Article Text

Abstract
Background Paravertebral nerve blocks (PVBs) are frequently used to treat pain during and following breast surgery, but have various undesirable risks such as pneumothorax. The erector spinae plane block (ESPB) also provides perioperative breast analgesia, but is purported to be easier to administer with a favorable safety profile. However, it remains unknown if the new ESPB provides comparable analgesia as the decades-old PVB technique.
Methods Subjects undergoing unilateral or bilateral non-mastectomy breast surgery were randomized to a single-injection ESPB or PVB in a subject-blinded fashion (ropivacaine 0.5% with epinephrine; 20 mL unilateral or 16 mL/side for bilateral). We hypothesized that (1) analgesia would be non-inferior in the recovery room as measured on a Numeric Rating Scale (NRS) with ESPB, and (2) opioid consumption would be non-inferior in the operating and recovery rooms with ESPB.
Results Both pain scores and opioid consumption were higher in subjects with ESPBs (n=50) than PVBs (n=50; median NRS 3.0 vs 0; 95% CI −3.0 to 0; p=0.0011; and median morphine equivalents 2.0 vs 1.5 mg; 95% CI −1.2 to −0.1; p=0.0043). No block-related adverse events occurred in either group.
Conclusions PVBs provided superior analgesia and reduced opioid requirements following non-mastectomy breast surgery. To compare the relatively rare complications between the techniques will require a sample size 1–2 orders of magnitude greater than the current investigation; however, without a dramatic improvement in safety profile for ESPBs, it appears that PVBs are superior to ESPBs for postoperative analgesia after non-mastectomy breast surgery.
Trial registration number NCT03549234.
- truncal blocks
- acute pain
- pain outcome measurement
Statistics from Altmetric.com
Introduction
Breast surgery is frequently associated with significant pain in the immediate postoperative period, which is, itself, associated with persistent postsurgical pain leading to a decreased quality of life.1–3 Multiple randomized, controlled clinical trials provide evidence that improving perioperative analgesia following mastectomy decreases pain in the immediate postoperative period, and chronic pain up to 12 months following surgery.4–6 Therefore, strategies to minimize acute postoperative pain after breast surgery with multimodal analgesic regimens and regional anesthetic techniques have been increasingly investigated and implemented.7
One such analgesic method for surgical procedures of the breast is the thoracic paravertebral nerve block (PVB), which decreases pain and opioid consumption in both the immediate and remote postoperative periods.8 However, given the proximity of the paravertebral space to the pleura, there remains a non-insignificant risk of iatrogenic pneumothorax during placement of PVBs,9 even with ultrasound guidance.10 Similarly, due to its depth and proximity to the neuraxis, this approach may be considered a more advanced regional anesthetic technique. And, for non-catheter techniques, injections at multiple thoracic levels are usually required to optimize analgesia,11 tripling or quadrupling the risks with each needle pass.12 There is therefore renewed interested in potentially safer and technically less-demanding fascial plane blocks.
The erector spinae plane block (ESPB) is the most recently described of the fascial plane blocks performed for breast surgery analgesia.13 The ESPB involves deposition of local anesthetic deep to the erector spinae muscle and superficial to the transverse process and paravertebral space.14 Although still possible,15 there is a theoretically decreased risk of serious complications such as pneumothorax and intrathecal injection compared with PVBs given the relatively superficial position of the ESPB and increased distance between the target plane and pleura/neuraxis. Interest in the ESPB is high, with over 200 publications involving this technique in the 2 years since its first description in 2016.16 Despite the proliferation of publications describing ESPBs, prospective, randomized controlled studies comparing ESPBs to conventional nerve blocks for breast surgery are sparse,17 18 and it remains unknown if the new ESPB provides comparable analgesia as the decades-old PVB technique.
We therefore undertook this randomized, subject-blinded, active-controlled, parallel-design clinical trial to determine if ESPBs provide comparable postoperative analgesia to PVBs following breast surgery, primarily to determine whether the more technically challenging PVB should be replaced with the more superficial and possibly lower risk fascial plane block. We hypothesized that ESPBs would provide non-inferior analgesia to PVBs following breast surgery, with dual primary end points of pain scores within the recovery room and opioid requirements in the operating and recovery rooms combined. In order to claim that ESPBs are non-inferior to PVBs, both primary end points had to be at least non-inferior.
Methods
Study participants
Written, informed consent was obtained from all participating subjects.
Inclusion and exclusion criteria
Adults (equal to or greater than 18 years) presenting for unilateral or bilateral breast surgery with at least moderate postoperative pain anticipated and a planned single-injection regional analgesic were screened for enrollment preoperatively. Exclusion criteria included: planned regional analgesic with perineural catheter placement, morbid obesity as defined as a body mass index>40 kg/m2, renal insufficiency (preoperative creatinine>1.5 mg/dL), current chronic opioid use (daily equivalent of >20 mg of oxycodone within the 2 weeks prior to surgery and duration of use>4 weeks), history of opioid abuse, any comorbidity that results in moderate or severe functional limitation, inability to communicate with the investigators or hospital staff, pregnancy, incarceration and allergy to study medications (ropivacaine).
Block procedures
Preoperatively, participating subjects were placed in the sitting position with standard American Society of Anesthesiologists monitors and supplemental oxygen. All block procedures were performed by a regional anesthesia attending or fellow as previously described.13 19 Sedation was provided with intravenous midazolam and fentanyl, titrated to patient comfort during the block procedure. For all subjects, a low-frequency curvilinear ultrasound transducer (6–2 MHz) was used to identify the T1 through T5 transverse processes and paravertebral spaces. After confirmation of acceptable ultrasound visualization of both potential block sites, subjects were randomized using a computer-generated list and opaque, sealed envelopes to one of two treatment groups stratified for unilateral versus bilateral surgery: (1) ESPB or (2) PVB. Subjects were blinded to treatment group allocation.
A 20-gage Tuohy needle was inserted into the appropriate plane/space under direct ultrasound guidance via an in-plane parasagittal approach. Local anesthetic (0.5% ropivacaine) with 1:400 000 of epinephrine was injected at the appropriate level(s) after negative aspiration (20 mL for unilateral surgery, 16 mL on each side for bilateral surgery). For PVBs, a two-level injection technique was performed: T2 and T4 for surgeries involving axillary work or T3 and T5 for surgeries not involving axillary work. For ESPBs, a single injection was performed at T3 for surgeries involving axillary work or T4 for surgeries not involving axillary work.
Blocks were considered successful if, within 30 min, the subject experienced decreased sensation to cold temperature over the level of the ipsilateral fourth thoracic dermatome at the level of anterior axillary line. For subjects undergoing a bilateral surgical procedure, a block using the same protocol was administered on the contralateral side.
In addition, preoperatively, patients were given oral acetaminophen. A standardized multimodal analgesic regimen postoperatively was not used and left to the surgical team’s discretion.
Intraoperative and postoperative management
Surgery was performed under general anesthesia with a combination of inhaled and intravenous anesthetics. Intraoperative fentanyl was administered at the discretion of the blinded anesthesia team based on cardiovascular responsiveness to noxious stimuli, and total fentanyl use was recorded. Subjects were extubated, taken to the postanesthesia care unit (PACU) and received by a nurse blinded to randomization. A standard PACU opioid algorithm was used which involved: (1) intravenous fentanyl 25 µg for Numeric Rating Scale (NRS) pain scores of less than 5, (2) intravenous fentanyl 50 µg for NRS of 5 or greater, (3) intravenous hydromorphone 0.5 mg for NRS of 5 or greater if fentanyl deemed ineffective, and (4) oxycodone 5 mg for NRS of 4–6 if able to tolerate oral medications. Subjects scheduled for outpatient surgery were discharged home with a prescription for oxycodone tablets (5 mg) for supplementary analgesia and instructed to record the time at which they took their first opioid tablet as well as the time at which they believed the block began to resolve. Admitted subjects were provided oxycodone 5 mg every 4 hours as needed for NRS of 4–6; and 10 mg every 4 hours as needed for NRS of 7–10.
Outcome measurements
Pain scores were recorded using the NRS. Within the PACU, pain scores, opioid requirements, and antiemetic administration were recorded by nursing staff blinded to treatment. The morning following surgery, all subjects were contacted by telephone or in person (if hospitalized) to record lowest, average, highest, and current pain scores, number of sleep disturbances, and nausea using a 0–10 Likert scale (0=no nausea; 10=vomiting). For ambulatory subjects, opioid requirements were recorded by patients while inpatient subjects had opioid requirements extracted from the electronic medical record. In addition, for inpatient subjects, antiemetic use and nursing-recorded pain scores were extracted from the electronic medical record. We collected the times at which subjects identified block resolution and the time at which they consumed their first oral opioid analgesic following PACU discharge. In addition, possible block-related side effects and adverse events were recorded.
Statistical analysis
We hypothesized that (1) analgesia would be non-inferior in the recovery room as measured on an NRS (0–10) with ESPB, and (2) opioid consumption would be non-inferior in the operating and recovery rooms with ESPB. In order to claim that ESPBs are non-inferior to PVBs, both hypotheses had to be at least non-inferior. We tested the non-inferiority of ESPB compared with PVB using the 95% CI associated with the Wilcoxon-Mann-Whitney exact test. If the lower limit of the 95% CI for median “average” PACU pain scores was greater than −1.25 (based on PVB minus ESPB), we concluded non-inferiority. The non-inferiority of ESPBs with regard to opioid consumption was similarly tested by comparing the limits of a 95% CI associated with the Wilcoxon-Mann-Whitney exact test to a predefined non-inferiority margin of 2 mg intravenous morphine equivalents. All subjects were analyzed on an intention-to-treat basis. R V.3.5.2 (https://www.r-project.org/) was used for all analyses. P values, if reported, are two sided.
Sample size justification
Power for the Wilcoxon-Mann-Whitney-derived non-inferiority testing was based on 10 000 simulated trials. We simulated pain scores from a discrete distribution with median (IQR) 2 (0–3).19 Between the quartiles, the probability of each score was assumed constant. The distribution for each group was assumed to be the same. The sample size of 50 per group provided 81% power to detect non-inferiority in pain (online supplementary appendix 1). Similarly, opioid consumption was assumed to follow a truncated normal distribution with mean 2.5 mg and SD 2 mg, and minimum value 0 mg. The sample size of 50 per group provided at least 95% power to detect non-inferiority with margin 2 mg (online supplementary appendix 1). Therefore, the planned enrollment for this study was 50 subjects for each of the two treatment groups with a total enrollment of 100 subjects.
Supplemental material
Results
One-hundred subjects were enrolled in the 10 months beginning July 2018 (figure 1). All subjects were randomized to either ESPB (n=50) or PVB (n=50) treatment groups after confirmation of adequate ultrasound visualization. All subjects completed the outcome measurements and follow-up call or visit on postoperative day (POD) 1. There were no postrandomization exclusions of any subjects due to protocol deviations.
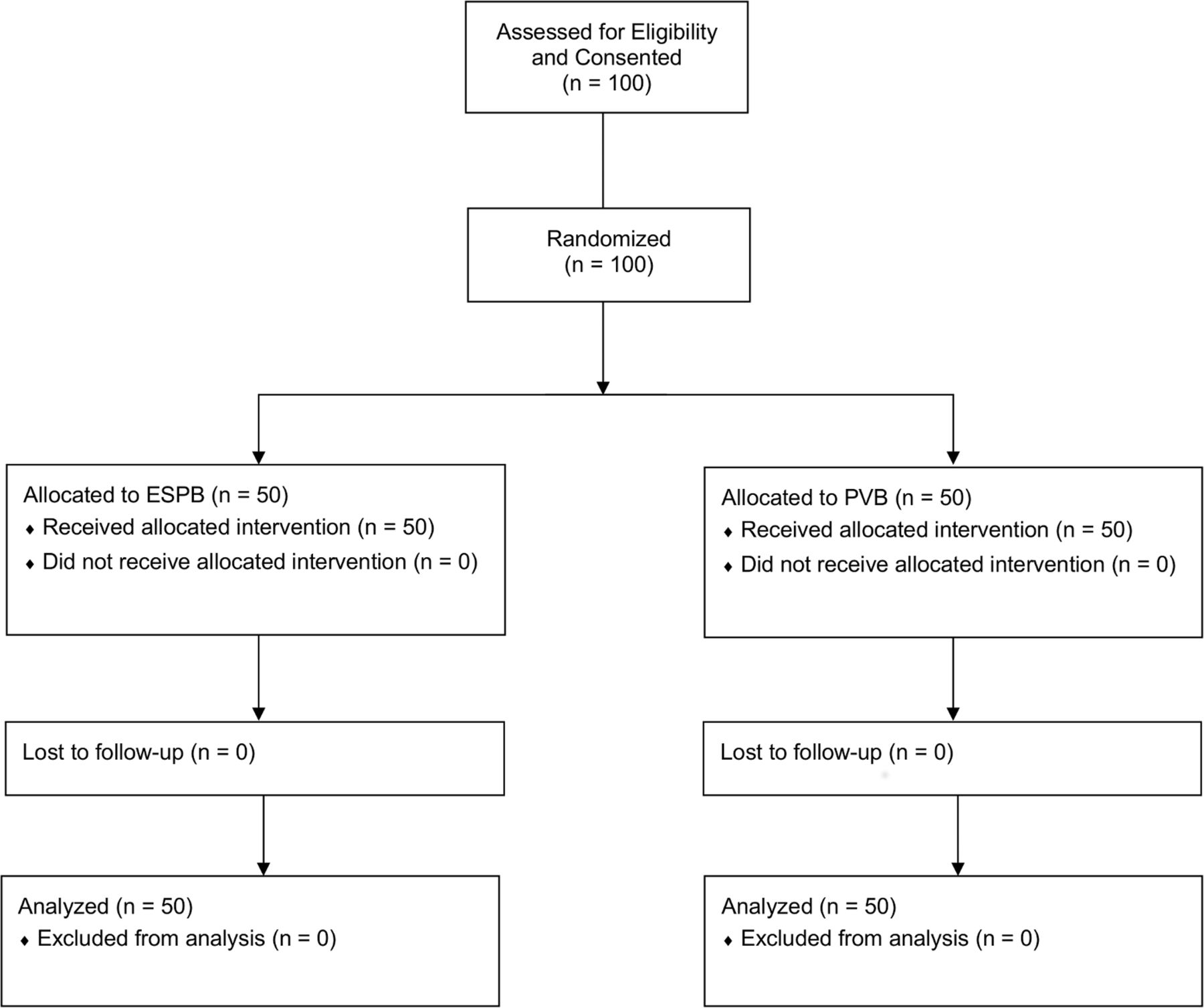
Consolidated standards of reporting trials statement diagram showing flow of study participants. ESPB, erector spinae plane block; PVB, paravertebral block.
No significant differences in anthropomorphic and surgical characteristics between the two treatment groups were identified (table 1), including an equal number of unilateral (n=25) and bilateral (n=25) procedures.
Anthropomorphic and surgical characteristics
The most common surgical procedures were lumpectomy with sentinel lymph node biopsy, breast reconstruction, and breast reduction (table 2).
Surgical procedures
Patients undergoing mastectomy were excluded since those patients are offered paravertebral catheters at our institution. All block procedures were successfully performed per protocol.
Compared with PVBs, the median time to perform the ESPB block procedure as measured from time of block needle insertion to removal of block needle was shorter to a statistically significant degree (1.9 min/side for ESPBs vs 4.1 min/side for PVBs; difference=2.5; p<0.001). There was no statistically significant difference in fentanyl requirements for block administration between the two treatment groups (table 3).
Block procedure data
Lastly, median average NRS pain scores during the block procedures were similar (2.0 for ESPBs vs 2.0 for PVBs; difference=0; p=0.609; table 3), as were the median maximum NRS pain scores (2.0 for ESPB vs 3.5 for PVB; difference=1; p=0.054; table 3).
Primary end point
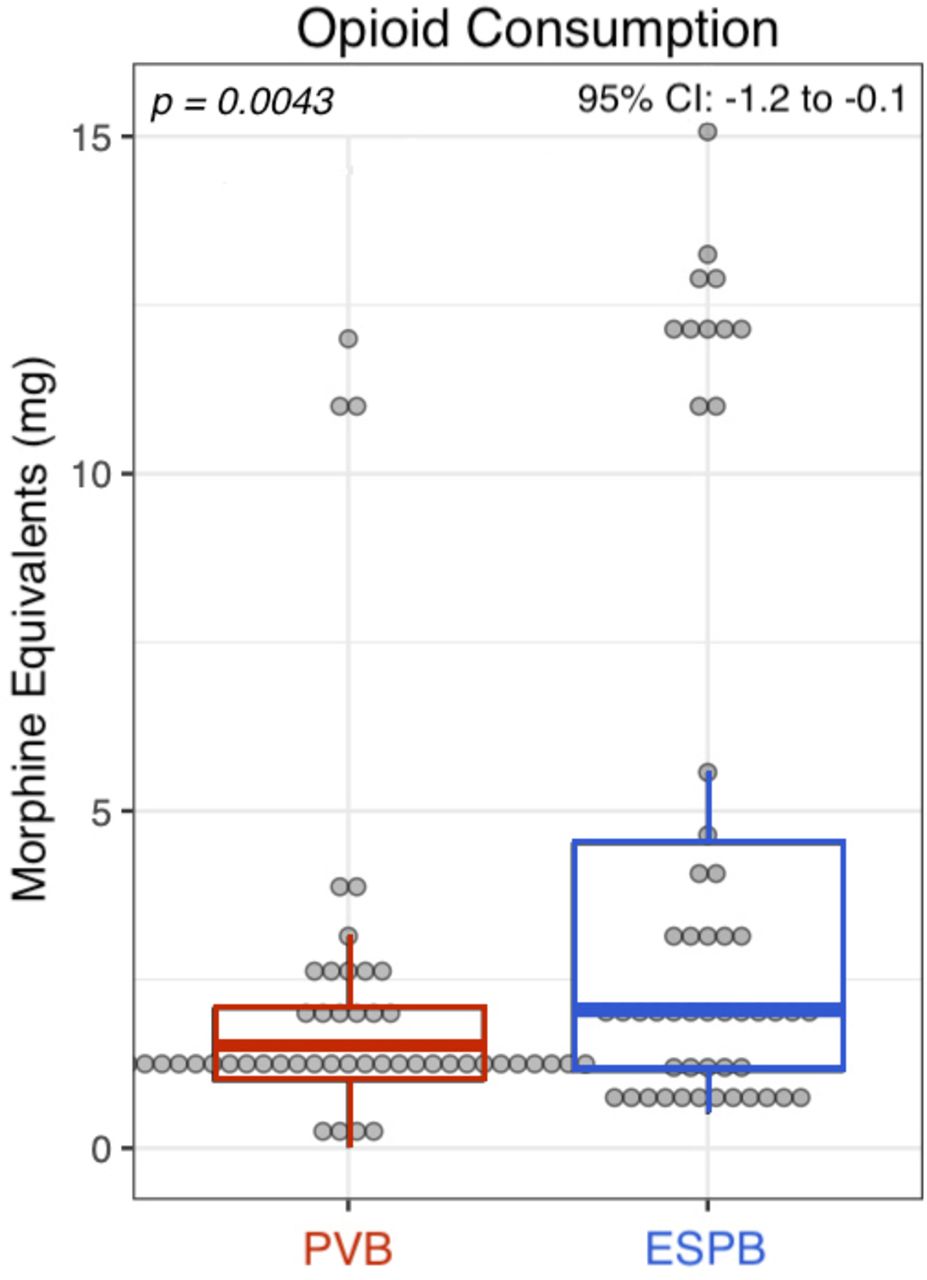
Pain experienced in the PACU by ESPB subjects was not non-inferior as originally hypothesized; in fact, ESPB subjects reported higher median PACU pain scores compared with their PVB counterparts (3.0 vs 0; difference = −2; 95% CI −3 to 0; p=0.0011; figure 2). Correspondingly, median operating room and PACU opioid requirements were higher for subjects with ESPB compared with PVB to a statistically significant degree (2.0 vs 1.5 mg; difference=−0.75; 95% CI −1.2 to −0.1; p=0.0043; figure 3).

Median Numeric Rating Scale pain scores in postanesthesia care unit (PACU) between two treatments groups. Horizontal lines indicate overall median for each treatment group; boxes indicate the 25th and 75th percentiles; vertical lines indicate the 5th and 95th percentiles. ESPB, erector spinae plane block; PVB, paravertebral block.
{kind=link}
{kind=link}
{kind=link}
Operating room and postanesthesia care unit morphine equivalents opioid consumption between two treatment groups. Horizontal lines indicate overall median for each treatment group; boxes indicate the 25th and 75th percentiles; vertical lines indicate the 5th and 95th percentiles. ESPB, erector spinae plane block; PVB, paravertebral block.
Secondary end points
There was no difference in median operating room opioid administration between the two treatment groups (1.0 mg morphine equivalents for ESPB group vs 1.0 mg for the PVB group; difference=0; p=0.206; table 4).
Secondary end points
Similarly, there was no statistically significant difference in antiemetic use in the PACU between the two groups (table 4). However, there was a decreased median PACU length of stay in the PVB group (105 min in PVB group vs 124 min in the ESPB group; difference = −16; p=0.047; table 4). Five subjects were admitted postoperatively from the ESPB group compared with four subjects in the PVB group, and inadequate pain control was not the reason for admission for any of the nine subjects. For subjects admitted postoperatively, five out of five ESPB subjects were discharged on POD 1 compared with three out of four PVB subjects (the other was discharged on POD 2). The number of hospitalized subjects was too small to make any conclusions regarding differences between groups in day of discharge.
On the morning of POD 1, no statistically significant differences were seen between subject-reported highest, lowest, average, or current pain scores (table 4). Similarly, subjects reported taking a median of 5 mg oxycodone after discharge in the ESPB group and 10 mg oxycodone in the PVB group (difference=0; p=0.323; table 4). No differences were also seen between median nausea Likert scores and number of overnight awakenings due to pain (table 4). Lastly, subject-reported median block durations were similar between the two groups (17.7 hours for ESPB group vs 16.0 hours for the PVB group; difference=−0.25; p=0.833; table 4).
Major protocol violations and adverse events
There were no adverse events related to the block procedures such as pneumothoraces, nerve injuries, bleeding complications, or infections. One subject in the PVB group had intraoperative anaphylaxis deemed secondary to the isosulfan blue dye injection. Another subject in the PVB group received naloxone 40 µg during emergence of anesthesia due to delayed emergence after receiving fentanyl 100 µg during induction of anesthesia. One subject with a history of a prior pleural effusion in the ESPB group was unexpectedly admitted for overnight observation due to low oxygen saturations in the PACU on room air and discharged on POD 1.
Discussion
Given the technical concerns with PVBs, there has been an abundance of recently developed fascial plane blocks performed for breast surgery including ESPBs, serratus plane blocks, and pectoralis fascial plane blocks. While generally thought to be technically easier to perform than PVBs, the comparative effectiveness and safety of these fascial plane blocks are not yet fully understood. Specifically, ESPBs have been touted as a potential “magic bullet” for postoperative thoracoabdominal analgesia that can be performed without the need for highly subspecialized training in advanced ultrasound-guided regional anesthesia that PVBs require.20 21 As such, if these fascial plane blocks are found to be non-inferior in terms of analgesia compared with traditional nerve blocks, these possibly safer and easier to perform blocks might increase the adoption of interventional regional anesthetic procedures available to patients with breast surgery.
However, this randomized, subject-blinded, active-controlled, parallel-arm clinical study provides compelling evidence that PVBs significantly improve short-term postoperative analgesia after breast surgery compared with ESPBs. Our initial hypotheses involved testing for non-inferiority of the newer ESPB relative to the decades-old PVB, due to the myriad of case reports/series and even randomized, placebo-controlled trial of apparent potent analgesia with the fascial plane technique.16 18 However, our active-controlled study strongly suggests that PVBs are superior to ESPBs for both short-term analgesia as well as opioid sparing following non-mastectomy breast surgery. This does not imply that there is no role for ESPBs, but simply that PVBs appear superior in certain important aspects. The individuals placing the blocks of this study were all fellowship-trained attendings or current fellows being overseen by attendings with a great deal of prior experience. Practitioners with less experience administering PVBs might decide that the risk–benefit ratio is superior with the more-superficial ESPB. In contrast, healthcare providers currently using PVBs for postoperative analgesia following breast surgery now have less impetus to change techniques.
Thus, given our findings, we can only speculate on the reason for the improved analgesia of PVBs over ESPBs. When comparing the analgesic effect of ESPBs to PVBs, the mechanism of action of ESPBs remains incompletely understood. Case reports have demonstrated extensive cutaneous sensory block suggesting both ventral and dorsal rami blockade.14 This clinical result has led to the hypothesis that ESPBs have a similar mechanism of action to PVBs.22 However, further cadaveric studies investigating the spread of injectate in ESPBs have shown inconsistent spread to the ventral rami or into the paravertebral space.14 22–24 Given these cadaveric findings and proposed mechanism of action, one might expect superior analgesia with PVBs over ESPBs as local anesthetic is directly deposited into the paravertebral space rather than indirectly spreading from the erector spinae plane.
Given the relatively recent description of ESPB as an analgesic technique, randomized, controlled trials are sparse. Despite the technical ease of performing and theoretically increased safety, comparison of fascial plane blocks to conventional nerve blocks with rigorous randomized, controlled trials is much needed.20 For postoperative analgesia after breast surgery, there is only one randomized, controlled comparison of ESPBs versus PVBs.18 This recent study of 75 subjects (ESPB n=25, PVB n=25, no intervention n=25) compared ESPB (n=25), PVB (n=25), and no intervention groups (n=25) for elective, unilateral breast surgery, of which 32% were mastectomies.18 While both ESPBs and PVBs showed superiority over the no intervention group, no differences in opioid consumption and pain scores were seen between the ESPB and PVB groups.18
This study represents the first published report showing the superiority of PVBs over ESPBs in terms of perioperative opioid consumption and pain scores after non-mastectomy breast surgery. In terms of perioperative opioid consumption, subjects receiving PVBs required 51% fewer MEQs in the OR and PACU compared with subjects receiving ESPBs. Similarly, mean PACU pain scores were 43% lower for subjects receiving PVBs compared with ESPBs. Of note, 8 subjects (16%) in the ESPB group had all zero pain scores in the PACU compared with 18 subjects (36%) in the PVB group. Similarly, 15 subjects (30%) in the ESPB group required no opioids in the PACU compared with 24 subjects in the PVB group (49%). As such, the improved PACU analgesia seen in the PVB group may have translated into a decreased PACU length of stay compared with the ESPB group. These findings indicate that PVBs provide more potent early postoperative analgesia compared with ESPBs for non-mastectomy breast surgery. The implications for patient experience and health-related outcomes of this early analgesic benefit are unclear. It is possible that the short-term gains demonstrated herein do not meaningfully impact on either patient safety or quality of the surgical outcomes.
In comparison to the only other randomized controlled study comparing PVBs to ESPBs for breast surgery, the difference in postoperative analgesia seen in this study could be attributed to a number of study-related factors, namely: (1) exclusion of mastectomy subjects, (2) inclusion of non-cancer reconstructive procedures, (3) block technique, (4) lack of use of morphine patient-controlled analgesia, and (5) volume and concentration of local anesthetic used.18 Specifically, with respect to the block technique used by Gürkan et al, the anatomy seen in their description of a paravertebral block appears to be a more lateral nerve block rather than a paravertebral block at the level of the transverse process just lateral to the lamina.18 In addition, we chose to use a similar volume of local anesthetic in a higher concentration (ropivacaine 0.5%) compared with bupivacaine 0.25%, which may have impacted our results.18 As such, the type, volume, and concentration of local anesthetic needed to provide optimal postoperative analgesia for ESPBs have not been elucidated.
The optimal analgesic regimen after non-mastectomy breast surgery has not been established. For major non-cosmetic breast surgery (including mastectomies and axillary lymph node dissections), the Procedure Specific Postoperative Pain Management (PROSPECT) collaboration recommends preoperative PVBs as the interventional analgesic of choice.25 For minor breast surgery, the risks of PVBs may seem to outweigh their benefits according to the PROSPECT collaboration.25 The risks of PVBs include pneumothorax, hypotension, bradycardia, epidural or intrathecal spread, vascular puncture, nerve damage, and Horner’s syndrome. Although most published reports suggest a relatively low incidence of pleural puncture and pneumothorax,9 10 26 27 PVBs have been shown to decrease early postoperative pain, nausea, vomiting, and to facilitate earlier return to normal activities after non-mastectomy breast surgery.7 28 In this current study, no pleural punctures or pneumothoraces were seen in either treatment group. To compare this relatively rare complication between the two techniques would require a sample size 1–2 orders of magnitude greater than the current investigation.
Limitations
Although the subjects of this investigation were blinded to treatment group assignment, investigators were aware of the randomization results. In addition, the results apply only to the specific local anesthetic type, concentration and volume of the current study. Similarly, different surgical procedures (eg, mastectomy), block techniques (eg, in vs out of plane), and administration approaches (eg, loss-of-resistance vs ultrasound) would probably alter the results. More specifically, a potential confounder of the results could be that ESPB subjects received one injection whereas PVB subjects received two injections. Although our goal was to compare our institutional practice of two-level PVBs to the customary single-level ESPB—increasing external validity—this difference may have impacted the blinding of subjects as well as the analgesic results. In addition, intraoperative opioid administration by the blinded operating room anesthesia provider was not standardized and was left to their discretion.
Another limitation of our study included the time interval of pain assessments in our primary outcome. Since pain was only recorded in the PACU, analgesia was not fully assessed for the duration of the blocks in both treatment groups. Since most of these surgeries were performed on an outpatient basis, we chose to limit our blinded pain assessments to the PACU. We did not detect any statistically significant differences in subject-reported pain scores during follow-up on POD 1 after block resolution. Lastly, since mastectomy subjects were excluded from our study, the results only apply to non-mastectomy breast surgery.
Conclusions
This randomized, active-controlled study suggests that PVBs compared with ESPBs provide improvements in short-term perioperative analgesia following non-mastectomy breast surgery.
References
Footnotes
Contributors MWS, MCD, and BMI: helped with literature search, data collection, study design, analysis of data, manuscript preparation, and review of manuscript. AMW, SLB, AH, and MKD: helped with literature search, study design, manuscript preparation, and review of manuscript. JS, ES, BK, MA, JF, RAG, and WA: helped with literature search, data collection, study design, manuscript preparation, and review of manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests MWS, JS, ES, BK, JF, RAG, WA, and BMI: The University of California has received funding and product for other research projects from Myoscience (Fremont, CA) and Epimed (Farmers Branch, TX); infusion pump manufacturer Infutronics (Natick, MA); and a manufacturer of a peripheral nerve stimulation device, SPR Therapeutics (Cleveland, OH). MBI: in addition to the above, MBI’s institution has received funding from a manufacturer of a long-acting bupivacaine formulation, Heron Pharmaceuticals.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Please contact the corresponding author for data.