Article Text

Abstract
This article in our point-of-care ultrasound (PoCUS) series is dedicated to the role the focused assessment with sonography in trauma (FAST) exam plays for the regional anesthesiologist and pain specialists in the perioperative setting. The FAST exam is a well-established and extensively studied PoCUS exam in both surgical and emergency medicine literature with over 20 years demonstrating its benefit in identifying the presence of free fluid in the abdomen following trauma. However, only recently has the FAST exam been shown to be beneficial to the anesthesiologist in the perioperative setting as a means to identify the extravasation of free fluid into the abdomen from the hip joint following hip arthroscopy. In this article, we will describe how to obtain the basic FAST views (subcostal four-chamber view, perihepatic right upper quadrant view, perisplenic left upper quadrant view, and pelvic view in the longitudinal and short axis) as well as cover the relevant sonoanatomy. We will describe pathological findings seen with the FAST exam, primarily free fluid in the peritoneal space as well as in the pericardial sac. As is the case with any PoCUS skill, the application evolves with understanding and utilization by new clinical specialties. Although this article will provide clinical examples of where the FAST exam is beneficial to the regional anesthesiologist and pain specialist, it also serves as an introduction to this powerful PoCUS skill in order to encourage clinical practitioners to expand the application of the FAST exam within the scope of regional anesthesia and pain management practice.
- point-of-care ultrasound
- FAST exam
- trauma
Statistics from Altmetric.com
Introduction
The focused assessment with sonography in trauma (FAST) exam is an ideal complement to the other point-of-care ultrasound (PoCUS) skills for the regional anesthesiology and pain specialist.1–3 Ultrasound machines have become a mainstay in the practice of regional anesthesiology and the increased presence of portable ultrasound equipment creates an opportunity to acquire skills in PoCUS. While the FAST exam was originally designed to move trauma patients expeditiously to the operating room, its role has expanded to include care of critical patients in the preoperative and postoperative periods. In fact, a positive FAST exam may identify the cause of hemodynamic instability in non-trauma patients in the perioperative period. The regional anesthesiologist is frequently the first perioperative physician to evaluate patients postoperatively, creating an opportunity to rapidly diagnose and treat patients with the aid of ultrasound.
Clinician-performed ultrasound for patients with thoracoabdominal trauma has been used in Europe since the 1980s. However, physicians in America only began using ultrasound for trauma in the 1990s.4–6 Prior to the FAST exam, critically ill trauma patients underwent invasive studies such as the diagnostic peritoneal lavage (DPL) to assist the clinical decision-making in the need for an exploratory laparotomy. The DPL has excellent sensitivity but poor specificity, and is an invasive procedure involving placement of a catheter into the abdomen. The term FAST originated from a number of papers by the trauma surgeon Grace Rozycki who created a protocol of imaging four potential spaces for free fluid in trauma patients: the right upper quadrant (RUQ) hepatorenal space (also known as Morison’s pouch), the left upper quadrant (LUQ) perisplenic space, the pelvis, and the pericardium.5 7–11 The FAST exam had excellent specificity: a positive FAST exam predicted the need for an exploratory laparotomy, but only moderate sensitivity. It is not capable of ruling out free fluid in the abdomen.12 Therefore, the FAST exam became the best initial imaging modality in trauma. Additional patient evaluation, repeat ultrasound, and CT scan are often needed when the FAST exam is negative.
In the past 20 years, the FAST exam has become a standard of care in major trauma centers, an integral component of advanced trauma life support, and the basis of training for many PoCUS curricula.13–15 In contrast, the FAST exam has only recently emerged as a key component of anesthesiology training and practice. It is a skill that is easily learned with a small number of exams.16 17 The FAST exam serves as the core building block for ultrasound curricula in emergency medicine, and it can serve a similar purpose in anesthesiology.18
In anesthesiology, the FAST exam has the greatest utility in urgent and emergent cases where patients are critically ill (box 1). A source of hypotension may be readily localized, and the decision to return to the operating room may become clear. For example, the FAST exam can uncover persistent bleeding following abdominal surgery, expediting the patient’s return to the operating room. It can also help identify undiagnosed pericardial effusions contributing to perioperative tamponade physiology or intra-abdominal fluid extravasation (IAFE) causing pain following hip arthroscopy.19 As with most PoCUS applications, it is helpful to use the indication, acquisition, interpretation, and management (I-AIM) method to integrate the FAST exam into clinical practice (table 1). This method directs the learner to the I-AIM of findings on the FAST exam.
Clinical indications for the focused assessment with sonography in trauma (FAST) exam
Hypotension in the postanesthesia care unit (PACU).
Narrowing the differential diagnosis in patients who are critically ill.
Nausea and/or abdominal pain following hip arthroscopy.
Identify a pericardial effusion causing tamponade physiology.
Persistent hypotension in the intensive care unit (ICU).
Initial evaluation of hypotensive trauma patients.
Re-evaluation of trauma patients.
Indication, acquisition, interpretation, and management (I-AIM)
It is imperative that clinicians learning the FAST exam understand the strengths and limitations. The FAST exam is not intended to be a definitive imaging modality. Its main purpose has been to identify adult trauma patients who need an emergent laparotomy. Its purpose is NOT to rule out free fluid in the abdomen. Multiple studies have demonstrated that additional workup is essential for hemodynamically stable patients with a negative FAST exam given the low sensitivity.12 20 21 A well-designed study by Branney et al demonstrated this effect in an elegant manner by examining the hepatorenal recess with ultrasound while DPL was being performed. They noted that minimum volumes of 300–1000 mL of fluid were identifiable by FAST exam and that high sensitivity was only achieved at the high end of this range.22 Like most ultrasound studies, clinicians with more ultrasound experience were able to identify smaller volumes than less experienced clinicians.
This article in our series on PoCUS for the regional anesthesiologist and pain management specialist1–3 describes the emerging role of the FAST exam in perioperative medicine: clinical indications and scanning technique for the FAST exam as well as pathologic findings, artifacts, incidental findings, and potential pitfalls. This article will also cover medical decision-making, the Extended FAST (E-FAST), and a comparison with other imaging modalities.
FAST exam fundamentals
Probe selection
Probe selection is important for performing the FAST exam. Classically, a curvilinear low-frequency transducer (2–5 MHz) has been used as it allows for a wide field of view and sufficient depth of penetration for optimal intra-abdominal views. A viable alternative is a phased array probe. It combines the advantage of a small footprint with the ability to obtain intra-abdominal, cardiac and thoracic/pleural view without having to switch probes and reoptimizing settings. However, for non-cardiac imaging, the phased array transducer provides lower resolution images compared with the curvilinear probe (figure 1).

Curvilinear and phased array ultrasound transducers.
Orientation marker and indicator
Multiple terms may be used for the marker on the probe and the indicator on the screen. In PoCUS, the term ultrasound probe indicator refers to the notch on the probe that is used to direct the probe while scanning.23 However, the terms ultrasound probe orientation marker and notch are frequently used in clinical practice. The on-screen indicator refers to the marker on the ultrasound screen that corresponds with the probe marker. The term leading edge may be used for the side of the ultrasound screen near the on-screen indicator; receding edge may be used for the opposite side. For abdominal scanning, the on-screen orientation indicator appears on the left side of the screen as opposed to cardiac scanning, where it is located on the right side. Keep this in mind when performing any cardiac scanning in the abdominal orientation. Images on the screen may be a mirror image when flipping between abdominal orientation and cardiac orientation.
Patient positioning
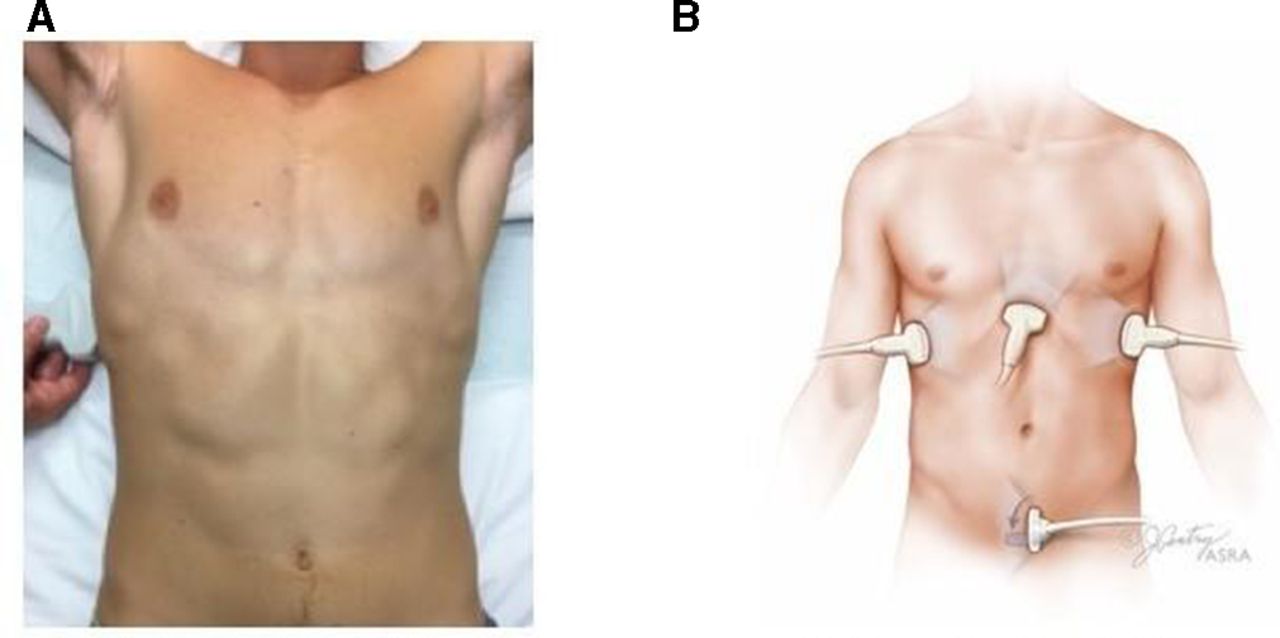
The FAST exam involves imaging multiple potential spaces via four views: subcostal four-chamber view, perihepatic RUQ view, perisplenic LUQ view, and pelvic view in the longitudinal and transverse planes. The patient is positioned supine with arms abducted or raised over their head, if possible (figure 2). Although not always possible, positioning in the Trendelenburg or revere Trendelenburg position will make the exam more sensitive in the RUQ and pelvic views, respectively. The clinician may start the exam at any location, but the RUQ (Morison’s pouch) view is the traditional starting location in blunt trauma as it is the most sensitive location for free fluid.24 Generous fanning of the ultrasound probe is of utmost importance for acquisition of the abdominal views. The E-FAST exam, which will be discussed later, adds imaging of the pleura to evaluate for pneumothorax.
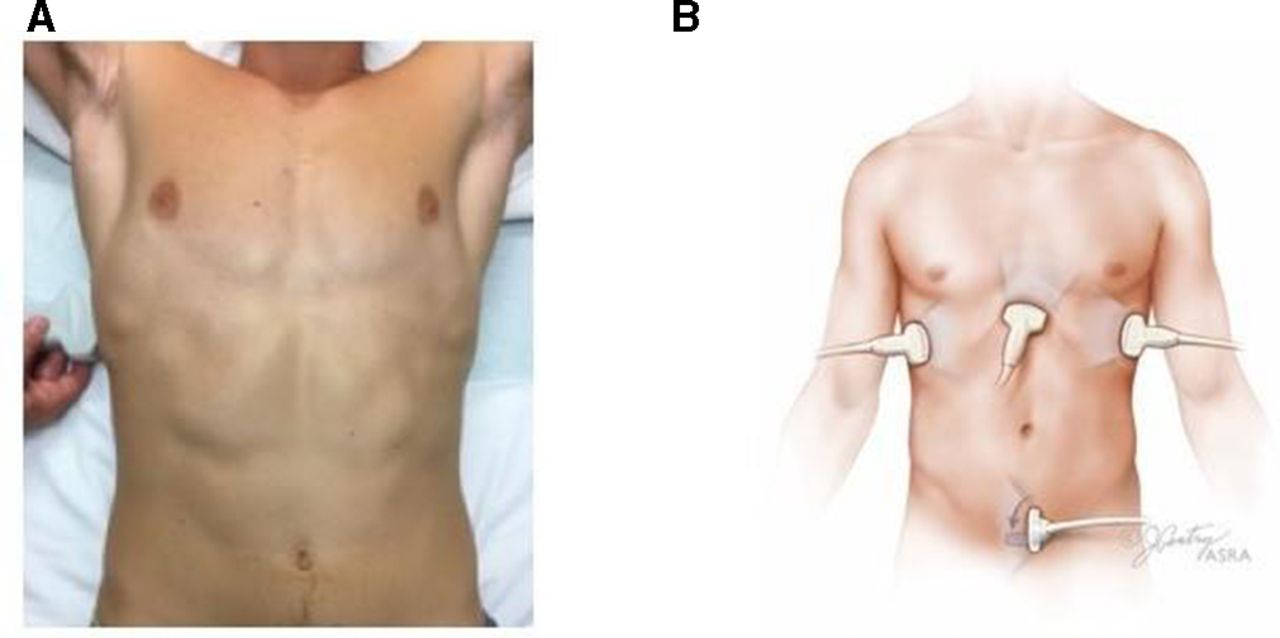
(A) Patient position for the FAST exam. (B) Probe positions for the FAST exam. FAST, focused assessment with sonography in trauma.
Sonoanatomy and scanning technique
Cardiac views
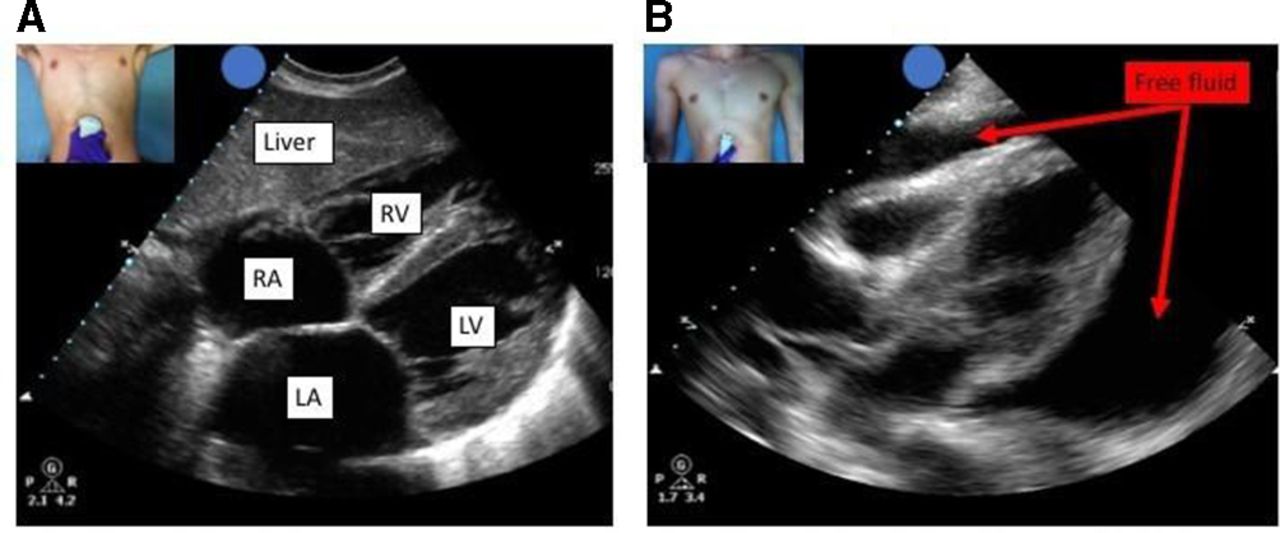
Pericardial effusions are most often imaged with the subxiphoid cardiac view, however when this view cannot be obtained, the parasternal long and short axis views may be useful alternatives. To acquire the subxiphoid view, the probe is held like a screwdriver immediately caudad to the sternum. The orientation marker is aimed to the patient’s right, and the probe is rotated 10°–15° counterclockwise (figure 3A). This view allows simultaneous visualization of pericardium and all chambers of the heart. Deep inspiration improves imaging by increasing venous return and movement of the heart toward the ultrasound probe. Depending on the patient’s body habitus, this image can require a depth of 20–25 cm to image the entire heart.

(A) Subcostal view of the heart. (B) Subcostal view with pericardial effusion. Free fluid can be seen surrounding the heart. LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.
The parasternal long-axis view is also sensitive for pericardial effusions and does not require patient cooperation. To acquire this view while scanning in abdominal mode (ie, the on-screen orientation indicator is on the left side), the probe is placed just left of the sternum in either the third or fourth intercostal space with the orientation marker aimed toward the left shoulder of the patient. For more details on the parasternal long-axis view, please refer to the RAPM article on Focused Cardiac Ultrasound.2
Right upper quadrant
The RUQ view is the ‘high-yield’ view of the abdomen because the hepatorenal recess (also known as Morrison’s pouch) is the most dependent point of the upper peritoneum in the supine patient. To obtain this view, place the ultrasound probe in the coronal plane in the 8th–11th intercostal spaces in the midaxillary to posterior-axillary line with the orientation marker directed cephalad (figure 4A). It is imperative to visualize the lower liver tip (right paracolic gutter) as fluid accumulates in this location first. Slight counterclockwise rotation can be helpful if rib shadows obstruct the view. The diaphragm and lower right thorax can be imaged by directing the probe cephalad. Pleural fluid will appear as an anechoic area just superior to the diaphragm, while intraperitoneal fluid superior to the liver may be revealed between liver and the diaphragm.

(A) Right upper quadrant view, demonstrating liver, kidney, Morison’s pouch, and the diaphragm. (B) Right upper quadrant view with free fluid around the inferior tip of the liver.
Left upper quadrant
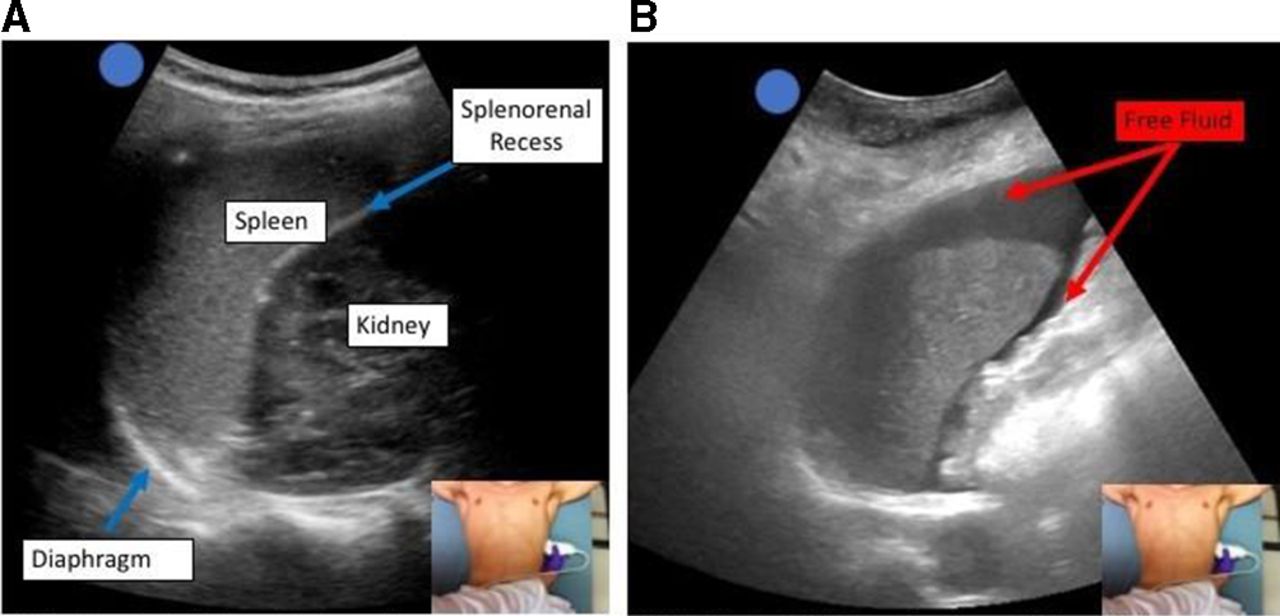
This view is typically the most challenging to obtain. To obtain this view, image in the coronal plane with the indicator directed cephalad. Compared with the RUQ, the LUQ view requires a slightly more cephalad position of the ultrasound probe in the sixth to ninth intercostal spaces and a more posterior probe location in the posterior axillary line (figure 5A). This location is necessary due to multiple factors: the smaller size of the spleen (compared with the liver), the spleen’s posterior location, and the presence of the stomach. To optimize the image, fan the probe posteriorly away from the anterior stomach. Slight clockwise rotation can be helpful if rib shadows obstruct the view. This view images the superior surface and lower tip of the spleen as well as the subphrenic space and splenorenal recess. For thorough examination of the LUQ it is imperative to visualize the entire superior pole of kidney. To achieve this, slowly fan anterior to posterior and back until the kidney goes completely out of view, comes back into view, and repeat this for the anterior portion. The left pericolic gutter is the most frequently missed area of the LUQ and is the most likely to accumulate isolated fluid.25 This area can be evaluated by moving down one rib space and scanning between the left edge of the spleen and the entire inferior pole of the kidney.
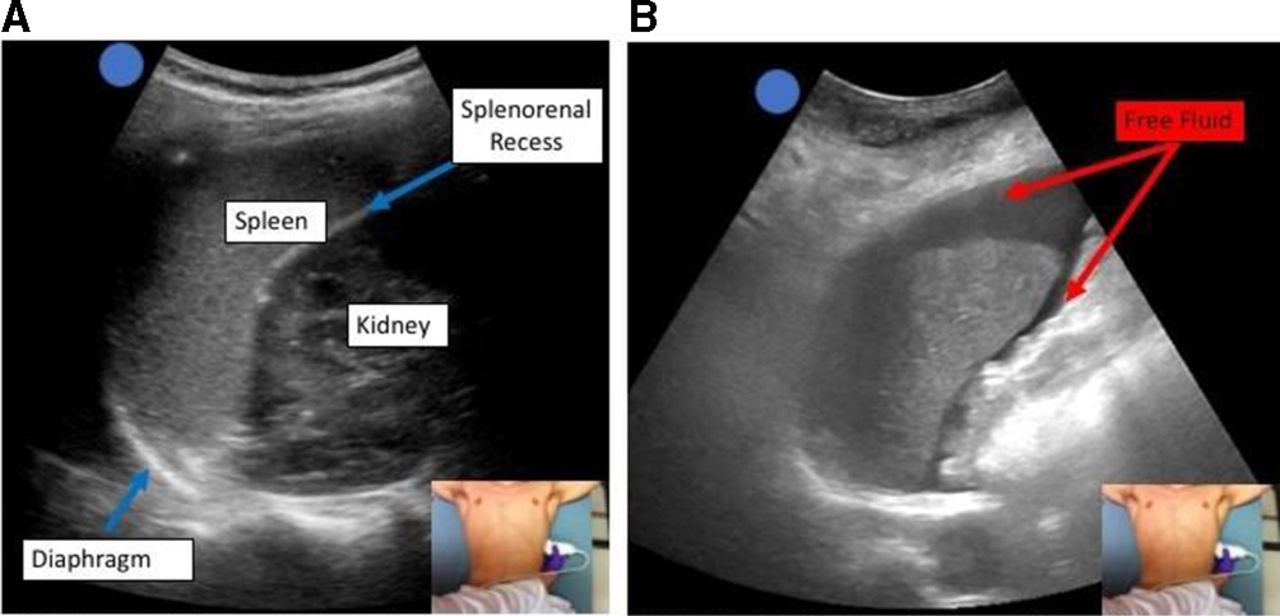
(A) Left upper quadrant view, demonstrating the splenorenal recess, spleen, kidney, and diaphragm. (B) Left upper quadrant view demonstrating free fluid surrounding the spleen.
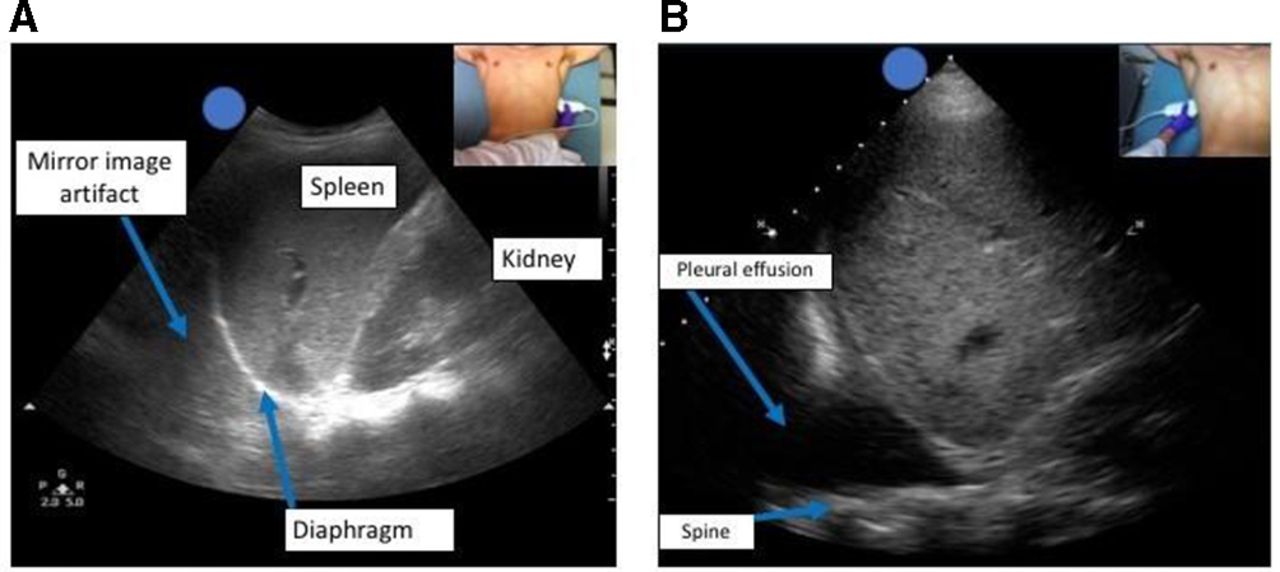
The diaphragm can be seen as a curved, hyperechoic line immediately superior to the spleen. Pleural fluid will appear as a hypoechoic or anechoic area superior to the diaphragm. To optimize the image, inspiration with breath holding, a slight increase in depth and gentle anterior fanning may be necessary. In the absence of pleural fluid, a mirror image of the spleen may be seen above the diaphragm, a normal artifact that occurs due to strong specular reflectors like the diaphragm (figure 6A: mirror image artifact).

(A) Mirror image artifact: the diaphragm acts as a specular reflector, and spleen tissue is seen cephalad to the diaphragm. This artifact only occurs in the absence of pleural effusions or hemothorax. (B) Spine sign: the spine is visible cephalad to the diaphragm due to presence of fluid in the thoracic cavity.
Another marker of intrathoracic free fluid is the spine sign. Normally, the spine and its shadowing do not extend cephalad beyond the diaphragm. However, if there is fluid in the thoracic cavity, the spine may be visualized past the diaphragm up into the thoracic area (figure 6B: spine sign).
Pelvic views
The suprapubic view on the FAST exam is generally the last of the four views performed. Although not as easily obtained as the RUQ view, the pelvic views are of great importance since the pelvis is the most dependent part of the peritoneum. The pelvic view can be the best view to identify free fluid following procedures in the pelvis. In females, the most dependent location is the rectouterine pouch or pouch of Douglas. In males, its counterpart is the rectovesical pouch posterior to the bladder wall. Theoretically, the pelvic view should be the most sensitive view to visualize free fluid; however, this does not seem to be the case. In fact, in the setting of ectopic pregnancy, a positive RUQ (Morison’s pouch) view best predicts the need for operative intervention.26 27 It should be noted that the FAST exam is frequently negative in pelvic fractures; however, recent literature indicates that it can still be useful in guiding therapeutic decision-making.24 28
When scanning the suprapubic area in both transverse and longitudinal planes, many anatomic structures are encountered including the bladder, bowel, pelvic bones, pelvic organs and rectum. While this might make it harder to distinguish free fluid from other structures, a structured exam can overcome these challenges.
Locating the bladder: Place the ultrasound probe directly superior to the pubic symphysis with the orientation marker directed cephalad. With this longitudinal view, direct the ultrasound beam slightly caudad into the pelvis by rocking the probe (figure 7). The bladder is just cephalad to the pubic bone. To obtain the transverse view, simply rotate the probe by 90° counterclockwise with the orientation marker pointing to the right (figure 8). While a nearly empty bladder can still be visualized, a full bladder enhances the ability to identify free fluid. A full bladder creates an improved acoustic window and minimizes gas scatter from bowel. If the patient has an empty bladder, it is advisable to give fluids, and repeat the scan when the bladder is more distended.29
Image optimization: Depth and gain adjustment are paramount to acquiring a good image, optimizing interpretation, and locating free fluid. More often than not, when transitioning to the suprapubic area, there is excess depth from scanning the upper quadrants and cardiac views. Decreasing the depth to about 13–16 cm optimizes the view. The goal is to have the bladder centered on the screen, to easily visualize the areas surrounding the bladder. The bladder is a fluid-filled structure, acting as an excellent acoustic window to deeper structures. An artifact called ‘posterior acoustic enhancement’ produces a hyperechoic and bright area deep to the bladder, making it challenging to visualize anechoic or black free fluid. Decreasing far-field gain will increase the ability to identify anechoic free fluid. An appropriate gain setting will allow for easy identification of pelvic organs.
Thorough examination: Free fluid in the pelvic cavity may collect anywhere—anterior, lateral, and posterior to the bladder as well as anterior, lateral, and posterior to the uterus in female patients. Factors dictating the location include patient’s positioning, filling state of the bladder, flexion of the uterus, and the size of the prostate, to name a few. The following four areas require close examination:
Anterior and cephalad to the bladder, especially if the bladder is empty. Free fluid can easily be mistaken for the bladder and thought to be a septated bladder.
Adjacent/lateral to the bladder. Free fluid will collect into a ‘wedge’ shape or triangular shape in between bowel folds. Fanning the probe will help identify free fluid.
Deep/posterior to the bladder and pelvic organs, especially in females. This area is often the location of free fluid between the bladder and the uterus.
Posterior to pelvic organs. Free fluid can collect deep to the uterus or prostate.
Fanning: Fanning is important in evaluating any region by ultrasound and is essential when evaluating the suprapubic area. Free fluid can ‘hide’ around the many structures present in this region. The authors strongly encourage fanning through the suprapubic area in two planes—horizontally and longitudinally.
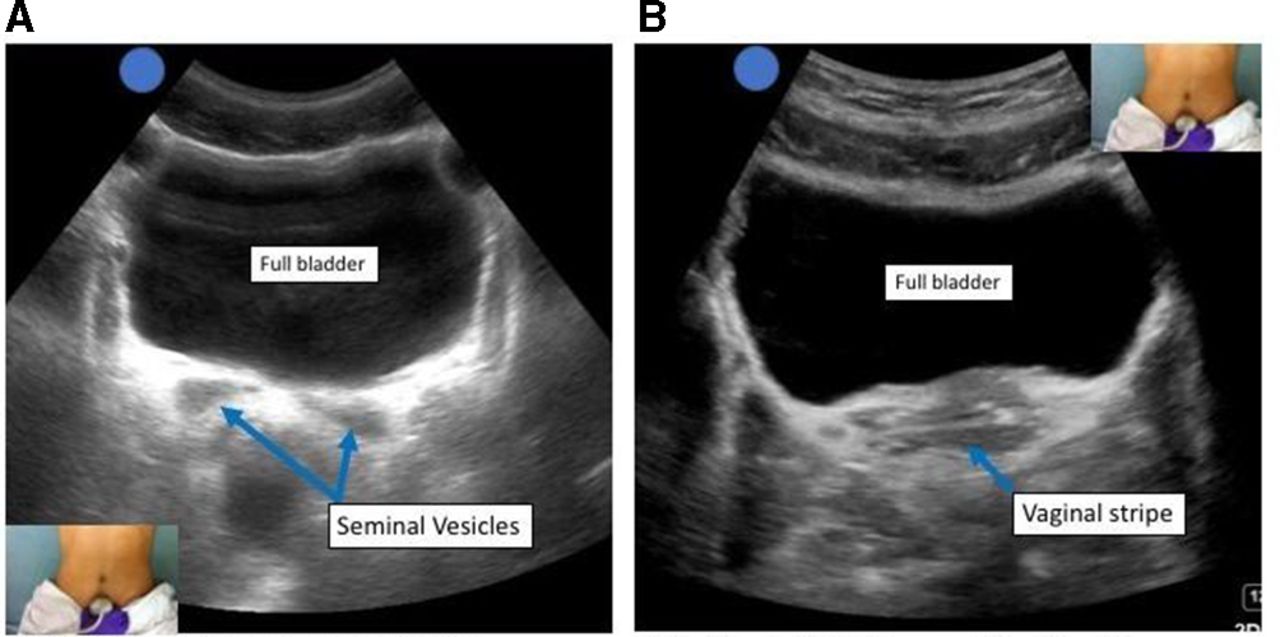
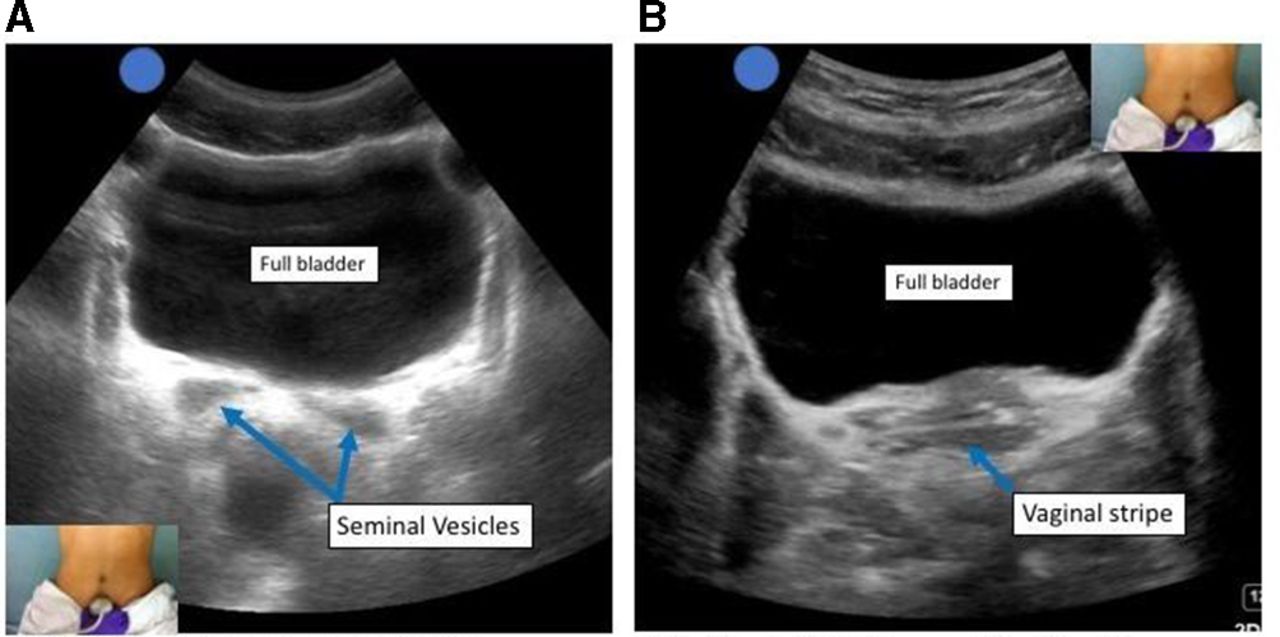
Physiologic findings: Seminal vesicles (figure 8) often appear as an anechoic ‘bow-tie’ shape immediately posterior to the bladder, with contained fluid and equal on each side. They will always appear in the same location, and you should fan slowly and carefully through the region to ensure that this is a contained structure not to be mistaken for free fluid. In menstruating females, physiological free fluid (figure 7) may be present in the pouch of Douglas. This physiological free fluid may be difficult to differentiate from traumatic free fluid. The amount and location can help differentiate physiological free fluid from pathologic fluid: fluid in the pouch of Douglas is normally not greater than one-third the length of the border of the uterus.

(A) Sagittal view of the male pelvis demonstrating a full bladder and the prostate. (B) Sagittal view of the female pelvis demonstrating the bladder, uterus, and vaginal stripe.
(A) Transverse view of the male pelvis demonstrating the bladder and prostate. (B) Transverse view of the female pelvis demonstrating the bladder and vaginal stripe.
Pathological findings on FAST exam
Free fluid in the peritoneal space or pericardial sac
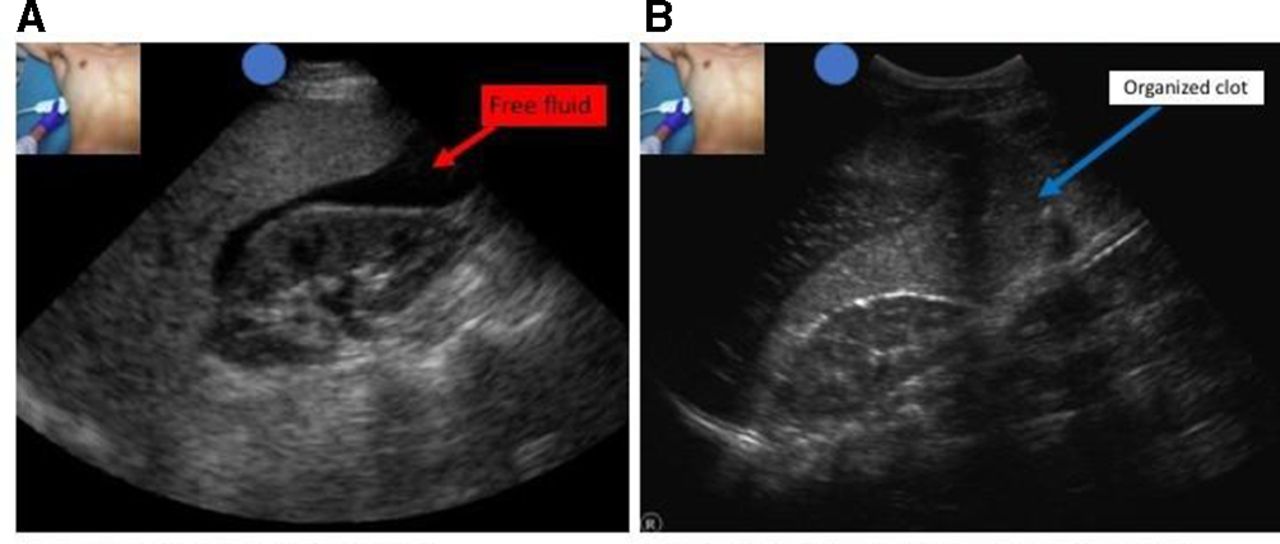
Simple free fluid such as fresh blood or ascites will appear as anechoic or hypoechoic areas filling in the potential spaces examined on the FAST exam (figure 9A). Dense or organized fluid such as clots or loculated collections may demonstrate echogenicity more similar to solid organ parenchyma (figure 9B). The RUQ, LUQ and pelvic views can reveal pooling of intraperitoneal fluid in the abdomen and pelvis (figures 4B, 5B, 10 and 11). The pericardial view of the FAST exam may reveal pericardial effusions or hemopericardium (figure 3B).

(A) Right upper quadrant view demonstrating free fluid in Morison’s pouch. (B) Right upper quadrant view demonstrating organized clot in Morison’s pouch. The echogenicity of the clot is more isoechoic with the liver parenchyma.

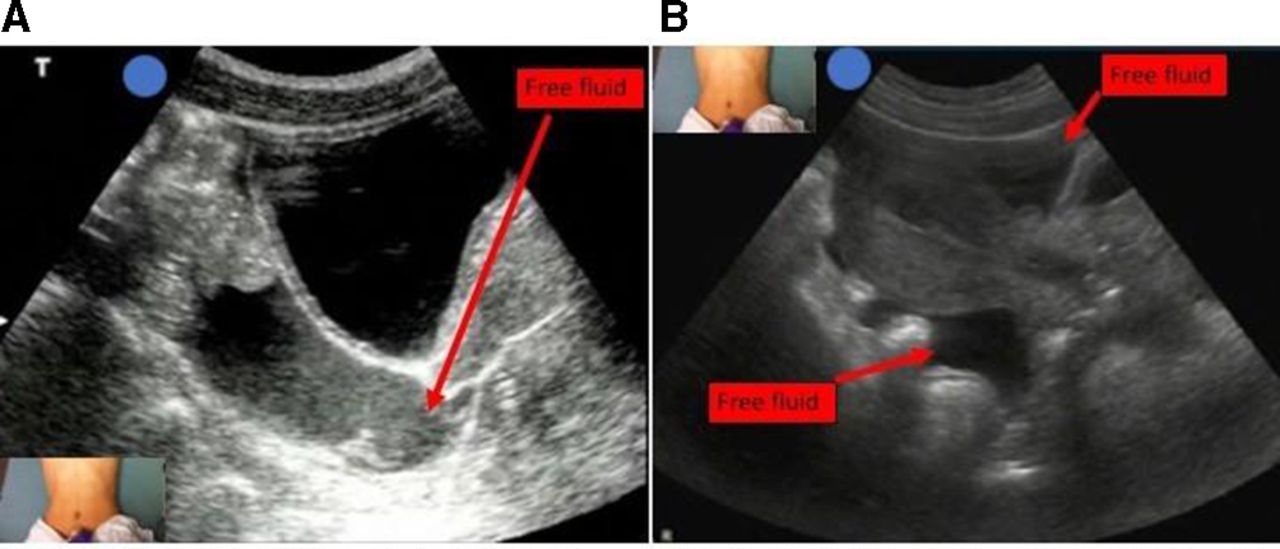
(A) Sagittal view of the male pelvis demonstrating free fluid in the rectovesical pouch. (B) Sagittal view of the female pelvis demonstrating fluid surrounding the uterus.

(A) Transverse view of the male pelvis demonstrating free fluid deep to the bladder. (B) Transverse view of the female pelvis demonstrating free fluid deep to the bladder.
Pitfalls and limitations
Sensitivity and specificity
Despite being a simple, reliable and well-studied PoCUS exam, some pitfalls and limitations can result in inaccurate diagnoses and interpretation of findings. Of most importance is that the FAST exam is a highly specific exam (as high as 99%)30 31 for diagnosing free fluid; however, it has poor sensitivity (60%–80%) and cannot be used to rule out free fluid.32 33 Branney et al found that the mean detectable fluid volume needed for visualization in the RUQ via assessment of Morison’s pouch was 619 mL while Von Kuenssberg and Wagner found that between 129 and 157 mL could be detected in the pelvis.22 34 While assessing for free fluid in the pelvis is more sensitive, a full bladder is required for an adequate acoustic window into the pelvis. If the bladder is empty, then the sensitivity and specificity of the pelvic views decrease significantly. Additionally, the FAST exam has an even more limited role in diagnosing solid organ injury (sensitivity of 41%–44%)35 36 because freshly coagulated blood in the injured solid organ has a similar echogenicity to the parenchyma.37
Several steps can be taken to improve the sensitivity of the FAST exam. Position can increase the sensitivity; for example, 5° of Trendelenburg can aid in visualization in hepatorenal (RUQ) and splenorenal (LUQ) space requiring only 400 mL of volume for visualization versus 700 mL.38 Reverse Trendelenburg can also help improve visualization in the pelvis. When clinically appropriate, avoid bladder catheterization before assessing the pelvis. Additionally, serial FAST examinations can decrease the false negative rate by up to 50% and increase sensitivity for the detection of free fluid from 69% to 85% with a negative predictive value (NPV) of 97%.39 As is the case with any procedural diagnostic test, there is a learning curve. One study suggested that 30 FAST exams performed with direct supervision doubled the likelihood of accurately performing the exam.40
False positives
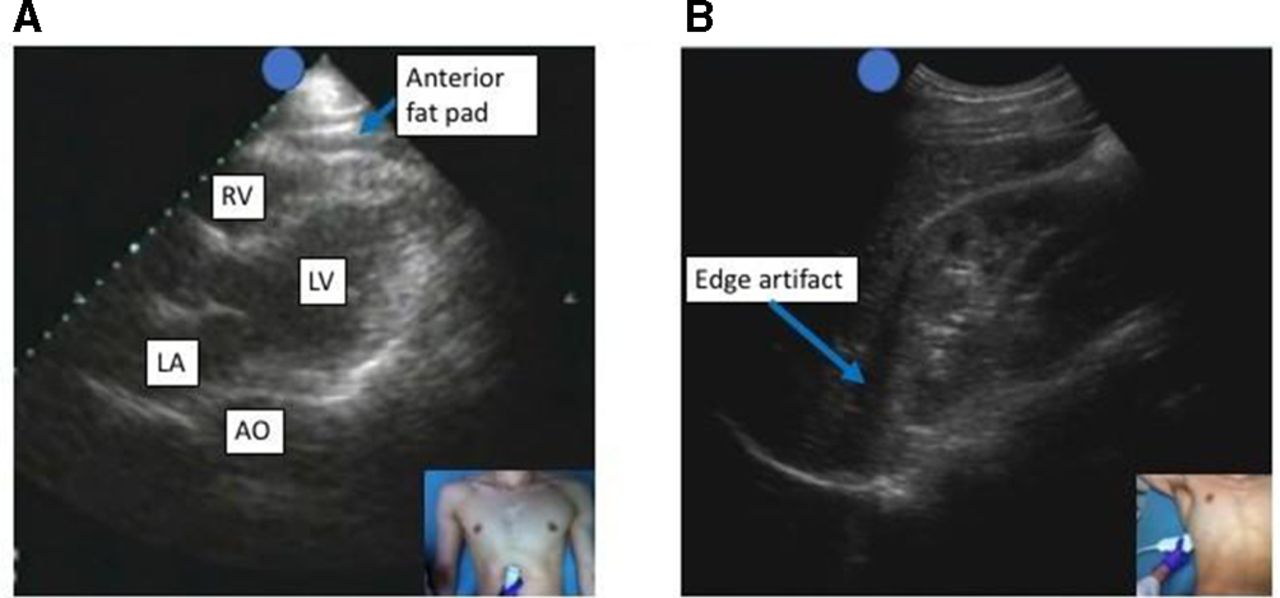
Several well-known normal findings can be mistaken for free fluid to the untrained eye. For example, fat, which is hypoechoic or anechoic-like fluid, can be misinterpreted in certain critical locations. Perinephric fat can increase the size of the hepatorenal and splenorenal interface, thereby looking like free fluid or a subcapsular hematoma—an appearance known as the ‘double-line’ sign.41 Pericardial fat can also mimic a pericardial effusion (figure 12A).

(A) Subcostal four-chamber view of the heart demonstrating an anterior fat pad. This fat pad can be a potential pitfall, as the novice may be tempted to incorrectly diagnose a pericardial effusion. (B) Edge artifact seen at the interface of the liver and kidney. Edge artifact is a potential pitfall that can masquerade as free fluid. Interrogation of Morison’s pouch with fanning the ultrasound probe will demonstrate that the anechoic area is an artifact rather than free fluid. AO, descending aorta; LA, left atrium; LV, left ventricle; RV, right ventricle.
Each FAST view has the potential for error. In the pericardial space, pleural effusions can be confused for pericardial effusions. In the RUQ, the gall bladder, hepatic veins or biliary ducts can be confused for free fluid. Edge artifact can also be mistaken for a false positive in the Morison’s pouch view (figure 12B). In the pelvis, ovarian cysts, seminal vesicles or atypical vasculature can result in a false positive exam. Finally, pre-existing peritoneal fluid as seen in patients with ascites or who have undergone peritoneal dialysis can be mistaken for new hemorrhage. It is essential to scan thoroughly in all four positions to minimize the potential for false positives. The anesthesiologist should consider utilization of other diagnostic modalities such as CT scan and DPL to differentiate between the sources of free fluid.
False negatives
False negative exams can be either patient or examiner dependent. A common source of error is suboptimal imaging due to obesity, which decreases image quality with increased depth requirements. Errors caused by the examiner include use of excess gain, which can mask small fluid collections, incomplete imaging of all spaces, or misinterpreting a full stomach for peritoneal fluid. Examples of incomplete imaging include viewing the splenorenal interface instead of the subdiaphragmatic area and inferior pole of spleen (figure 13) or failing to view the pelvis in both sagittal and transverse planes. An early examination may miss small fluid collections, especially in hollow viscus injury (bowel, gall bladder, bladder) or diaphragm injury as there is minimal fluid extravasation following injury.42 A delayed exam may only reveal clotted blood in the peritoneum, which can be difficult to distinguish from normal parenchyma by an untrained eye. The FAST exam is also not as useful in diagnosing solid organ injury. Although serial FAST exams can decrease the rate of false negatives, when a clinical question is left unanswered by the FAST exam, a CT scan is the gold standard for diagnosing the presence of free fluid and the source.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Left upper quadrant view demonstrating free fluid in the subdiaphragmatic area and inferior tip of the spleen. There is no free fluid at the splenorenal interface. This is a potential pitfall, as a novice may only image the splenorenal interface and miss the free fluid.
FAST exam in clinical decision-making
When incorporating the FAST exam into clinical decision-making, it is helpful to use the I-AIM model as a framework to guide clinical management. This model guides the clinician as a mnemonic and checklist when performing PoCUS. The I-AIM model can be used for various clinical scenarios: trauma patients, patients who are critically ill in the PACU, as well as hip arthroscopy patients (table 1).
The FAST exam has a long-standing history as a valuable tool in the management of trauma patients both in the emergency and operating rooms. As an example, Christian et al reviewed their pelvic fracture database, finding 81 patients with refractory shock who underwent abdominal packing.28 A negative FAST correlated with conservative treatment in 98% of patients (52/53), while a positive FAST exam was confirmed by CT or laparotomy in 98% (52/53) of patients. The sensitivity and specificity for FAST in this population were 96% and 96%; while positive predictive value was 93% and NPV was 98%, respectively. The false negative and positive rates for FAST were 2% and 7%.
About a third of stable trauma patients initially present with a negative FAST exam. Blackbourne et al demonstrated the utility of serial exams by performing a secondary ultrasound survey (SUS) in a prospective, observational study of 547 trauma patients.29 They observed an increase in sensitivity from 31.1% on the initial ultrasound to 72.1% on SUS (p<0.001) for intra-abdominal injury or intra-abdominal fluid, while specificity remained unchanged at 99.8%. The NPV was 92.0% for the initial ultrasound and increased to 96.6% for SUS (p=0.002). The accuracy of the initial ultrasound was 92.1% and increased to 96.7% on the SUS (p<0.002). No patient with a negative SUS after 4 hours developed clinically significant hemoperitoneum.
Another valuable use of the FAST exam is providing prognostic information with minimal expense during the early stages of resuscitation in hemodynamically stable patients presenting with blunt abdominal trauma (BAT). In one retrospective study of 421 patients, the FAST exam was evaluated as a potential risk stratification instrument in hemodynamically stable patients presenting after BAT.43 The investigators examined the association between FAST findings and laparoscopy/laparotomy, angiographic embolization and death. Four hundred and seven of 421 (96.7%) patients had a negative FAST exam, six of whom (1.4% of all patients) had free intraperitoneal fluid. A positive FAST exam was more strongly associated with an adverse outcome than Injury Severity Score or any other individual clinical or biochemical variable measured at presentation in the emergency department (positive likelihood ratio 34.3 [15.1–78.5]).
Various sources of hemodynamic instability such as the cardiovascular and pulmonary systems and other exams such as the E-FAST, rapid ultrasound for shock and hypotension (RUSH), focused echocardiography in emergency life support (FEEL), or focus assessed transthoracic echocardiography (FATE) must be considered in unstable patients.44–47 These exams have varying degrees of crossover (E-FAST-peritoneum plus lung, FEEL-cardiovascular exam during cardiopulmonary resuscitation, FATE-cardiac and pleura, RUSH-cardiac, lung, peritoneum) and different exams could each provide the ‘missing link’ or source of hypotension that one might miss by solely focusing on one organ system.
The FAST exam has recently shown utility in a subset of patients with postoperative pain. Haskins et al evaluated the utility of the FAST exam in patients after hip arthroscopy where intra-abdominal fluid extravasation is a potential contributory factor for nausea and pain by causing peritoneal irritation.19 They found an incidence of IAFE of about 16% that correlated with a larger increase in pain score from baseline (adjusted difference in means [99% CI]: 2.1 points [0.4–3.9]; p=0.002), and a trend toward increase in opioid use (adjusted difference in means [99% CI]: 7.8 mg oral morphine equivalents [−2.8 to 18.3]; p=0.053). The FAST exam can and should be considered for other perioperative applications relevant to the regional anesthesiologist as part of the PoCUS toolset.
The E-FAST exam
The E-FAST exam allows for the additional evaluation of a pneumothorax. This extension of the FAST exam is particularly helpful in the trauma bay, as portable chest X-ray has poor sensitivity and specificity to identify a small to moderate pneumothorax. This is especially true for trauma patients lying supine on a rigid backboard. In 2004, Kirkpatrick and colleagues described the E-FAST, adding two additional views to the FAST exam: bilateral views of the pleura using the high-frequency linear probe.44 This study of 225 patients demonstrated that the E-FAST performed with an overall greater accuracy than chest X-ray as exemplified by the detection of an occult pneumothorax missed on chest X-ray. While this mid-sized study did not eliminate the chest X-ray from early trauma management, it further emphasized the importance and utility that ultrasound brings to patients who are critically ill.
The identification of pneumothorax has already been covered in this series, and will not be covered further here. For more information on the identification of pneumothorax with ultrasound, see Lung Ultrasound for the Regional Anesthesiology and Pain Management Specialist in RAPM.3
The FAST exam for special populations
Pregnancy
The FAST exam has been used to detect pregnancy in unstable female trauma patients of reproductive age pending definitive laboratory testing. Moreover, FAST and its obstetric corollary focused assessment with sonography for obstetrics have been used to detect causes of instability in pregnant patients, such as uterine rupture causing free fluid in the peritoneum.48 While there is insufficient evidence to support the routine use of FAST by anesthesiologists in unstable pregnant patients, it may be considered as an adjuvant diagnostic tool in emergency situations. Of note, the practitioner must be aware of normal abdominal ultrasound findings in pregnant patients in order to avoid false negative or false positive assessments. It is best to defer abdominal ultrasound of the pregnant patient to an obstetrician when available.
Pediatrics
While its utility has been well established in adult trauma patients, the role of FAST in pediatrics is controversial. Only 1% of pediatric hospitals use the FAST exam and this is likely due in part to the high false negative rate associated with low intra-abdominal fluid levels with trauma in stable pediatric patients. FAST may, however, be a useful modality for detecting intraperitoneal fluid in pediatric patients who have undergone hip arthroscopy as has been shown in adults or in children who are at risk for significant postoperative intra-abdominal bleeding.
Comparison with other diagnostic modalities
The FAST exam has been demonstrated to be a highly specific exam; however, due to low sensitivity, there are circumstances where free fluid or organ injury may be missed with ultrasound evaluation. For these clinical scenarios, an alternative diagnostic modality is appropriate. See table 2 for a comparison of these imaging modalities.
Comparison of DPL, FAST exam, and CT scan
CT scan
CT scan of the abdomen and pelvis is considered the gold standard for evaluating for free fluid and can provide insight into the source of injury and bleeding. Specifically, CT scan is superior at diagnosing solid organ injury from hollow viscus injury (bowel, bladder, gall bladder), evaluating for retroperitoneal bleeding as well as identifying potential bony injuries like fractures to the spine and pelvis.35 37 However, CT scans are time-consuming and expensive diagnostic modalities in comparison to bedside ultrasound, and patients must be hemodynamically stable to undergo a CT scan. Therefore, the indications for a CT scan are (1) the presence of a negative (or inconclusive) FAST exam with ongoing suspicion of injury, or (2) evaluation for organ or bony injury in the setting of a positive FAST exam.
Diagnostic peritoneal lavage
DPL is a highly sensitive invasive bedside procedure that involves placing a catheter into the peritoneal space and aspirating for signs of blood or fluid followed by cavity lavage if needed. Once considered the gold standard in assessing for hemorrhage following abdominal trauma, DPL has been largely replaced by CT scan and the FAST exam. The decline in the use of DPL is due to the many disadvantages such as its invasive nature, the potential for organ injury during placement of the catheter and the inability to determine the source or degree of injury, among others. However, there are still certain clinical indications for DPL. DPL can differentiate between new hemorrhage and ascites or residual fluid from peritoneal dialysis. Additionally, DPL has been shown to be more sensitive than CT scan for evaluation of injury to hollow viscous organs.49 50
Incidental findings
Performing PoCUS carries significant responsibility. Incidental findings are frequently found on PoCUS exams. The incidence of incidental findings ranges from 8% to 26%.51–53 Incidental findings during the FAST exam findings are especially significant: abdominal organs frequently contain masses, cysts, and other abnormalities. Since PoCUS is performed by clinicians with specialties other than radiology, the clinician is not expected to match the diagnostic ultrasound skill of a radiologist. Nevertheless, the anesthesiologist performing PoCUS has the same responsibility to manage an abnormality as he or she would manage an abnormal finding on physical exam. The anesthesiologist must refer patients with incidental findings for appropriate follow-up. But appropriate follow-up may be different for one incidental finding than another. For instance, multiple hyperechoic lesions identified in the liver may be managed very differently than a small pericardial effusion seen in a patient with lupus.
The sonographic appearance of incidental findings will help classify the abnormality. Cysts are typically thin-walled structures with anechoic centers. Simple renal cysts are common abnormalities, but cysts may also be present in the liver, spleen, or ovaries. The presence of hypervascularity, abnormal borders, solid structures, and septations are more concerning findings. Various masses may present as atypical echogenic structures. All cysts, masses, and abnormal organ sizes should have follow-up arranged.54
Conclusion
The FAST exam can be an invaluable tool for the regional anesthesiologist and pain specialist. However, it is important to understand the strengths and limitations of the exam including its excellent specificity but poor sensitivity. The anesthesiologist should consider this exam when re-evaluating trauma patients, when examining critical patients in the recovery area, and evaluating patients following procedures at risk for IAFE. The regional anesthesiologist and pain specialist must schedule follow-up for any abnormal findings discovered during the FAST exam.
Acknowledgments
The authors thank Scott Heller, MD, for his contributions to this paper.
References
Footnotes
Contributors JB, SCH, and CLW developed the idea for the paper. WCM planned and designed the paper. WCM, MK, JB, and SCH all contributed to writing and editing this article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.