Article Text

Abstract
Background and objectives The nerve to vastus medialis (NVM) supplies sensation to important structures relevant to total knee arthroplasty via a medial parapatellar approach. There are opposing findings in the literature about the presence of the NVM within the adductor canal (AC). The objective of this cadaveric study is to compare the effect of injection site (distal femoral triangle (FT) vs distal AC) on injectate spread to the saphenous nerve (SN) and the NVM.
Methods Four unembalmed fresh-frozen cadavers acted as their own control with one thigh receiving 20 mL of dye injected via an ultrasound-guided injection in the distal FT while the other thigh received an ultrasound-guided injection in the distal AC. A standardized dissection took place 1 hour later to observe the extent of staining to the NVM and SN in all cadaver thigh specimens.
Results In all specimens where the injectate was introduced into the distal FT, both the SN and NVM were stained. In contrast, when the dye was administered in the distal AC only the SN was stained.
Conclusions Our findings suggest that an injection in the distal AC may be suboptimal for knee analgesia as it may spare the NVM, while an injection in the distal FT could provide greater analgesia to the knee but may result in undesirable motor blockade from spread to the nerve to vastus intermedius.
Statistics from Altmetric.com
Introduction
Total knee arthroplasty (TKA) is a common surgical procedure for arthritis and is increasingly prevalent with an ageing population. It is frequently associated with severe postoperative pain, particularly on movement.1 To enable successful rehabilitation following TKA, multimodal analgesia incorporating a regional anesthetic technique should be used. Ideally, the regional anesthetic technique should alleviate pain without causing significant leg weakness.
Combining proximal nerve blocks (eg, femoral, sciatic, and obturator) provides optimal analgesia for TKA,2 but the muscle weakness induced can impair postoperative mobility and contribute to an increased risk of falls.3 Blocking nerves at a more distal site to maximize inhibition of nociceptive afferents while minimizing motor involvement is desirable.
One peripheral block that has gained much popularity for TKA is the adductor canal (AC) block. This involves depositing local anesthetic within the triangular shaped neurovascular tunnel formed by the sartorius muscle superficially, the vastus medialis muscle (VMM) anterolaterally and the adductor longus muscle (ALM) and adductor magnus muscle posteromedially. The AC extends proximally from the apex of the femoral triangle (FT), at which point it communicates with that compartment, and distally to the adductor hiatus, through which it communicates openly with the popliteal fossa. Compared with femoral nerve block, an AC block has the desirable effect of preserving quadriceps function while maintaining a similar analgesic profile.4 , 5
A consistent contributor of knee innervation is provided by the nerve to vastus medialis (NVM). The NVM has large intramuscular and extramuscular branches that travel obliquely through and round the medial (deep) aspect of the VMM belly.6 These branches are in close proximity to the junction of the medial epicondyle and femoral shaft and terminate distally on the anteromedial knee capsule via the medial retinacular nerve.7 It is this supply to the medial retinacular complex that makes the NVM such a vital nerve to target when managing pain for patients undergoing surgery involving the medial region of the knee at the distal portion of the femur and the anterior capsule (ie, TKA via a medial parapatellar approach).8
There is inconsistency in the literature as to the presence of the NVM within the AC. Burckett-St Laurant et al found 100% of the intramuscular NVM branches and 35% of extramuscular branches within the AC.6 In contrast, Horner and Dellon describe the NVM to be within the VMM belly in 90% of subjects throughout the AC.9 In addition, the NVM has been shown to travel in a separate fascial sheath distinct from the AC below the level of the FT.10
A further explanation for this variation in dissection findings is the disparity in the definition of where exactly the AC is located in the thigh.11 Manickam et al described the injection of local anesthetic in the distal AC, just proximal to the adductor hiatus to obtain an isolated saphenous nerve (SN) block to provide medial ankle analgesia.12 Lund et al described a more proximal approach directed by surface anatomy to place local anesthetic at the midpoint between the anterior superior iliac spine (ASIS) and the base of the patella to provide analgesia to the anterior knee.13 Using surface anatomy to identify the midpoint of the thigh will result in local anesthetic being injected into the FT, not the AC.14 This problem was highlighted in a recent meta-analysis comparing AC block with femoral nerve block where the authors concluded that a high variation in location of AC block performed in the literature made it difficult to draw strong conclusions.15
The inconsistency of anatomical study findings attempting to locate the NVM in the AC and the variation in anatomical landmark description of the AC in study designs may explain why a degree of uncertainty exists regarding which nerves are affected when one carries out what they perceive to be an AC block.
The primary objective of this cadaver study is to determine the effect of injectate location site by comparing an injection in the distal FT with an injection in the distal AC on achieving successful spread to the NVM.
Secondary objectives include:
Demonstration of a separate fascial sheath present around the NVM in the AC and if this could inhibit spread of injectate to this important nerve.
Using discrete ultrasonographical landmarks to identify reproducible locations in the distal FT and distal AC and comparing these with mid-thigh measurements based on surface anatomy landmarks of ASIS and the inferior border of the patella.
Methods
This cadaveric study was conducted in June 2017 within the Anatomy Licensed Area in the Centre for Biomedical Sciences Education at Queen’s University Belfast. Four unembalmed fresh-frozen human cadavers with no evident scars from previous hip, thigh, or knee surgery or trauma were used for this anatomical study. Consent for anatomical examination had been obtained from each of the donors whose remains were used for this study. Identifiable information of the deceased (such as height, weight, medical history, or ethnic background) was not available to study investigators.
Prior to ultrasound-guided determination of injection locations, surface anatomy landmarks frequently used in the literature to identify the midpoint of the thigh were marked on the cadavers. These landmarks included the ASIS, the distal sartorius segment at the medial epicondyle of the femur and the midpoint at the base of the patella.
Distal FT injection point
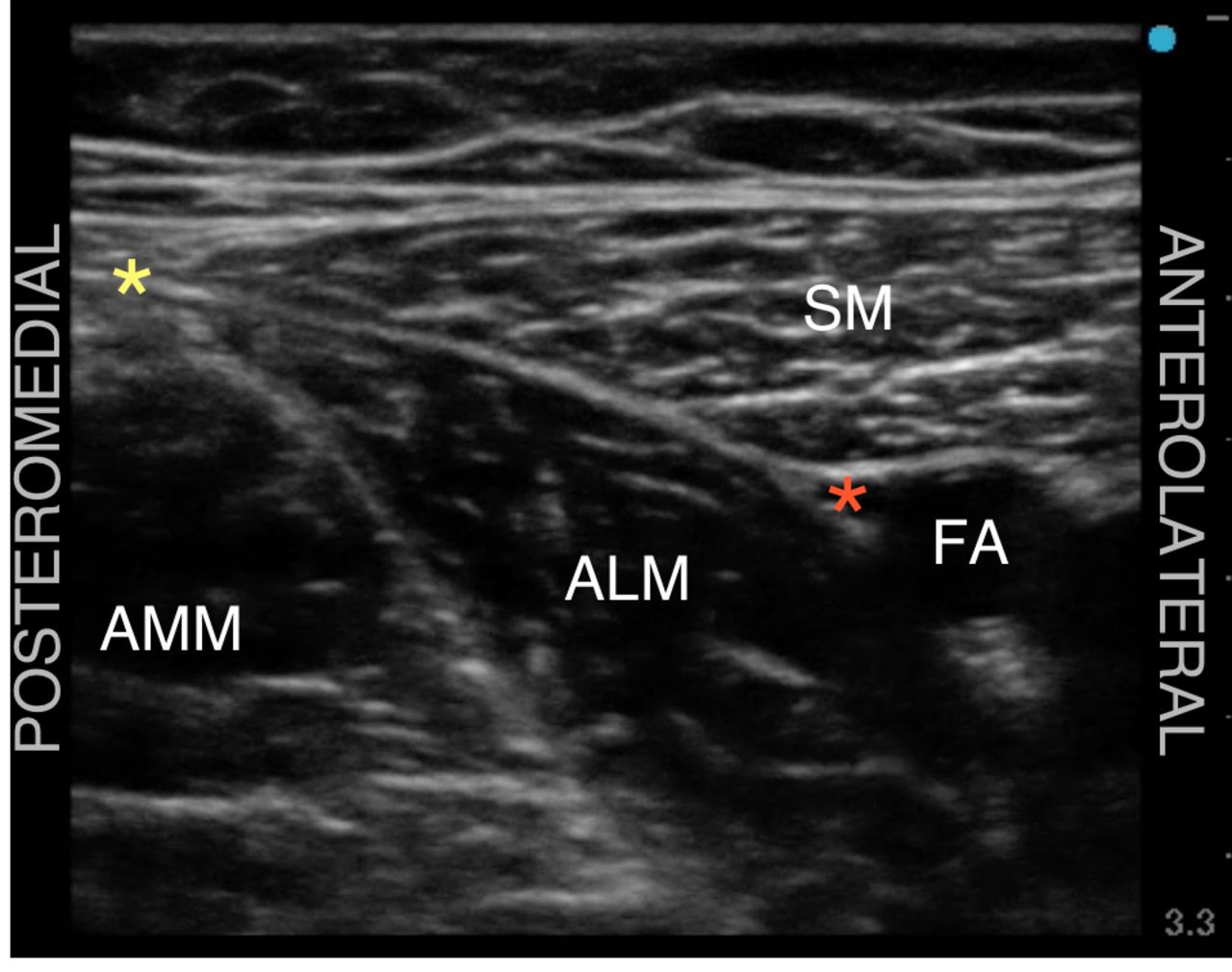
A 13.6 MHz 6 cm high-frequency linear transducer Sonoite Edge (FUJIFILM SonoSite, Bothell, Washington) was used to confirm FT position by scanning distally from the ASIS along the sartorius muscle path (DFJ). The distal FT injection point was marked 1 cm proximal to the triangle apex (ie, its distal margin). This was identified at the point where medial borders of sartorius muscle and ALM aligned (figure 1).11

Ultrasound image demonstrating the femoral triangle apex. This point was confirmed to lie distal to the femoral triangle injection point. Red asterisk: endpoint target for needle tip; yellow asterisk: alignment of medial borders of sartorius and adductor longus muscles. ALM, adductor longus muscle; AMM, adductor magnus muscle; FA, femoral artery; SM, sartorius muscle.
Distal AC injection point
The AC was then scanned distally until the femoral artery could be seen descending deep toward the adductor hiatus (DJ). The point where the femoral vessels plunge between ALM and gracilis muscles was taken as the distal margin of the AC.16 This is demonstrated in figure 2. The injection location was marked at 1 cm proximal to the divergence of the femoral artery at the AC distal margin.

Ultrasound image demonstrating the distal adductor canal. The point at which the femoral artery descended toward the adductor hiatus was taken as the distal adductor canal margin. Red asterisk: corresponding endpoint target for needle tip (this was inserted just proximal to this image). AMM, adductor magnus muscle; DGA, descending geniculate artery; FA, femoral artery; SM, sartorius muscle; VMM, vastus medialis muscle.
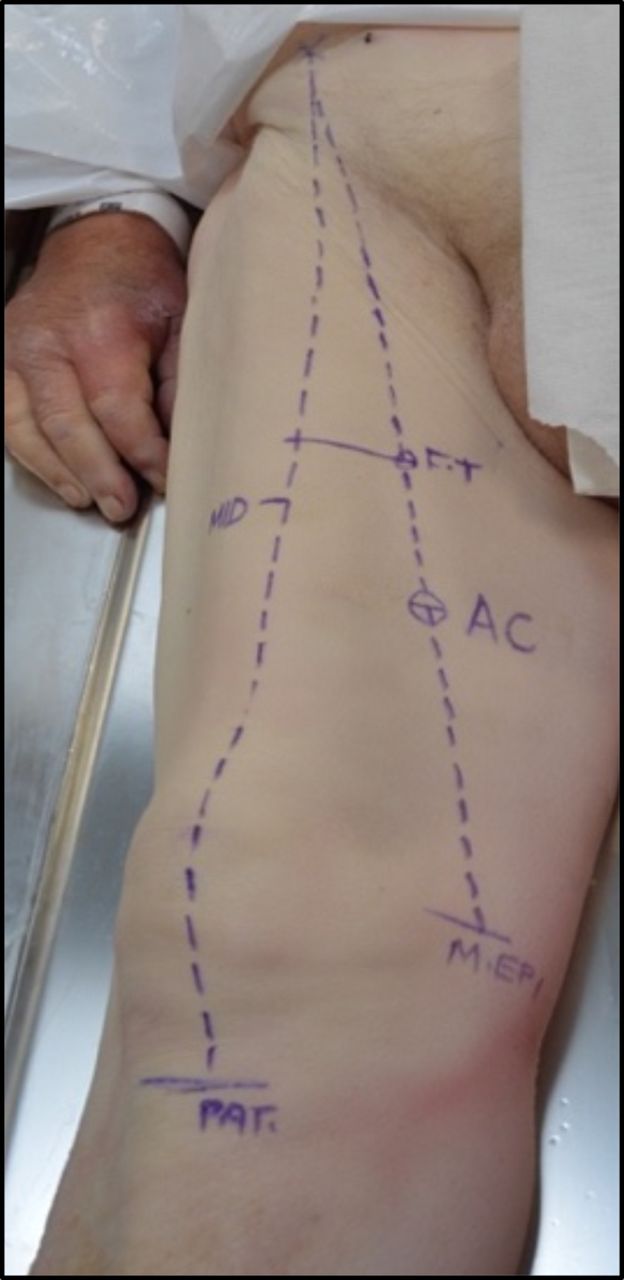
Surface markings for injection points and surface anatomy landmarks are shown in figure 3.
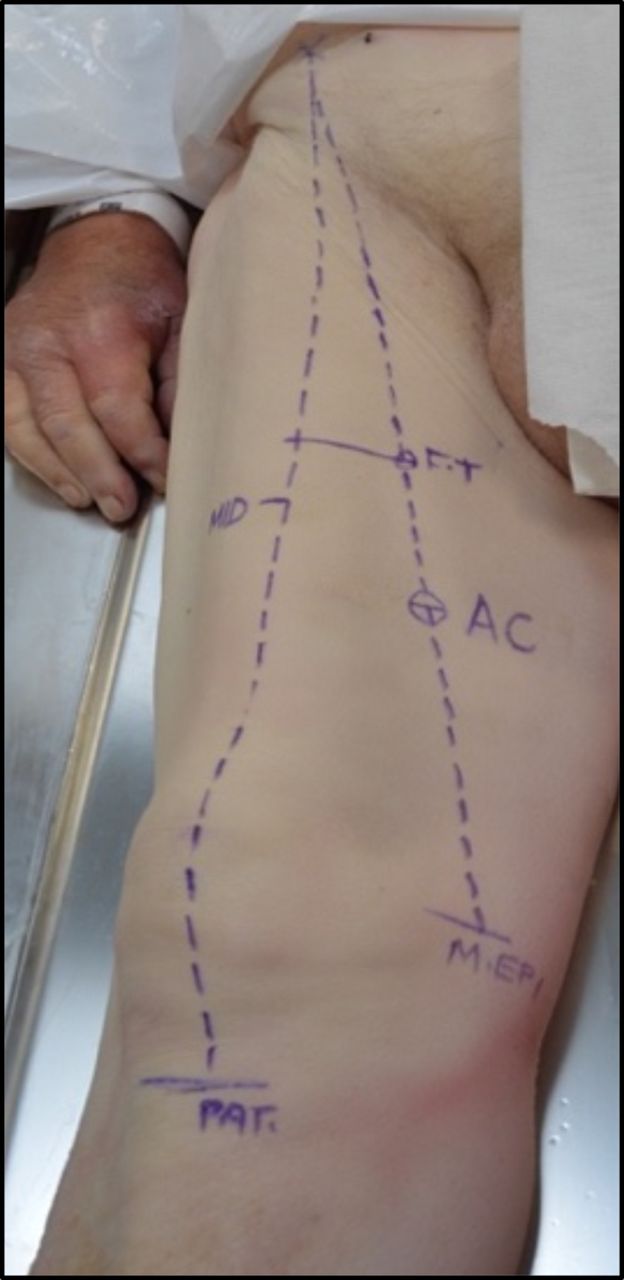
Surface landmarks of thigh (right). AC, adductor canal; FT, femoral triangle injection point; M EPI, medial femoral epicondyle; MID, midpoint of thigh.
Each cadaver acted as their own control to compare injectate spread (ie, where an FT injection was placed in one thigh, an AC injection would be placed in the other). Laterality was decided by the toss of a coin prior to starting injections.
Injections were all performed by the same investigator (NB). A saline flushed 90 mm SonoPlex 20 G needle (Pajunk, Geisingen, Germany) attached to a 20 mL syringe containing saline was advanced in plane from an anterolateral to posteromedial direction. Identical depth and gain settings were used for each injection. Distal FT or AC injections were carried out according to the coin toss at the exact point previously marked on the specimen thigh. Once the needle tip had traversed through the deep fascia of the sartorius muscle at the 9–11 o’clock position relative to the superficial femoral artery, 2 mL of saline was injected to confirm position (red asterisk marked in figures 1 and 2). Once confirmed, a 20 mL syringe containing 19.5 mL of methyl cellulose mixed with 0.5 mL green ink was attached to the needle connecter. Continuous pressure was used to inject the entire contents over 30 s without moving the needle from its confirmed position.
A separate study investigator (RC) performed all dissections which were commenced exactly 1 hour after injectate completion. A longitudinal incision was made from the medial tibial plateau as far superiorly as possible toward the midpoint of the inguinal crease. A second incision was made from the ASIS to meet the proximal aspect of the first. A transverse incision was then made from the medial tibial plateau laterally toward the head of the fibula. This pattern of dissection allowed reflection of the skin and subcutaneous tissue overlying the thigh laterally in one piece.
After skin and subcutaneous fat was reflected, the sartorius muscle was incised proximally, close to its origin at ASIS and distally at the pes anserinus. The sartorius muscle was reflected medially in one piece to expose the underlying subsartorial canal. The femoral nerve was identified in the FT, immediately inferior to the inguinal ligament. The branches of the nerve were then followed distally until the NVM and SN were located. Once the NVM had been located, the nerve with its muscular branches was dissected carefully taking care not to contaminate findings with spill of injected contents. After NVM dissection, the SN was then dissected out of the AC. All dissection findings were photographed and archived by an independent observer blinded to injectate group.
Results
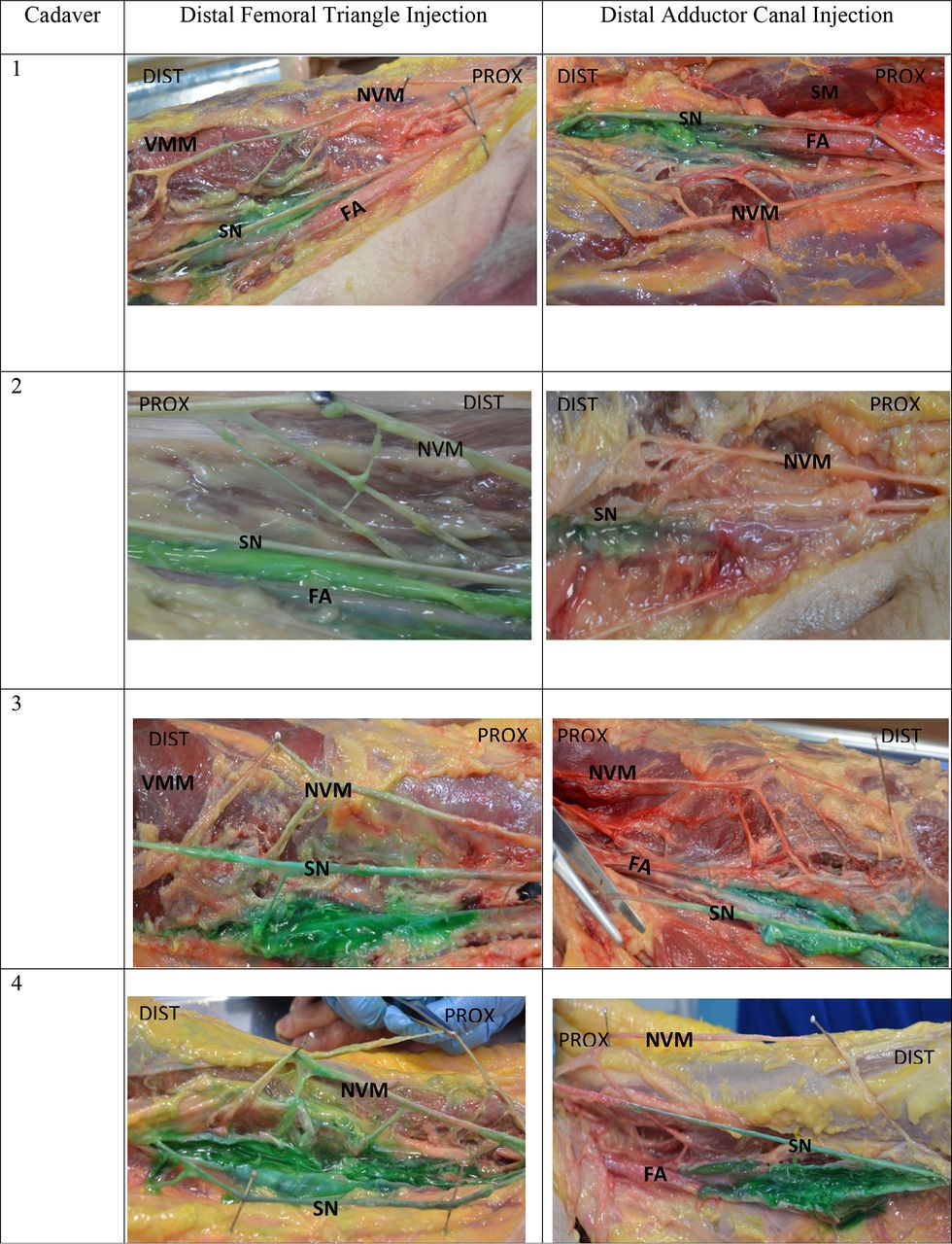
Results from the surface landmarks and cadaver age are recorded in table 1. In all eight specimens, the SN and NVM were identified. Results for staining of these nerves are displayed in figure 4. In all specimens where the injectate was introduced into the distal FT, the SN and NVM were both stained, while in all specimens where the distal AC injection was performed, only the SN was stained.
Age, gender and thigh measurements of cadaver specimens

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Dissection findings of four cadaver thigh specimens one hour after femoral triangle injections (left column) and adductor canal injections (right column). DIST, distal; FA, femoral artery; NVM, nerve to vastus medialis; PROX, proximal; SM, sartorius muscle; SN, saphenous nerve; VMM, vastus medialis muscle.
A consistent finding was the presence of the tough fascial layer of the vastoadductor membrane. This surrounded the AC and seemed to prevent the spread of the four AC injectates toward a more superficial and proximal direction. This fascial layer was separate from the deep connective tissue layer of the investing sartorius muscle fascia.
Discussion
This is the first cadaveric study to directly compare the impact of injection location on the reliability of staining the NVM using reproducible sonographic landmarks. Numerous anatomical studies have confirmed the importance of the NVM contribution to knee innervation.6 17–20 , , This is relevant for TKA via medial parapatellar arthrotomy because the NVM enters the knee capsule deep to medial retinaculum, supplies the medial collateral ligament and terminates as the medial retinacular nerve. This terminal branch then pierces the medial knee capsule deep to the medial retinaculum and supplies the ligamentous intra-articular knee structures and the undersurface of the patella.9 21 22
While addressing the issue of locating NVM it is important to clarify the terms AC and FT. The FT is a region located between the inguinal ligament proximally, the sartorius muscle laterally and the ALM medially. The apex of the FT is defined as the intersection between the medial borders of the sartorius muscle and the lateral border of the ALM.23 The subsartorial canal exists immediately distal to the apex of the FT (ie, where the femoral vessels travel deep to the sartorius muscle). The AC continues distally until the superficial femoral artery descends through the adductor hiatus. The take-off of the descending genicular artery is commonly seen just proximal to this point. Accessibility to this region is aided by the patient’s ability to flex and externally rotate the hip.
The distal location of the FT injection point was chosen to minimize proximal injectate spread toward the inguinal ligament. This was to reflect clinical practice where regional anesthetists will often seek to achieve analgesia of distal femoral nerve branches (eg, SN and NVM) while minimizing the risk of causing quadriceps weakness due to femoral nerve involvement. Consequently, a distal point of the AC was chosen to give sufficient distance from the FT injection point to allow a measurable comparison between the distal margins of the two anatomical locations. Choosing the proximal or midpoints of the AC may not have given the same contrasting results. One potential drawback of the distal AC location is the observation of injectate spread into the popliteal fossa via the adductor hiatus which has been previously described.24 Despite attempts to maintain motor sparing effects by placing distal AC injections, motor nerve involvement may still occur due to spread toward the popliteal fossa.
We confirmed that the distal FT injection point defined sonographically was consistently superior to the midpoint of the thigh (halfway point between ASIS and inferior border of patella) consistent with the findings of Wong et al.14 The nomenclature adapted for sonoanatomical descriptions of injection techniques of the thigh can be misleading. The injection performed in this study for the FT was actually performed deep to the sartorius muscle 1 cm proximal to the apposition of the medial borders of sartorius and ALM (ie, superior to the proximal margin of the AC). This was not technically a direct FT injection but rather a subsartorial injection at the level of the FT. Injection here will undoubtedly spread into the FT itself as it is a continuous plane with no fascial borders separating the two locations. In order to define ultrasound-guided injections, where the needle will be passed through the sartorius to juxtaposition the tip lateral to the superficial femoral artery, we as regional anesthetists have erroneously been calling this an FT block. Perhaps a ‘mid-thigh sub-sartorial block’ would be technically more accurate. Altering the name from a mid-thigh AC block to a mid-thigh FT block (or even to a mid-thigh subsartorial block) should not alter the results or interpretations of the published clinical findings that describe subsartorial injections in the mid-thigh area. One such example of this was the volunteer study conducted by Grevstad et al.25 Healthy volunteers underwent ‘mid-thigh AC block’ procedures with varying volumes of local anesthetic. The VMM had volume dependent effects demonstrated by electromyography brought about by the mid-thigh injections. Details of specific sonoanatomical landmarks for the injections of this study were not included other than the injection point being described as ‘mid-thigh ACB’. One could contend the injections were actually being performed at the level of the FT, but the involvement of the NVM was demonstrated consistently for mid-thigh injections nonetheless.
In all AC injectates the echogenic vastoadductor membrane could be readily visualized on ultrasound as well as sensed with a definite loss of tactile resistance change as the needle tip advanced into the AC. In contrast, the needle pass for the FT injections lacked the vastoadductor membrane ‘ceiling’ and the change of needle resistance was much more subtle as the deep fascia of sartorius was breached. On dissection findings, the vastoadductor membrane was easily located and could be seen as a continuous partition throughout its length. The proximal margin of the vastoadductor membrane was consistently found between our two chosen injection points. This may contribute to why proximal spread of AC injectate to stain other branches of the femoral nerve was inhibited.
It is interesting that while vessels and nerves can pass from FT to AC, proximal spread of injectate placed just 9–10 cm distally is prevented. Our findings of reduced proximal spread of AC injectate into the distal FT are consistent with previous cadaveric studies. Dissections by Cowlishaw and Kotze26 and Ishiguro et al 27 also demonstrated limited cephalad spread from the AC into the FT with consequent sparing of femoral nerve branches to sartorius, rectus femoris and vastus lateralis.
In live patients, elements including dynamic tissue planes, patient positioning and inflation of a thigh tourniquet may result in different spread than what was demonstrated in cadaver specimens. The use of methylcellulose as an injectate stabilizing agent to facilitate dissections may have limited proximal spread that may not have been reflective of less viscous injectates (such as local anesthetic agents or MRI contrast used by Jæger et al where injections of 20 mL into the AC spread proximally to the FT in 50% of cases).28 Consequently, a distal AC block in vivo could indeed still result in more proximal spread toward the NVM. The small number of cadaver specimens is a further limitation to this study.
Cadaver 4 had an estimated weight of around 50 kg and in the FT injectate side, some of the dye spread proximally toward the inguinal crease and stained other branches of the femoral nerve (nerve to vastus intermedius). This only happened on one out of four FT injections but none of the AC injections. In clinical practice, this may represent a potential drawback of performing an FT block at a more proximal location in an attempt to anesthetize the NVM; other branches of the femoral nerve may become blocked.
This study does pose an important clinical question: If the NVM contributes significant analgesia for TKA undergoing medial parapatellar approach, should the regional anesthetist opt for a true distal FT block instead of distal AC block? The findings from this small cadaveric study suggest that a distal AC block may miss the NVM and likely result in suboptimal analgesia compared with more proximal injections. This is in keeping with the findings by Burckett-St Laurant et al who recommended an injection in the mid-AC as a means to block both the SN and NVM.6 The converse argument would contend that injectate placed within the distal AC could avoid blocking the NVM as an advantage to prevent VMM weakness while still blocking the SN with its infrapatellar branch and the subsartorial plexus. This could contribute to analgesia without causing quadriceps weakness. A clinical study of TKA patients comparing distal AC with distal FT blocks is needed to compare outcomes of pain, analgesia consumption and quadriceps strength.
Conclusions
In summary, this small cadaveric study suggests that an injection in the distal AC may consistently reach the SN only while it spares the NVM, while an injection in the distal FT consistently reaches both nerves. In addition, our findings also suggest that involvement of additional motor nerves (such as the nerve to vastus intermedius) is more likely to occur with an injection in the FT compared with the distal AC.
Acknowledgments
Thanks to Declan McLaughlin who photographed the anatomy specimens following dissection.
References
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Provenance and peer review Not commissioned; externally peer reviewed