Article Text

Abstract
Background and objectives Both posterior quadratus lumborum (QL) and erector spinae plane (ESP) blocks have been described as new truncal interfascial plane blocks. Distribution of injectate is influenced by fascial anatomy; therefore, different injection sites may produce similar spread. This anatomic study was designed to test the hypothesis that a posteromedial QL block at L2 level will more closely resemble a low thoracic ESP block when compared with the posterolateral approach at L2 level.
Methods Left-sided ESP blocks were performed in six cadavers at T10–11. Three of these cadavers received right-sided posteromedial QL block at L2, while the other three received right-sided posterolateral QL block at L2. All injections were composed of 20 mL methylcellulose 0.5 % mixed with India ink and 10 mL of Omnipaque (Iohexol) 240 mg/mL. CT 24 hours after injection and cadaver dissection were used to evaluate injectate spread.
Results Cephalocaudal spread of injectate by CT and cadaveric dissection was highly correlated (r=0.85 [95% CI 0.51 to 0.95]). Cadaver dissection showed ESP injectate spread deep to the muscle (mean [SD]) 11.7 (2.3) levels compared with 7.3 (1.2) levels for posterolateral QL and 9.7 (1.5) for posteromedial QL (p=0.04 overall, with a statistically significant pairwise difference between ESP and posterolateral QL only). The subcostal nerve and dorsal rami were commonly involved in most blocks, but the paravertebral space and ventral rami had inconsistent involvement. The lumbocostal ligament limited cranial spread from the posterlateral QL block approach.
Conclusions The posteromedial QL block at L2 produces more cranial spread beyond the lumbocostal ligament than the posterolateral QL block, and this spread is comparable with a low thoracic ESP block. Both posterior QL and ESP blocks show unreliable spread of injectate to the paravertebral space and ventral rami, but the dorsal rami were frequently covered.
- regional anesthesia
- interfascial plane blocks
- quadratus lumborum block
- erector spinae plane block
- cadaver
- anatomy
Statistics from Altmetric.com
- regional anesthesia
- interfascial plane blocks
- quadratus lumborum block
- erector spinae plane block
- cadaver
- anatomy
Introduction
The recent rise in ultrasound-guided interfascial plane block techniques has generated a number of questions regarding the indications, comparative effectiveness and nomenclature of these regional anesthesia procedures.1 In particular, the erector spinae plane (ESP) and quadratus lumborum (QL) blocks have both been described for similar surgical procedures, such as abdominal wall hernia repair.2 3
High thoracic dermatomal blockade with posterior QL block has been described clinically but not reliably demonstrated in cadaveric studies.4–6 In contrast, ESP injections deep to the erector spinae (ES) musclesin cadavers show craniocaudal spread in the midthoracic and upper thoracic levels in the immediate vicinity of the dorsal and ventral rami of the thoracic spinal nerve roots.6–8 The fascial plane deep to ES is in continuity with the tissue plane posterior to the QL muscle, which is the point of the injection for posterior QL block and potentially may serve as a route for injectate spread to the thoracic spinal nerve roots.1
Anatomically, the lumbocostal ligament and architecture of the QL muscle may affect injectate spread.7–9 The lateral part of the QL muscle is multisegmental, and the medial part is unisegmental.9 10 The lumbocostal ligament is a thickened cranial portion of the middle thoracolumbar fascia (MTLF) that is posterior (superficial) to the QL muscle.10 This ligament has the potential to restrict the cranial spread of local anesthetic deep to the ES muscle. To date, no published studies have assessed the differences in injectate spread between posterior QL and ESP blocks. Moreover, it is unknown which location of injection for posterior QL blocks, either medially or laterally, may more closely resemble ESP blocks. This anatomic study was therefore designed to assess injectate spread after simulated low thoracic ESP and L2 posterior QL blocks. We hypothesized that the fascial plane deep to the ES muscle is in continuity with the plane superficial to the QL muscle; thus, a posteromedial approach to the QL block will lead to greater cephalocaudal spread than a posterolateral injection.
Methods
Six non-embalmed adult cadavers were chosen to constitute different genders and body habitus. Cadavers with evidence of spine deformities or previous back surgery were excluded. All cadavers were maintained at room temperature for at least 24 hours before injections and additional 24 hours before the imaging and dissection. All procedures (simulated blocks) were performed in the prone position by one investigator (HE).
Ultrasound-guided left-sided low thoracic ESP blocks were performed in six cadavers. Three of these cadavers also received ultrasound-guided L2 right-sided posteromedial QL block11; the other three received right-sided L2 posterolateral QL block. All injections were performed with an 8 cm, 17-gauge echogenic Tuohy needle (Pajunk, Geisingen, Germany), and the injectate consisted of 20 mL methylcellulose 0.5% mixed with India ink and 10 mL of Omnipaque (Iohexol) 240 mg/mL.
Posterior QL block technique
A low-frequency curvilinear transducer (2–5 MHz, Fujifilm SonoSite, Bothell, Washington, USA) was placed in a transverse orientation 3–4 cm lateral to the midline at L1–2 level to view the L2 vertebral body, L2 transverse process, latissimus dorsi, QL and psoas major muscles in transverse plane. For posterolateral QL block, the needle was advanced lateral-to-medial in-plane through the latissimus dorsi to position the needle tip posterolateral to the QL muscle and within the MTLF (figure 1A). Correct needle tip position was confirmed after injecting 2–3 mL of sodium chloride 0.9% followed by the injectate mixture (figure 1B). For posteromedial QL block approaches, the needle tip was advanced posterior to the medial edge of the QL muscle (attachment of the QL muscle to the transverse process of L2) between the QL muscle and ES muscle and within the MTLF (figure 1A). Appropriate location was confirmed with sodium chloride 0.9%, observing injectate spread toward the posterior midline, transverse process and the intertransverse region. The dye mixture was then administered, seeking spread between the QL and the iliocostalis part of the ES muscle (figure 1C).
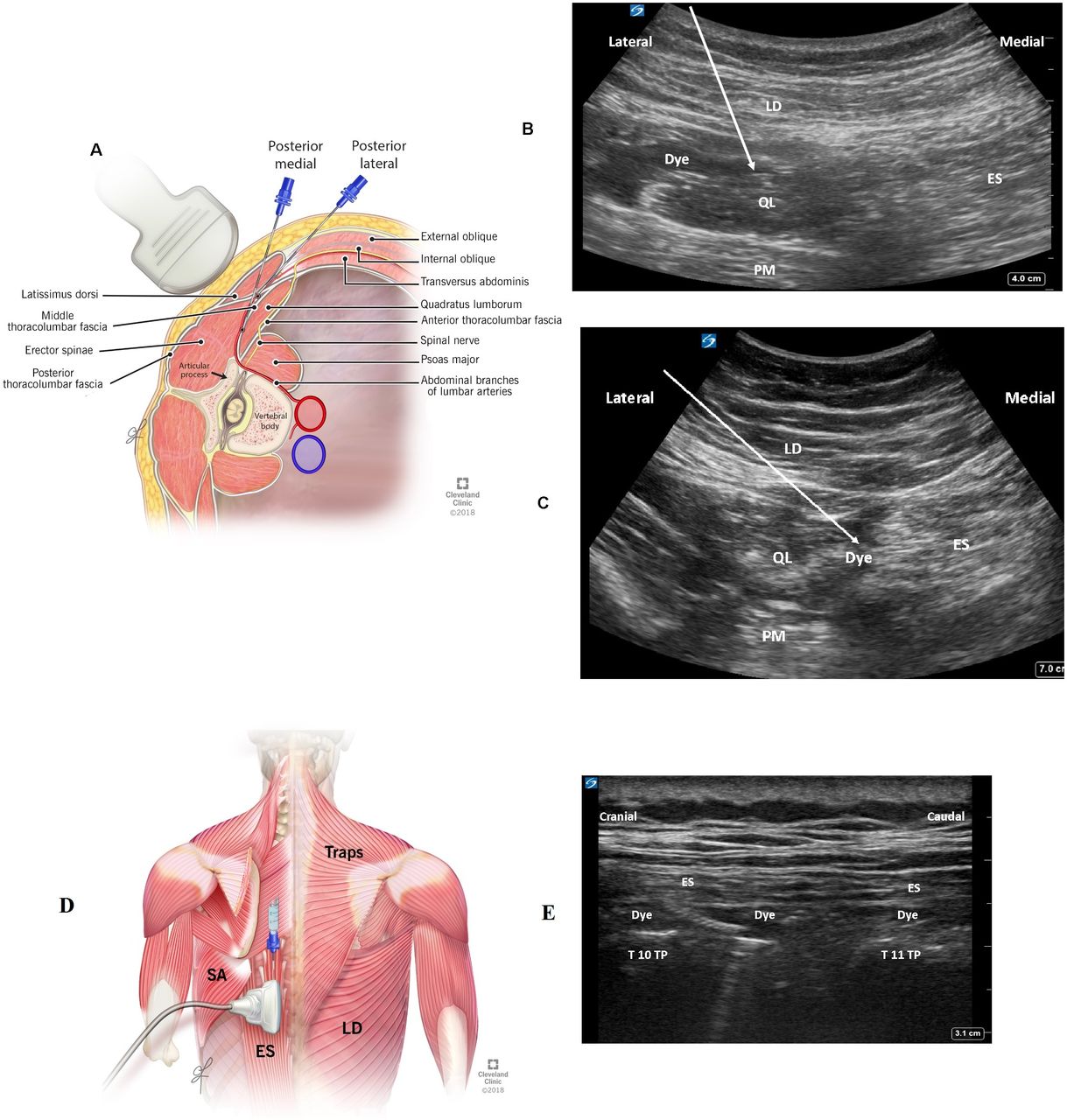
(A) Illustration showing the ultrasound transducer position when performing posterior quadratus lumborum block in two locations: lateral and medial. (B) Ultrasound image demonstrating sonographic landmarks, needle approach (white arrow) and dye spread in posterolateral QL block. (C) Ultrasound image demonstrating sonographic landmarks, needle approach (white arrow) and dye spread in posteromedial QL block. (D) Illustration demonstrating landmarks and needle approach to the erector spinae plane block. (E) Ultrasound image demonstrating sonographic landmarks and needle approach to the erector spinae plane block. ES, erector spinae; LD, latissimus dorsi; QL, quadratus lumborum; TP, transverse process.
ESP block technique
A high-frequency linear transducer (5–12 MHz, 4C–SC, Fujifilm SonoSite) was placed between T10–11 lateral to the spinous process in a parasagittal orientation. The ES muscle was identified superficial to the transverse processes. The needle was advanced in-plane in a craniocaudal direction, through the ES muscles to position the needle-tip in the tissue plane deep to the ES muscles and superficial to a point midway between the T10 and T11 transverse processes and intertransverse muscles (figure 1D). Correct needle-tip position was confirmed after injecting 2–3 mL of sodium chloride 0.9% followed by injectate mixture, seeking craniocaudad spread deep to the ES muscles and superficial to the transverse processes, the intertransverse muscles and connective tissue (figure 1E).
Cadaveric imaging
Twenty-four hours after injection, the cadavers underwent 128-slice CT scan (Siemens Flash CT; Somatom Definition Edge; Siemens Healthcare, Malvern, Pennsylvania, USA). High-resolution CT with volume rendered three-dimensional reconstruction images (transverse, sagittal and coronal) were created to evaluate the spread of the contrast. Images from C7 to S1 were acquired using routine spine protocol with 120 Kvp, 300 mAs reference mAs, rotation time 1 s, pitch 0.8, 0.6 mm collimation. Diagnostic images were acquired at 1.0 mm slice thickness with 1.00 mm interval using a soft tissue algorithm. All scans were reviewed by a staff radiologist, staff anesthesiologist and a chief radiology technician. All were blinded to the injection technique.
Cadaveric dissection
The cadavers were dissected in the prone position bilaterally in layers from superficial to deep by an anatomist (RD). Longitudinal (C6–L5) and transverse (midthoracic) incisions were made. The latissimus dorsi muscle was reflected laterally allowing visualization of the ES muscles. Then, the ES muscles were reflected medially to identify the thoracic transverse processes and the origins of the dorsal rami. The craniocaudal and mediolateral extent of contrast spread deep to the ES and serratus anterior muscles was evaluated. Dissection was also performed to identify dye spread, if applicable, to the transversus abdominis plane (TAP), intercostal spaces, thoracic paravertebral spaces, ventral rami, intercostal nerves, pleura and posterior aspect of the QL muscle. Specifically, spread to the paravertebral space was defined as dye present within the paravertebral space or involvement of the ventral rami within this space. Dye within the retrolaminar space was defined as staining in the tissue plane deep to the ES muscles and superficial to the lamina. The dorsal rami, subcostal nerves, and ilioinguinal and iliohypogastric nerves were also identified. From T11–L2 deep to the ES muscles and superficial to the QL muscle attachment to the last rib, the lumbocostal ligament and the dye in relationship to the ligament and middle layer of the thoracolumbar fascia was identified. The epidural space was not dissected. The stepwise progression of the anatomic dissection was photographed, documented and reviewed by two investigators (HE and RD).
Statistical analysis
Statistical analysis was performed using NCSS Statistical Software (NCSS, LLC, Kaysville, Utah, USA). A prior sample size was not estimated since the availability of cadaver specimens dictated a convenience sample. For the purposes of analysis, each injection was considered an independent event. Normality of distribution was determined for the outcome variables (number of levels by CT and cadaver dissection) using the Kolmogorov-Smirnov test. Pearson’s r was used to measure the strength of association between the two outcomes. If normally distributed, comparisons by injection technique were performed using two-way analysis of variance with post hoc Tukey-Kramer multiple comparison test. Comparisons of outcomes based on sex and obesity status (body mass index [BMI] ≥30) were performed using Student’s t-test. For all comparisons, p<0.05 was considered statistically significant.
Results
Baseline characteristics of the cadavers are shown in online supplementary table 1. All procedures were successfully performed. The results of radiologic evaluation and dissection are listed in online supplementary tables 2 and 3, respectively. The craniocaudal extent of dye spread evaluated by CT imaging and dissection is summarized in figure 2. Cephalocaudal spread of injectate by CT and cadaveric dissection was highly correlated (r=0.85 (95% CI 0.51 to 0.95]).
Supplemental material
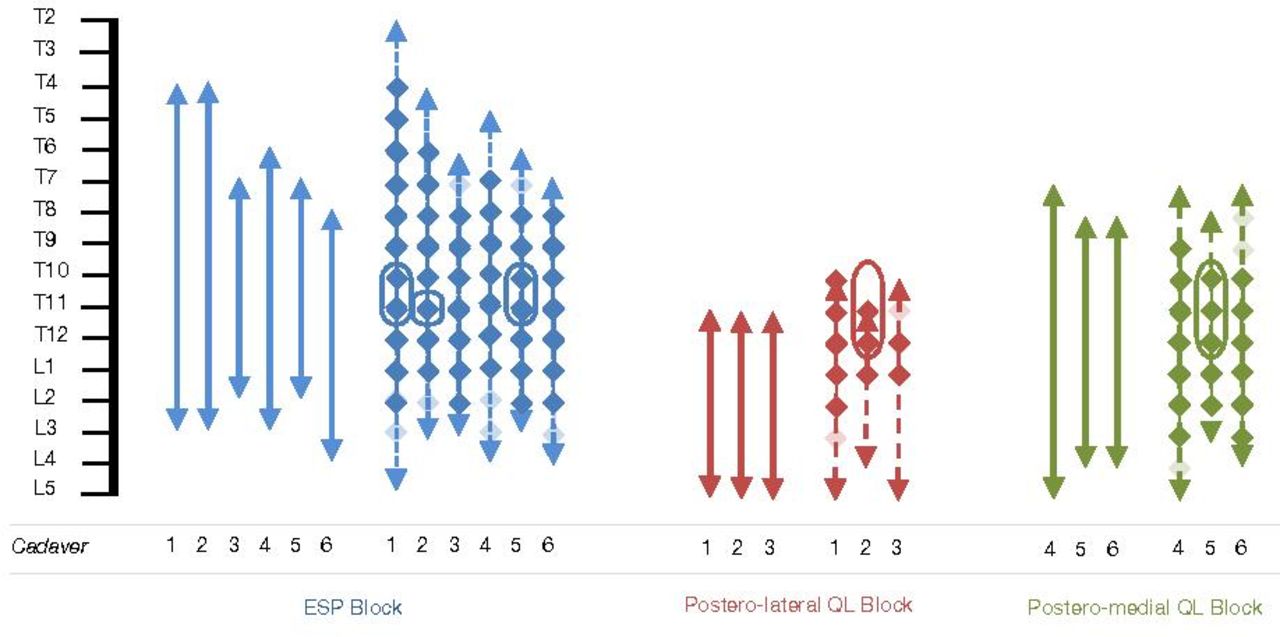
Craniocaudal extent of dye spread deep to the erector spinae muscle in cadavers as seen by CT scan and dissection. Plain arrows denote extent of dye in CT scan, while dotted arrows denote extent of dye spread in dissection. Solid diamond denotes darkly stained dorsal rami, and faded diamonds denote faintly stained dorsal rami as seen in dissection. Circles around diamonds represent levels in which staining of the ventral rami within the paravertebral space took place. ESP, erector spinae plane; QL, quadratus lumborum.
CT imaging demonstrated injectate spread following low thoracic ESP (mean [SD]) 9.8 (1.8) levels compared with 7.0 (0.0) levels for L2 posterolateral QL block and 9.7 (1.2) levels for L2 posteromedial QL block (p=0.06 overall with no pairwise differences). On cadaver dissection, the ESP injectate spread 11.7 (2.3) levels compared with 7.3 (1.2) levels for posterolateral QL and 9.7 (1.5) for posteromedial QL (p=0.04 overall with a statistically significant pairwise difference between ESP and posterolateral QL only). Injectate spread for female and male cadavers was similar by CT (p=0.92) and dissection (p=0.88). There were also no differences in injectate spread between obese (BMI ≥30) and non-obese (BMI <30) cadavers by CT (p=0.46) and dissection (p=0.34).
ESP block
Radiologic results
The highest level achieved was T4, and the lowest level was L4, and the median cephalocaudal spread of dye deep to the ES muscle was 9.5 vertebral segments (figure 3A). Contrast spread laterally to the junction between transverse process and rib in all but one cadaver, where it spread to the posterior axillary line. Transverse imaging of cadavers demonstrated caudal contrast spread between ES and QL muscles to L3 in all but one cadaver, where it spread to L2. All cadavers demonstrated evidence of dye spread to the retrolaminar space, while there was no evidence of spread to the epidural, intercostal, intraperitoneal space or transverse abdominis plane. Only one of the cadavers (cadaver 4) demonstrated spread of dye to the paravertebral space (figure 3B).
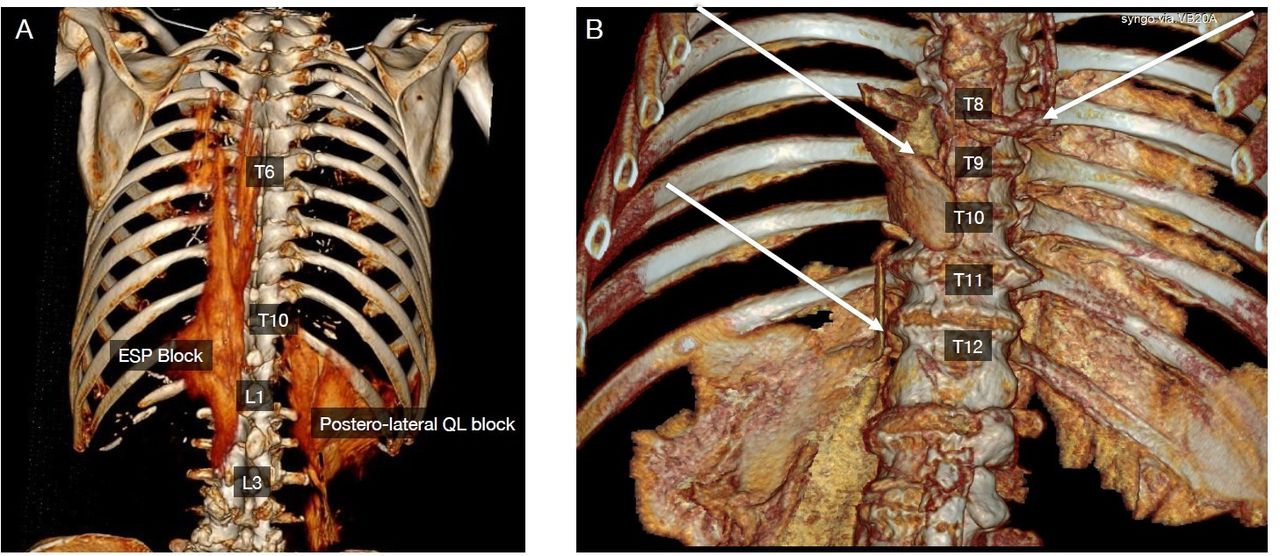
(A) CT three-dimensional reconstruction sagittal image (posterior view) following ESP plane block (left side) and posterolateral QL block (right side). The ESP block was associated with cephalocaudal contrast spread from T4–L3. The posterolateral QL block was associated with cephalocaudal contrast spread from T10–L4. (B) CT three-dimensional reconstruction sagittal image (anterior view) following ESP block (right side of the image) and posteromedial QL block (left side of the image). The ESP block was associated with contrast spread anterior to the transverse processes and into the paravertebral space at T8 (right white arrow). The posteromedial QL block was associated with contrast spread anterior to the transverse processes and into the paravertebral space at T9–12 (left white arrows directed to the paravertebral contrast spread). ESP, erector spinae plane; QL, quadratus lumborum.
Dissection results
The highest level for dye spreads deep to the ES muscle achieved was T2, the lowest level was L5 and median of 11.7 levels (figure 4A). Three out of six cadavers demonstrated lateral spread deep to the serratus anterior muscle. Four to five dorsal rami were stained in all cadavers below the point of injection (T10–T11), while three to seven dorsal rami were stained with dye above the point of injection (figure 4B). The subcostal nerve was stained in all six cadavers. None of the cadavers demonstrated staining of lumbar nerve roots or branches of the lumbar plexus. All but one cadaver demonstrated dye spread to the retrolaminar space. The paravertebral space was faintly stained at T10–11 level in three cadavers. There were faint intercostal nerves spread restricted to level T9–T12 in three cadavers and at T11 in one cadaver. None of the cadavers demonstrated spread of dye to pleura, intraperitoneal space or the TAP.

Cadaveric specimen following erector spinae plane (ESP) block. (A) Dye staining can be seen deep to the ES muscle extending from T6 down to T12 and caudal to the LCL. (B) Dye staining can be seen deep to the ES muscle extending from T7–L3 posterior to the quadratus lumborum (QL) muscle. DR, dorsal root; ES, erector spinae; LCL, lumbocostal ligament; PP, parietal peritoneum; PVS, paravertebral space.
Posterolateral QL block
Radiologic results
Contrast distribution consistently spread from T11–L5 (figure 3A). Two of the three cadavers had lateral contrast spread up to the posterior axillary line, while the third had lateral spread up to the midaxillary line. One of the cadavers demonstrated medial spread deep to the ES muscles and in the retrolaminar space (cadaver 1). In addition, one cadaver demonstrated spread to the paravertebral space at level T10–12 (online supplementary figure 1). There was no evidence of intercostal, intraperitoneal or TAP spread.
Supplemental material
Dissection results
The highest level achieved of dye spread deep to the ES muscle was T10 with the lowest level L5 (figure 5A). There was cranial dye extension to the lumbocostal ligament in one cadaver, while the other two did not have dye spread above the lumbocostal ligament. The lateral extent of dye spread was to the posterior axillary line in two cadavers and the midaxillary line in the third. Dorsal rami were stained up to 3–4 levels above the site of injection (L1–L2), while in one cadaver, the dorsal rami were stained 1–2 levels below site of injection. The subcostal nerve was stained in all three cadavers, but lumbar plexus branches and lumbar nerve roots were spared. One cadaver demonstrated spread to the retrolaminar space. The paravertebral space was spared except in one cadaver where it was faintly stained at level T10–12 (figure 5B). There was no staining of the pleural space, intercostal space, intraperitoneal space or the TAP.

(A) Cadaveric specimen following posterolateral quadratus lumborum (QL) block. Dye staining can be seen deep to the erector spinae muscle (ESM) and stained the dorsal rami (DR) up to T9. (B) Cadaveric specimen following posterolateral QL block. Dye staining can be seen deep to the ESM, to the DR and faint staining inside the paravertebral space and intercostal nerves (ICN). (C) Cadaveric specimen following posteromedial QL block. Dye staining can be seen deep to the ESM and stained the dorsal rami up to T6. (D) Cadaveric specimen following posteromedial QL block. Dye staining can be seen deep (anterior) to the transverse process (TP) and affecting the 11th ICN and the subcostal nerve (SCN). LCL, lumbocostal ligament; PP, parietal peritoneum; TP, transverse process.
Posteromedial QL block
Radiologic results
The highest level achieved of dye spread deep to the ES muscle reached by contrast was T7, and the lowest level was L5. Two cadavers demonstrated lateral extension to the transverse process rib articulation, while in one cadaver, contrast extended to the posterior axillary line. Medially, contrast extended deep to the ES muscles to the spinous process with evidence of retrolaminar extension in all three cadavers. There was evidence of T10–T12 paravertebral spread in two cadavers (figure 3B). There was no radiologic evidence of dye spread to the epidural, intercostal, intraperitoneal spaces or the TAP.
Dissection results
Dye spread deep to the ES muscle was seen as high as T7 and as low as L5 (figure 5C,D). All three cadavers had evidence of dye spread cranial to the lumbocostal ligament. Laterally, the dye extended 2–3 cm lateral to the transverse process in two cadavers and to the posterior axillary line in one. The dorsal rami were stained up to 2–3 levels below the site of injection, while 4–6 dorsal rami were stained above the site of injection (figure 5C,D). The subcostal nerve was stained in all specimens, and the retrolaminar space was stained in two of the three cadavers. Faint paravertebral extension and ventral rami staining were evident in two cadavers (Figure 5D, online Supplemental figure 2). No cadavers demonstrated staining of the branches of lumbar plexus, the lumbar nerve, intercostal, the TAP, pleura or peritoneum.
Supplemental material
Discussion
This study provides insight into the underlying mechanistic actions of newer truncal interfascial plane blocks. Both posterior QL and ESP blocks show unreliable spread of injectate to the paravertebral space and ventral rami, but the dorsal rami were frequently covered. The low thoracic ESP demonstrates more cranial spread, but the total extent of injectate distribution was similar to L2 posterior QL blocks when using the posteromedial approach due to continuity of the fascial plane. Based on these findings, we postulate that the L2 posteromedial QL block approach and the lower thoracic ESP block may have clinical utility for upper and lower abdominal surgery analgesia, while applications of the L2 postero-lateral QL block approach may be restricted to lower abdominal surgery.
Injection of dye deep to the ES muscles in cadavers has been shown to penetrate the epidural space, neural foramen and intercostal spaces in one study.7 This is the proposed mechanism by which visceral and somatic sensory block may be achieved with ESP block.12 Other cadaver studies have not shown evidence of direct ventral rami staining or paravertebral spread after injection at T5 vertebral level.4 8 This is further confirmed in this study where only faint dye in the paravertebral space in one cadaver was observed. No previous studies have reported cranial spread after posterior QL block deep to the ES muscle with staining of the dorsal and ventral rami. Possible explanations for this inconsistency between different cadaveric studies include anatomic differences in the lumbar versus thoracic areas, complex anatomy of the fascial layers and different injection points between layers with resulting variation in spread. Further investigation is needed with clinical correlation as local anesthetic spread and effects may differ in live patients and may be influenced by many factors.1 Anatomy of the fascia and surrounding tissues in the context of ultrasound-guided interfascial plane blocks has only been addressed to a very limited degree.1 An understanding of the architecture of the QL muscle, fascial planes and the lumbocostal ligament is important as it directly affects the spread of injectate and may be responsible for the observed differences between the medial and lateral QL approaches.
QL muscle
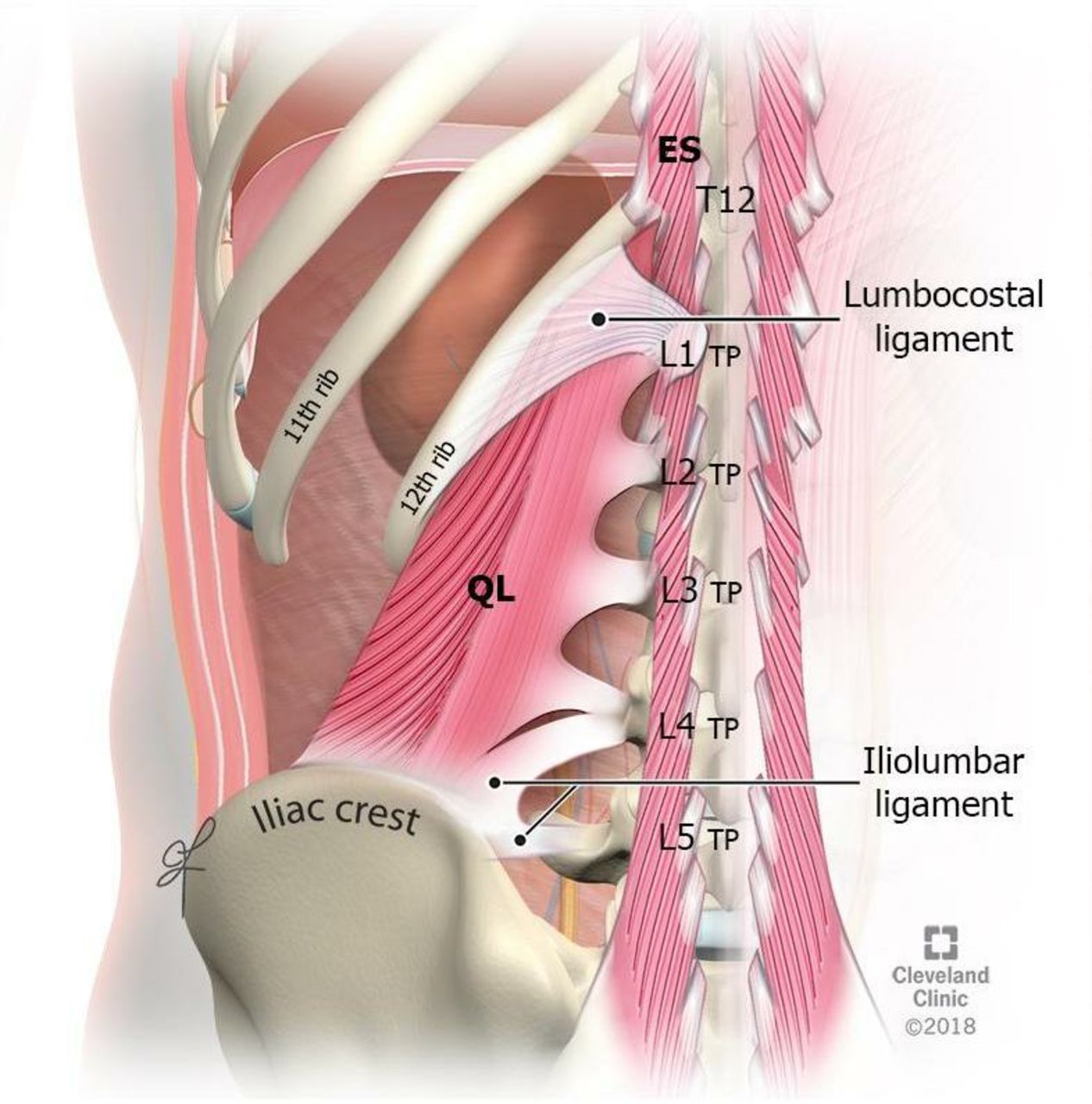
The QL muscle has unisegmental (medial) and multisegmental (lateral) components. The medial unisegmental portion descends vertically from the 12th rib, with tendons attaching to the lumbar transverse processes. The lateral multisegmental component emerges obliquely from the lumbar transverse processes and descends to the iliac crest9 10 (figure 6). These architectural features may affect the spread of dye. After injection posterior to the posterolateral multisegmental component (between the QL and latissimus dorsi), the cranial spread of injectate was limited. However, after injection posterior to the medial unisegmental component (between the QL and ES muscles), dye spreads deep to the ES muscle to a higher thoracic level than a posterolateral injection.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Illustration demonstrating the lumbocostal ligament and iliolumbar ligament locations, as well as the unisegmental (medial) component of the QL muscle and multisegmental (lateral) components of the QL muscle. ES, erector spinae; QL, quadratus lumborum; TP, transverse process.
Thoracolumbar fascia and lumbocostal ligament
The MTLF is situated between the QL and ES muscles and attaches to the tips of the lumbar transverse processes. The MTLF is thin and not continuous between the lumbar transverse processes where the posterior primary ramus exits the paravertebral space.10 13 The lumbocostal ligament is a thickened cranial part of the MTLF.14 15 The lumbocostal ligament is posterior (superficial) to the cranial part of the QL muscle16 17 (figure 6). Cranially in the thoracic area above the last rib, the MTLF becomes thinner and fuses with the fascia on the posterior aspect of the ribs and transverse processes anterior (deep) to ES muscle.18 The lumbocostal ligament, therefore, restricts the cranial spread of the dye deep to the ES muscle when using the posterolateral QL approach in the current study.
ES muscle
The ES muscles lie posterior to the QL muscle and are encircled by the posterior thoracolumbar fascia.14 This fascia is continuous throughout the cervical, thoracic and lumbar spine,18 19 which facilitates injectate spread.6 This study provides evidence that the fascial plane in the thoracic area deep to ES muscles, the target for ESP block, is in continuity caudally with the MTLF in the lumbar region posterior to the QL muscle, medially superficial to the laminae for the retrolaminar block and laterally with the tissue plane deep to the rhomboid and serratus anterior muscles for the rhomboid intercostal and subserratus block.20 With current nomenclature, injection at any of these points along the same tissue plane may be considered different techniques based on needle insertion site despite continuity of planes.
This study has limitations. First, the injection level for the posterior QL approaches (medial and lateral) was at L2, while the ESP was at T10–11. There were 3–4 vertebral levels difference that can lead to a difference in the spread of dye. In addition, the ultrasound transducer orientation and needle trajectory were different. The ESP blocks were performed with a parasagittal ultrasound orientation and craniocaudal needle insertion. The QL approaches were done with transverse orientation from lateral to medial. A further limitation is that there are differences in cadaver tissue compared with live humans as well as a difference in the viscosity of the local anesthetic versus dye injectate. To mitigate this limitation, unembalmed fresh human cadavers at room temperature and 0.5% methylcellulose with India ink as the injectate were used. The 0.5% methylcellulose solution has comparative viscosity to local anesthetics. A further limitation is that we noted small discrepancies between cadaveric and radiologic findings, which can occur in studies such as this. This may be due to variation in timing of dissection and imaging, dye leakage during anatomic dissection and the subjective nature of both methods. One specific drawback of QL blocks, which is not limited to this study only, is that the highest level one can perform them is at L2, in contrast to ESP blocks that can be performed at the levels of interest. Finally, this study is purely anatomic with small numbers of cadavers, and clinical correlation is still needed to confirm that ESP and posterior QL blocks have comparable clinical effects. By injecting closer to the neuraxial midline, and the paravertebral space, there is also an increased likelihood that the local anesthetic will penetrate to the paravertebral space and result in visceral analgesia. Both blocks should be compared with paravertebral block and other interfascial plane block, for example, rhomboid intercostal and serratus plane block.20
In conclusion, posteromedial QL block at L2 level results in cephalocaudal spread of dye comparable with low thoracic ESP block and cranial extension beyond the lumbocostal ligament. Restriction of cephalocaudal injectate spread using the L2 posterolateral QL block approach can be attributed to restriction by the lumbocostal ligament. Both posterior QL and ESP blocks show unreliable spread of injectate to the paravertebral space and ventral rami, but the dorsal rami were frequently covered.
Supplemental material
Supplemental material
Acknowledgments
Rahul Dinkar Renapurkar, MD, Loran Mounir Soliman, MD, and Elion Hijazi (radiology senior technician).
References
Footnotes
Contributors Study design/planning: all authors. Data analysis: all authors. Drafting and writing paper: all authoirs. Revision and approval of the final manuscript: all authors. All authors agree to be accountable for all aspects of the work thereby ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests HE is a consultant for PACIRA (Troy Hills, New Jersey, USA). This company had no input into any aspect of the present project design or manuscript preparation.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note Permission to use included images was obtained from the Cleveland Clinic Department of Art Photography.