associated with small increases in patient-reported opioid consumption after surgery for most patients, though greater differences exist for patients with chronic use. For most patients with preoperative opioid exposure, existing guidelines may meet their postoperative needs. However, guidelines may need tailoring for patients with chronic use, and providers should anticipate a higher likelihood of postoperative refills for all opioid-exposed patients.
- analgesics, opioid
- pain, postoperative
- outcome assessment, health care
- acute pain
Data availability statement
No data are available.
Statistics from Altmetric.com
Introduction
Excess opioid prescribing continues to play a role in the opioid crisis in the USA. As overdose deaths reach new peaks, more than one in three opioid overdose deaths have been found to involve prescription opioids.1 Surgical prescribing has been increasingly implicated as a key contributor to this problem.2 Opioid prescribing in the perioperative setting results in leftover tablets, new persistent use of opioids, and escalation in doses after surgery for patients on chronic opioid therapy, all of which increase opioid-related harms to patients, their families, and communities.3 4
To optimize prescribing of opioids after surgery, best practices and recommendations from prescribing guidelines aim to balance adequate pain control while minimizing the risks of overprescribing.5 Data-driven guidelines for surgical prescribing have advanced this effort by relying on patients to report their actual opioid consumption after surgery alongside measures of pain and satisfaction. For example, the use of procedure-specific prescribing guidelines based on patient-reported opioid consumption has been shown to markedly reduce postoperative opioid prescribing while providing satisfactory pain care.6 7 Nonetheless, these studies either focus solely on opioid-naïve patients or do not distinguish between opioid-naïve and opioid-exposed patients. As such, current prescribing recommendations are not tailored to preoperative opioid exposure.8 Despite this, opioid exposure before surgery has been shown to result in worse outcomes for patients, including higher costs, longer length of stay, and greater risk for postoperative complications.9 10
Opioid use before surgery is common, with estimates suggesting that up to 1 in three adults report the use of opioid medications in the past year before surgery.3 9 Therefore, understanding the impact of opioid exposure before surgery on postoperative opioid use is critical to calibrate prescribing to meet patients’ needs, eliminate excess prescribing, and ensure a safe and comfortable postoperative recovery. In this context, we sought to determine how opioid use in the year prior to surgery influences opioid consumption in the month following common surgical procedures. We hypothesized that preoperative opioid exposure will be associated with greater opioid consumption after surgery when compared with opioid-naïve patients. In addition, we hypothesized that patients with opioid exposure before surgery will have higher rates of consuming any opioids after surgery and greater postoperative prescribing as evidenced by larger prescription sizes and higher rates of opioid prescription refills.
Methods
We retrospectively analyzed prospectively collected data from 70 hospitals participating in the Michigan Surgical Quality Collaborative (MSQC), a patient safety organization that captures data on participants undergoing general and gynecologic surgical procedures. As previously described, the MSQC database includes demographic, perioperative, clinical, and mortality characteristics collected via postoperative surveys.11 Patient-reported outcomes including patient-reported opioid consumption are collected using surveys administered between days 30 and 90 following discharge. A sampling algorithm facilitates case review while minimizing selection bias and ensuring a representative sample.12 Data integrity was enhanced via collection and audit by MSQC-trained nurse reviewers using standardized data definitions, with data checks and assessments for accuracy by a centralized coordinated center.11 Data from MSQC was then linked to data from the Michigan Automated Prescription System, which serves as the state’s prescription drug monitoring program (PDMP) and aggregates data on all controlled substance fills in the state of Michigan. To safeguard participant privacy, linkage followed a state-approved process and was accomplished by a third party that removed all protected health information from the final dataset.
Study cohort and period
We included participants undergoing surgery from January 1, 2017 to October 31, 2019. The study cohort consisted of adult patients ≥18 years who underwent elective, emergent or urgent surgery in outpatient and inpatient settings. Surgical procedures included laparoscopic appendectomy, laparoscopic cholecystectomy, colectomy (laparoscopic or open), hernia (abdominal or minor), and hysterectomy (laparoscopic, vaginal, or total abdominal). We excluded patients who lacked self-reported data on consumption, who had discrepant discharge opioid prescription data between PDMP and MSQC, who had multiple PDMP matches, who underwent additional surgeries within 90 days following the index operation, who were not discharged home, who had a length of stay >30 days, and who had 30-day readmissions, reoperations, or complications. Patients without valid opioid prescription data, surgeon data, or who resided outside the state of Michigan were also excluded. We defined the study period for the year before surgery as spanning 365 days before to 31 days before surgery. The perioperative period for the first opioid prescription fill spanned 30 days before to 3 days after surgery. Refills were identified as additional fills after the initial prescription within 30 days of discharge after surgery.
Opioid exposures and covariates
The key explanatory variable was preoperative opioid exposure (yes/no), defined as any opioid fill in the year before surgery from the PDMP. Opioid prescriptions in MSQC were defined using names from the Centers for Disease Control and Prevention, which included tramadol but not methadone or buprenorphine.13 The amount of consumed opioids as reported by patients after surgery came from MSQC. Opioid pharmacy fills (type, dose, quantity) during the study period came from the PDMP, which included buprenorphine. These were standardized to oral morphine equivalents (OME).13 Report of opioid fill in the perioperative period by either PDMP or MSQC was used to indicate an opioid fill.
Opioid exposure in the year before surgery from PDMP data was classified into four groups adapted from a machine learning cluster analysis technique, with the following mutually exclusive categories based on quantity and duration: (1) naïve, no opioid prescription fills; (2) minimal,≤1 month fill with <675 OMEs (ie, 90 pills of oxycodone 5 mg); (3) intermittent, between 1 month with ≥675 OMEs and 8 months filled; and (4) chronic ≥9 months filled.9
Demographic data included age, sex, race/ethnicity, and insurance type. Patient characteristics included American Society of Anesthesiologists (ASA) physical status classification, alcohol use, body mass index (BMI) (<25, 25 to <30, 30 to <35, ≥35), tobacco use over past year, and relevant patient comorbidities. Procedure and clinical characteristics included type of surgery, admission status (inpatient vs outpatient), surgical priority (elective vs urgent/emergent), and length of stay (days).
Outcomes
The primary outcome was patient-reported opioid consumption after discharge from surgery, defined as the amount of prescription opioids reported as consumed by patients in the 30-day postoperative period from MSQC. Secondary outcomes included likelihood of patient-reported opioid consumption after surgery, number and likelihood of opioid refills, and the average amount of opioid refill, defined as the quantity in OMEs for any fills after the initial perioperative prescription and within 30 days of discharge.
Statistical analysis
Baseline clinical and prescribing patterns for subgroups of participants were characterized using descriptive statistics. Opioid amounts were reported in median OMEs, IQR, and ranges. Initial comparisons of outcomes for opioid-naïve and opioid-exposed participants were performed using χ2 or t-tests. Generalized linear mixed models were used to examine association of preoperative opioid exposure with each outcome. To account for clustering within surgeons, surgeon was included as a random effect. Robust standard errors were used for models with the primary outcome of opioid consumption and opioid amount in refills. A Gaussian distribution/identity link function was used to determine the association of preoperative opioid exposure with opioid consumption while adjusting for characteristics that differed between opioid-exposed and naïve participants. We used a Bernoulli distribution/logit link function to examine outcomes for likelihood of opioid consumption and refill, and used a negative binomial distribution/log link function for number of refills. A Gaussian distribution/identity link function was used to examine opioid exposure and amount of opioid prescribed in refills. Refills, number of refills, and amount of opioids in refills were evaluated only in participants filling a perioperative prescription.
In secondary analyses of the primary outcome, we examined models of patient-reported postoperative opioid consumption as a function of opioid exposure in the year before surgery using four classifications of naïve, minimal, intermittent, and chronic use and, in a sensitivity analysis, models based on total opioid dose in the year before surgery. The significance level was p<0.05. Analyses were performed using Stata/SE V.15.1 (StataCorp).
Results
Among 58 468 potential participants at 70 hospitals, 26,001 participants (mean age 54, SD 16; 57% female) met inclusion criteria for the primary analysis, including 6800 (26%) opioid-exposed participants who filled at least one opioid prescription in the year before surgery and 19 201 (74%) opioid-naïve participants with no opioid prescription fills in the year before surgery (online supplemental efigure 1). Compared with opioid-naïve participants, those with opioid exposure were more likely to be female, have Medicaid insurance, have a higher ASA classification status, and have a higher BMI (table 1).
Supplemental material
Patientcharacteristics by opioid exposure status in the year before surgery
Patients with opioid exposure before surgery were more likely to have comorbidities including bleeding disorders, coronary artery disease, diabetes, dialysis use, hypertension, cancer, sleep apnea, immunosuppression, and peripheral vascular disease. They were also more likely to undergo elective surgery.
While most participants (89%) received preoperative opioid doses of <50 OME per day on average, higher-risk exposures of 50 to <100 OME (9%) and 100 OME or more (2%) did occur. Among opioid-exposed participants, 52% (n=3524) met criteria for minimal opioid exposure, while intermittent and chronic exposure occurred in 38% (n=2599) and 10% (n=677), respectively.
In unadjusted comparisons, opioid-exposed participants were prescribed opioids at discharge more often (81% vs 66%) and were prescribed larger total quantities (median OME 100; IQR 50, 200 vs 60; 0, 100) in the initial discharge prescription than opioid-naïve participants.
Opioid consumption after discharge from surgery
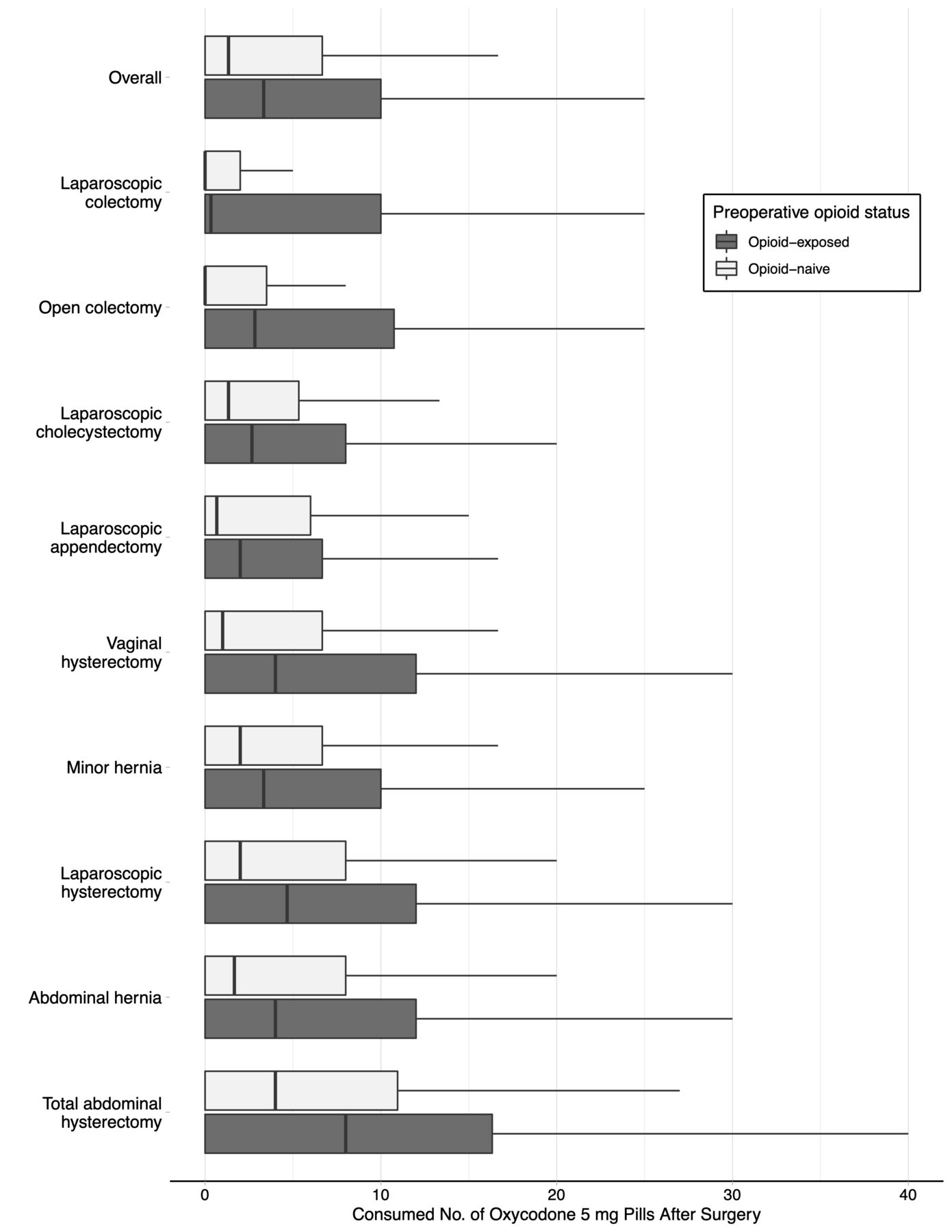
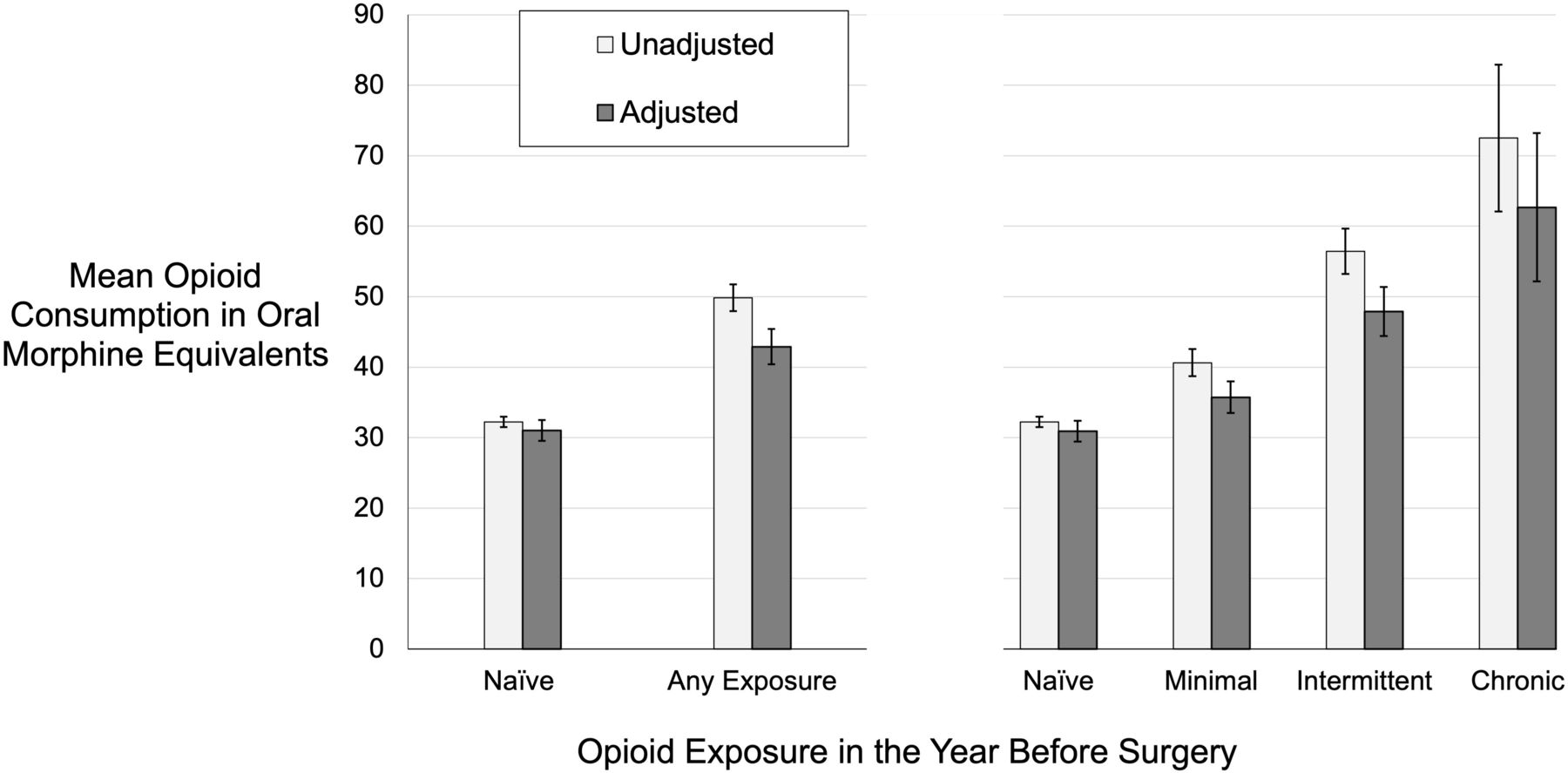
Patients with any opioid exposure in the year before surgery reported consuming greater amounts of opioids at 30 days after surgery when compared with opioid-naïve participants across all procedure types (figure 1). For unadjusted consumption, opioid exposed participants consumed more than opioid-naïve participants (median OME 25; IQR 0, 75 vs 10; 0, 50, p<0.001). Consumption was higher for opioid-exposed participants across all procedures, with the greatest differences occurring for participants undergoing hysterectomy procedures, abdominal hernia repair, and colectomy (online supplemental etable 1). After adjusting for participant, clinical, and surgical factors, participants with any opioid exposure consumed 42.9 OMEs (95% CI 40.4 to 45.3) while opioid-naïve participants consumed 31.0 OMEs (95% CI 29.5 to 32.5), resulting in a difference of 11.9 OMEs (95% CI 9.8 to 14.0) (figure 2, online supplemental etable 2). In a secondary analysis adjusting for similar factors, participants with greater opioid exposures before surgery reported consuming greater amounts of opioids at 30 days after surgery in a dose-dependent manner. Compared with opioid-naïve participants, consumption was higher among participants with minimal preoperative exposure by 4.8 OME (95% CI 2.9 to 5.8) and for intermittent exposure by 17.0 OME (95% CI 13.9 to 20.1). Chronic opioid exposure before surgery was associated with the largest increase in consumption by 31.8 OMEs (95% CI 21.3 to 42.2) compared with opioid-naïve participants. A sensitivity analysis based on the dose of opioid in the year before surgery revealed similar increases in consumption as the dose of prescription opioids increased (online supplemental etable 3). Finally, the likelihood of opioid consumption after surgery was higher for opioid-exposed compared with opioid-naïve participants (adjusted rate 57% vs 54%; adjusted OR 1.16, 95% CI 1.09 to 1.24) (online supplemental etable 4).

Patient-reported opioid consumption at 30 days after surgery by procedure type and opioid exposure status in the year before surgery, unadjusted consumption amount in first 30 days after surgery as reported by patients is unadjusted and expressed in pills of oxycodone 5 mg (7.5 oral morphine equivalents (OME)). Boxplots represent distribution of opioid consumption, with box representing 25–75th percentile, and middle line of box 50th percentile/median. For all procedures, opioid consumption at 10th and 25th percentiles was 0 pills (0 OME). A p value for overall comparison of opioid-exposed and naïve using the Mann-Whitney I test is <0.001. A p value for comparison of procedures using Kruskal-Wallis is 0.001.
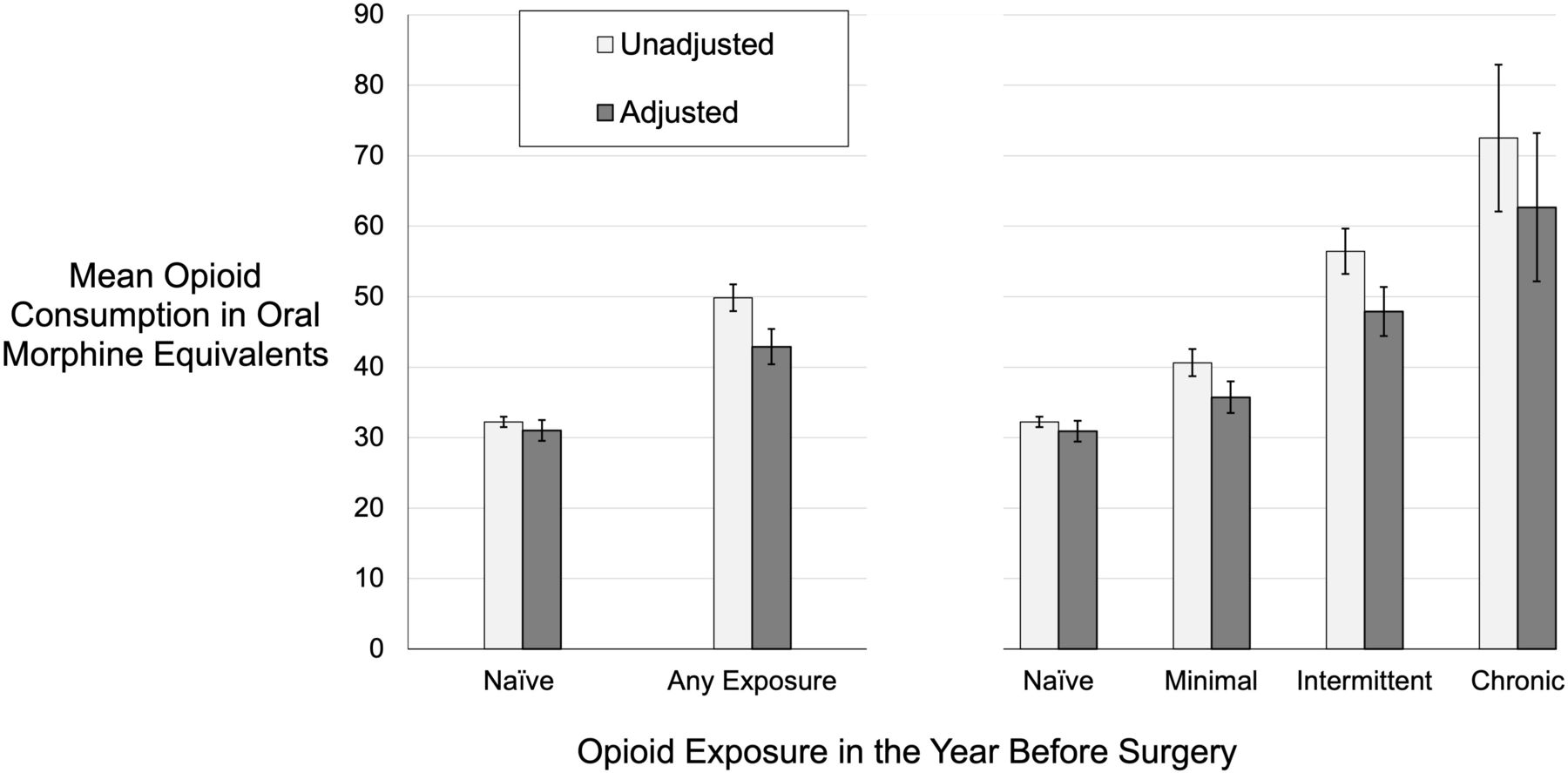
Adjusted patient-reported opioid consumption at 30 days after surgery by opioid exposure status in the year before surgery consumption amount is mean total reported opioid use and reflects adjustment in linear regression models for age, sex, race/ethnicity, insurance, American Society of Anesthesiologists physical classification, 13 other patient comorbidities, surgery type, and surgery priority. naïve indicates no opioid fills in year before surgery. bars represent 95% CIs. A p value for trend of opioid consumption by preoperative opioid exposure status is <0.001 for both unadjusted (linear-by-linear test) and adjusted groups (orthogonal polynomial contrast test). To calculate number of pills of oxycodone 5 mg, divide oral morphine equivalents (OME) by 7.5. For example, 30 OME is 4 pills of oxycodone 5 mg while 60 OME is eight pills.
Opioid Refills
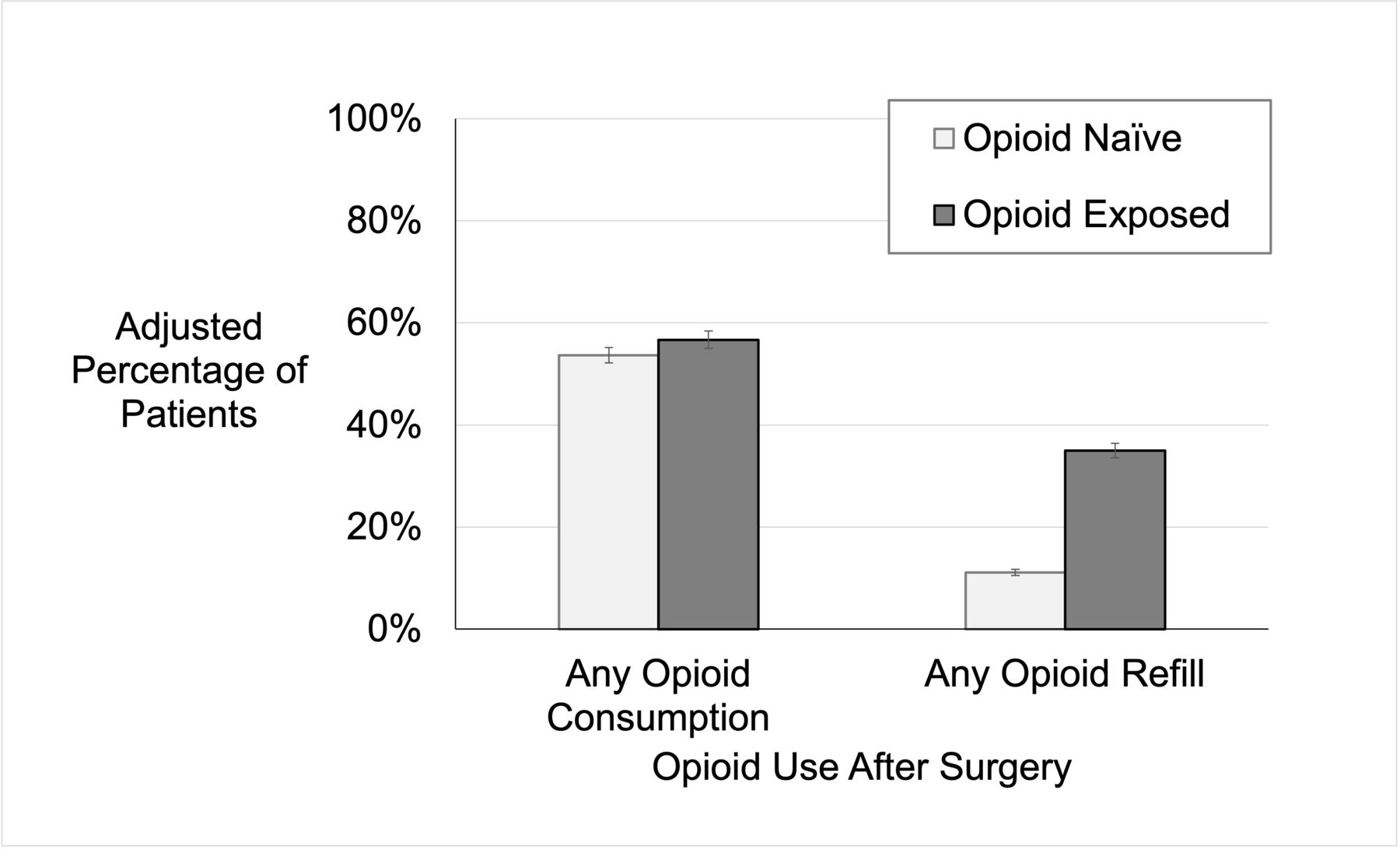
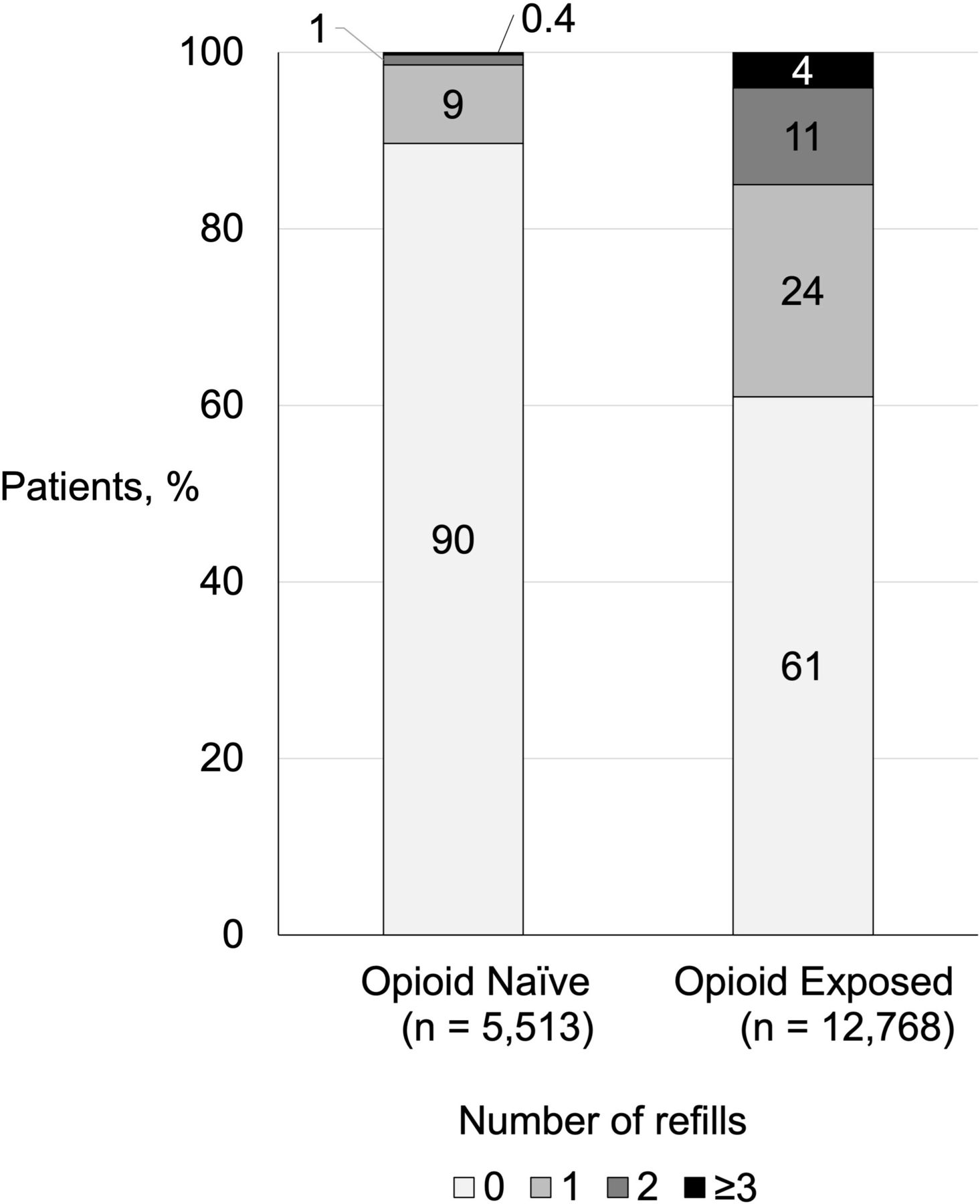
Opioid prescription refills were identified in 19% (3481/18,281) of participants who filled a perioperative prescription, and more often among opioid-exposed than opioid-naïve participants ((39%, (2167/5,513) vs 10% (1314/12,768), p<0.001). In adjusted models, the likelihood of receiving an opioid refill was also higher for opioid-exposed participants (adjusted rate 35% vs 11%; adjusted OR 4.74, 95% CI 4.36 to 5.15) when compared with opioid-naïve participants (figure 3). Opioid-exposed participants also received higher numbers of opioid prescription refills in the first 30 days after surgery (adjusted incidence rate ratio 3.97, 95% CI 3.71 to 4.25) (figure 4). Further, the average amount of opioids filled through refills was higher for opioid-exposed participants when compared with opioid-naïve participants (median OME 0, IQR 0, 200 vs 0; 0, 0, p<0.001). In adjusted models, this difference persisted (adjusted refill OME 360; 95% CI 320 to 400 vs 27; 21, 33; adjusted difference refill OME 333, 95% CI 292 to 374).

Distribution of prescription opioid refills after surgery by opioid exposure status in the year before surgery rates of consumption and refill reflect adjustment in logistic regression models for age, sex, race/ethnicity, insurance, American Society of Anesthesiologists physical classification, 13 other patient comorbidities, surgery type, and surgery priority. Naïve indicates no opioid fills in year before surgery. Bars represent 95% CIs.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of participants who refilled opioid prescriptions after surgery according to opioid exposure status in the year before surgery number of refills determined by opioid prescriptions in state prescription drug monitoring database. Results are unadjusted. For opioid naïve group, percentages without rounding add to 100%.
Discussion
In this population-based cohort study, exposure to prescription opioids in the year before undergoing general and gynecologic surgical procedures was associated with increases in the consumption of opioids as reported by participants at 30 days after surgery, as well as prescribing and refills. However, the differences varied by procedure type and preoperative opioid exposure. Compared with participants with no opioid exposure in the year before surgery, the amount of patient-reported opioid consumption after surgery was similar among those with minimal exposure (<90 pills and ≤1 month), greater for intermittent exposure, and greatest among participants with chronic opioid exposure (≥9 months). These findings suggest opioid stewardship efforts should align prescriptions with the actual use of opioids after surgery, which to date have focused primarily on opioid-naïve patients, to better meet the needs of opioid-exposed patients.
These data represent one of the first attempts at examining self-reported opioid consumption by patients with opioid exposure in the year prior to surgery, and could provide practicing clinicians with an additional resource to guide the management of postoperative pain. For example, 75% of all opioid-exposed patients used less than 17 pills. Further, 90% of opioid-exposed patients reported consuming 20 pills or less after undergoing 8 of the 9 types of procedures included in this analysis, and opioid-exposed patients accounted for two of every three refills given after surgery. Although it has been shown previously that patients with opioid exposure before surgery receive more frequent and larger postoperative opioid prescriptions, this prior work did not capture self-reported consumption of pain medication after surgery.3 9 14 Consumption of pain medication prescribed to surgical patients after discharge from surgery has previously been shown to differ markedly from self-reported consumption for opioid-naïve patients.15 Quality improvement efforts to address the oversupply of prescription opioids among opioid-naïve surgical patients have led to reductions in prescribing by 50% or more without compromising patient-reported outcomes such as pain or satisfaction.6 7 16 Achieving similar outcomes for surgical patients with prior opioid exposure is likely to require approaches that account for the additional complexities of caring for surgical patients with chronic pain who have recently or currently taken prescription opioids.17
The dose–response relationship of opioid consumption with opioid exposure may seem intuitive but has important implications for the care of surgical patients. First, opioid use and prescribing was elevated even among opioid-exposed patients without chronic use before surgery, for whom the expectation of continued use would not be high. Second, this work suggests that opioid exposure of any type has an association with higher consumption, and it is important to quantify the amount of opioid exposure in the year before surgery. For example, small opioid exposures before surgery may result in increases in consumption equivalent to one opioid pill or less, which may not equate to a clinically meaningful difference when recently developed guidelines from Michigan OPEN, the Mayo Clinic, and Johns Hopkins recommend prescribing up to ten opioid pills after many types of surgery for opioid-naïve patients.18–20 However, the same may not be true for larger opioid exposures over the course of the year prior to surgery. Additional evidence to guide opioid prescriptions at the time of discharge from surgery needs to clarify how discharge prescriptions should be modified based on opioid exposure before surgery, if at all. Surgical teams also need efficient ways to determine opioid exposure in the year before surgery through tools that efficiently integrate data from patients with queries of the PDMP, which track prescriptions for controlled substances in 49 of 50 states but lack consistent use in some surgical settings.21 22
Finally, this work reinforces the finding that patients with opioid exposure before surgery have greater and more complex comorbidities, as seen by higher ASA physical status classification scores, greater BMI, and higher diagnoses for diseases such as chronic obstructive pulmonary disease, among others. The greater burden of comorbidities aligns with prior studies showing these patients have higher baseline health risks, which reinforces the need for screening programs to identify these risks to allow for potential mitigation strategies.23 Among patients prescribed opioids, comorbidities such as obesity and chronic obstructive pulmonary disease increase the risk for respiratory depression and compromise, and lead to differences in the dose response curves with respect to analgesia and respiratory depression.24 It is possible that patients with higher opioid exposure may require higher doses to achieve pain relief, but with markedly increased risk of respiratory depression. As such, prescribing for these vulnerable individuals requires careful consideration, including care coordination and risk mitigating strategies, such as coprescribing with naloxone.
This study should be placed in the context of several limitations. First, these associations should not be classified as causal, though this represents one of the largest studies with patients reporting actual consumption after surgery, and multiple measures of preoperative opioid exposure suggest greater postoperative opioid utilization. Second, unmeasured confounding may be present, though adjusted models account for several relevant patient, clinical, and operative variables. Third, data on consumption of opioids relies on patient report, which has the potential to differ from actual use. In response, we employed the novel capture of data on controlled substance use by linking surgical and PDMP data. This permitted identification of discrepancies in opioid prescription fills as reported by patients and those as cataloged in the PDMP, with such patients excluded from the study. Fourth, the analysis occurs in the context of a dynamic surgical quality collaborative with robust efforts to modify opioid prescribing at discharge from surgery, with such efforts resulting in significant reductions of prescription opioids that may attenuate differences in utilization for opioid-naïve and opioid-exposed surgical patients.7 8
Conclusion
In a large cohort of patients undergoing general and gynecologic surgery, exposure to prescription opioids in the year before surgery was associated with higher opioid consumption after surgery. Further, higher consumption was identified among patients with higher preoperative opioid exposures in a dose-dependent manner. Opioid exposure in the year before surgery represents a critical characteristic that should be considered when crafting opioid stewardship efforts to optimize opioid prescribing for the treatment of acute pain in the context of surgery.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
The University of Michigan Institutional Review Board approved this study of deidentified data as exempt from review and did not require the need for participant consent.
Acknowledgments
Drs Bicket and Gunaseelan had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @MarkBicket, @drchadb
Contributors MCB and VG contributed to planning, designing, and conducting the study, data analysis, drafting, revising, and submitting the manuscript. MCB and VG act as guarantor. PL, ACF, AB, EA, and MS contributed to conducting the study, data interpretation, drafting, and revising the manuscript. MJE, CMB, and JFW contributed to the planning, designing, and conducting the study, data analysis, drafting, and revising the manuscript.
Funding MCB reports grants from the National Institutes of Health (R01DA042859, R01DA044987, R01DA049789), the Arnold Foundation, Michigan Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, and the US Centers for Disease Control and Prevention during the conduct of the study, and serving as consultant for Axial Healthcare and Alosa Health outside the submitted work. JFW receives funding from Michigan Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, and the Centers for Disease Control and Prevention. CMB receives funding from Michigan Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, and the Centers for Disease Control and Prevention. CMB is also supported by NIAMS P50 AR070600, NIDA R01DA038261, NIDA R01DA042859, and Common Fund UM1 NS118922. He also serves as a consultant for Heron Therapeutics, Vertex Pharmaceuticals, and Alosa Health, and provides expert medicolegal testimony.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH, MDHHS, or SAMHSA.
Competing interests MCB has received consulting fees from Axial Healthcare and Alosa Health. CMB has served as a consultant for Heron Therapeutics, Vertex Pharmaceuticals, and Alosa Health, and provides expert medicolegal testimony. Otherwise the authors declare no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.