Article Text

Abstract
Background Evidence regarding the role of cannabinoids in managing acute postoperative pain is conflicting. The purpose of this systematic review and meta-analysis was to determine the analgesic efficacy of perioperative cannabinoid compounds for acute pain management after surgery.
Methods Original research articles evaluating the addition of cannabinoids to standard opioid-based systemic analgesia (Control) in the postoperative period were sought. Our primary outcomes were cumulative oral morphine equivalent consumption and rest pain severity at 24 hours postoperatively. We also assessed analgesic consumption in the postanesthesia care unit (PACU), pain scores in PACU, 6 and 12 hours postoperatively, and opioid-related and cannabinoid-related side effects, patient satisfaction, and quality of recovery as secondary outcomes.
Results Eight randomized controlled trials (924 patients) and four observational studies (4259 patients) were analyzed and included. There were insufficient data to pool for quantification of differences in cumulative oral morphine equivalent consumption and rest pain severity at 24 hours postoperatively with the addition of cannabinoids in comparison to Control. Qualitative synthesis revealed no differences in cumulative oral opioid consumption or pain at rest 24 hours postoperatively with the addition of cannabinoids in comparison to Control. Patients receiving cannabinoids appeared to have an increased weighted mean difference 95% CI of pain at 12 hours by 0.83 cm (0.04 to 1.63) (p=0.04). Patients receiving cannabinoids also appeared to have 3.24 times increased odds of developing hypotension postoperatively (95% CI 1.12 to 9.36) (p=0.03). Qualitative and quantitative synthesis revealed no differences in any other secondary outcomes.
Conclusions Our quantitative and qualitative review of the literature suggests that the analgesic role of perioperative cannabinoid compounds is limited, with no clinically important benefits detected when cannabinoids are added to traditional systemic analgesics compared with traditional systemic analgesics alone. Notably, there appears to be a signal towards increased postoperative pain and hypotension associated with the addition of perioperative cannabinoids to traditional systemic analgesics. These results do not support the routine use of cannabinoids to manage acute postoperative pain at the present time.
- acute pain
- alternative therapies
- pain medicine
- regional anesthesia
Statistics from Altmetric.com
Background
The global opioid crisis has prompted a clear and present urgency to find alternative strategies to treat acute postsurgical pain. In addition to traditional systemic analgesic adjuncts such as acetaminophen, non-steroidal anti-inflammatories, and gabapentinoids, novel alternatives such as N-methyl-D-aspartate receptor antagonists, alpha-2 adrenergic agonists, glucocorticoids, and selective serotonin reuptake inhibitors are increasingly used in the perioperative setting to spare or avoid opioids. Attention has recently turned to cannabinoids as the key chemical components of cannabis, namely tetrahydrocannabinol (THC) and cannabidiol (CBD), have been shown to produce antinociceptive effects.1–3 While evidence accumulates in support of cannabinoids for the management of chronic pain,4–6 the available literature regarding the analgesic efficacy of cannabinoids for acute postsurgical pain is conflicting.7 Therefore, we performed a systematic review and meta-analysis to evaluate analgesic outcomes in patients receiving cannabis compounds for acute pain management in the surgical setting.
Methods
This systematic review was prepared in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement guidelines. The review was not registered with The International Prospective Register of Systematic Reviews (PROSPERO) under the number. We sought all quantitative and observational studies involving adult patients receiving cannabinoids for acute postoperative analgesia and evaluated these studies using a predesigned protocol. The review was not registered with PROSPERO.
Eligibility criteria
Any observational or quantitative original research articles involving adult patients (≥18 years old) comparing the addition of any cannabinoid or cannabinoid containing product to Control (standard opioid-based unimodal (opioids only) or multimodal (combination of opioids and other adjuvants) systemic analgesia) for the purposes of acute postoperative pain management were considered for inclusion. Observational studies in adult patients who were chronically prescribed cannabinoids were also considered for inclusion provided that they evaluated their impact on acute postoperative analgesia. All types of surgeries were considered including cardiac, dental, general, neurological, orthopedic, urologic, and vascular. All routes of administration and dosages of cannabinoids were also considered for inclusion. We excluded research articles evaluating the effects of cannabinoid use on cancer, chronic, and neuropathic pain. No language restrictions were placed on study inclusion, and non-English trials were translated using an online translator.
Search methods
A systematic search strategy was created by an evidence-based medicine librarian (EM) for the following databases: US National Library of Medicine database (MEDLINE); the Cochrane Database of Systematic Reviews; and the Excerpta Medica database (EMBASE). The search strategy was designed to capture articles from database inception to September 1, 2019. The medical subject headings (MeSH) and keywords used in the development of the search strategy consisted of terms relevant to the central research question and revolved around the following key domains: cannabinoid, marijuana, surgery, pain, analgesia, and pain control. The complete search strategy for the MEDLINE database can be viewed in online supplementary appendix A; all subsequent search strategies were based on the results generated by the initial MEDLINE search. We also hand-searched the citation list and bibliographies of all included articles to identify any other potentially eligible observational or quantitative studies, as well as the published abstracts of the following international meetings: American Society of Anesthesiologists (ASA) 2011–2018, American Society of Regional Anesthesia and Pain Medicine (ASRA) 2013–2018, the European Society of Regional Anesthesia (ESRA) 2014–2018, and the European Society of Anesthesiology (ESA) 2015–2018. Finally, the clinical trial registry (www.clinicaltrials.gov) was also searched, and authors of potentially eligible ongoing or completed investigations were contacted for additional data.
Supplemental material
Selection of included studies
Two independent reviewers (FA and NH) reviewed the title and abstracts of the citations generated from the systematic search strategy. Subsequently, both reviewers then assessed the full-text versions of all potentially eligible citations; any disagreements between the two reviewers on full-text eligibility were discussed until an agreement was reached. In situations when an agreement could not be reached, a third reviewer (RB), assessed the study in question and made the final decision.
Data extraction
A standardized data extraction form was created and piloted by an independent reviewer (NH). Data were subsequently extracted in duplicate by two independent reviewers (NH and TW). The data extraction form specifically collected information regarding the following variables: year of publication; age of participants; type of surgery performed; nature of primary outcome investigated; preoperative, intraoperative, and postoperative analgesic regimens; nature of investigated cannabinoid (compound, dose, route of administration, and preoperative and/or postoperative regimen); postoperative pain scores; interval postoperative opioid consumption; level of satisfaction with pain relief; opioid-related and cannabinoid-related side effects; and quality of recovery.
The primary source of all data was the numerical values reported in the tables and figures of the source articles. Any data reported in graphical form was extracted with a graph digitizing software (GraphClick, Arizona Software, USA). The corresponding authors of the source articles were contacted if additional methodological trial information and outcome data were needed.
Assessment of methodological quality of individual studies
Risks of bias assessments were performed using specific critical appraisal tools, which varied, based on study design. The methodological quality of randomized controlled trials was assessed using the Cochrane Collaboration’s Risk of Bias questionnaire.8 Items in this questionnaire evaluate various methodological aspects including quality randomization (generation and concealment); blinding of study investigator, patients, and outcome assessors; loss to follow-up; and degree selective outcome data reporting and each is rated as having low, unclear, or high risk of bias.8 The methodological quality of observational studies was assessed using the Newcastle-Ottawa Scale (NOS).9 Items in this scale evaluate case selection, case-control comparability, and exposure or outcome assessment.9 This method uses a “star system” to denote higher quality observational studies with regard to selection, comparability of study participants, and outcome assessments. The following factors were evaluated: case definition (one star); representativeness of cases (one star); control definition (one star); control selection (one star); comparability of cases and controls on basis of design or analysis (two stars); ascertainment of exposure (one star); same method of ascertainment (one star); and non-response rate (one star).9 The NOS rating was then converted to conform with Agency for Healthcare Research & Quality standards for study quality (ie, poor, fair, or good). A poor quality study received either no or one star in the selection domain, no stars in the comparability domain, or no star in the outcome domain; a fair quality study received two stars in the selection domain, one or two stars in the comparability domain, and two or three stars in the outcome domain; and a good quality study received three or four stars in selection domain, one or two stars in the comparability domain, and two or three stars in the outcome domain.9 Finally, a risk of bias assessment was not performed for any case study included in this review given that there are no well-established risk of bias assessment tools.
Two independent reviewers (FA and NH) evaluated each factor/domain for all included research articles. Any disagreements on risk of bias assessment were discussed until a decision was reached. In situations when a decision could not be reached, a third reviewer (RB) assessed the trial in question and made the final decision.
Assessment of methodological quality of individual outcomes
The quality of evidence across all statistically pooled outcomes in this review were evaluated using the guidelines created by Grades of Recommendation, Assessment, Development, and Evaluation (GRADE).10 11 (i) These guidelines rate the quality of evidence for each outcome as high quality, that is, further research is very unlikely to change the confidence in the estimate of effect; (ii) moderate quality, that is, further research is very likely to have an important impact on the confidence of the estimate of effect and may change the estimate; (iii) low quality, that is, further research is very likely to have a significant influence on the confidence in the estimate of effect and is likely to alter the estimate; or (iv) very low quality, that is, there is uncertainty surrounding the estimate.10 11 These ratings are based on criteria pertaining to study quality, consistency, directness, precision, and degree of publication bias.11
Primary and secondary outcomes
We designated two coprimary analgesic outcomes for this review, namely, (i) analgesic consumption, as measured by cumulative oral morphine equivalent consumption (mg) during the first 24 hours time interval and (ii) rest pain severity, as measured by Visual Analog Scale (VAS) pain scores, at 24 hours postoperatively.
The secondary analgesic outcomes in this meta-analysis were cumulative postoperative oral morphine equivalent (mg) during the postoperative anesthesia care unit (PACU) stay and during the 24–48-hour time interval; postoperative rest pain severity (VAS) in PACU (0–2 hours), 6, and 12 hours; patient satisfaction; and quality of recovery (QoR), as measured by a validated questionnaire such as the ambulatory surgery QoR questionnaire.12 For safety outcomes, we sought opioid-related side effects (postoperative nausea and vomiting, excessive sedation, respiratory depression, pruritus, hypotension, urinary retention) and cannabinoid-related side effects (increased awareness, drowsiness, dry mouth, palpitations, change of mood, difficulty with memory, slurring of speech, blurred vision, dizziness, hallucinations, headache, involuntary muscle twitching, change in behavior and tremor).13 14
Measurement of outcome data
In order to facilitate analysis, we converted all reported opioid consumption dosage data into oral morphine equivalents (mg).15 For all rest pain severity outcome data, all pain scores were converted to an equivalent score on a 0–10 cm VAS pain scale (0 cm=no pain, 10 cm=worst pain imaginable).16 Patient satisfaction outcome data were also converted to a 0–10 cm VAS scale score (0 cm=least satisfied, 10 cm=most satisfied).16 Finally, any quality of recovery outcome data were converted to an equivalent score on the QoR questionnaire.16 17
Statistical analysis
For all continuous outcomes in this review, a mean and SD was extracted. In situations where these values were unavailable, the median and IQR were used as an approximation.18 If required for statistical pooling, all dichotomous data were converted to continuous data in the form of a mean and SD.19 For instances where a 95% CI was reported, the value was converted to a SD.20 The value of the SD was imputed if a measure variation (ie, SD, CI, or IQR) was not provided by the included study,19 and the median was used to approximate the mean in situation where the mean could not be derived. For all dichotomous outcomes in this review, data were converted to overall incidence numbers.
Meta-analysis
Data were pooled only if available from three or more research articles; otherwise, we qualitatively summarized the results in situations when data from less than three articles were available. In situations when continuous data could be statistically pooled, we used the inverse variance method with random-effects modeling since we anticipated the presence of clinical heterogeneity between the included articles. Similarly, when dichotomous outcome data could be pooled, the Mantel-Haenszel random-effects model was used.21
For the primary outcomes of this review, namely cumulative oral morphine equivalent consumption (mg) and rest pain severity (VAS) at 24 hours postoperatively, a weighted mean difference (WMD) with a 95% CI was calculated. For the continuous secondary outcomes of this review, namely VAS pain scores in PACU (0–2 hours), 6 and 12 hours, cumulative postoperative oral morphine equivalent (mg) during the PACU stay and during the 24–48-hour time interval, patient satisfaction, and quality of recovery (QoR), a WMD with a 95% CI was also calculated. For the dichotomous secondary outcomes of this review, namely opioid related side-effects and cannabinoid-related side effects, an OR with a 95% CI was calculated. For the two coprimary outcomes of this review, our threshold for significance was p<0.025. For the secondary outcomes of this review, p<0.05 was considered significant. All tests of significance were two-tailed.
Exploration of heterogeneity
An I 2 statistic was used to assess heterogeneity between research articles included in the pooled estimates. We considered an I 2 value greater than 40% in the pooled estimate to be indicative of significant heterogeneity, as suggested by the Cochrane Handbook for Systematic Reviews.20 In situations where heterogeneity exceeded our predefined threshold, we conducted meta-regression analysis using mixed effects modeling to explore whether a priori specified clinical predictors influenced the estimates of effect in our primary outcomes. Meta-regression was performed only if each subgroup within a covariate/clinical predictor included at least two articles. The following covariates were used in meta-regression analysis: (i) type of surgery (elective vs in-hospital);22 23 (ii) type of cannabinoid compound used (synthetic versus isolated natural compound); (iii) timing of cannabinoid administration (preoperative versus postoperative versus both preoperative and postoperative); (iv) dosing schedule of cannabinoid (single dose versus multiple doses), (v) opioid naivety (opioid naïve vs opioid exposed patients). For each covariate, a coefficient of determination (R2) was calculated which ranges between 0 and 1; a value of 0 means that 0% of the model is explained by the covariate, while a value of 1 means that 100% of the model is explained by the covariate.24 Sensitivity analysis was performed by sequentially excluding research articles with the above co-variates in situations where meta-regression analysis could not be performed (ie, <2 trials available for specific covariate).
Assessment of publication bias
We assessed the risk of publication bias in the two coprimary outcomes of this review using the Egger’s regression test25 and also by visual inspection of a funnel plot. In situations of low risk of publication bias, the funnel plot should generally take the shape of a symmetrical, inverted funnel.20
Data management
The forest and funnel plots created for this review were generated using Review Manager Software (RevMan V.5.2; Nordic Cochrane Centre, Cochrane Collaboration). Meta-regression analysis was performed using Comprehensive Meta-Analysis 3.0 (Engelwood, USA).
Results
The primary literature search identified 121 unique citations whereas hand-searching of abstracts from international conference proceedings identified one potentially eligible citation. An additional review of registered trials (www.clinicaltrials.gov) did not identify any potentially eligible citations. Thus, from the primary literature screen based on title and abstract alone, a total of 107 citations did not satisfy the inclusion criteria and were excluded from our review. Reasons for exclusion included: lack of intervention of interest (n=96), investigation limited to impact of cannabinoids on chronic cancer or noncancer pain (n=5), and nonoriginal (ie, review) article (n=6). The remaining 15 citations had their full-text versions retrieved for assessment of eligibility, and of these, three were excluded (chronic cancer or noncancer pain, n=1); author reply to an existing article, n=2). As a result, a total of 12 original research articles13 14 26–35 were included in this systematic review and meta-analysis. Among the 12 articles included herein, eight13 14 26 29 31–34 were randomized controlled trials and four27 28 30 35 were observational studies. The flow diagram for study inclusion is presented in figure 1.
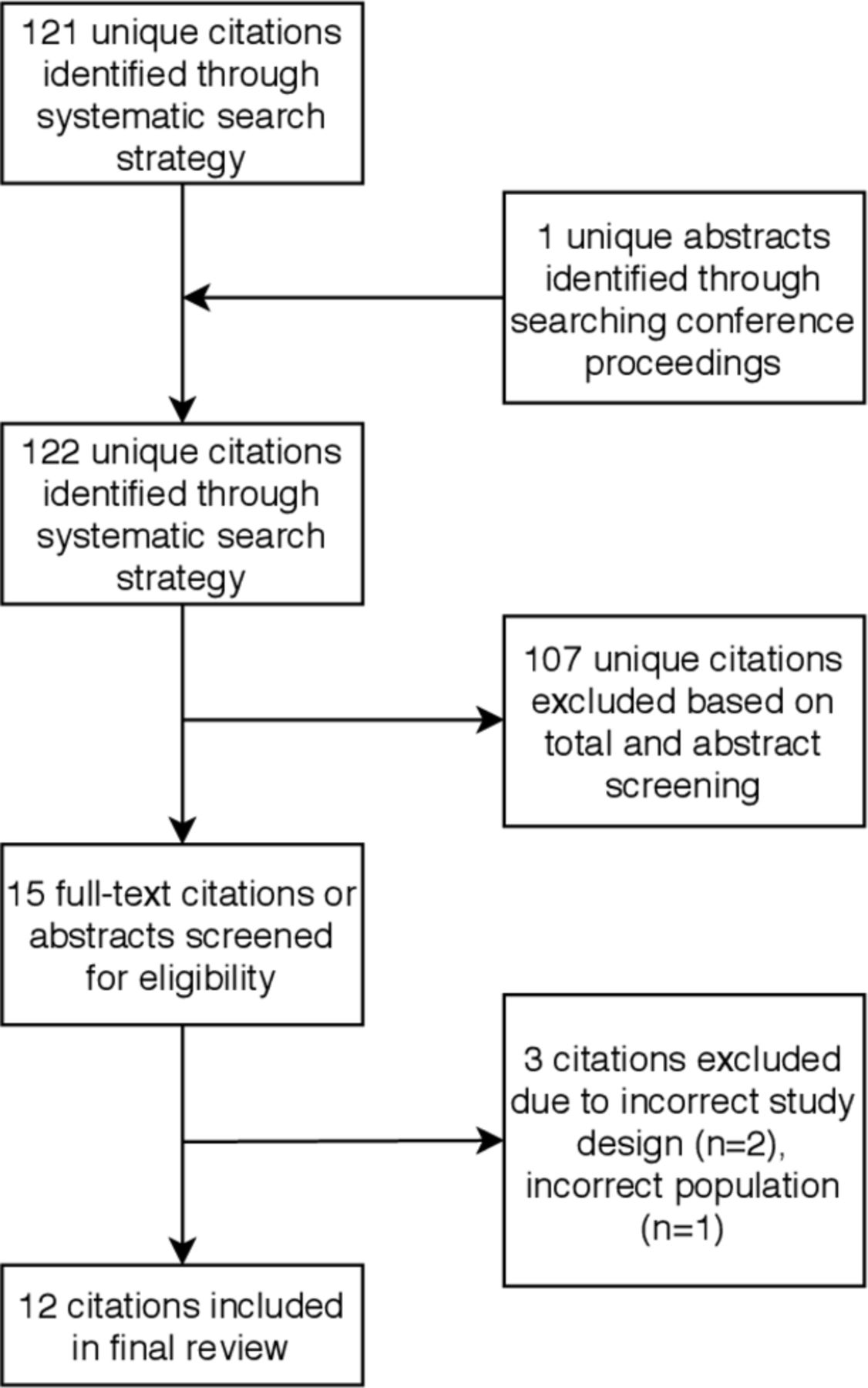
Study flow diagram.
Study characteristics
The study characteristics and information regarding analgesic outcomes assessed are presented in table 1. A total of 924 patients were investigated within the eight randomized trials,13 14 26 29 31–34 among which 470 patients received cannabinoids for acute postoperative analgesia and 454 patients received Control. A total of 4259 patients were investigated within the four observational studies,27 28 30 35 among which 373 patients either had received or were existing users of cannabinoids and 3886 patients received Control. A wide variety of surgical procedures were examined for which cannabinoids were used to treat acute postoperative pain, including abdominal,13 14 pelvic,34 dental,31 33 orthopedic,27 30 35 and other various surgical procedures.26 28 29 32 A primary outcome of interest was clearly specified by 713 26 27 31–33 35 of the 12 research articles. Eleven of the 12 articles each reported to have assessed postoperative pain severity13 14 26–29 31–35 and opioid consumption.13 14 26–28 30–35
Study characteristics and outcomes of interest assessed in included studies
The types of the cannabinoid compounds used to treat acute postoperative pain varied across all articles included in this review (table 2). For example, −9-Tetrahydrocannabinol was used by three13 28 34 articles, Levonantradol by two,14 29 Nabilone by two,26 32 and Dronabinol by one.27 Two research articles31 33 used investigational compounds under development and another two30 35 used various oral edible cannabis or cannabinoid oil-containing compounds. Besides the variability of compounds, the purity and THC:CBD ratio of the studied compounds was not specified, except in one article, wherein it ranged from 1:0.3 to 1:0.5.28 Similarly, the doses, routes of administration, timing, and frequency varied among the research articles. Specifically, the doses used ranged between1.5 mg and 800 mg. Moreover, 10 of the 12 articles examined the oral (PO) route13 26–28 30–35 while 214 29 articles used the intramuscular (IM) route. Cannabinoid compounds were administered preoperatively in four articles,29 31–33 postoperatively in four articles,13 14 27 28 while two articles used a combination of both preoperative and postoperative cannabinoids.26 34 A variety of coanalgesic regimens were also used; unimodal opioid-based analgesia was used in four articles,13 26 28 34 multimodal analgesia in four articles,14 27 31 33 while four articles29 30 32 35 used an unspecified multimodal analgesic regimen. Finally, two articles30 35 included patients who were chronic cannabinoid users.
Details of cannabinoid and analgesic regimens used in included studies
Risk of bias assessment
The risk of bias assessment for all randomized trials and observational studies included in this review is presented in figure 2. For the randomized trials, three32–34 studies adequately described the methods used for randomization and were rated as having a low risk of selection bias; in contrast, the remaining five studies13 14 26 29 31 did not provide sufficient details and were rated as having an unclear risk of bias. In regard to blinding, five studies13 26 32 33 concealed subject allocation from study participants, personnel, and outcome assessors and were rated as having a low risk of performance and detection bias. The remaining three studies14 29 34 did not provide sufficient details regarding the level of blinding and had an unclear risk of performance and detection bias. Six studies13 26 31–34 reported a <20% loss to follow-up or accounted for missing patients and thus were at a low risk for attrition bias. In contrast, two studies14 29 did not provide sufficient information on missing study participants and were at an unclear risk for attrition bias. Finally, only one study33 was rated as having a low risk of reporting bias given that it was preregistered with a clinical trial registry and had a full-text protocol available for review; the remaining seven studies13 14 26 29 31 32 34 were rated as having an unclear risk of reporting bias.

{kind=link}
{kind=link}
Risk of bias assessment for (A) randomized controlled trials using the Cochrane collaboration risk of bias tool and (B) qualitative trials using the Newcastle Ottawa score.
For the observational studies included in this review, all four27 28 30 31 35 were rated as being of good quality per the NOS rating scale given that they had adequate methods for case selection, comparability, and outcome assessment.
Primary outcomes
Cumulative oral morphine equivalent consumption at 24 hours postoperatively
Only two randomized trials26 34 inclusive of 153 patients (Cannabinoid: 72, Control: 74) provided data on this outcome, thereby precluding statistical pooling and meta-regression analysis. Neither trial26 34 found a significant difference in oral morphine equivalent consumption at 24 hours in patients who received cannabinoid compounds versus Control.
Only two observational studies27 35 inclusive of 4052 patients (Cannabinoid: 237, Control: 3815) provided data on this outcome, thereby precluding statistical pooling. Neither study27 35 found a significant difference in oral morphine equivalent consumption at 24 hours in patients prescribed cannabinoid compounds vs Control.
Rest pain scores at 24 hours postoperatively
Only two randomized trials26 34 inclusive of 146 patients (Cannabinoid: 72, Control: 74) assessed provided data on this outcome, thereby precluding statistical pooling and meta-regression analysis. One trial34 reported that perioperative cannabinoid did not produce a difference in VAS pain score at 24 hours; however, the other reported that perioperative cannabinoid was associated with increased pain during the same time interval in comparison to Control.26
Only two observational studies27 35 inclusive of 4052 patients (Cannabinoid: 237, Control: 3815) provided data on this outcome, thereby precluding statistical pooling. Neither study27 35 found a significant difference in VAS pain scores at 24 hours.
Secondary outcomes
Interval rest pain severity scores
The number of randomized trials that provided data for this outcome varied across each time point, with seven at PACU stay,13 14 27 30 32 33 35 six at 6 hours,13 14 27 30 32 35 and three at 12 hours.27 34 35 Patients receiving cannabinoids had worse pain at 12 hours by a WMD (95% CI) of 0.83 (0.04 to 1.63) (p=0.04, I 2 =72%).26 33 34 No statistically significant differences were detected in rest pain severity at any other measured time interval (table 3). The quality of evidence was moderate for each of these time intervals given significant heterogeneity in the pooled estimate.
Secondary outcome results
Reported side effects
For the observational studies, only one study27 inclusive of 259 patients (Cannabinoid: 81, Control: 178) assessed this outcome, thereby precluding statistical analysis. No significance difference was found in pain at rest during the PACU stay.28 None of the included observational studies assessed postoperative pain at 6 or 12 hours.
Oral morphine equivalent consumption during PACU stay
Only three randomized trials26 32 34 inclusive of 486 patients (Cannabinoid: 244, Control: 242) provided data on this outcome that allowed for statistical pooling. Perioperative cannabinoid did not reduce oral morphine equivalent consumption during the PACU stay compared with Control, with a WMD (95% CI) of 1.12 (–4.71 to 6.94) (p=0.71, I 2 =91%) (table 3). The quality of evidence was moderate for this outcome given significant heterogeneity in the pooled estimate.
Only one observational study27 inclusive of 259 patients (Cannabinoid: 81, Control: 178) assessed this outcome and reported oral morphine equivalent consumption during PACU stay, thereby precluding statistical pooling. No significance difference was found between the two groups.
Cumulative oral morphine equivalent consumption between 24 and 48 hours postoperatively
Among the randomized trials, none assessed oral morphine consumption during the 24–48-hour time interval.
Only two observational studies27 30 inclusive of 401 patients (Cannabinoid: 152, Control: 249) provided data on this outcome, thereby precluding statistical pooling. Neither study27 30 found a significant difference in oral morphine equivalent consumption during the 24–48-hour time interval.
Quality of recovery
None on the included randomized trials or observational studies assessed this outcome.
Patient satisfaction
None on the included randomized trials or observational studies assessed this outcome.
Opioid-related side effects
None on the included randomized trials or observational studies assessed this outcome.
Cannabinoid-related side effects
All eight randomized trials13 14 26 29 31–34 inclusive of 924 patients (Cannabinoids: 470, Control: 454) reported side effects related to cannabinoids. The most common side effects reported were blurred vision, hypotension, dizziness, drowsiness, dry mouth, hallucinations, headache, and nausea. Patients receiving cannabinoids had 3.24 times increased odds of developing hypotension in the postoperative period (95% CI 1.12 to 9.36) (p=0.03, I 2 =41%). Statistical pooling detected no significant differences in the remaining cannabinoid-related side effects (table 4).
Three observational studies27 28 35 inclusive of 4117 patients (Cannabinoids: 302, Control: 3815) reported side effects related to cannabinoids. Commonly reported side effects included nausea and vomiting and sleep disturbance; however, each side effect was reported by less than three studies which precluded statistical pooling (table 4).
Discussion
The results of this systematic review and meta-analysis suggest that the addition of cannabinoid-based compounds to standard systemic analgesia for acute postoperative pain management does not impact analgesic outcomes. More specifically, the best available qualitative evidence suggests no differences in cumulative opioid consumption and no differences in the severity of rest pain at 24 hours postoperatively. However, evidence appears to signal increased pain in patients receiving cannabinoids at 12 hours postoperatively. There also appears to be evidence of an increased odds of hypotension in the postoperative period. Although our review found no evidence of benefit when patients received cannabinoid compounds, there may be a signal towards increased risk with its use, as orthostatic hypotension itself is a risk factor for cerebrovascular disease.36
Previous systematic reviews on this topic4 7 37 have been limited by lack of statistical pooling and a comprehensive evaluation of analgesic outcomes over time. Specifically, evidence from previous reviews were limited by (i) mixing heterogenous patient populations (ie, chronic pain, acute pain, cancer pain);4 37 (ii) lacking a statistical assessment of postoperative analgesic outcomes;7 and (iii) an inability to quantify the adverse event profile of perioperative cannabinoid compounds.4 7 37 In contrast, our review provides new insight into the limited role of cannabinoid compounds for acute postoperative analgesia and is the first to perform statistical pooling of postoperative pain scores and analgesic consumption.
Analgesic efficacy of cannabinoid compounds previously demonstrated in patients suffering from chronic pain conditions, such as chronic non-cancer pain,38 39 painful HIV-associated peripheral neuropathy,40 and chronic rheumatic pain41 may be due to neuroplastic changes that occur over time, such as (i) an upregulation of the cannabinoid receptor, CB1 and CB2 42 43; (ii) alteration of cannabinoid receptor function;44 and (iii) the release of endogenous cannabinoids (anandamide and 2-arachidonoylglycerol).45 Although these changes have been proposed to occur in the chronic setting, their relevance in the acute setting is likely limited which may help to explain our findings. Further, unlike chronic pain, which is dynamic and often neuropathic in nature, acute postoperative pain is often localized, resulting from the release of inflammatory mediators, and is nociceptive in nature,46 47 which may also help explain the lack of differences in acute pain outcomes detected herein. Indeed, current investigation in healthy volunteers has suggested a limited role of cannabis for acute nociceptive pain.48
Two noteworthy findings of this review were increased pain at 12 hours postoperatively and the increased odds of hypotension detected in patients receiving cannabinoids. The delayed worsening of acute postoperative pain has been suggested earlier, although with limited evidence. Specifically, it has been found that increasing dosage of cannabinoids results in significantly increased pain49 50 and possibly opioid consumption.50 This paradoxical response appears to be directly related to the dosage of cannabinoids and follows a biphasic distribution, with higher doses leading to increased pain.49 On the molecular level, there also appears to be signal corroborating this finding; CB1 activation may lead to reduced inhibitory neurotransmitters and an increased intensity of even non-painful signals.51 The biphasic response also appears to occur at the level of the autonomic nervous system, with lower doses stimulating the sympathetic nervous system, possibly leading to tachyarrhythmias, and higher doses stimulating the parasympathetic nervous system, possibly leading to bradycardia and hypotension.52 53 This effect of cannabinoids on the autonomic nervous system may explain the recently reported increased odds of postoperative myocardial infarction in active users.54 Although our review was unable to conduct additional analysis on dose-dependent changes due to limited evidence, such observations warrant additional investigations before practice recommendations are made.
Strengths and limitations
Our review has several notable strengths. First, our literature search was exhaustive and included non-English trials and published abstracts. Second, in contrast to the prior reviews on the topic, we were able to successfully pool across analgesic outcomes and provide estimates of effect for commonly reported safety outcomes. Third, the majority of the randomized trials included in this review were characterized by a low risk of bias and all observational studies were deemed to be of ‘good’ quality, thereby improving the external validity of our review.
Our review also comes with limitations related to the quality of evidence available and the research methods we used. First, the optimal dose, route of administration, perioperative timing, frequency and relative ratio of THC and CBD in the cannabinoid compounds used for acute pain is largely unknown.55 Among all studies included in our review, only one28 provided details regarding the THC:CBD ratio of the investigated compound. Second, the evidence on long-term harms and adverse events of acute cannabinoid compound has not been adequately captured in any of the studies examined.56 Indeed, many dried cannabinoid compounds have THC concentrations of 15% or greater;57 and the THC component in these compounds has been found to be associated with addiction potential and harmful side-effects. Third, none of the included studies13 14 26 29 31–34 used multimodal analgesia inclusive of central neuraxial or peripheral nerve blockade. From a methodological perspective, we were unable to statistically pool across both of our primary outcomes (analgesic consumption and rest pain scores at 24 hours) due to limited reporting across all research articles. As a result, we were also unable to assess for risk of publication bias for our primary outcomes. Furthermore, outcomes that we were able to successfully pool were characterized by a high level of heterogeneity. These were likely due to (i) the variations in the cannabinoid compounds used, including the dose route and timing of administration and (ii) the variation in the surgical procedures performed. Additionally, many of the articles included had small sample sizes which may affect the quality and external validity of our estimates of effect. Finally, we were unable to provide pooled estimates of effects for the important outcomes of opioid related side-effects and QoR. It is entirely possible that perioperative cannabinoids impact the emotional aspects of pain and thereby QoR without affecting subjective pain scores; however, we were unable to assess this question in our review.
Conclusion
Our quantitative and qualitative review of the literature suggests that the analgesic role of perioperative cannabinoid compounds is limited, with no clinically important benefits detected when cannabinoids are added to traditional systemic analgesics compared with traditional systemic analgesics alone. Notably, there appears to be a signal towards increased postoperative pain and hypotension associated with the addition of perioperative cannabinoids to traditional systemic analgesics. These results do not support the routine use of cannabinoids to manage acute postoperative pain at the present time.
References
Footnotes
FWA and NH are co-primary authors.
Twitter @Faraj_RegAnesth
Contributors All authors contributed to the final manuscript and played an active role in development.
Funding FWA receives research time support from the Department of Anesthesiology and Pain Medicine, and the Ottawa Hospital Research Institute, University of Ottawa. RB receives research time support from the Evelyn Bateman Cara Operations Endowed Chair in Ambulatory Anesthesia and Women’s Health, Women’s College Hospital, Toronto, Ontario, Canada.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.