Article Text

Abstract
Background Erector spinae plane block (ESPB) is a novel regional anesthesia technique that is gaining popularity for postoperative pain management. This randomized controlled trial evaluated the effect of ESPB on quality of recovery (QoR) in patients undergoing modified radical mastectomy.
Methods Eighty-two female patients undergoing modified radical mastectomy were included. Patients were randomly assigned to receive preoperative ultrasound-guided ESPB with either 0.5% ropivacaine or saline. The primary outcome was QoR, assessed 24 hours postoperatively using the 15-item QoR questionnaire (QoR-15). Secondary outcomes included postoperative pain scores, postoperative cumulative opioid consumption, postanesthesia care unit (PACU) discharge time, postoperative nausea or vomiting and dizziness.
Results Global QoR-15 scores 24 hours postoperatively were significantly higher (indicating better quality) in the ESPB group (median 120, IQR 118–124) compared with the control group (median 110, IQR 108.3–112.8), with a median difference of 10 (95% CI 9 to 12, p<0.001). Compared with the control group, ESPB with ropivacaine reduced pain scores up to 8 hours after surgery, as well as reduced postoperative cumulative opioid consumption and PACU discharge time.
Conclusions A single preoperative injection of ESPB with ropivacaine may improve QoR postoperatively and acute postoperative analgesia in patients undergoing a modified radical mastectomy.
Trial registration number ChiCTR-1800019599.
- truncal blocks
- acute pain
- interventional pain management
- postoperative pain
Statistics from Altmetric.com
Introduction
Breast cancer is the most frequently diagnosed malignancy and is the leading cause of cancer-related death among the female population.1 Modified radical mastectomy is a standard surgical treatment, which may be associated with moderate to severe acute postoperative pain. Adequate postoperative pain relief is imperative to improve functional outcomes and to accelerate discharge from the hospital.2
Several strategies, including local and regional anesthesia, are now performed as core components of multimodal analgesia for postoperative pain.3–5 Ultrasound-guided erector spinae plane block (ESPB) is a novel interfacial plane block first introduced by Forero et al 6 for pain control. Due to its feasibility, safety and efficacy, ESPB is gaining popularity for perioperative analgesia for many different types of surgeries.7–9 However, its efficacy for analgesia related to breast procedures is not convincing.10 Additionally, to date, the effectiveness of ESPB on the quality of recovery (QoR) from the patient’s perspective following breast cancer surgery remains unclear.
In this randomized, controlled trial, we hypothesized that a single adjunct injection of ESPB with general anesthesia would improve the pain relief and recovery of patients after breast cancer surgery.
Methods
Design and patients
The study was registered at the Chinese Clinical Trial Registry (http://www.chictr.org.cn) on 19 November 2018. All Consolidated Standards of Reporting Trials guidelines for reporting randomized controlled trials were followed. Eighty-two female participants, aged 18–65 years with American Society of Anesthesiologists (ASA) physical status I or II, who were scheduled for elective unilateral modified radical mastectomy, were invited to participate. Exclusion criteria included known local anesthetics or non-steroidal anti-inflammatory drugs allergies, infection near the puncture site, known coagulation disorders, chronic pain, use of pain medications and inability to provide consent.
After written informed consent was obtained, participants were randomly assigned to undergo ESPB with either 25 mL of 0.5% ropivacaine (ESPB group) or 0.9% physiological saline (control group) before general anesthesia. Randomization was performed with a 1:1 ratio using a computerized random number generator (http://www.randomization.com). Assignments were sealed in sequentially numbered envelopes. Randomization, blinding procedures and study drug preparations were handled by a research nurse who was not involved in the trial. The study drugs, 0.5% ropivacaine and saline, were drawn up into syringes that looked identical. All participants, the surgeon and the anesthesiologist, postanesthesia care unit (PACU) personnel and research staff who collected the study data were not informed of the group assignments.
Intervention
Ultrasound-guided unilateral ESPB was performed before general anesthesia in a lateral decubitus position. After 2 mg of midazolam was administered intravenously, an experienced attending anesthesiologist (Dr Hao Li) performed the blocks for all patients using real-time ultrasound similar to Yavuz et al.11 Briefly, a 6–13 MHz linear array transducer was placed longitudinally 2–3 cm lateral to the T4 spinous process under aseptic conditions to achieve clear visualization of the erector spinae, rhomboid major and trapezius muscles. An 80 mm 22-gage b-bevel needle was inserted into the interfacial plane between the erector spinae muscle and the transverse process of the vertebra using an in-plane technique. Once the correct location was confirmed by hydrodissection of the interfascial plane with 2 mL of saline solution, 25 mL of 0.5% ropivacaine or saline was injected for the block.
Anesthetic procedure
All patients fasted for at least 6 hours prior to the procedure. On arrival at the operating room, standardized monitoring, including noninvasive blood pressure, ECG, peripheral pulse oximetry, capnography and temperature were continuously monitored. General anesthesia was induced using 0.5 µg/kg sufentanil and 2.0 mg/kg propofol. After induction, a bolus injection of 0.15 mg/kg cisatracurium was given to facilitate laryngeal mask airway (LMA) insertion. All patients received sevoflurane in a mixture of oxygen and fresh air to maintain the hemodynamic parameters (heart rate and mean arterial blood pressure) within 20% of original preoperative values. Muscle relaxation was maintained by intermittent injections of cisatracurium as needed. At the end of the procedure, residual neuromuscular blockade was antagonized with 40 µg/kg neostigmine and 20 µg/kg atropine. After removal of the LMA, all patients were admitted to the PACU and were observed for at least 2 hours. Postoperative pain control was standardized in this study. Before skin incision occurred, 50 mg of flurbiprofen axetil (a non-steroidal anti-inflammatory drug) was given intravenously, followed by injections of 50 mg flurbiprofen axetil injection every 8 hours. Additionally, all participants received patient-controlled intravenous analgesia (PCIA) with sufentanil for postoperative analgesia. The PCIA was set to deliver sufentanil at a rate of 1 µg/hour. If the visual analog scale (VAS) score was above 3, an intravenous bolus injection of 2 µg sufentanil was administered as a rescue analgesic, with a lock-out interval of 6 min via the PCIA device.
Outcomes
In this study, the primary outcome was QoR, assessed 24 hours after surgery using the Chinese version of the 15-item QoR questionnaire (QoR-15).12 The QoR-15 covers five clinical dimensions, including physical comfort (five items), emotional state (four items), psychological support (two items), physical independence (two items) and pain (two items). The global QoR-15 score ranges from 0 (poor recovery) to 150 (excellent recovery).13 Secondary outcomes included postoperative pain scores, postoperative cumulative opioid consumption, PACU discharge time, the incidence of PONV and dizziness, and ESPB-related adverse events. A single trained research assistant blinded to group assignment assessed all outcomes. Self-reported VAS pain scores (0=no pain and 10=worst imaginable pain) at rest and on movement were scored at 0.5, 1.0, 2.0, 4.0, 8.0 and 24.0 hours postoperatively. The PACU discharge time was defined as the time from PACU admission to the time the patients’ modified Aldrete score reached 10.14 Postoperative nausea or vomiting (PONV) was treated with intravenous administration of 4 mg ondansetron plus 5 mg dexamethasone. Dizziness (on sitting) was recorded from 2 to 24 hours postoperatively.
Statistical analysis
The sample size was calculated based on the global QoR-15 score. A change of 8 for the QoR-15 scores was considered to represent a clinically relevant difference.15 According to our preliminary study without ESPB, the QoR-15 scores 24 hours postoperatively were equivalent to 114 (10.6). We estimated that our research would have 90% power to detect an increment of 8 in the QoR-15 scores at a significance threshold of 0.05 with 37 participants in each group. Taking into consideration a 10% dropout rate, we enrolled a total of 82 participants in this study.
All statistical analyses were performed with IBM SPSS software V.25.0. We assessed the normality of quantitative variables with the Shapiro-Wilk test and Q–Q plots. The quantitative variables were expressed as mean (SD) or median (IQR). Student t-tests were used to compare the mean values of age, weight, height, duration of surgery and PACU discharge times. Mann-Whitney U-tests were used to analyze the global QoR-15 score and postoperative cumulative sufentanil consumption. For each statistical comparison, the 95% CI of the difference is given. Qualitative variables were reported as number and proportion. The χ2 test was used to compare the ASA classification proportions and the number of patients reporting PONV. Fisher’s exact test was used to compare the proportion of dizziness between groups. Additionally, a two-way repeated-measures analysis of variance using a Bonferroni correction for multiple comparisons was used to evaluate postoperative pain scores up to 24 hours after surgery. P values less than 0.05 for two-tailed tests were considered statistically significant.
Results
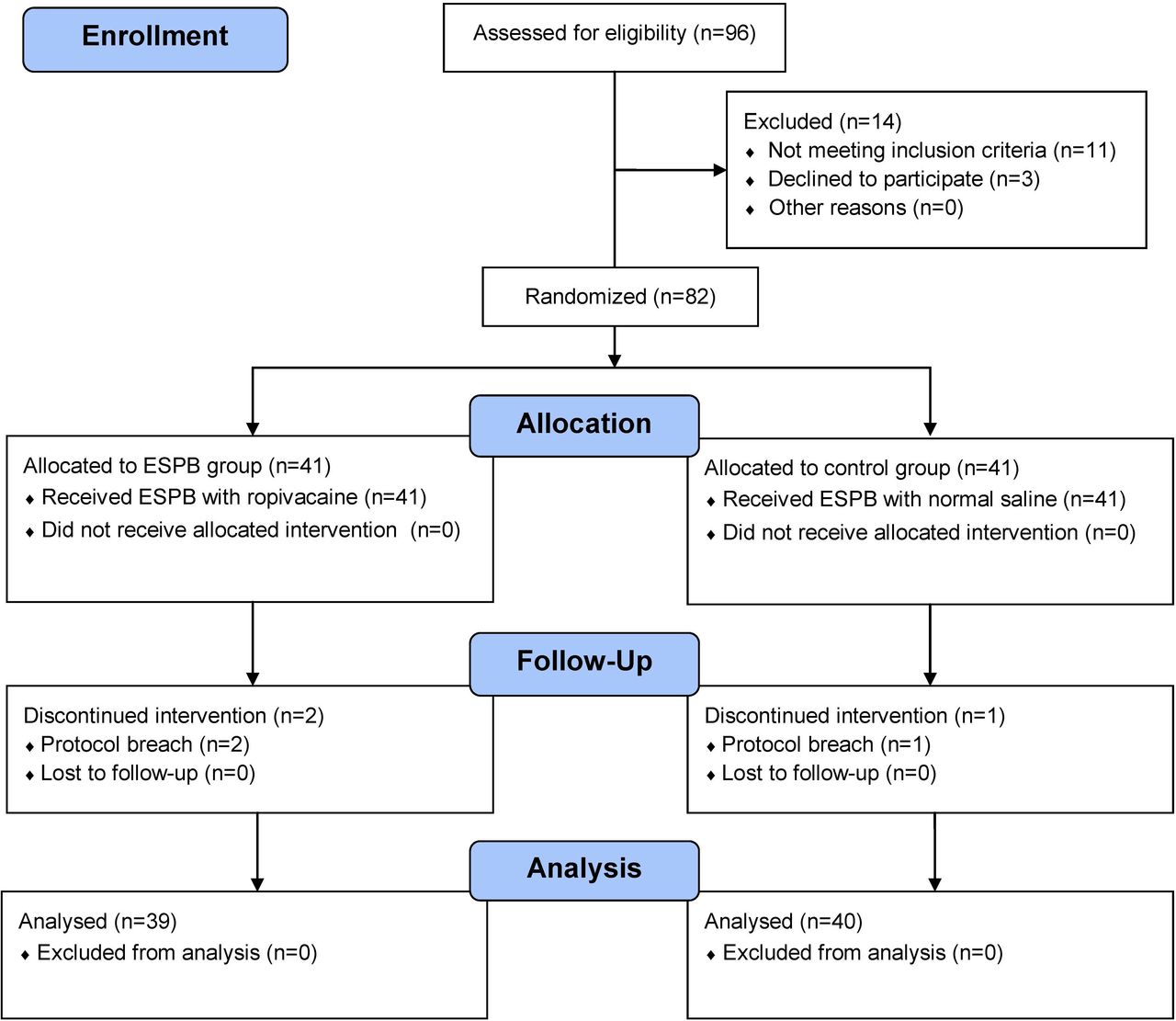
The CONSORT 2010 flowchart is shown in figure 1. From January to August 2019, we screened 96 potential participants who were scheduled for elective unilateral modified radical mastectomy under general anesthesia. Eleven participants were deemed ineligible based on the inclusion criteria, and three declined to participate. A total of 82 participants were enrolled in this trial. Following randomization, two patients from the ESPB group and one patient from the control group were excluded due to a breach in protocol. Thus, data from 79 patients were used in the final analyses. The patient demographics and duration of surgery were similar between groups (table 1).
Patient characteristic and clinical data in the study

Consolidated standards of reporting trials (CONSORT) flowchart describing patient progress through the study. ESPB, erector spinae plane block.
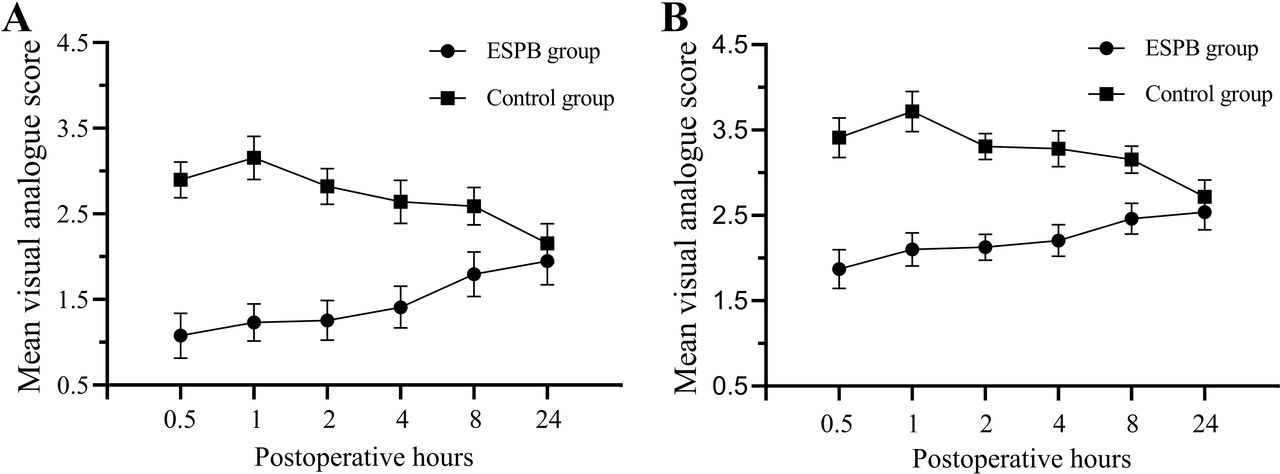
The global QoR-15 scores are shown in figure 2. The global QoR-15 score 24 hours postoperatively was significantly higher (better recovery) in the ESPB group than in the control group (estimated median difference: 10, 95% CI 9 to 12, p<0.001). Administration of ESPB with 0.5% ropivacaine before surgery reduced acute VAS pain scores both at rest and on movement during the first 8 hours postoperatively (all p<0.001, figure 3). There was no significant difference 24 hours postoperatively at rest (p=0.13) or on movement (p=0.18). Compared with the control group, postoperative cumulative opioid (sufentanil) consumption during the first 24 hours after surgery was lower in the ESPB group (median 24 μg, IQR 24–28, vs median 40 μg, IQR 36–42; p<0.001). The median difference between the ESPB and the control group was 14 µg (95% CI 12 to 16, p<0.001).

Violin plots of the global QoR-15 scores (79 patients) before surgery and 24 hours after surgery. The global QoR-15 scores in the ESPB group were higher than those in the control group (median difference: 10,95% CI 9 to 12, p<0.001 by the Mann-Whitney U-test). Notes: the violin plots show the distributional shape of the data using kernel density estimation. The white dot represents the median; the thick bar represents the IQR; and the thin line represents the rest of the distribution. ESPB, erector spinae plane block; QoR, quality of recovery.

{kind=link}
{kind=link}
{kind=link}
Mean visual analog scale pain scores at rest (A) and on movement (B) in patients receiving ESPB with 0.5% ropivacaine or saline during the first 24 hours postoperatively. There was a significant time-by-group interaction at rest and on movement (both p<0.001). Note: the error bars represent 95% CIs. ESPB, erector spinae plane block.
As shown in table 2, the incidence of PONV was 3/39 (7.7%) in the ESPB group and 9/40 (22.5%) in the control group, which was not significantly different (p=0.07). One and five patients in the ESPB and control groups reported dizziness, respectively. Furthermore, participants in the ESPB group met the PACU discharge criteria earlier than the control group (mean difference 11.2 min, 95% CI 9.9 to 12.5, p<0.001). No ESPB-related adverse events (eg, local anesthetic toxicity, pneumothorax, bleeding or infection) were observed in the study.
Outcome measurements during the study period
Discussion
Our study demonstrated that the combination of ESPB with 0.5% ropivacaine improves the QoR compared with general anesthesia alone. Furthermore, a preoperative single injection of ESPB provided superior pain relief in the early postoperative period, reduced the postoperative cumulative opioid consumption and shortened the duration of PACU admission. Taken together, these findings indicate that preoperative administration of ESPB may be a useful intervention to aid recovery following breast cancer surgery. Hence, our results have important clinical and social implications as an optimal QoR is required to ensure early discharge from the hospital.
Recovery after surgery and anesthesia is a multidimensional, inter-related and complex process with several inter-related domains that extends beyond postoperative pain. Thus, the implementation of patient-centered outcomes has been proposed by several national healthcare organizations to enhance the quality of care.16 The QoR-15 is a validated quality assessment tool that can be used to evaluate the efficacy of interventions on the QoR after surgery from the patient’s perspective.17 18 In this study, preoperative ESPB resulted in a change of 10 for the QoR-15 score, signifying a clinically relevant improvement in the early postoperative health status of patients.
Although this study was not sufficiently powered to detect differences in the incidences of PONV and dizziness, participants in the ESPB group showed lower scores in both domains. No episodes of clinically significant hypotension or bradycardia were reported in this study, possibly because ESPB only produces a somatic blockade, not a sympathetic blockade. Additionally, no side effects related to ESPB (eg, pneumothorax, local anesthetic toxicity and injury to vascular or nervous structures) were identified during this study. Given the ease of ultrasound identification of the anatomical structures (even in obese patients, and the relatively low risk of adverse effects, ESPB is a promising potential component of multimodal analgesia strategies for patients undergoing breast surgery when the thoracic epidural analgesia or paravertebral block is not feasible.
This study had some limitations that will need to be clarified in order to determine the validity of the results. First, all participants received a standardized postoperative multimodal analgesic regimen, including flurbiprofen axetil and sufentanil, which are known to distort the effectiveness of ESPB. Second, the dermatomal distribution of ESPB was not evaluated by thermal quantitative sensory testing due to the blinded nature of this study. However, the ultrasound-guided ESPB is likely the most accurate approach, and all blocks were administered by a single experienced anesthesiologist. Hence, we believe that most of the blocks were implemented successfully. Lastly, the generalizability of the results is limited, considering that the present study was from a single center with restrictive inclusion criteria, and lacked typical preoperative multimodal methods of analgesia.
Conclusions
In summary, it appears that under our experimental conditions, a single preoperative injection of ESPB is an effective strategy for enhancing the QoR following breast cancer surgery.
Acknowledgments
We thank Dr Hui Zhang and Dr Lei Han for their assistance with the study.
Footnotes
YY and HL contributed equally.
Contributors YY: conceptualization, design, supervision, validation, formal analysis and writing of the original draft. HL: design, project administration, data curation and writing of the original draft. QH: project administration, data curation, writing of the review and editing. TC: project administration, data curation and formal analysis. YW: project administration, data curation. XZ: conceptualization, design, resources, supervision, validation, writing, review and editing. All authors read and gave final approval of the version to be published.
Funding This study was supported by Fujian Medical University Startup Fund for scientific research (grant number 2018QH1142), Fujian Joint Funds for the Innovation of Science and Technology (grant number 2017Y9066), Natural Science Foundation of Fujian Province (grant number 2018J01246), Fujian Medical Innovation Project (grant number 2019-CXB-6) and Fujian educational research projects (grant number JAT160234).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Our institutional research ethics board approved the study protocol for this single-center, prospective, randomized, double-blind, placebo-controlled clinical trial.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.