Article Text

Abstract
Background Opioids are prescribed in excess after surgery. We leveraged our continuous quality improvement infrastructure to implement opioid prescribing guidelines and subsequently evaluate changes in postoperative opioid prescribing, consumption and patient satisfaction/pain in a statewide regional health system.
Methods We collected data regarding postoperative prescription size, opioid consumption and patient-reported outcomes from February 2017 to May 2019, from a 70-hospital surgical collaborative. Three iterations of prescribing guidelines were released. An interrupted time series analysis before and after each guideline release was performed. Linear regression was used to identify trends in consumption and patient-reported outcomes over time.
Results We included 36 022 patients from 69 hospitals who underwent one of nine procedures in the guidelines, of which 15 174 (37.3%) had complete patient-reported outcomes data following surgery. Before the intervention, prescription size was decreasing over time (slope: −0.7 tablets of 5 mg oxycodone/month, 95% CI −1.0 to −0.5 tablets, p<0.001). After the first guideline release, prescription size declined by −1.4 tablets/month (95% CI −1.8 to −1.0 tablets, p<0.001). The difference between these slopes was significant (p=0.006). The second guideline release resulted in a relative increase in slope (−0.3 tablets/month, 95% CI −0.1 to −0.6, p<0.001). The third guideline release resulted in no change (p=0.563 for the intervention). Overall, mean (SD) prescription size decreased from 25 (17) tablets of 5 mg oxycodone to 12 (8) tablets. Opioid consumption also decreased from 11 (16) to 5 (7) tablets (p<0.001), while satisfaction and postoperative pain remained unchanged.
Conclusions The use of procedure-specific prescribing guidelines reduced statewide postoperative opioid prescribing by 50% while providing satisfactory pain care. These results demonstrate meaningful impact on opioid prescribing using evidence-based best practices and serve as an example of successful utilisation of a regional health collaborative for quality improvement.
- clinical practice guidelines
- continuous quality improvement
- health policy
- patient satisfaction
- quality improvement
Statistics from Altmetric.com
- clinical practice guidelines
- continuous quality improvement
- health policy
- patient satisfaction
- quality improvement
Introduction
Morbidity and mortality from prescription opioids remain a national public health crisis in the USA as well as multiple other nations and impact nearly every aspect of clinical care.1 2 Opioids prescribed after surgery are a major contributor to this problem.3 4 Prescriptions after surgery account for a substantial share of prescriptions in the USA,5 and the majority of postoperative opioids prescribed to opioid-naïve patients remain unused.6 7 These unused tablets are rarely discarded and have the potential to cause harm in at least two distinct ways. First, a significant proportion of patients who receive excess opioids in the postoperative setting will continue using opioids and transition to chronic opioid users. About 10% of paediatric and adult patients continue to fill opioid prescriptions for months after surgery, particularly if receiving larger prescriptions.8–11 While most patients will let these pills sit in their cabinets and not transition to persistent use, the larger the postoperative prescription, the higher the risk of persistent use. Second, unused tablets can be diverted towards non-medical use or abuse and are a primary pathway for transition to heroin use.12 13 In response, surgeons have faced substantial pressure to decrease opioid prescribing for acute and postoperative pain to minimise the risks of opioid diversion and chronic opioid use. For example, 37 US states have introduced legislation limiting the duration of opioid prescriptions for acute pain.14
Prescribing guidelines that recommend specific prescription sizes after surgical procedures are a potential approach to reduce excessive opioid prescribing and additionally represent an opportunity to reduce the variability in prescribing habits, but their effectiveness has not yet been demonstrated over a large population of patients. Successful reductions in postoperative prescribing using guidelines have been limited to individual institutions, but the inclusion of key patient reported outcomes, including pain and satisfaction, has been variable.15–20 In addition, interventions aimed only at surgeons are unlikely to result in sustained improvements. Numerous factors influence surgeons’ prescribing behaviours,21 and nurses, residents, pharmacists and other clinicians also play important roles in postoperative pain care, including patient counselling and expectation setting. Engaging these stakeholders can streamline communication with patients and address barriers to practice change. A resulting reduction in overall size and variability in prescribing may help prevent further harm by decreasing the flow of excess tablets into patients’ homes and the community.
Here we describe the iterative implementation of prescribing guidelines to reduce excessive postoperative opioid prescribing across a statewide population using a learning statewide health system. These guidelines were disseminated using targeted engagement of multidisciplinary clinicians, patients and other diverse stakeholders. This study evaluates the impact of these interventions on postoperative opioid prescription size, patient opioid consumption, variability in prescribing habits and postoperative satisfaction and pain.
Methods
Context
In 2016, the Michigan Opioid Prescribing Engagement Network (Michigan-OPEN) was established to achieve substantive impact around opioid prescribing in the acute care setting. Michigan-OPEN is a partnership between clinicians in multiple specialties (surgery, primary care and anesthesiology), the Michigan Department of Health and Human Services and Blue Cross Blue Shield of Michigan (a major private payer in the state of Michigan in the USA). This clinician-led, public–private partnership assembled key stakeholders who collectively prioritised improving opioid prescribing after surgery as a preventative approach to combat the opioid crisis.
Michigan-OPEN developed prescribing guidelines to reduce postoperative prescribing based on prescription size, patient consumption and patient-reported outcomes. The impact of these guidelines was evaluated using an interrupted time series analysis of postoperative prescription size using data from February 2017 to May 2019. This model tested whether the point in time when each of three sets of guidelines (online supplemental figures S1, S2, and S3) were released (October 2017, April 2018 and January 2019) was associated with a change in either intercept or slope for the linear best fit line for prescription size before compared with after the intervention. Trends in patient-reported opioid consumption, satisfaction and postoperative pain were also investigated.
Supplemental material
Supplemental material
Supplemental material
This report follows the Revised Standards for Quality Improvement Reporting Excellence 2.0 Guidelines for quality improvement reports.22
Data source and prescribing guideline creation
One factor contributing to excessive postoperative prescribing was a lack of evidence for how much to prescribe after any given procedure.23 To create guidelines based on actual patient opioid use, Michigan-OPEN partnered with the Michigan Surgical Quality Collaborative (MSQC), a regional surgical quality improvement collaborative of 70 hospitals (including all hospitals performing major surgery in the state). The MSQC functions as a learning health system and maintains a validated clinical registry for general, vascular and gynaecological surgeries, capturing a random sample of 50 000 patients per year. Hospital participation is voluntary, and hospitals receive funding from Blue Cross Blue Shield of Michigan to employ a trained clinical nurse reviewer to abstract patient characteristics, perioperative processes of care, 30-day postoperative and patient-reported outcomes, and healthcare utilisation measures. Cases included in the MSQC are randomly sampled according to an algorithm designed to minimise selection bias and represent all eligible cases at each hospital. Data are regularly audited to ensure validity.24 Of the 70 hospitals included in the MSQC, 69 were able to provide valid prescription data for this project and were therefore included in the analysis.
Starting 1 January 2017, Michigan-OPEN leveraged the MSQC’s existing data flows to collect data on postoperative opioid prescriptions, patient-reported opioid consumption, refill and other patient-reported outcomes including satisfaction with care and postoperative pain. At hospitals participating in this data collection effort, prescription data were abstracted from the medical chart for a subset of patients included in the MSQC registry. These patients were contacted for patient-reported outcomes, as described in more detail previously.25 Patients received a telephone or mail survey at postoperative day 30 and were given 90 days to respond (online supplemental appendix 1). Patients reported how many opioid tablets they had consumed in the first 30 days postoperatively, their satisfaction with care and their pain score in the first 7 days after surgery. Data regarding preoperative opioid use were not collected.
Supplemental material
In October 2017, Michigan-OPEN used opioid consumption data to form procedure-specific prescribing guidelines (online supplemental figure S1) for nine procedures (in tablets of 5 mg oxycodone):
Laparoscopic cholecystectomy (10 tablets).
Laparoscopic appendectomy (10 tablets).
Minor hernia repair, including laparoscopic or open inguinal, femoral, umbilical and epigastric hernia repair (10 tablets).
Open ventral/incisional hernia repair (25 tablets).
Laparoscopic colectomy (25 tablets).
Open colectomy (25 tablets).
Vaginal hysterectomy (15 tablets).
Laparoscopic hysterectomy (20 tablets).
Open abdominal hysterectomy (25 tablets).
These nine procedures were selected as they had 25 or more cases with opioid consumption data. The 75th percentile of patient consumption served as the starting point for each recommendation, similar to a model used successfully elsewhere.15 The prescribing guidelines were released on 6 October 2017. With continued data collection, guidelines were updated in April 2018 and January 2019 to include more procedures and reflect up-to-date patient consumption.26
Specific change management techniques were used by Michigan-OPEN and the MSQC. First, institution-specific dashboards are created so that each hospital has access to their specific data. This data system was previously established for collaborative quality improvement work. Second, these data were linked to an aggressive communication strategy that focused on tying institution and physician-specific practices to emotion. Significant harm had occurred within our state related to overprescribing, and we made it clear to every practitioner that they were potentially part of the problem. Efforts were made to communicate this message to thousands of practitioners across the state. Multiple communication methods were used to promote the guidelines to clinicians, patients, community members and other stakeholders. Electronic methods included Twitter, MSQC mailing networks, webinars, videos, Blue Cross Blue Shield of Michigan newsletters and the Michigan-OPEN and MSQC websites. In addition, over 135 in-person presentations were given to an estimated 12 000 attendees, with a variety of audiences including surgical and non-surgical clinician groups, nurses, primary care consortiums, community health organisations and layperson audiences in the US state of Michigan. Third, a specific pathway for change was provided in the form of statewide prescribing guidelines as described above. Overall, these institution-specific data were linked to compelling stories so that there was a clear goal and clear motivation for change. The care pathway in the form of prescribing guidelines was used as a template for practice change.
The strength of this collaborative model for quality improvement is that change happens by nurses and doctors at the bedside, and each institution uses different strategies to make this change with variable effectiveness. A surgeon champion and surgical quality nurse reviewer for each institution attend collaborative meetings and receive all content from the MSQC. The MSQC provides ongoing support and answers questions. Intentional efforts are made to link similar institutions so that ideas can be shared regarding change techniques. The quality collaborative provides guidance and motivation for change but does not prescribe specific techniques to individual institutions.
Study of the intervention and measures
The primary outcome of interest was postoperative opioid prescription size in oral morphine equivalents. In this way, prescription size encompasses both tablet strength as well as prescription quantity. Secondary outcomes were patient-reported consumption, prescription refill, satisfaction and pain after discharge. Change in prescribing practice variability was calculated as the difference in the preguideline and postguideline coefficient of variation (itself calculated as the ratio of the SD and the mean prescription size for a given time period) divided by the preguideline coefficient of variation, displayed in percentage points. Only patients who received a prescription for opioids at discharge were included in this analysis. Prescription and consumption data were converted into oral morphine equivalents (OME) to adjust for potencies of different medications and allow for comparison across patients x opioid types.27 For ease of interpretation, prescription and consumption are presented in equivalent numbers of 5 mg oxycodone tablets, where one 5 mg oxycodone tablet equals 7.5 mg OME.
A questionnaire was sent to all patients 30 days postoperatively (online supplemental file 1). Patient-reported satisfaction was measured on a scale of 1–10 (1=‘extremely dissatisfied’, 10=‘extremely satisfied’). For pain, patients were asked to rate their pain in the first 7 days after surgery on a scale of 1–4 (1=‘no pain’, 2=‘minimal pain’, 3=‘moderate pain’ and 4=‘severe pain’). Patient characteristics included age (<45 years, 45–64 years and 65+ years), gender, race (white, black and other), tobacco use within 1 year, history of alcohol abuse, functional status and ASA classification. Refills were also assessed as part of the postoperative questionnaire. Patients were asked whether they received a refill of their pain medication prescription at any point between the surgery and the date of the survey, and this is reported as a proportion.
Supplemental material
Analysis
Data collection began as a pilot effort in January 2017. We elected to exclude data from January 2017 during the immediate implementation period for consistency. For analysis, we included data from February 2017 to May 2019. We then excluded patients who did not undergo one of the nine procedures included in the guidelines. The month of the interventions was set as October 2017, April 2018 and January 2019, corresponding to each iterative release of prescribing guidelines from the collaborative.
Univariate comparisons of patient characteristics were performed between the preintervention and postintervention cohort using χ2 tests. Interrupted time series analyses of postoperative prescription size was performed to determine trends before and after the intervention (guideline release).28 Prescription data were grouped by month of surgery, and the mean for each month served as a data point. The Cumby-Huizinga test for autocorrelation was performed. There was no significant autocorrelation, and we used ordinary least squares regression to determine trends in postoperative opioid prescribing and guideline concordance across time period. Opioid consumption, satisfaction, refill and pain were analysed by month of the operation using linear regression to calculate trends over time. Significance was set at p value <0.05. All analyses were performed with Stata V.16.
Ethical considerations
Owing to the use of data for quality improvement as well as the deidentified nature of the data, the institutional review board at the University of Michigan, Ann Arbor, Michigan, USA, deemed this study exempt from approval. There were no specific ethical issues considered when developing this quality improvement intervention. There were no conflicts of interest for any of the authors of the study. Blue Cross Blue Shield of Michigan, a private non-profit insurance company within the state of Michigan, USA, provided financial support for this initiative and had no other involvement in the project, including the guideline development, data analysis, drafting of the manuscript, critical revision or the decision to submit for publication.
Results
Characteristics of the cohort
We collected valid prescription data for 40 672 patients from 69 hospitals; we then excluded 4413 patients who did not undergo one of the nine procedures included in the prescribing guidelines. Two hundred and thirty-seven patients from January 2017 were also excluded, leaving a final cohort of 36 022 patients. The preintervention and postintervention patients were generally similar (table 1). Overall, 20 768 (57.7%) patients were women. The mean (SD) age was 51.5 years (16.3 years). Out of this cohort, a subset of 15 174 (37.3%) patients had complete patient-reported outcomes after surgery.
Patient characteristics
Change in opioid prescription size and guideline concordance after guideline release
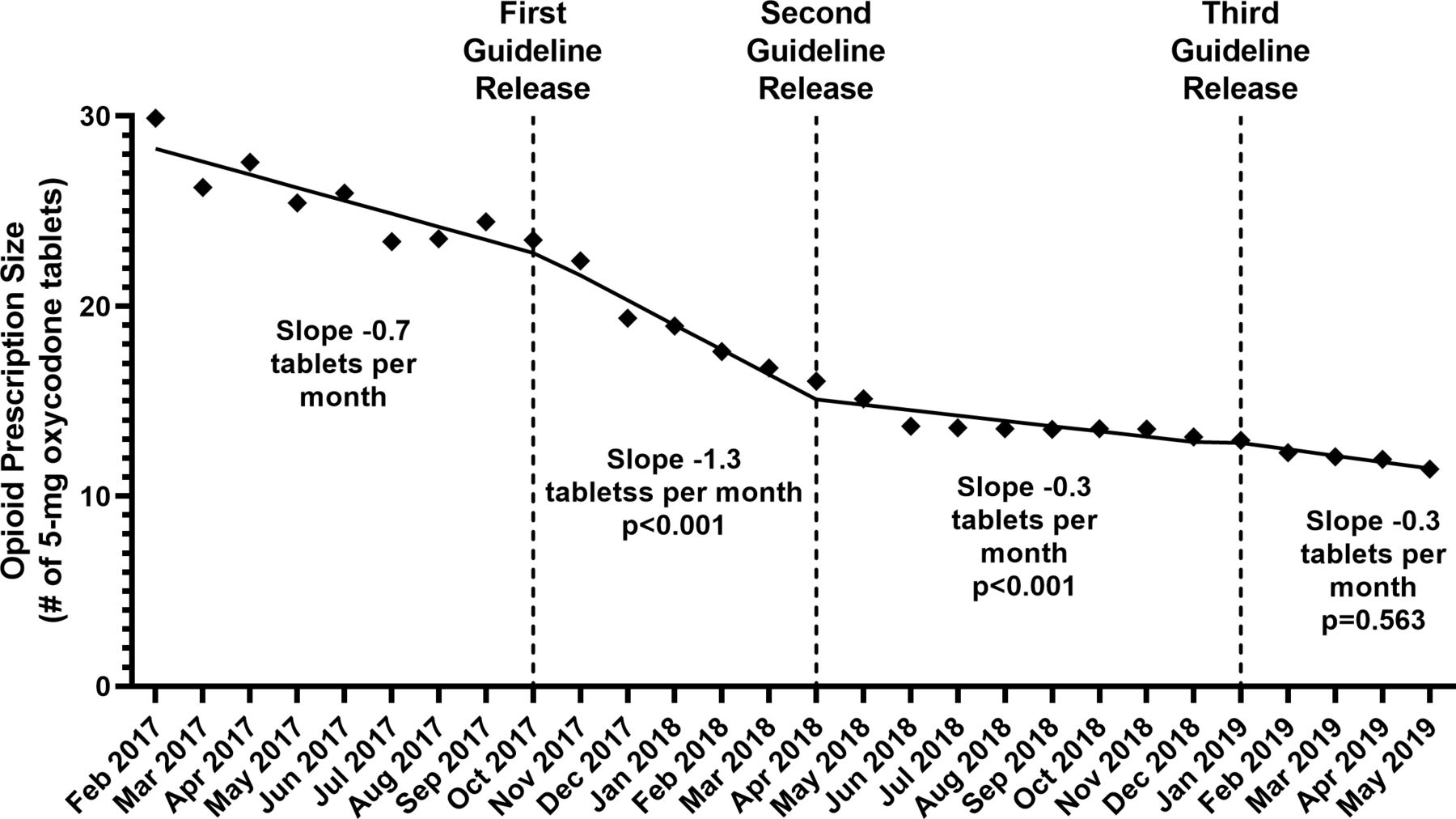
Starting in February 2017, the mean (SD) opioid prescription size after surgery was 224 (113) OME, equivalent to about 30 (15) tablets of 5 mg oxycodone. Before guideline release, there was a significant change in prescription size over time (slope −5.2 mg OME or −0.7 tablets per month, 95% CI −0.9 to −0.4 tablets, p<0.001). After guideline release, there was a significant decline in prescription size of –5.2 mg OME or −1.3 tablets per month (95% CI −1.6 to −1.0 tablets, p<0.001). This represented a significant decrease of −0.6 tablets per month in slope (95% CI −1.1 to −0.14, p=0.014) between the preintervention and postintervention trends. There was no immediate change in prescription size at the time of guideline release (p=0.449). Following the second guideline release in April 2018, the decrease in prescription size per month slowed to a slope of −0.3 tablets per month (95% CI –0.5 to −0.1 tablets, p=0.005 for the slope, p<0.001 for the intervention effect on slope). There was also no effect of the guideline release on the intercept for prescription size (p=0.978). The third guideline was released in January 2019 and resulted in no significant change in the slope of −0.3 tablets per month (95% CI −0.4 to −0.3 tablets, p<0.001 for the slope, p=0.562 for the intervention effect on slope). Again, we found no immediate effect of guideline release on prescription size (p=0.563). In May 2018, the mean prescription size was equivalent to 15 (9) tablets or a 50% decrease (figure 1).

Prescription size before and after guideline release. After the prescribing guidelines were released in October 2017, postoperative opioid prescription size declined significantly. Change in slope (ie, decrease in prescription size in tablets of 5 mg oxycodone per month) from before to after guideline release was statistically significant at p<0.05 for both the first and second guideline releases. P values shown are for the change in slope at the time of the previous intervention. Linear trends for each time period are statistically significant with p<0.001.
Decreases in procedure-specific prescribing were also seen. The largest decreases in postoperative prescription size were seen for open colectomy, which decreased from 34 (33) to 15 (10) tablets (p<0.001), and major hernia repair, which decreased from 28 (18) to 14 (9) tablets (p<0.001). The smallest decrease was seen for vaginal hysterectomy (23 (13) to 14 (7) tablets, p<0.001) (table 2).
Procedure prescription sizes in February 2017 and May 2019
Opioid consumption, refill, satisfaction and pain over time
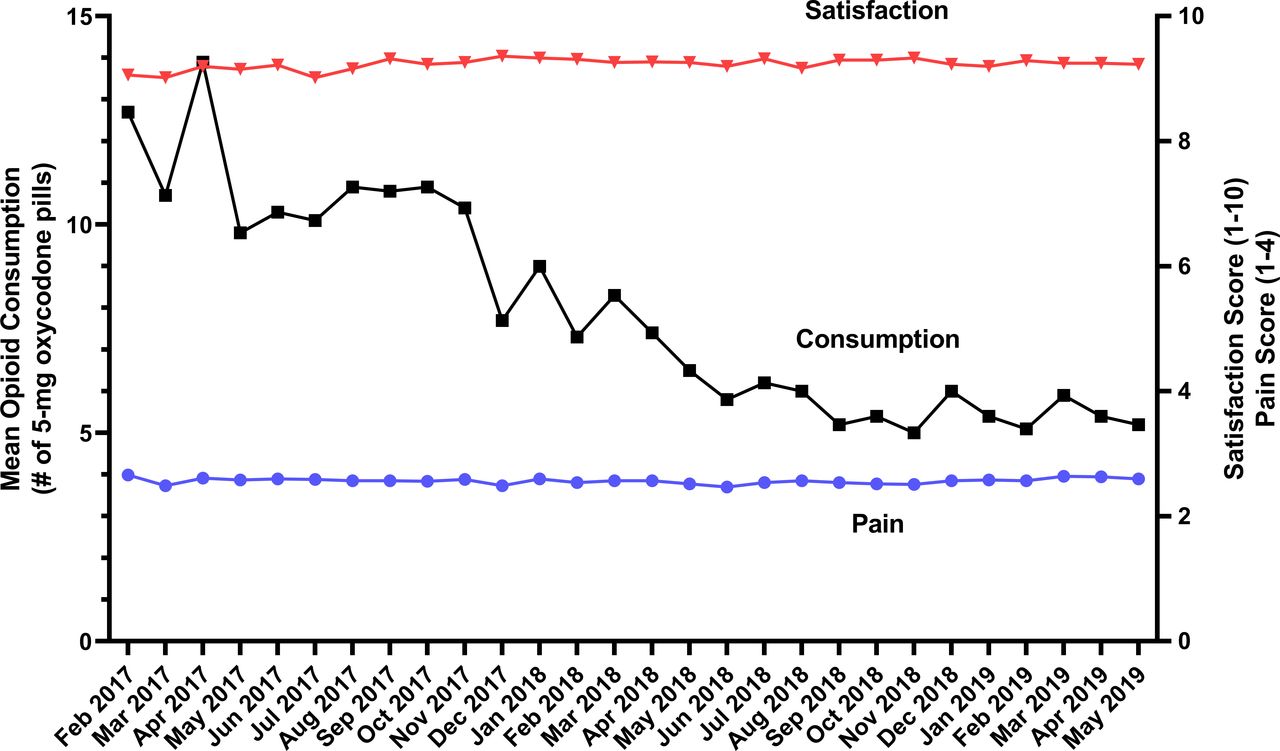
Mean (SD) opioid consumption after surgery decreased by 50% from 13 (17) tablets in February 2017 to 6 (7) tablets in May 2019 (p<0.001). Six per cent of patients received a refill in February 2017 compared with 3% in May 2019 (p<0.001) (online supplemental appendix 1). During this time period, patient-reported outcomes remained clinically stable (figure 2). In February 2017, mean (SD) satisfaction with care score was 9.0 (1.9) points out of 10, and there was a statistically significant increase of 0.005 points/month (95% CI −0.002 to –0.009, p<0.001). Mean (SD) reported postoperative pain score in February 2017 was 2.7 (0.9) points out of 4 and 2.6 (0.8) in May 2019, without a significant change over time (p=0.801).

Opioid consumption and patient-reported outcomes. Patient-reported opioid consumption decreased by 50% over the study time period, while patient-reported satisfaction with care and pain in the week after surgery remained stable (n=15 552).
Variability in prescribing practices over time
Significant variability was seen in prescribing practices for the time period prior to any prescribing guideline release, with an overall coefficient of variation of 68. This narrowed to 64 for the time period following the third guideline release, representing a relative improvement of 5.9% in unifying practice patterns across prescribers. Change in the coefficient of variation was highly dependent on the type of procedure, as shown graphically in figure 3. Total abdominal hysterectomy and open colectomy represented procedures with a particularly large decrease in the coefficient of variation (−24.6% and −33.3%, respectively), while guideline release was associated with a relatively smaller magnitude change in coefficient of variation for other surgical procedures included.

{kind=link}
{kind=link}
{kind=link}
Change in coefficient of variation for prescription size before and after guideline release. Change in coefficient of variation represents the proportional change in coefficient of variation from before the release of the first guidelines to after the release of the third guidelines. Negative values result from less variability in prescribing in the postguideline release period, while positive values result from more variability in prescribing.
Discussion
Over a 1.5-year period in the state of Michigan, mean postoperative prescription size after a variety of surgical procedures decreased by half, from an equivalent of 30 to 15 tablets of 5 mg oxycodone. After the release of procedure-specific prescribing recommendations, there was a significant decline in postoperative prescription size and an increase in guideline concordant prescribing, suggesting success of the guidelines in changing prescribing practice. Despite significant decreases in both prescribing and consumption, patient-reported satisfaction and pain scores remained stable. Variation in prescribing patterns was also shown to decrease following release of the guidelines and particularly for two of the operations included. We cannot evaluate the reasons for these procedure-specific effects on prescription variability based on these data alone. However, it is notable that the procedures where a decrease in variability was found were procedures that are completed less commonly. Common procedures are more likely to have individual or institution specific standard prescription sizes. Guidelines for the uncommon procedures would therefore serve to provide both a lower overall prescription size target as well as serve to standardise what was previously highly variable prescribing practices. This contrasts with common operations for which prescriptions were already consistent but larger than necessary. Overall, this example demonstrates the potential to substantially reduce excessive prescribing and variation in prescribing patterns after surgery—which can reduce the risk to patients and communities—without adversely affecting the patient experience.
Although similar changes in prescribing have been previously demonstrated at the institutional level,20 29–31 this work is an expansion of our initial experience with using this model to affect change within Michigan.32 Prior work including a recent study from the group at Massachusetts General Hospital showed improvement in prescription sizes without an increase in refill requests, but their guidelines were generated by surgeon consensus rather than actual patient consumption data, and furthermore they failed to assess patient-reported outcomes data such as pain scores and satisfaction that may be adversely affected by guideline implementation, particularly when those guidelines did not include the patient experience in their development.33 Importantly, the prescribing guidelines in this intervention were based on actual patient-reported opioid use, potentially mitigating concerns about inadequate pain control for patients. Adjustments for preoperative opioid use were not specified, so these guidelines can theoretically apply to all postoperative patients. In addition, continuous data collection allowed us to iteratively revise the guidelines to reflect decreases in patient consumption, while confirming that patient-reported outcomes were not negatively impacted. These changes are aligned with recommendations from the Centers for Disease Control and Prevention to prescribe the ‘lowest effective dosage’ for opioid analgesia.34 Further reductions may allow surgeons to better match prescribing to consumption to minimise excess medication, while continued consumption and patient-reported outcomes data will help indicate the ‘floor’ of prescribing to provide the minimum necessary analgesia. The observed decrease in opioid consumption also suggests that surgeons can have a direct influence on their patients’ opioid use after surgery by modifying their own prescribing practices.
Another crucial component of this intervention was strategic partnership with patients, payers, interprofessional groups and the community. With these communication efforts, we sought support for our intervention from key stakeholders in postoperative pain care, rather than targeting prescribers alone. Involvement of these groups facilitated guideline dissemination and addressed barriers to guideline adoption. Ongoing in-person and electronic communication ensured that prescribers had access to the most up-to-date evidence when the guidelines changed. This strategy helped build relationships, foster collaboration and motivate practice change towards overall improved prescription sizes as well as uniformity across the state. While a significant undertaking, we believe this represents an important example of the successful development, implementation and utilisation of a regional health system to address an important clinical and public health concern using the infrastructure of the health system itself.
Our data suggest that an iterative learning process is important and also reveal that not every intervention is successful, but rather success stems from the iterative process and continuous learning that is a critical component of these efforts. We believe the inclusive nature of the system is a central principle of regional system design. Specifically, all stakeholders need to be engaged for their input and unique perspective. This involves casting a wide net initially, including the entire breadth of hospital types/sizes/locations within the proposed system to ensure that any solution developed works for all members. Furthermore, input cannot be sourced from a single individual at each health system, but rather must empower all the individuals who will be affected by the intervention, including physicians, nurses, pharmacists, healthcare administrators, payers and communities, to be engaged in the learning process and serve as an important source of knowledge and feedback for iterative improvement. Finally, flexibility is an essential attribute for the system and any intervention it implements. There will be unforeseen challenges and consequences of the interventions over time and having the organisational agility to manoeuvre around these obstacles will allow for prompt solutions to these challenges. One example here is our difficulty initially in linking data from the Prescription Drug Monitoring Program in Michigan due to legislative constraints at the state level. This required us to develop alternative methods of patient-reported outcome measurement in order to develop improved guidelines. In our system, strong central leadership combined with broad organisational buy-in from participating health systems and payers are the critical components that allowed success in addressing the opioid epidemic. A recent systematic review of behavioural interventions to decrease opioid prescribing found that consensus-based processes, clinical practice guidelines, educational meetings and clinician reminders, among others, were all effective strategies. Our intervention combined these strategies to maximally impact opioid prescribing across the collaborative.35 Our experience should serve as a platform for future health system development and guide other systems in implementation of a successful intervention.
This project is not without limitations. First, a causal relationship between the prescribing guidelines and the decrease in postoperative prescribing cannot be inferred from this quasiexperimental study. It is possible that the observed decrease reflected temporal trends, given the increase in general awareness about the opioid crisis. However, while contemporaneous population-level data for surgical patients is not available given the recency of this study, studies up to 2012 and 2016 suggest that surgical prescription sizes are actually increasing over time.5 36 In addition, a study of complete US opioid prescriptions from 2012 to 2017 (including surgical and non-surgical prescriptions) found a decreasing trend in opioid prescription sizes of −0.62 mg OME/month from March 2016 to December 2017. This rate is much smaller than our observed downtrend after the intervention of −10.5 mg OME/month, suggesting that temporal trends alone may not be responsible for the decrease observed in our study. The slope changes in prescription size as well as the improvement in prescribing variation after release of prescribing guidelines also suggest a direct effect of the intervention on prescribing practice. Over the time period of this study, new regulatory efforts also drew attention to prescribing, though the specific statewide limitations were many-fold higher than the mean prescribing amounts detailed here in. Another limitation is inherent to the use of patient-reported outcomes, including incomplete data collection in patients who did not complete a postoperative survey, and the problem of recall bias depending on when a patient is surveyed.37 Recall of personal opioid consumption following surgery, assessed at 30 days, may be particularly susceptible to recall bias due to the interval between measurement and event. However, differential recovery and pain trajectories for the variety of surgical procedures included may also function as a source of bias, particularly early on in the recovery period. For this reason, we believe patient-reported outcome assessment at 30 days allows for a balance between the risk of recall bias and temporal bias on outcome measurement in this study. Only patients who received a prescription for opioids at discharge were included in this analysis. In this way, it is possible that there was a significant change in the proportion of patients who received no opioids over the course of the study and also that the guidelines may have influenced this proportion. An increase in the proportion of patients without a discharge opioid prescription would serve to bias our results towards the null rather than inflate the effect size found here. Finally, this study also did not collect data that may have been beneficial to report, such as clinical outcomes.
Conclusion
In summary, this study describes a 50% decrease in postoperative opioid prescribing across a statewide regional health system following release of procedure-specific prescribing guidelines. For other clinicians, the increasing consolidation of hospitals into healthcare networks represents an opportunity for large-scale replication of these results, leveraging existing relationships to disseminate evidence-based best practices for postoperative opioid prescribing. These groups may avoid duplication of work by adopting existing guidelines from this study or other sources. Their effort can then be spent collecting prescribing data and patient-reported outcomes to measure the effect of interventions. As clinicians respond to legislative and clinical pressures to reduce postoperative opioid prescribing, they must ensure that patients are satisfied with pain care.
References
Footnotes
Twitter @MichaelEnglesbe
Funding National Institute on Drug Abuse (5 R01 DA 042859 03) and Michigan Department of Health and Human Services (E20203204-00, E20203205-00, E20203206-00, E20203373-00 and E20203374-00).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Owing to the use of data for quality improvement as well as the deidentified nature of the data, the institutional review board at the University of Michigan, Ann Arbor, Michigan, USA, deemed this study exempt from approval.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement Data are available on reasonable request. Data belong to the Michigan Surgical Quality Collaborative and are available on reasonable request to Kathy Bishop at the following email address: MSQCCustomerSupport@med.umich.edu.