Article Text

Abstract
Background and objectives At our institution, we developed an individualized discharge opioid prescribing and tapering protocol for joint replacement patients and implemented the same protocol for neurosurgical spine patients. We then tested the hypothesis that this protocol will decrease the oral morphine milligram equivalent (MME) dose of opioid prescribed postdischarge after elective primary spine surgery.
Methods In this retrospective cohort study, we identified all consecutive elective primary spine surgery cases 1 year before and after introduction of the protocol. This protocol used the patient’s prior 24-hour inpatient opioid consumption to determine discharge opioid pill count and tapering schedule. The primary outcome was total opioid dose prescribed in oral MME from discharge through 6 weeks. Secondary outcomes included in-hospital opioid consumption in MME, hospital length of stay, MME prescribed at discharge, opioid refills, and rates of minor and major adverse events.
Results Eighty-three cases comprised the final sample (45 preintervention and 38 postintervention). There were no differences in baseline characteristics. The total oral MME (median (IQR)) from discharge through 6 weeks postoperatively was 900 (420–1440) preintervention compared with 300 (112–806) postintervention (p<0.01, Mann-Whitney U test), and opioid refill rates were not different between groups. There were no differences in other outcomes.
Conclusions This patient-specific prescribing and tapering protocol effectively decreases the total opioid dose prescribed for 6 weeks postdischarge after elective primary spine surgery. Our experience also demonstrates the potential generalizability of this protocol, which was originally designed for joint replacement patients, to other surgical populations.
- opioids, adverse effects
- acute pain
- postoperative pain
Statistics from Altmetric.com
Introduction
Opioids continue to be an important component of perioperative multimodal pain management for most surgical patients,1 but overprescribing and lack of guidance with regard to tapering and cessation2 3 have contributed to a complex public health epidemic. For the surgical patient, experts recommend developing a postoperative pain management plan tailored to the individual patient and surgical procedure involved.4 To date, no specific guidelines exist for the spine surgery patient. We implemented a patient-specific discharge opioid prescribing and tapering protocol for orthopedic joint replacement patients at our institution that has successfully decreased the amount of opioid prescribed2 and subsequently applied the same protocol to neurosurgical spine patients. We designed this retrospective cohort study to test the hypothesis that this patient-specific protocol for elective primary spine surgery will decrease the oral morphine milligram equivalent (MME) dose of opioid prescribed postoperatively.
Methods
The study design followed the Strengthening the Reporting of Observational Studies in Epidemiology checklist for case–control studies.5
Study population and setting
The project took place at a tertiary care university-affiliated Veterans Affairs (VA) hospital with a perioperative surgical home (PSH) and an integrated Regional Anesthesiology and Acute Pain Medicine (RAAPM) program which is staffed daily by an attending anesthesiologist, RAAPM fellow, and nurse practitioner.6 7 The RAAPM program directly comanages all orthopedic surgery and neurosurgical spine surgery patients from admission to discharge and is available round the clock for issues related to pain management.7
Analgesic clinical pathway
Multimodal analgesia is instituted on the day of surgery using a standardized order set in the electronic medical record (EMR) which can be adjusted to the individual patient; patients on chronic pain medications including opioids are continued on their preoperative regimens. Preoperative analgesics include oral acetaminophen 500–1000 mg and gabapentin 600 mg (or home dose). Following surgery, patients are prescribed oral acetaminophen (1000 mg every 6 hours), gabapentin if indicated, oxycodone (5 mg every 6 hours scheduled for the first 24 hours and only if taking opioids preoperatively, plus 5–10 mg every 4 hours as needed), and hydromorphone (0.2 mg intravenously every 4 hours as needed) except when any of these agents is contraindicated. Intraoperative anesthesia is not standardized.
Implementing the opioid prescribing and tapering protocol
Prior to implementing the discharge opioid prescribing and tapering protocol, there was no standard work at our institution for discharge opioid prescribing. Regimens were based on provider preference and did not include tapering instructions. In May 2018, a multidisciplinary team from anesthesiology, orthopedic surgery, ambulatory care, and pain medicine developed a patient-specific discharge opioid prescribing and tapering protocol for joint replacement patients. This protocol (figure 1) used the patient’s prior 24-hour oral opioid consumption (eg, oxycodone) to determine the discharge opioid prescription details including the total pill number and an individualized tapering schedule with the aid of computerized order entry.2 Patients were also continued on their non-opioid analgesics postdischarge and managed by the prescribing clinician. For our hip arthroplasty population, this protocol was associated with a 63% reduction in postdischarge opioid dose.2 In July 2018, this protocol was expanded to the neurosurgical spine surgery patient population with the support of the attending neurosurgeons and other prescribing neurosurgery clinicians.

Discharge opioid prescribing and tapering protocol based on each patient’s prior 24-hour oral opioid use.
Data elements
We queried the PSH database7 and EMR for all consecutive elective primary spine surgery cases 1 year before (preintervention) and after (postintervention) introduction of the protocol. This was a convenience sample, and no a priori sample size estimate was performed. We only included patients who were admitted postoperatively to the surgical ward and discharged home. We excluded all revisions, surgeries involving >3 spinal levels, patients admitted to a higher level of care after surgery (eg, intensive care unit), and patients discharged to subacute rehabilitation or skilled nursing facilities. Baseline characteristics were age, sex, morphometrics, American Society of Anesthesiologists physical status, psychiatric comorbidity or substance abuse disorder, preoperative opioid use history, preoperative diagnosis, and type of surgery. Individual charts were manually reviewed to characterize each patient’s inpatient opioid use and clinical course. Prescription records within the EMR were used to quantify postoperative opioid prescribing.
Outcomes
All data elements to be collected, outcomes (including specification of the primary outcome), and stepwise analytic plan were determined prior to initiating the study and any data collection. The primary outcome was total opioid dosage in oral MME prescribed at hospital discharge plus refills through a 6-week period postoperatively. The 6-week interval was chosen to be consistent with our prior study2 and to represent the postoperative interval when analgesic prescribing is still primarily the responsibility of the surgeon. Secondary outcomes included in-hospital opioid consumption in MME, hospital length of stay, MME on the initial discharge prescription (not including refills), opioid refills after the initial discharge prescription, minor and major postoperative adverse events, emergency room visits, and readmissions.
Statistical analysis
Statistical analysis was performed using NCSS Statistical Software (NCSS, Kaysville, Utah, USA) and IBM SPSS Statistics V.23. MME was calculated using standard conversion factors available through a free online tool produced by the Oregon Health Authority (https://www.oregonpainguidance.org/opioidmedcalculator/). Normality of distribution was determined for all scale variables using the Kolmogorov-Smirnov test and evaluation of histograms. For normally distributed data, single comparisons were performed using Student’s t-test; for continuous data in non-normal distributions, the Mann-Whitney U test was used. The χ2 test or Fisher’s exact test (n<5 in any field) was used for comparisons of categorical data. For the primary outcome, a two-sided p<0.05 was considered statistically significant. Because this was an exploratory analysis, we did not adjust for multiple comparisons.
Results
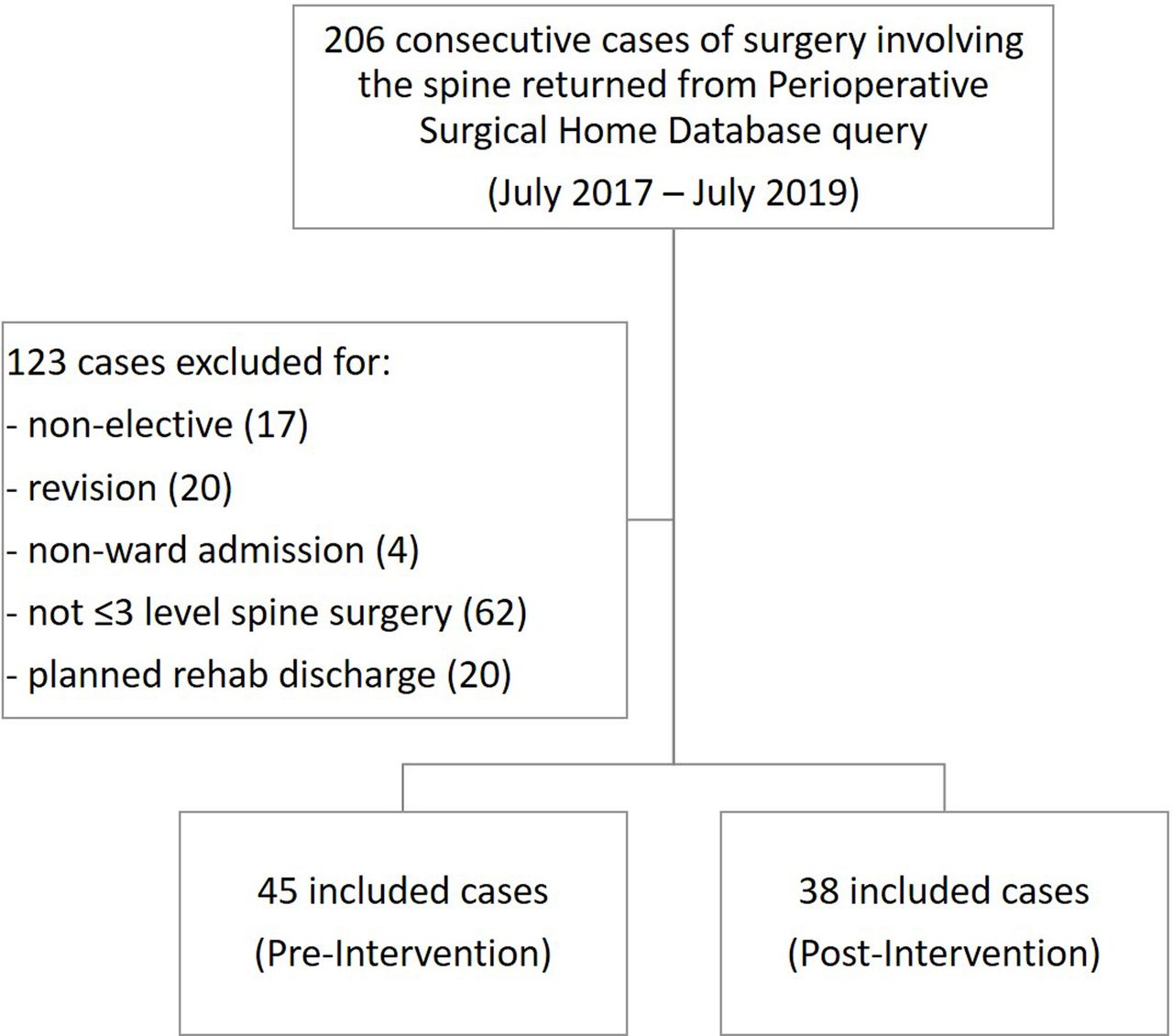
Two hundred and six patients underwent surgery involving the spine from July 2017 to July 2019. After applying the inclusion and exclusion criteria, 83 cases comprised the final sample (45 preintervention and 38 postintervention; figure 2). There were no differences in baseline characteristics between groups (table 1).
Demographics and baseline characteristics
{kind=link}
{kind=link}
STROBE study diagram. STROBE, Strengthening the Reporting of Observational Studies in Epidemiology.
Primary outcome
The total oral MME (median (IQR)) from discharge through 6 weeks postoperatively was 900 (420–1440) preintervention compared with 300 (112–806) postintervention (p<0.01, Mann-Whitney U test). This decrease was driven by discharge prescription MME (630 (400–900) preintervention compared with 280 (90–450) postintervention; p<0.01, Mann-Whitney U test) since the refill MME (0 (0–300) preintervention and 0 (0–138) postintervention) did not differ (p=0.66, Mann-Whitney U test), and the proportion of patients who received an opioid refill was not different between groups (table 2).
Secondary outcomes
Other postoperative outcomes are shown in table 2. There were no differences between groups in minor and major adverse events, emergency room visits, or readmissions.
Discussion
The implementation of a patient-specific protocol to guide opioid prescribing and tapering after elective primary spine surgery decreases the total dose of opioids prescribed at discharge and through 6 weeks postoperatively without an increase in refill rates. Our experience also demonstrates the potential generalizability of this protocol, which was originally designed for joint replacement patients, to other populations of patients undergoing major surgery.
After surgery, patients’ outpatient opioid prescriptions are traditionally written in arbitrary dosages and pill quantities in excess of actual need.8 Since the publication of the opioid guideline for chronic pain by the Centers for Disease Control and Prevention,9 many initiatives have been put in place to curb overprescribing.10–12 While these are good examples of successful tactics to decrease initial prescription doses and pill numbers, there is little to no guidance for patients on how to taper off opioids after surgery.2 Musculoskeletal surgery has been associated with a greater time to cessation of opioids,13 and much attention has been focused on orthopedic surgeons, who are the third-highest prescribers of opioid prescriptions among physicians in the USA.14 Although the protocol we implemented was originally designed for joint replacement patients,2 our data show that it can be applied successfully to other types of major surgery and may have the potential for broader translation.
Surgeons at the Hospital for Special Surgery have published consensus-based institutional opioid prescribing guidelines for their spine surgery service developed by a multidisciplinary committee of pain medicine physicians, anesthesiologists, nurse managers, and spine surgeons. Unlike our protocol, these guidelines focused exclusively on decreasing initial prescription dose and pill number through prescriber education and did not address tapering.15 Although these investigators report decreases in the mean dose and number of opioid tablets prescribed at discharge after lumbar spine surgery, they also note a concerning trend in increasing refill rates after implementation (12.4% vs 7.6% preintervention; p=0.07).15 As recommended in the multisociety guideline on the management of postoperative pain,4 we believe that any discharge opioid stewardship initiative must address tapering.
It is easy to assume that implementing any prescribing protocol at discharge will have to work. However, many contextual factors influence the ability to implement and sustain change in clinical practice.16 Our institution employs a mature PSH model which coordinates care of the surgical patient and involves a multidisciplinary team.7 This model has been shown to facilitate and maintain long-term anesthesia changes.17 18 Multimodal perioperative pain management starts before surgery with advance consultation for complex patients and continues on the day of surgery with oral preoperative analgesics and a multimodal analgesic protocol postoperatively.19 Since RAAPM clinicians comanage spine patients including daily analgesic prescribing, typically patients are off intravenous opioids and have only as-needed oral opioids with non-opioid systemic analgesics by postoperative day 1. We speculate that this direct care throughout the perioperative period by RAAPM may be the critical element that sets up the patient for a successful pain management transition home with lower opioid requirements.
There are several limitations to this study. First, this was a retrospective study of real patient data, which may contain errors, and not a homogeneous clinical trial sample. We included patients who were on chronic opioids for pain management rather than excluding them, since unfortunately opioid use is common in this patient population. We did attempt to limit the variability in our sample by excluding more invasive surgeries involving more than three spinal levels and more complex postoperative recovery and rehabilitation in order to measure an effect within a group of similar patients. Further, we cannot rule out temporal trends toward decreased opioid prescribing as a potential influencing factor, although the VA launched its opioid safety initiative years earlier.20 Statistical process control, employing a control chart, offers an effective means to account for naturally occurring variation.21 Second, this study measured only opioid prescriptions and routine clinical outcomes but did not arguably address patient-centered outcomes, such as patient experience with pain control, which are very important.22 Third, since the protocol has only been instituted for two types of major inpatient surgery to date, we speculate that it may need to be adjusted for short-stay and outpatient surgical populations. Fourth, this study was limited by the length of the postintervention follow-up period (6 weeks). This interval2 was chosen since opioid prescriptions are still primarily provided by the surgeon and not primary care. Fifth, data were restricted to prescription information within our EMR and not actual opioid consumption. Although it is reasonable to assume that veteran patients who have surgery at the VA will receive prescriptions through the VA, we cannot exclude the possibility that patients received outside prescription for opioids. Finally, the VA patient population has unique characteristics23 that may limit the generalizability of our results. However, we believe the patient-specific assessment of opioid use and application to tailored prescribing and tapering can be revised for other institutional settings.
In conclusion, a patient-specific opioid prescribing and tapering protocol at discharge designed for one major surgery population can be successfully applied to another with similar decreases in the total dose of opioid prescribed through 6 weeks after surgery. We recommend that all institutions who care for surgical patients consider adopting a process of multidisciplinary collaboration to consider our protocol and practices or develop modifications to suit their own patients’ needs.
Acknowledgments
This material is a result of the work supported with resources and use of facilities at the Veterans Affairs (VA) Palo Alto Health Care System (Palo Alto, California, USA). The content does not represent the views of the Department of Veterans Affairs or the US Government.
References
Footnotes
Twitter @EMARIANOMD
Presented at Accepted for presentation at the 2020 spring annual meeting of the American Society of Regional Anesthesia and Pain Medicine.
Contributors SSJ helped design the study, collected data, drafted and revised the initial manuscript, reviewed and approved the submitted manuscript. OOH helped design the study, implemented the tapering protocol, collected data, reviewed and approved the submitted manuscript. MT helped design the study, collected data, reviewed and approved the submitted manuscript. JCL helped design the study, implemented the tapering protocol, reviewed and approved the submitted manuscript. TKH, SCM, and RRW helped design the study, reviewed and approved the submitted manuscript. KK implemented the tapering protocol, collected data, reviewed and approved the submitted manuscript. JDK, SS, ST, and ES implemented the tapering protocol, collected data, reviewed and approved the submitted manuscript. AK helped design the study, collected and analyzed data, reviewed and approved the submitted manuscript. ERM helped design the study, collected and analyzed data, drafted and revised the initial manuscript, reviewed and approved the submitted manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This retrospective cohort study was reviewed and approved with waiver of informed consent by the local institutional review board (Stanford, California) and the Veterans Affairs Research Committee (Palo Alto, California).
Provenance and peer review Not commissioned; externally peer reviewed.