Article Text

Abstract
Backgrounds and objectives The anterior approach to the subomohyoid suprascapular (SOS) nerve is a new, technically easy and reliable regional anesthesia technique for postoperative shoulder analgesia. However, due to its proximity, the injectate may spread to the brachial plexus and phrenic nerve. The goal of this anatomic study with dye injection in the subomohyoid space and subsequent cadaver dissection was to establish the likely spread of local anesthesia and the extent of brachial plexus and phrenic nerve involvement resulting from ultrasound-guided SOS nerve block.
Methods The suprascapular nerve (SSN) under the inferior belly of omohyoid muscle in the posterior triangle of the neck was identified. Using a contrast dye, 10 ultrasound-guided SOS nerve injections of 5 mL were done bilaterally, in five fresh cadavers. The area was then dissected to evaluate the spread of the contrast dye in the immediate proximity of the brachial plexus, phrenic and SSN.
Results The SSN and omohyoid muscle were easily identified on each cadaver. SOS nerve staining with contrast dye was seen in 90% of dissections. The superior trunk was stained in 90% and the middle trunk was stained in 80% of dissections. The inferior trunk was stained in 20% of dissections. A spread of dye around the SSN was observed in 90% and the phrenic nerve was mildly stained in 20% of the dissections.
Conclusion In-plane ultrasound-guided needle injection with a 5 mL volume for SOS block was sufficient to stain the SSN. This conservative volume involved other parts of the brachial plexus and may potentially spread to the phrenic nerve. Further clinical studies are required for confirmation.
- anatomy
- regional anesthesia
- ultrasound in pain medicine
Statistics from Altmetric.com
Introduction
Ultrasound-guided (USG) suprascapular nerve (SSN) block has been recommended as a substitute for interscalene block (ISB) to allow phrenic nerve sparing.1 ISB, the accepted gold standard regional anesthetic technique for perioperative shoulder analgesia,2 was associated with a high incidence of phrenic nerve blockade in the past3 and continues to do so, despite abundant alterations in techniques.4
The best technique for the SSN block remains uncertain with posterior as well as anterior approach descriptions. The classic posterior approach to the nerve was first introduced in 1941.5 This approach to the SSN (in the supraspinatus fossa) proposed as an alternative analgesic block while preserving phrenic nerve function6 can be associated with higher technical failures.7 It has been modified multiple times, is technically challenging and has shown conflicting results.8 The anterior approach (in the supraclavicular fossa) has been recently proposed as a reliable and easy technique9 with similar efficacy for shoulder surgery.10 However, the proximity to the brachial plexus in this region may result in a potential extension of local anesthetic to the phrenic nerve if conventional large volumes are used. Although sonographic measurements of the SSN and omohyoid have been done,11 there is not enough literature defining the spread of the local anesthetic to the phrenic nerve during SSN block. In a volunteer study of SSN block, smaller volumes of 1 mL resulted in only 40% success.12 Studies to ascertain the volume that would preserve efficacy while sparing the phrenic nerve are awaited.13
The primary outcome of this study was to evaluate the spread of 5 mL fixed volume injectate following in-plane USG subomohyoid suprascapular (SOS) injections in fresh cadavers. The secondary outcome included the extent of brachial plexus staining. Based on the hypothesis that the injectate can be effectively and safely administered deep to the superficial cervical fascia, laterally within the inferior posterior triangle of the neck. We predicted that using the inferior belly of omohyoid as a landmark, low volumes (5 mL) of injectate will limit the spread to the phrenic nerve while staining the SSN in a satisfactory manner.
Methods
Between January and July 2017, body bequeathal programme at Western University, London, Ontario, Canada, in accordance with the Anatomy Act of Ontario and Western’s Committee for Cadaveric Use in Research (approval number #24062016) provided all specimens that were dissected in the department of Anatomy at the Schulich School of Medicine, Western University, London, Canada. Five unembalmed (cryopreserved) adult human cadavers were thawed to room temperature for 3 days prior to the study. Emaciated cadavers or those with any apparent pathology or surgery in the neck over the supraclavicular area were excluded.
Block technique and anatomic dissection
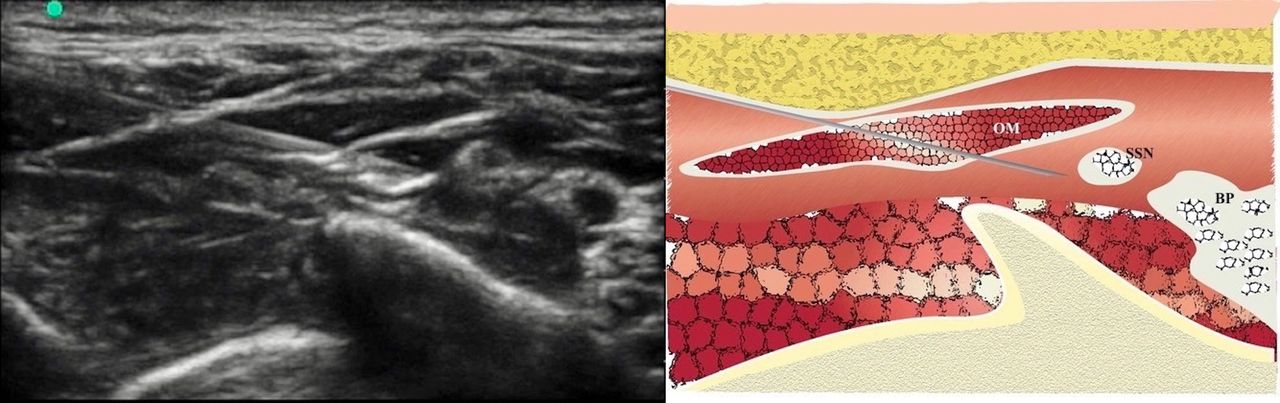
With cadavers in the supine position, the supraclavicular fossa was scanned using a protective sheath covered linear transducer (13–6 MHz; Fujifilm, SonoSite, USA). The SSN was identified under the inferior belly of omohyoid muscle in the supraclavicular area with the method described by Siegenthaler et al.14 Using an in-plane approach, a 50 mm, 22G insulated needle (Pajunk, Geisengen, Germany) was advanced in the lateral to medial direction in the supraclavicular area. After confirming the correct plane with 0.5 mL normal saline, 5 mL of a methylene blue dye mixture (15 mL 0.5% methyl cellulose, 5 mL of 1% methylene blue, 10 mL of 0.9% NaCl) was injected directly through the needle in real-time ultrasound vision (figure 1). The viscosity of fluid and injection approach was designed to be comparable to clinical procedures and determined best for the spread and staining based on experience from our center.15 This volume was selected arbitrarily.
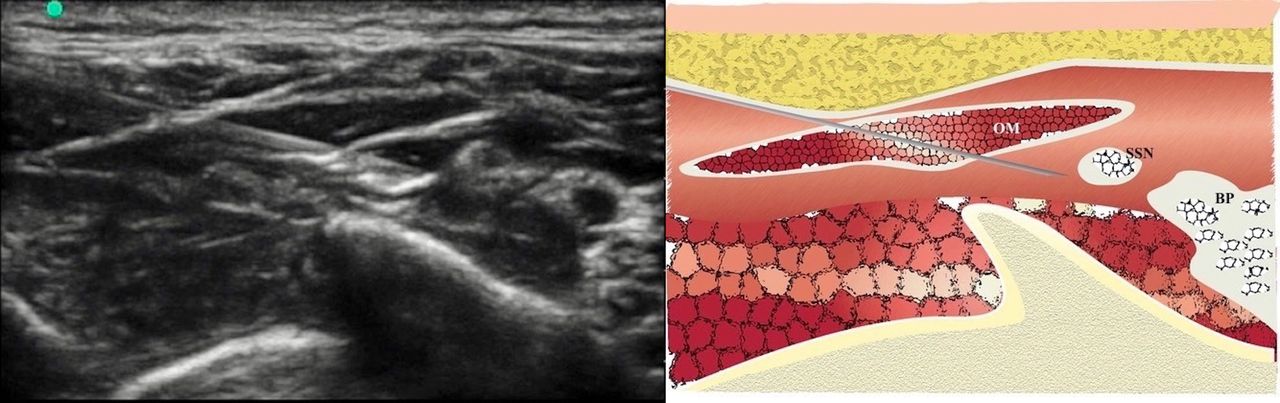
Ultrasound-guided dye injection in the subomohyoid space with the needle approaching the suprascapular nerve under the omohyoid muscle and surrounding brachial plexus and its schematic representation. BP, brachial plexus; OM, omohyoid muscle; SSN, suprascapular nerve.
Dissection of the supraclavicular area 15 min after the injection exposed the brachial plexus. A skin incision along the superior border of the clavicle from the sternum to its lateral end was followed superiorly along the posterior border of the sternocleidomastoid muscle and the skin flap reflected upward and laterally. The clavicular head of the sternocleidomastoid was reflected. The investing fascia was removed to identify and reflect the transverse cervical and suprascapular vessels. The inferior belly of the omohyoid was identified crossing this inferior aspect of the posterior triangle. The deeper prevertebral fascia was excised and the trunks of the brachial plexus identified emerging between the anterior and middle scalene muscles. The phrenic nerve was landmarked superficial to the anterior scalene muscle. The SSN was identified leaving the superior trunk of the brachial plexus, traveling in the intermediate space between the investing superficial cervical fascia and the prevertebral fascia, first inferior and then parallel to the inferior belly of the omohyoid. The arrangement of the SSN in relation to the omohyoid muscle and phrenic nerve in relation to the anterior scalene muscle were then evaluated. The observations recorded and documented photographically included staining of the SSN, other parts of the brachial plexus, phrenic nerve as well as the length of the SSN stained and horizontal and vertical spread of the dye around the brachial plexus. The staining intensity was graded on a four-point scale (0=no staining, 1=weak staining, 2=moderate staining, 3=strong staining). Distances were measured by a caliper and a measuring scale. Data are expressed as mean±SD (range).
Results
Five cadavers (two women and three men) with a mean age at death of 82 years (range 75–90 years) were examined, bilaterally.
The SSN was identified in all cadavers using ultrasound. It was seen arising from the superior trunk of the brachial plexus, lying under and then parallel to the omohyoid muscle and then passing posteriorly through the inferior part of the posterior triangle, toward the superior aspect of the scapula. Of the 10 completed injections, one failed as the dye was deposited above the investing superficial cervical fascia of the omohyoid muscle and did not reach the SSN or the brachial plexus. Circumferential contrast dye staining of the SSN was present in 9 of the 10 injections performed with seven showing strong staining. Details regarding the SSN staining can be found in the supplemental files.
It was easy to separate the brachial plexus trunks, but some dissection was needed to separate the connective tissue between them. The anatomic arrangements of the trunks were consistent as was the relationship of the SSN. There was some spread to the trunks of the brachial plexus with average dye distribution of 49.8±12.4 (range 27–60) mm in the craniocaudal and 46±−12 (range 34–67) mm in the mediolateral dimension. There was spread to the inferior trunk in two dissections (cadaver 5, bilaterally).
In seven dissections, the phrenic nerve staining was absent and in two dissections the staining was mild (online supplementary file). The shortest distance from the dye stain to the phrenic nerve in the cadavers where it was not stained was 14±5.96 (range 3–20) mm. Summary of staining characteristics is in table 1 (online supplementary file). The figure 2 shows the characteristic spread of the contrast dye in the dissections.
Characteristics of dye dispersion in all studies

{kind=link}
{kind=link}
Suprascapular nerve (SSN) dissection. Dye stained SSN seen emerging from the superior trunk (ST) and parts of the brachial plexus with phrenic nerve (PN) sparing.
Discussion
The findings of our study support the technical ease and reliability of the anterior approach to the SSN, under the inferior belly of the omohyoid muscle. Our aim was to define the anatomy and the location of the SSN and the phrenic nerve and thereby establish the anatomic basis for USG SOS nerve block using an arbitrary volume of 5 mL of dye to mimic the local anesthetic. Our findings show that the superior and middle trunks were fairly close together and the injection showed irregular but consistent spread involving both. This is the first study to demonstrate that such injections are likely to spread to both these trunks of the brachial plexus with a small likelihood of staining of the inferior trunk.
The ISB along with multimodal analgesia is the standard for perioperative shoulder analgesia but carries risk of respiratory complications due to the adjacent phrenic nerve involvement.16 In addition, higher risk of nerve damage,17 rebound pain18 and other undesirable effects19 have augmented the interest in finding safer alternatives and diaphragm-sparing techniques for shoulder analgesia. SSN supplies a large portion of the shoulder joint20 and in all likelihood, its block would provide considerable analgesia. First introduced in 1941,5 various safer modifications to the classic posterior approach to SSN block have been studied.21 USG anterior approach was described in 2012.14 A recent systematic review has challenged the accepted dominance of ISB over SSN for shoulder analgesia.1 Though the axillary nerve supplies rest of the joint, the evidence for axillary nerve supplementation is still unclear.22
The findings of our study support the technical ease and reliability of the anterior approach to the SSN, under the inferior belly of the omohyoid muscle. The findings show that the superior and middle trunks were fairly close together and the injection showed irregular but consistent spread involving both. This is the first study to demonstrate that such injections are likely to spread to both these trunks of the brachial plexus with a small likelihood of staining of the inferior trunk. The deep cervical fascia, also known as the prevertebral fascia, separates the SSN and the brachial plexus and even though the needle did not penetrate it, the dye did track to parts of the plexus. This tracking may have a positive effect on the extent of analgesia in a clinical situation. The SSN was targeted and stained in all but one injection where the dye was above the plane of interest. When injected above the plane, the blue color of the dye seemed to spread all over the supraclavicular area, but there was an unbroken investing layer of the superficial cervical fascia through which the needle did not penetrate to reach the SSN. Mild staining of phrenic nerve in two of nine dissections (when the dye was deposited in the correct plane) suggests that this possibility exists, even with a conservative volume of 5 mL. In their anatomical treatise, Kodama et al have mentioned a 3% incidence of ‘ phrenicosuprascapular communications’ and the possibility of the dye tracking to the phrenic nerve via these could not be ruled out.22 However, it stands to reason that incidence of diaphragmatic involvement would be indirectly proportional to the distance from the nerve roots.23
Similar to prior studies, we elected to use unembalmed cadavers to prevent alterations in the tissue characteristics by embalming process.24 Position of the needle tip in relation to the omohyoid muscle and its investing fascia is pivotal. We ascertained that the SSN block should involve injection below the superficial cervical fascia that is the investing layer of the omohyoid muscle and only then the drug would enter the anatomic subomohyoid space and reach the SSN. We also chose to use a fixed 5 ml volume. Without volume studies for SSN nerve block, our results explain, at least partly the extent of spread of a fixed 5 ml volume for this block. Though this was a cadaver study, we observed definite phrenic sparing in a majority of dissections.
This study has several limitations. First, cadaver tissues may behave differently from living tissues25 and the spread of the dye may not be similar. Second, though we tried to match the physical properties of the injectate, its behavior may not have been identical to the local anesthetic. Third, the dissection itself may have influenced the dye spread though there was a time period of 15 min between the injection and dissection. Fourth, injection of local anesthetic may spread to the phrenic nerve due to slow diffusion or tissue absorption, in vivo. A cadaveric study is ill-suited to illustrate this. However, this is the first study to address questions regarding the spread of the injectate to other structures in the vicinity, particularly the brachial plexus and the phrenic nerve in the setting of a SOS block.
Our study raises a number of questions for future research. First, volume studies in vivo may add to our observations in cadavers. It is possible that the dye spread may have been different if a smaller volume was used. Second, further dissection may reveal the caudad extent of the injectate spread. Third, clinical dose and volume studies might examine and confirm these findings for the anterior approach.
In conclusion, our cadaveric study is a proof of the concept that USG SOS nerve block is technically easy and a reliable technique. It also establishes that such injections invariably involve other parts of the brachial plexus and may potentially spread to the phrenic nerve despite the use of conservative volumes warranting further cadaveric and clinical studies for this novel block.
Acknowledgments
We wish to thank the staff of the department of Anatomy and Cell Biology, Western University, London, Ontario, Canada.
References
Footnotes
Contributors SD, HS and MJ contributed to the study design, planning and study conduct. SD contributed to the writing of the manuscript. SD and MJ revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- PostScript
- PostScript