Article Text

Abstract
Background and objectives Fascia iliaca compartment block (FICB) has been shown to provide excellent pain relief in patients undergoing total hip arthroplasty (THA). However, the analgesic efficacy of FICB, in comparison with periarticular infiltration (PAI) for THA, has not been evaluated. This randomized, controlled, observer-blinded study was designed to compare suprainguinal FICB (SFICB) with PAI in patients undergoing THA via posterior approach.
Methods After institutional review board approval, 60 consenting patients scheduled for elective THA were randomized to one of two groups: ultrasound-guided SFICB block or PAI. The local anesthetic solution for both the groups included 60 mL ropivacaine 300 mg and epinephrine 150 µg. The remaining aspects of perioperative care, including general anesthetic and non-opioid multimodal analgesic techniques, were standardized. An investigator blinded to group allocation documented pain scores at rest and with movement and supplemental opioid requirements at various time points. Patients were evaluated for sensory changes and quadriceps weakness in the operated extremity.
Results There were no differences between the groups with respect to demographics, intraoperative opioid use, duration of surgery, recovery room stay, nausea scores, need for rescue antiemetics, time to ambulation and time to discharge readiness as well as 48 hours postoperative opioid requirements. The pain scores at rest and with movement also were similar at all time points. Significantly more patients in the SFICB group experienced muscle weakness at 6 hours after surgery.
Conclusions Under the circumstances of our study, in patients undergoing THA, SFICB provided the similar pain relief compared with PAI, but was associated with muscle weakness at 6 hours postoperatively.
Trial registration number NCT02658240.
- total hip arthroplasty
- suprainguinal fascia iliaca compartment block
- periarticular infiltration
- multimodal analgesia
- postoperative pain management
Statistics from Altmetric.com
- total hip arthroplasty
- suprainguinal fascia iliaca compartment block
- periarticular infiltration
- multimodal analgesia
- postoperative pain management
Introduction
Local and/or regional analgesia techniques are critical components of an optimal multimodal analgesia technique, as they have been shown to improve pain relief as well as reduce opioid requirements.1 2 Optimal pain management technique balances pain relief with concerns about safety and adverse effects associated with analgesic techniques.3 4 Suprainguinal fascia iliaca compartment block (SFICB) has been reported to reduce opioid requirements after total hip arthroplasty (THA).5 6 However, one of the concerns with SFICB is the potential for quadriceps weakness that might delay ambulation.
Periarticular infiltration (PAI) is increasingly included as a component of multimodal analgesia technique for patients undergoing THA, as it provides improved postoperative pain relief with no effects on quadriceps function.7 8 A recent network meta-analysis reported that head-to-head studies comparing PAI to peripheral nerve blocks for pain and opioid control after THA were lacking.9 This meta-analysis showed no difference between peripheral nerve blocks including FICB and placebo, but there was significant heterogeneity in the included studies.9
Therefore, we designed a randomized controlled trial to compare ultrasound-guided SFICB with PAI as a component of non-opioid analgesic regimen in patients undergoing THA via posterior approach. We hypothesized that SFICB would provide superior analgesia when compared with PAI. The primary aim of this study was to compare the pain scores and the secondary objectives were to compare opioid requirements, sensory changes in the operative extremity, degree of muscle weakness, opioid-related adverse effects such as nausea, vomiting, and need for rescue antiemetics, time to ambulation, and time to discharge readiness.
Methods
The trial was registered prior to patient enrollment with the US National Clinical Trials Registry (identifier NCT02658240, principal investigator: IG, date of registration: 14 January 2016).
After written informed consent was obtained, patients aged 18–80 years, American Society of Anesthesiologists Physical Status I–III, scheduled for elective THA via posterior approach at Parkland Health and Hospital Systems, Dallas, Texas, were enrolled in this study. Participants were excluded if they had a history of relevant drug allergy, significant psychiatric disturbances, history of alcohol or drug addiction or were currently using more than 20 mg of oral morphine equivalents. In addition, patients with contraindication to acetaminophen (eg, significant hepatic dysfunction) as well as ketorolac (eg, significant renal dysfunction and reactive airway disease) were also excluded. One of the investigators performed a baseline neurological evaluation before surgery including assessment of temperature sensation over the lateral and anterior aspects of the thigh and the qualitative assessment of the motor strength of the quadriceps muscle in the operative extremity compared with the non-operative extremity. Patients were block randomized according to a computer-generated randomization schedule (www.randomization.com) to one of two groups: SFICB and PAI. Randomization group allocations were concealed in sequentially numbered sealed opaque envelopes until all the entry criteria for the study had been verified.
At the end of surgery after the skin closure, but before emergence from general anesthesia (GA), patients randomized to SFICB group received ultrasound-guided SFICB block performed by one of the authors with significant previous experience in ultrasound-guided techniques (IG and JCA). The block was performed at the end of surgery to best match the timing of PAI performed by the surgeon. With the patient in the supine position, the ultrasound transducer was placed in a parasagittal orientation over the inguinal ligament, inferior medially to the anterior superior iliac spine.10 Using real-time ultrasound imaging internal oblique, sartorius and iliacus muscles, covered by the fascia iliacus, were identified. After aseptic preparation of the injection site and the ultrasound probe, a 22 G 100 mm insulated needle (Stimuplex A, B-Braun Medical, Melsungen, Germany) was introduced parallel to the ultrasound-guided beam (in-plane technique) from caudad-to-cephalad direction, through the sartorius muscle, directed towards the iliacus muscle, until its tip reached the plane between internal oblique and iliacus muscles. With the needle tip placed beneath the fascia and above the iliacus muscle, local anesthetic (LA) solution 2–4 mL was injected slowly to lift the fascia off the iliacus muscle. After negative aspiration, the rest of LA solution (ropivacaine 300 mg and epinephrine 150 µg, a total of 60 mL) was injected in 5 mL increments to further separate the fascia iliaca from the iliacus muscle. We observed LA spread under real-time imaging between the internal oblique and iliacus muscles. Of note, 60 mL of LA was used to match the volume of LA used by our surgeons for PAI.
Patients randomized to the PAI group received periarticular wound infiltration at the end of the surgery by the surgeon (KE and JW) with significant previous experience in infiltration techniques. The injection solution included ropivacaine 300 mg and epinephrine 150 µg diluted to a total of 60 mL. Using a 22 G, 1.5-inch needle, 20 mL of the solution was infiltrated deep into the posterior capsule and posterior soft tissue, 20 mL was infiltrated in the mid-layer, and 20 mL was infiltrated into the subdermal tissues and around the drain. All injections were performed as the needle was being withdrawn.9
As is common in our practice for patients undergoing THA, a standardized general anesthetic technique was used for all patients including induction with fentanyl (1–2 µg/kg), propofol (~2 mg/kg), and rocuronium (0.6 mg/kg) and maintenance with oxygen/nitrous oxide/desflurane or sevoflurane. Fentanyl 25–50 µg intravenous boluses were administered to maintain mean arterial blood pressure and/or heart rate within 20% of the baseline values. All patients received a standardized perioperative analgesic technique including gabapentin 600 mg and oxycodone CR 10 mg, orally 2 hours, preoperatively. Intraoperatively, patients received dexamethasone 8 mg and acetaminophen 1000 mg, intravenously after induction of anesthesia and ketorolac 30 mg, intravenously during skin closure.
In the postanesthesia care unit (PACU), patients suffering from pain (visual analog scale (VAS, 0=no pain, 10=worst pain)>4/10) received hydromorphone 0.1–0.2 mg intravenous boluses. Postoperative analgesic regimen for the first 24 hours’ period included acetaminophen 1000 mg and gabapentin 300 mg, orally every 8 hours, meloxicam 15 mg orally daily, oxycodone controlled release 10 mg orally the evening of surgery, and hydromorphone 0.2–0.4 mg, intravenous boluses, every 3 hours, as needed as a rescue. In the 24–48 hours’ postoperative period, patients received meloxicam 15 mg daily, gabapentin 300 mg every 8 hours and hydrocodone/acetaminophen 10 mg/325 mg orally every 4 hours, as needed. Rescue antiemetics were administered with complaints of nausea and/or vomiting.
Data collected included patient demographics (ie, age, gender, weight, and height), duration of surgery and duration of PACU stay. In addition, an investigator blinded to group allocation assessed the intensity of pain at rest and on movement using a VAS, opioid consumption (ie, intraoperative period, PACU, and postoperative intravenous and oral opioids). Opioids were converted to equivalents of oral morphine for normalization.11 The incidence and severity of postoperative nausea (none=0, mild=1, moderate=2, severe=3), episodes of vomiting, and need for rescue antiemetics was also documented. All variables were assessed in the PACU, at 2, 6, 12, 24, and 48 hours postoperatively.
Patients were evaluated for sensation to the cold temperature over the lateral and anterior aspects of the thigh and quadriceps weakness in the operative extremity was tested using the approach described by Neal,12 specifically while supporting the knee under the popliteal fossa, the patient was asked to extend the knee against resistance. This approach has also been used by Desmet et al 13 and Bullock et al.14 Measurements were performed in the supine position with the operated extremity measured first, followed by the non-operated extremity. Times to ambulation and readiness to discharge home were recorded.
Statistical analyses
The sample size was calculated using the PASS software. The study was powered to detect a mean difference of 1.5 in pain scores in favor of patients undergoing SFICB procedure assuming an SD of 2.5. With a two-sided alpha level of 0.05, a total of 52 patients would be needed to have 80% power using a repeated measures analysis of variance (ANOVA) F test with six observations on each subject. Correlation on the repeat observations was assumed to be 0.5. Assuming a 14% loss to follow-up, 60 patients were enrolled at 1:1 ratio. Continuous data were summarized as mean and SD or median and IQR. Categorical data were summarized as frequency and percentages. Assumptions of normality for continuous variables were assessed using normal probability plots. Baseline comparisons between the two treatment groups were made using Student’s t-test or Wilcoxon-Mann-Whitney test based on the viability of the normality assumption for continuous variables. Resting and movement VAS scores at different time points were analyzed using a repeated measures ANOVA model with one between-subject (treatment group) and one within-subject (time) factors and their interaction and was followed up with pairwise comparisons between the groups at each time point. Incidences of nausea, vomiting, muscle weakness and sensory changes at each time were compared using Fisher’s exact test. Statistical significance was set at p<0.05 and for each outcome, Bonferroni corrections were used for multiple comparisons. All analyses were done using SAS V.9.3 (SAS).
Results
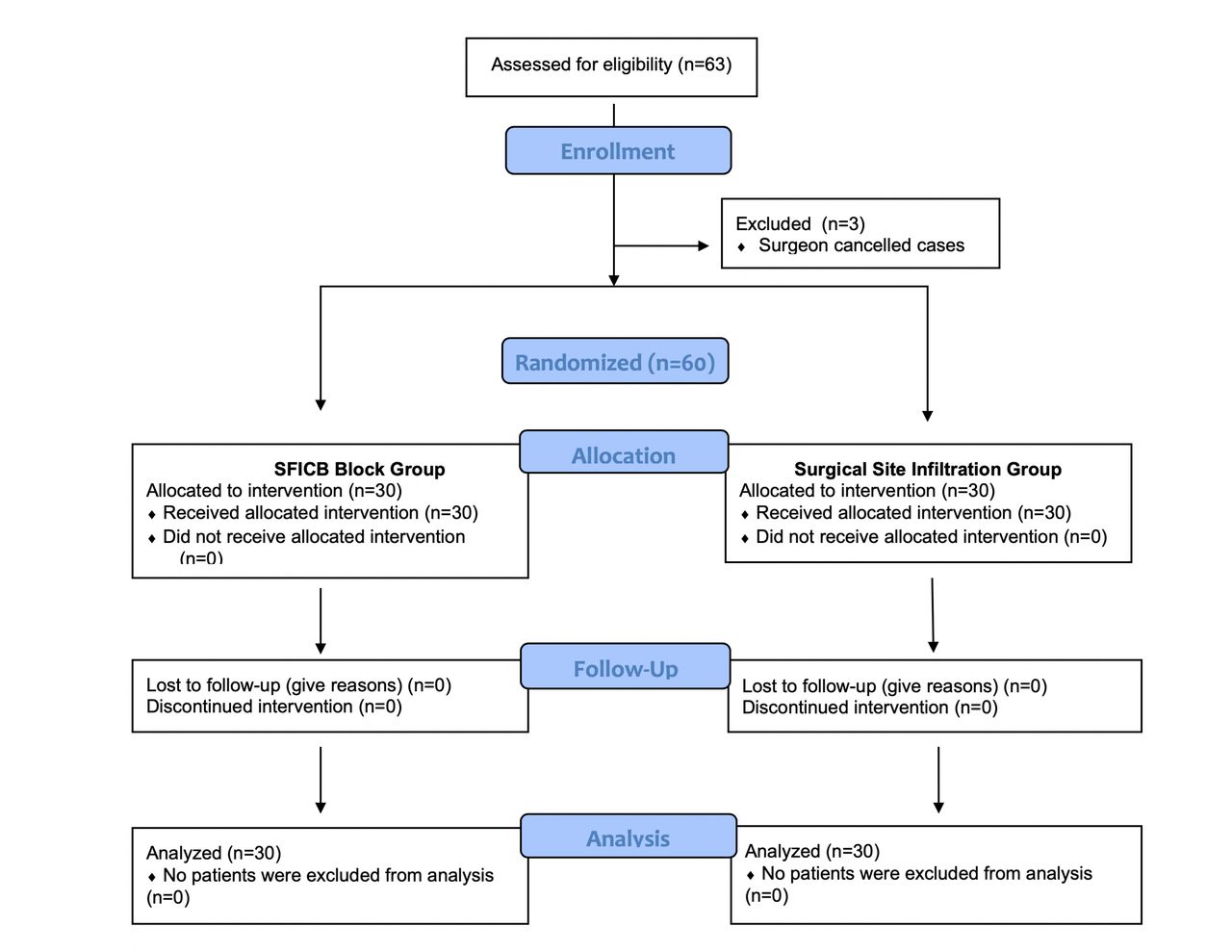
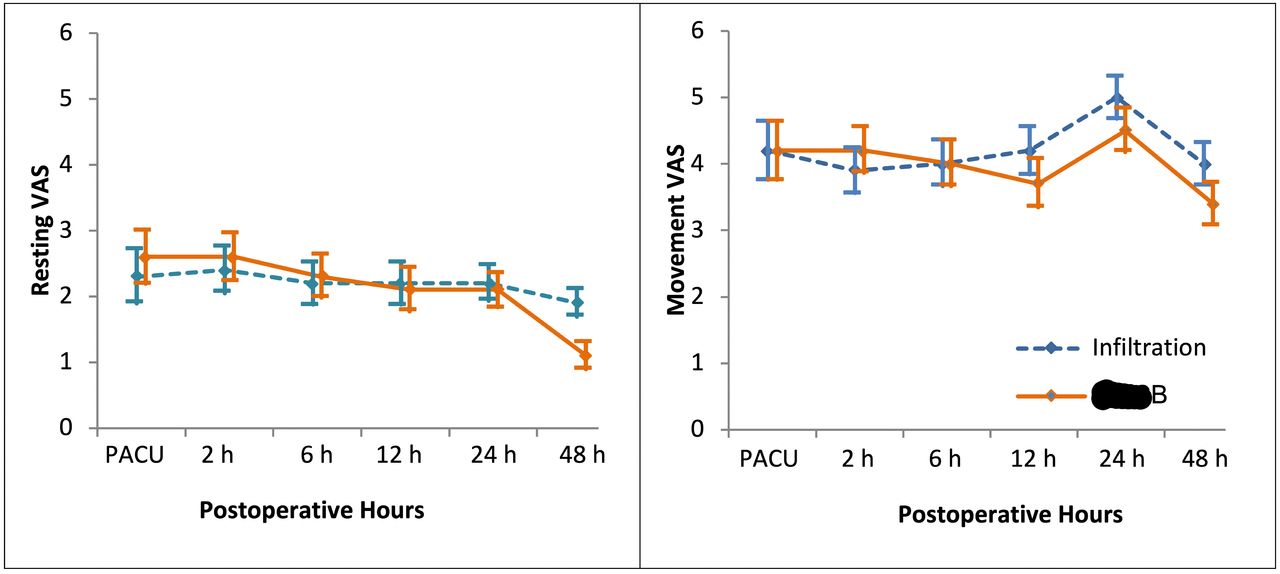
A total of 63 patients were assessed as eligible for the study. The CONSORT flow diagram is presented in figure 1. The groups were comparable with respect to patient demographics (ie, age, height, weight, and body mass index), duration of surgery, and duration of PACU stay (table 1). Opioid requirements at all time points as well as total morphine equivalent requirements were similar in the two groups (table 2). Repeated measures ANOVA revealed that pain scores during resting and with movement changed over time (p<0.01). However, there were no significant differences between the two treatment groups (p>0.50) in terms of pain scores throughout the study period (figure 2). Additionally, no significant interaction between treatment groups and time was found (p>0.23). Consequently, post hoc comparisons between treatment groups at different times were not statistically significant (figure 2).

Flow diagram of screened, randomized, and excluded patients. SFICB, suprainguinal fascia iliaca compartment block.
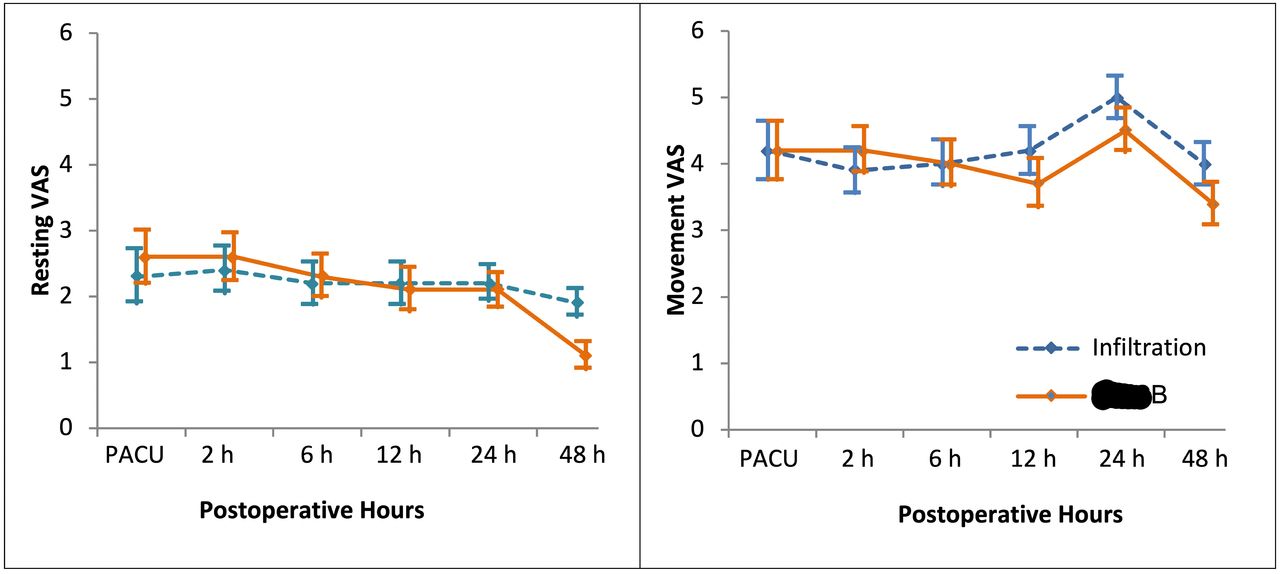
Postoperative pain scores at rest and with movement at various time points. Data are expressed as mean (SE). There were no statistically significant differences between the two groups. PACU, postanesthesia care unit; PAI, periarticular infiltration; SFICB, suprainguinal fascia iliaca compartment block; VAS, visual analogue scale.
Demographic characteristics and clinical variables by treatment assignment
Outcome variables by treatment assignment
The overall incidence of nausea between the two groups across all the time points was not statistically significantly different. In the SFICB group, two patients (3.3%) experienced nausea (nausea score of 2 in both) in PACU, and one patient experienced nausea at 12 and 24 hours (nausea score of 1 at both time points); in the PAI group, two patients (3.3%) suffered from nausea at 2 hours (nausea score of 2 in both). Only one patient in the SFICB block group had emesis at 24 hours and required an antiemetic.
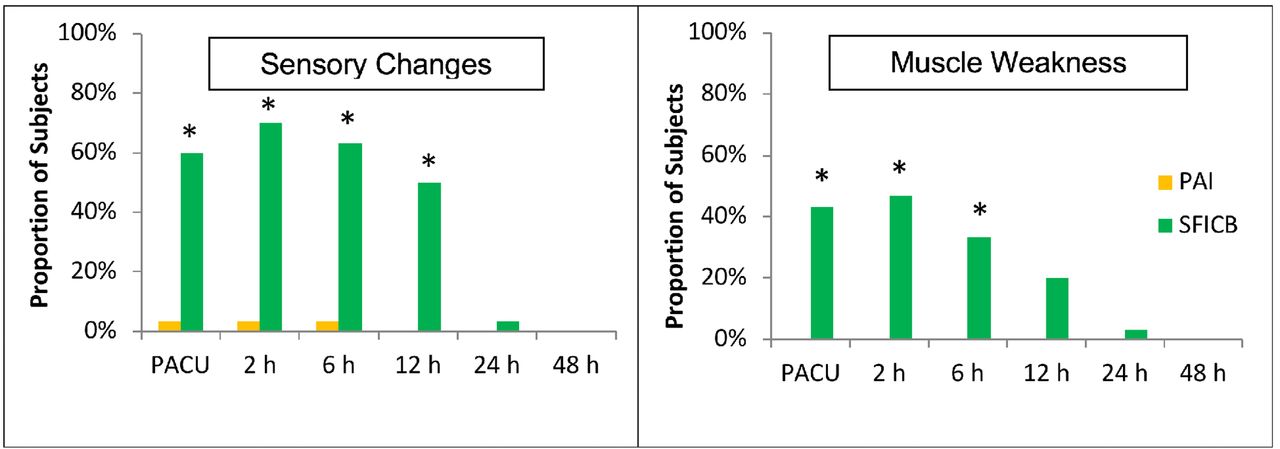
As expected, a significantly higher number of patients in the SFICB group experienced sensory changes over the lateral and anterior aspects of the thigh, which persisted for 12 hours (figure 3). Also, a significantly higher number of patients in the SFICB group experienced muscle weakness in the PACU and at postoperative 2 and 6 hours, p<0.0001 (figure 3). There were no significant differences between time to ambulation and time to discharge readiness (table 2).
{kind=link}
{kind=link}
{kind=link}
Sensory changes and muscle weakness among the treatment groups. Data are expressed as number (%). No subject in the PAI group experienced muscle weakness. Bonferroni adjusted p values for comparing treatment groups at each time are reported. *P<0.001. PACU, postanesthesia care unit; PAI, periarticular infiltration; SFICB, suprainguinal fascia iliaca compartment block.
Discussion
The main finding of this study is that, at the dose and volume of LA used, there were no observed differences between the use of SFICB and PAI after elective THA. Although SFICB was associated with significantly higher incidence of muscle weakness at 6 hours after surgery, there were no clinically relevant consequences such as interference with ambulation or physical therapy because our patients were ambulated on the morning after surgery. However, muscle weakness may be of consequence if the patients were expected to ambulate within 6 hours after surgery (eg, ambulatory surgery setting). Although there was a trend to a faster discharge readiness in the SFICB group, a larger sample size would be necessary to observe statistical differences, if any.
All patients received a well-recognized multimodal analgesic technique including acetaminophen, non-steroidal anti-inflammatory drug, and gabapentin on a scheduled basis. Thus, one may assume that the regional/local analgesic techniques may not be contributing significantly towards pain relief. However, this assumption may be refuted by the fact that all patients required rescue opioids. It is worth mentioning the approach to THA (ie, posterior vs anterior) may influence the degree of postoperative pain.15 16 Patients undergoing THA through the anterior approach have been reported to have significantly less pain than those receiving posterior approach.15 16 Previous studies of SFICB have included patients undergoing THA via the anterior approach13 14 or the approach was not mentioned.5 6
Both PAI and SFICB require meticulous technique to achieve maximal efficacy. The PAI technique used in this study involves numerous injections of small volumes (~1–1.5 mL) of LA solution every 1–2 cm into the deep, middle, and superficial tissue planes.7 We used an SFICB with parasagittal orientation in order to be able to direct the needle in a caudal-to-cranial direction to maximize proximal spread of the flow of LA.10 17 One perceived benefit of the suprainguinal needle placement compared with at or below the level of the inguinal ligament is that the needle tip is further away from the femoral nerve, thus lowering the risk of neural injury.10 In addition, the course of the femoral nerve and lateral femoral cutaneous nerve more consistently lie in the plane between the fascia iliaca and iliacus muscle above the inguinal ligament, thus making blockade at this level more consistently efficacious.10
Significant variation exists in the available literature related to FICB in regard to block technique (eg, landmark-based vs ultrasound-guided approach and infrainguinal vs suprainguinal approach), LA agent, and total LA dose/volume.6 9 13 14 18 19 Such variation makes it difficult to delineate best practices. Given this it is not surprising that the evidence evaluating the analgesic efficacy of FICB for THA has been contradictory.9
The dose (300 mg) and volume (60 mL) of ropivacaine used for SFICB was determined to match that used routinely for PAI by our surgical colleagues. The optimal balance of LA dose and volume to provide effective analgesia while preserving motor function remains unclear. Few studies have included formal assessment of postoperative motor function in patients receiving SFICB,13 14 so it is difficult to ascertain which variables related to the block impact the incidence of motor block as well as any difference in clinical outcomes based on changing such variables.
Previous studies have used a volume of 30–40 mL of ropivacaine 0.5% or bupivacaine 0.25%.5 6 13 20 However, there has been growing appreciation for the use of higher volumes in SFICB to achieve more effective and consistent block. Higher volumes may be necessary due to the fact that the needle tip is not adjacent to a specific neural structure, but is in a fascial plane through which several nerves traverse. Although sufficient dose of LA must be delivered to the target nerves, care must be taken to limit total dose to mitigate the risk of motor blockade and local anesthetic systemic toxicity. Absorption of LAs is dependent on tissue vascularization, and the injection site is an important variable.21 In the study by Desmet et al,13 the total and free serum levels after 40 mL 0.5% ropivacaine were measured at 0.79–1.62 mg/L and 0.036 (0.004–0.07) mg/L, respectively. These concentrations are considered to be safe.22
There are several limitations to this study. First, we did not use a double-blind design or a placebo (ie, sham) group, as it was considered unethical by our institutional review board. Nonetheless, a blinded investigator was used to collect the postoperative data. Also, study participants were blinded as both interventions were done under GA. In addition, the nurses administering opioids were also blinded to the allocated group. Unlike common practice of performing the SFICB preoperatively, we administered the block at the end of surgery to match with the timing of PAI. However, we believe that this might not have influenced intraoperative opioid use, which was minimal (an average of 150–200 µg fentanyl) for a surgical procedure with an average duration of 90–100 min. In our experience, the intraoperative opioid use was similar when we performed the SFICB preoperatively, probably because of our preoperative analgesic bundle that included gabapentin and controlled release oxycodone. Another limitation is that the volume used for SFICB was higher than that used in clinical practice (ie, 60 mL vs 30–40 mL). The higher volume used may have influenced the incidence of reduced motor function observed at 6 hours. We elected to use the same LA dose and volume in both groups to maintain standardization. Of note, our results are specific to patients receiving GA, as it is possible that use of spinal anesthesia may provide different outcomes in the immediate postoperative period.
In conclusion, in patients undergoing elective THA through the posterior approach, PAI and SFICB are equally efficacious with regard to postoperative analgesia and opioid use. However, SFICB was associated with muscle weakness at 6 hours after surgery. Further studies are needed to determine the optimal LA dose and volume for SFICB to provide analgesia while preserving motor function.
References
Footnotes
Presented at Interim data from this work were presented at the 2018 World Congress on Regional Anesthesia and Pain Medicine in New York, NY, 19 April to 21 April 2018.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests GPJ has received honoraria from Pacira Pharmaceuticals (Exparel), Baxter Pharmaceuticals, Mallinckrodt Pharmaceuticals, and Merck Pharmaceuticals.
Patient consent Obtained
Ethics approval This study was approved by the Institutional Review Board of University of Texas Southwestern Medical Center, Dallas, Texas, USA.
Linked Articles
- PostScript
- PostScript
- PostScript