Placebos in chronic pain: evidence, theory, ethics, and use in clinical practice
BMJ 2020; 370 doi: https://doi.org/10.1136/bmj.m1668 (Published 20 July 2020) Cite this as: BMJ 2020;370:m1668
- Ted J Kaptchuk, professor of medicine1*,
- Christopher C Hemond, assistant professor of neurology2*,
- Franklin G Miller, professor of medical ethics3
- 1Beth Israel Hospital/Harvard Medical School, Boston, MA 02139, USA
- 2University of Massachusetts Medical School, Worcester, MA 01655, USA
- 3Weill Cornell Medicine, New York, NY 10065, USA
- *Contributed equally
- Correspondence to: T J Kaptchuk ted_kaptchuk{at}hms.harvard.edu
ABSTRACT
Despite their ubiquitous presence, placebos and placebo effects retain an ambiguous and unsettling presence in biomedicine. Specifically focused on chronic pain, this review examines the effect of placebo treatment under three distinct frameworks: double blind, deception, and open label honestly prescribed. These specific conditions do not necessarily differentially modify placebo outcomes. Psychological, clinical, and neurological theories of placebo effects are scrutinized. In chronic pain, conscious expectation does not reliably predict placebo effects. A supportive patient-physician relationship may enhance placebo effects. This review highlights “predictive coding” and “bayesian brain” as emerging models derived from computational neurobiology that offer a unified framework to explain the heterogeneous evidence on placebos. These models invert the dogma of the brain as a stimulus driven organ to one in which perception relies heavily on learnt, top down, cortical predictions to infer the source of incoming sensory data. In predictive coding/bayesian brain, both chronic pain (significantly modulated by central sensitization) and its alleviation with placebo treatment are explicated as centrally encoded, mostly non-conscious, bayesian biases. The review then evaluates seven ways in which placebos are used in clinical practice and research and their bioethical implications. In this way, it shows that placebo effects are evidence based, clinically relevant, and potentially ethical tools for relieving chronic pain.
Introduction
Despite their pervasive presence, placebos and placebo effects retain an ambiguous and unsettling presence in biomedicine (see box 1 for definitions).1 Placebos occupy some of biomedicine’s most prestigious terrain: placebo controls in randomized controlled trials (RCTs) are an indispensable tool for rigorous evaluation of pharmaceuticals and procedures. They draw a line in the sand: either treatment shows superiority over placebo or treatment fails. However, patients with subjectively defined symptoms assigned to dummy treatments in RCTs often improve by a magnitude that can sometimes mimic interventions known to be effective. Although such improvement is intriguing, accommodating it scientifically can be challenging. Additionally, placebos have been tainted by associations with deception, trickery, and chicanery.23 Placebos are traditionally caught in a double bind conundrum between beneficial/powerful and unethical/quackery.
Definitions
Placebos are pills composed of inert substances (eg, microcrystalline cellulose) or sham procedures without any direct effect on pathophysiology
Placebo controls are simulated treatments (pills or procedures) designed to appear indistinguishable from the intervention under investigation while lacking the properties thought to be therapeutic
Placebo effects are the salubrious clinical outcomes patients derive from participation in the rituals, symbols, and behaviors of medical treatment. This descriptive definition avoids any premature inference about putative mechanism(s). The definition also avoids the oxymoronic idea of an “inert” substance causing symptom relief
Placebo responses are outcomes detected with placebo controls in randomized controlled trials that include both genuine placebo effects and such non-specific effects as regression to the mean, spontaneous improvement, and normal fluctuations in illness. Placebo responses also accompany most clinical interventions for subjective complaints
Placebo treatment is an inclusive term for different conditions under which placebos can be administered: double blind, deceptively, or honest open label
RETURN TO TEXTRecent shifts in placebo theory and evidence provide an opportunity to reassess the role of placebo effects in medicine. The emergence of a family of interrelated theories and empirical investigations of perception and learning—known as “predictive coding” and “bayesian brain,” developed at the intersection of computational biology, cognitive science, and artificial intelligence—has provided new insights into placebo effects.45678 At the same time, emergent data suggest that the dominant psychological theories of placebos are insufficient in explaining placebo effects in chronic pain.9 Finally, recent research has challenged the axiomatic presumption in biomedicine that eliciting placebo effects requires either deception in clinical practice or concealment in RCTs. In a recent series of small “proof of concept” RCTs with open label placebo (OLP), patients who received placebos subsequently achieved significant symptom relief.10
This review focuses on three primary aspects of placebos in chronic pain (see box 2 for definition and types of pain). Firstly, we examine the effect of placebo treatment in three different conditions: double blind RCTs, deceptive placebo experiments, and OLP. Secondly, we analyze evidence for various psychological and clinical theories of placebo effects. In the context of central sensitization, we argue that “predictive coding” and its corollary “bayesian brain” offer a unified neurobiological framework to elucidate placebo effects in chronic pain. We conclude by examining seven ways in which placebos should or should not be used in clinical and research practice.
Definition and types of pain
The taxonomy of pain remains a matter of debate.11 For the purpose of this review, we adopt modified versions of the definitions provided by the International Association for the Study of Pain, as follows:
Pain—An unpleasant sensory experience associated with actual or potential tissue damage or described in terms of such damage. It is generally described on the basis of its presumed source, although concepts of pain are frequently overlapping
Nociceptive pain—Short lived pain that arises from damage to non-neural tissue and is caused by the activation of nociceptors
Neuropathic pain—Pain caused by a lesion or disease of the somatosensory nervous system
Nociplastic pain—Pain that arises from altered nociception despite no clear evidence of actual tissue damage
Central sensitization—Pain related to sensory amplification, which is experienced as localized somatic or visceral pain but is primarily or exclusively maintained by functional and/or structural neuroplastic changes in the nervous system
Incidence and prevalence of chronic pain
The Institute of Medicine conservatively estimates that at least 100 million American adults—more than the number affected by heart disease, diabetes, and cancer combined—live with chronic pain, costing between $560bn (£448bn; €516bn) and $635bn each year.12 A World Health Organization summary of chronic pain from 10 developed countries and seven developing countries found the prevalence to be 37.3% and 41.7%, respectively.13 The Institute of Medicine reports that the most common type of chronic pain is musculoskeletal pain, especially joint pain from arthritis and back/neck pain. Migraine and severe headaches are also very prominent. Many people with chronic pain have multiple sites of pain (for example, fibromyalgia), and the most common chronic visceral pain condition is irritable bowel syndrome. Chronic low back pain alone is the leading cause of disability in most countries in the world.14
Sources and selection criteria
This review focuses on clinically relevant data derived from patients with chronic pain. Because of distinct characteristics and different underlying pathophysiology of chronic versus acute pain (see discussion below), this review touches on data in acute pain only to contrast with chronic pain. Between March 2019 and July 2019, we searched the PubMed, Cochrane, and Journal of Interdisciplinary Placebo Studies databases. We used dozens of combinations of search terms, such as: placebo effect, placebo response, expectation, conditioning, predictive coding, meta-analyses, and patient-physician relationship. In various combinations, we also searched dozens of keywords relating to somatic and visceral pain, including the conditions listed above in “Incidence and prevalence” but also conditions such as, but not limited to: carpal tunnel, cervical, myofacial, chronic pancreatitis, complex regional, oral facial, neuropathic, post-herpetic neuralgia, non-cardiac chest, endometriosis, interstitial cystitis, vulvodynia, osteoarthritis, and rheumatoid arthritis. These materials were supplemented by the extensive hard copy holdings of the library of the Program in Placebo Studies at Beth Israel Deaconess Medical Center/Harvard Medical School. We prioritized large meta-analyses. For certain sections for which such evidence was lacking, we used smaller meta-analyses or the largest available RCTs. The quality and strength of cited evidence are discussed throughout the paper.
Placebo treatments in different contexts
Placebo treatments can be administered with three distinct informational contexts: binary uncertainty in double blind RCTs, “you may receive the drug or placebo;” certainty in deceptive experiments, “you will now receive a powerful drug;” or honestly as with OLP, “I’m prescribing you a placebo,” which is a kind of paradoxical diffuse “certainty of uncertainty.” The evidence for their effect is presented below.
Uncertainty: placebo responses in RCTs
Discussion of placebo effects in the biomedical literature is predominantly based on outcomes detected in the double blind placebo control group of RCTs testing pharmaceuticals, biologics, devices, and procedures. Such clinical outcomes are best described as “placebo responses,” incorporating “placebo effects” and also encompassing regression to the mean, spontaneous improvement, normal disease fluctuations, known and unknown co-interventions, baseline misclassification, and other artefacts. Such placebo responses also accompany most biomedical (and other non-conventional) treatments for subjective complaints. Without carefully designed no-treatment controls, separating placebo effects from composite placebo responses in RCTs is difficult, if not impossible. We distinguish these two effects throughout this review.
In the past two decades, several RCTs in chronic pain that prospectively investigated placebo effects, as opposed to placebo responses, using carefully designed no-treatment controls, have shown significant and clinically meaningful placebo effects embedded within larger placebo responses.3 Studies with such no-treatment controls will be noted throughout this review. Despite being incapable of separating placebo response from placebo effects, most data from pharmaceutical RCTs provide accurate estimates of the magnitude of responses to placebo treatments in concealed or “uncertain” circumstances. Table 1 summarizes large meta-analyses of studies involving at least 400 patients that aggregate placebo responses for various chronic pain conditions. Overall, table 1 shows that placebo responses are pervasive, with effects that are sometimes large but generally modest to moderate.
Placebo responses in large meta-analyses of randomized controlled trials (RCTs) in pain conditions
Another approach to examining placebo responses in RCTs is to calculate the percentage of the observed pharmaceutical responses that can be attributed to placebo responses. Figure 1, based on an illustration appearing in one of the largest meta-analyses on osteoarthritis (n=41 391),31 shows that placebo response (here called “contextual” effect) can account for about 75% of responses to drugs commonly used in osteoarthritis. Several other studies in table 1 report similar findings whereby placebo responses make up between 50% and 75% of drug responses.

Overall treatment effect and proportion attributable to contextual effect for pain in osteoarthritis. CS=chondroitin sulfate; GS=glucosamine sulfate; IACS=intra-articular corticosteroid; IAHA=intra-articular hyaluronic acid; NSAID=non-steroidal anti-inflammatory drug; PEMF=pulsed electromagnetic filed therapy. Adapted from Zou et al, 201631
{kind=link}
Supporting these kinds of data on placebo responses, a US Food and Drug Administration report that included data from unpublished as well as published RCTs found that studies of analgesics are among the most common classes of pharmaceutical studies that routinely lack assay sensitivity and that such drugs “are often indistinguishable from placebo in well designed and well conducted trials.”35
Certainty: placebos with deception
To what extent does concealed administration of placebo in RCTs differ from placebos administered under circumstances in which placebos are given under the guise that they are medications (that is, certainty)? In a related question, how are pharmaceutical outcomes modulated under such different informational presentations regarding degrees of confidence/certainty? Unfortunately, data to answer these important questions remain scarce. To our knowledge, only three small RCTs in pain conditions have prospectively compared concealed placebo (and/or concealed drug) versus placebo/drugs prescribed with certainty, two of which are in acute pain only. Table 2 summarizes these three trials. Although these limited data are insufficient to make definitive conclusions, the two larger studies report that deception/certainty placebo is either no different from or inferior to double blind/uncertainty placebo.
Double blind treatments versus certainty of receiving treatments
Another stream of placebo research seeks to determine whether raising the degrees of confidence (certainty) of receiving medication in RCTs (that is, being randomly assigned to active treatment versus placebo with ratios from 1:1 up to 4:1) evokes higher placebo responses. Evidence from four large meta-analyses of knee osteoarthritis (149 RCTs; n=39 814),39 one in diverse types of osteoarthritis (215 RCTs; n=41 391),31 and one in irritable bowel syndrome (73 RCTs; n=8264)25 found no such effect. A meta-analysis of diverse chronic pain conditions (9 RCTs; n=2017) found a negative correlation: a greater likelihood of receiving medication led to significantly lower placebo responses.22 In chronic pain, more confidence in receiving medication seems not to lead to higher placebo responses.
Placebos with “certainty of uncertainty”: open label placebo
An emergent category of placebo investigation and treatment is open label, honestly prescribed placebo. A summary of OLP clinical studies in a range of conditions including pain and non-pain conditions—discussing both strengths and weaknesses—has been reported elsewhere910; table 3 summarizes evidence drawn exclusively from the subset of OLP trials in chronic pain. Patients are told that placebo treatments in RCTs can elicit positive responses in double blind studies, but that whether placebos “work” when patients are aware of receiving placebo is unknown. If evidence exists from previous OLP RCTs, this information is conveyed with an explanation that replication is needed to verify earlier findings. Researchers emphasize honesty and never say “it will work;” they rather say, “let’s see what happens.”45 When patients express their skepticism about treatment with “sugar pills” (or microcrystalline cellulose), which happens frequently, researchers support patients by expressing their own genuine doubts and puzzlement.45 Patients in OLP trials are generally receiving stable routine or optimal medical care before recruitment, yet their symptomatic improvement in the trial is commonly more than 50% greater than that of patients in “no additional treatment” controls. Nevertheless, the small sample sizes and short duration of these trials preclude drawing strong conclusions. Even so, OLP RCTs provide valuable proof of concept data suggesting that concealment and deception are not needed to elicit placebo effects. These trials, given their no-treatment controls, also provide evidence that placebo effects constitute more than spontaneous improvement. Comparisons of double blind placebo with OLP would be illuminating. We are unaware of any published direct comparison of double blind placebo treatment and OLP, although at least one study is under way.45
Open label placebo randomized controlled trials in chronic pain conditions
Evidence for theories of placebo effects
The three main prevailing explanatory domains used to explain placebo effects—traditional psychological theory (for example, expectation and conditioning), patient-physician relationship, and neurocomputational theories—are summarized below. Although these categories can overlap, we have separated them to facilitate clarity and respect what are often very distinct research trajectories.
Traditional psychological theories
Expectation
Expectation, the dominant theory of placebo effects in the literature, posits that positive conscious expectations (for example, pain reduction) in medical encounters will cause beneficial outcomes.4647 This notion of self-fulfilling prophecy is generally thought to be conscious and conceptual and to involve anticipation of probable benefit.48
Most research on placebo expectation has involved healthy people; in the past 20 years, at least 80% of publications on placebo have involved volunteers (often university students) in laboratory studies of experimentally induced pain, mostly exploring how deceptive expectations modulate placebo or pharmaceutical effects.49 These experiments generally show that placebos with positive expectation reduce calibrated nociceptive pain in timeframes typically measured in seconds, minutes, or, very rarely, hours.
These outcomes are more reproducible if people are first given an unimpeachable experience of placebo effects by surreptitiously lowering the calibrated pain when they receive placebo for the first time. However, acute pain in healthy participants is not an appropriate surrogate for chronic pain, given that patients with chronic pain are characterized by significant changes in their underlying neuroanatomical structural volumes as well as functional brain connectivity.505152 Furthermore, placebo treatments in chronic pain engage neurotransmitters that are distinct from those engaged by acute pain experienced in the laboratory.53 Nevertheless, acute pain experiments provide important proof of concept findings elucidating placebo effects.
When these experiments include various neurotransmitter antagonists or neuroimaging technology, they have also shown potential neurotransmitters and brain activations underlying acute pain, which may or may not apply to chronic pain (see below). In the predictive coding/bayesian brain section of the review, we will contend that such expectation effects are compatible with and explainable from predictive coding/bayesian brain perspectives.67
Owing, at least in part, to ethical difficulties involving deception in patient populations, few direct research data exist on how positive or enhanced expectation might modulate chronic pain over time. One common surrogate marker is to examine correlations between measured baseline expectations and outcomes in RCTs. RCTs of acupuncture furnish the largest and most concerted and deliberate effort testing this hypothesis. Given that large RCTs of acupuncture often include a third arm with no treatment, they can also provide more precise estimates of placebo effects distinct from placebo responses.
A systematic review of all acupuncture trials testing the effect of expectation (n=58 RCTs, nearly half in pain) found no consistent association between baseline expectations and subsequent pain relief.54Table 4 summarizes the findings of the four largest RCTs in chronic pain hypothesizing that baseline expectations predict outcomes. Again, inconsistency dominates the picture.
Largest studies examining baseline expectation and correlation with placebo effects
In other types of chronic pain, results of RCTs are similarly equivocal.9 Large observational studies are also consistent with this. For example, to our knowledge, the largest baseline expectation study is a systematic review of observational studies in patients undergoing total knee and total hip arthroplasty (18 studies; n=7455); it found “no consistency in association between patients’ pre-operative expectations and outcomes.”60
The existence of non-conscious expectation effects further complicates expectation theory. In multiple neuroimaging experiments, participants were exposed to placebo cues on a timeframe of 12 milliseconds; these cues produced placebo effects and activated brain regions that are similar to those engaged with “conscious” cues.616263646566 Additionally, two earlier RCTs on postoperative pain after third molar extractions showed that medical and nursing behaviors outside of the conscious awareness of patients can elicit placebo effects.6768 Separating conscious and non-conscious components of placebo effects outside of laboratory experiments remains a challenge. To what extent such non-conscious processes underlie conscious expectation remains unknown.
A series of qualitative interviews embedded in RCTs in irritable bowel syndrome,69 chronic low back pain,56 and chronic temporomandibular disorder70 further disrupts a conscious expectation theory. In interviews performed by anthropologists, patients overwhelmingly denied positive expectations and instead described a history of repeated therapeutic failures.69 Patients spontaneously brought up “hope,” a concept that seems to embody a tragic-optimistic stance intimately connected to despair. Hope seems to be a complex process connected with uncertainty, patience, forbearance, tolerance, and honesty; it also involves affect, cognitive reflection, and prospection, as well as cultural rules of what is reasonable when one looks into the future.97172Although a more complex construct than expectation, we hypothesize that, even if it could be effectively measured, hope would also have poor reliability for predicting placebo effects; hope may be necessary for placebo effects but insufficient to causally elicit them.
Conditioning
Classical conditioning is the second most discussed psychological model for understanding placebo effects.47 Classical conditioning describes how, after initial pairing of unconditioned stimulus (for example, an opioid) with a conditioned stimulus (for example, saline injection), subsequent conditioned stimuli alone evoke pain relief, albeit often of reduced magnitude.73 Apart from situations with deliberate pairing of unconditioned and conditioned stimuli, it seems unlikely that classical conditioning is involved in chronic pain placebo effects because, in most cases, patients’ previous experiences with pain treatment have been unsuccessful, especially when they enroll in RCTs. Nevertheless, conditioning has given rise to proposals for various techniques of “dose extension” or “partial reinforcement,” whereby powerful drugs such as opioids or other potent medications are initially paired with placebo vehicles and then interspersed with placebos, with the intention of reducing the dosages of medication needed.7475 We are unaware of any such experiment in chronic pain, but proof of concept studies exist in non-pain conditions.76777879 Clearly, this technique deserves investigation in chronic pain.
Clinical theories of placebo effects
Clinical theories of placebo do not focus on single psychological, social, or behavioral factors but rather incorporate many possible components of therapeutic encounters. The two most important such approaches are described below.
Patient-physician relationship
The clinical encounter is a complex assemblage of explicit behaviors (such as attention, warmth, focused touch, validation, empathic witnessing, diagnostic procedures, diagnosis itself, acts of kindness) and embodied and implicit, but not necessarily conscious, non-verbal cues (such as voice, facial, eye, and bodily expressiveness, non-focused touch, style of conversation, proximity relations, presence).80 Other aspects of the relationship, such as trust and competence, are even harder to categorize. Designing reproducible and rigorous RCTs to examine the therapeutic effects of the clinical encounter is challenging because of difficulties in keeping known and unknown active ingredients constant. Nevertheless, patient-clinician engagement has been correlated with patients’ satisfaction, adherence, and perceptions of healthcare quality in various conditions.818283 RCTs investigating whether clinical relationships can enhance placebo or drug effects in chronic pain are sparse. Again, acupuncture and/or sham acupuncture research is a frequently used medium of investigation. The four largest such RCTs offer reasonable positive support for the therapeutic benefit of the patient-physician relationship, notwithstanding some inconsistency. Table 5 summarizes the results.
Randomized controlled trials of patient-physician relationship and placebo effects
Medical ritual
“Medical ritual” is a term used in anthropology to describe the patterns of more or less invariant sequences of embodied behaviors, potent symbols, and cultural narratives involved in non-biomedical healing practices.8788 It overlaps with patient-physician behaviors as described above but is more expansive by including evocative symbols (such as paraphernalia, costumes, and healing spaces), embodied behaviors (such as diagnostic procedures and treatment protocols) that connect to “potent” cultural beliefs, and participation in socially appropriate activity (such as visiting healers or adopting a sick role). Anthropology often adopts an idea of “embodied cognition” that claims that the physical body including the motor system can shape cognition.89909192 No direct evidence shows that embodied cognition directly influences placebo effects.9 Recently, some medical researchers have adopted the nomenclature “ritual” as a descriptive-behavioral term for the amalgam of all that happens in clinical encounters apart from any purported active pharmacological/physiological ingredient(s).
Sometimes the term “ritual” is used more narrowly to indicate the route of administration of placebo treatment (for example, fake surgery, sham device, placebo pill, or inactive cream). Variations in magnitude of placebo effects/responses among different placebo procedures (distinct placebo “rituals”) provide valuable data on the plasticity of placebo effects.93 Furthermore, route of administration may help to explain the seemingly high placebo responses in placebo controlled surgery trials.94 To our knowledge, four meta-analyses directly compare placebo responses in chronic pain by different methods of delivery. Table 6 summarizes these meta-analyses and suggests that more elaborate rituals are superior to simpler rituals in relief of chronic pain.
Meta-analyses comparing types of placebos and pain responses
Central sensitization, predictive coding, and bayesian brain
Central sensitization and nociplastic pain
For the purpose of this review, in chronic pain, predictive coding/bayesian brain is most easily understood from the perspective of central sensitization or its overlapping conceptual description as nociplastic pain. Central sensitization is the family of phenomena wherein signal amplification occurs at one or more levels of the sensory pain processing hierarchy. It causes “bottom-up” stimuli to be exaggerated and occurs not only in the wake of tissue damage but also with minimal impairment or even in the absence of any clear pathophysiology or injury.
In the 1980s, on the basis of animal models, central sensitization was described as a physiological phenomenon that was localized to the peripheral neurons and spinal cord.9697 Subsequent human neuroimaging experiments have shown that this amplification/sensitization process can occur in hierarchically higher structures, including the brainstem and the thalamic, insular, and/or somatosensory cortices, blurring the lines of neurobiological definition.9899 Maladaptive changes in high level cortical areas of sensory and interoceptive representation or the brainstem may create an independent, automatic “top-down,” non-conscious bias toward interpreting otherwise benign sensory data as painful.5195100101102103104105106
Central sensitization helps to explain the common disjunction between objective pathological findings and patients’ experiences of chronic pain. It is now thought to be important in most chronic pain conditions, including those with ongoing nociceptive input (neuropathic pain such as diabetic peripheral neuropathy) and those without such input (nociplastic pain such as fibromyalgia); the National Institutes of Health now collectively refers to such diverse conditions as chronic overlapping pain conditions.107108
Predictive coding and bayesian brain
Predictive coding theory is a computational neurobiological model that offers an inclusive explanation for experimental findings in central sensitization, acute and chronic pain, and placebo modulation of pain perception.678109 In this theory, the brain continuously and non-consciously streams cortically generated, top-down, feed-forward hypotheses/predictions about incoming afferent bottom-up data.45110111 The driving bottom-up sensory signal provides corrective feedback on the top-down predictions.4 The brain is interested in “prediction errors,” which are discrepancies or mismatches between these two data streams.
Prediction errors must be resolved in one of three ways. Firstly, these discrepancies can be used to update the prediction model, mostly non-consciously, in an effort to increase the accuracy of future predictions.4 Secondly, prediction errors can be suppressed through attenuation of sensory input. Thirdly, the sensory signal can be amplified to meet the prediction. On a millisecond time scale, the brain, mostly non-consciously, calculates how much weight should be assigned to a sensory signal. How much should a bottom-up signal weaken, modulate, or override the prediction? Or should the prediction override the signal? Prioritizing errors that deviate from relatively stable predictions allows the brain not to be overwhelmed by a barrage of incoming peripheral sensory information and instead focus on “the difference that makes a difference.”112
Prediction errors must be minimized to avoid ongoing chaos and disorganization of information processing.113 This constant interaction/updating of top-down and bottom-up implies that predictions and sensory signals are mutually embedded, inseparable, and inextricably linked. At some level of explanation, one could say that prediction is already coded at the very instant of perceived sensory information. The brain is active and not simply stimulus driven, and it behaves as a “statistical organ that actively generates explanations from the stimuli it encounters, in terms of hypotheses that are tested against sensory evidence (predictions); ‘hypotheses’ and ‘beliefs’ should in this context be understood not as consciously held mental states but as neural encoded probability distributions (that is, bayesian belief, priors) that are tested against sensory evidence (posteriors).”111
Theories of predictive coding have compelling and widely accepted empirical scientific validation in the visual and auditory systems.113114 Evidence for involvement of predictive coding in acute pain perception and placebo analgesia is accumulating from experimental and clinical data,78103110 as well as statistical modeling experiments.115116
Predictive coding is underwritten by Bayes’ theorem, meaning that new afferent data are probabilistically weighted and interpreted in the context of the model, to provide the best estimated output under conditions of uncertainty.117118119 Conceptually simplified, the two core elements comprising a bayesian probability computation are the bottom-up (bayesian language: likelihood function) sensory inputs, and the top-down (bayesian: prior) probability, computed together to yield a proportional output, the (bayesian: posterior) perceptual inference. Bayesian systems represent signals or parameters as probability density functions defined by a statistical mean representing the prediction and a value of precision, also called inverse variance or noise (fig 2).118 Importantly, perceptual processes can be highly biased toward either top-down or bottom-up signaling on the basis of the relative “precision weights” afforded to these inputs, a process thought to be related in part to dopaminergic attentional mechanisms.120

Bayesian statistics operate on the basis of input probability density functions containing both a mean value and a precision (inverse variance or noise)
{kind=link}
Predictive coding and placebo (expectation) treatment in acute pain
An acute pain model of predictive coding/bayesian brain is easier to understand and will provide a helpful contrast to the chronic predictive coding/bayesian brain model to be described just below. Given that healthy volunteers have no previous exposure (for example, top-down predictions) to the experimental calibrated pain, when they receive a pain stimulus or injury this nociceptive signal is combined with the (lack of) prediction to yield an unambiguous pain perception that cleanly matches the sensory signal (fig 3).6 As discussed earlier, in acute placebo experiments, healthy volunteers are verbally told that placebos will lower their pain or, more effectively, receive direct experience of “placebos” disguised as “powerful drugs” by surreptitiously lowering the calibrated pain when they are first exposed to placebo treatments. Such manipulations create new top-down predictions (expectations) of hypoalgesia. When these predictions of hypoalgesia are combined with experimentally calibrated pain sensations, they yield a bayesian perception/experience of short term pain reduction (fig 4).7110115 A negative (nocebo) placebo effect could be similarly created through conscious expectation of pain greater than the actual stimulus.

Healthy normal bayesian perceptual model of acute pain perception. This is characterized by a lack of prior pain prediction (orange), yielding congruence between the sensory signal (blue) and perception (green). VAS=visual analog scale
{kind=link}

Placebo hypoalgesia of acute experimental pain can be modulated in healthy people via a temporary expectation-prediction lower in intensity than the painful stimulus. VAS=visual analog scale
{kind=link}
Evidence also strongly suggests that placebo treatments are unlikely to directly modulate bottom-up sensory signals, but rather are influencing high level top-down processes.121 Therefore, predictive coding/bayesian brain contends that in acute pain, placebos can influence pain perception through the induction of top-down expectations of pain, transiently biasing the bayesian computation toward this prediction. Thus, in acute experimental pain in healthy nervous systems, placebo effects are dependent on the creation of a transient, mostly conscious prior prediction (expectation) of hypoalgesia.7110115 Recent evidence with healthy volunteers also shows that these transient expectations can become embedded and resistant to extinction via suppression of prediction errors via the prefrontal cortex.122
Predictive coding and placebo treatment in chronic pain
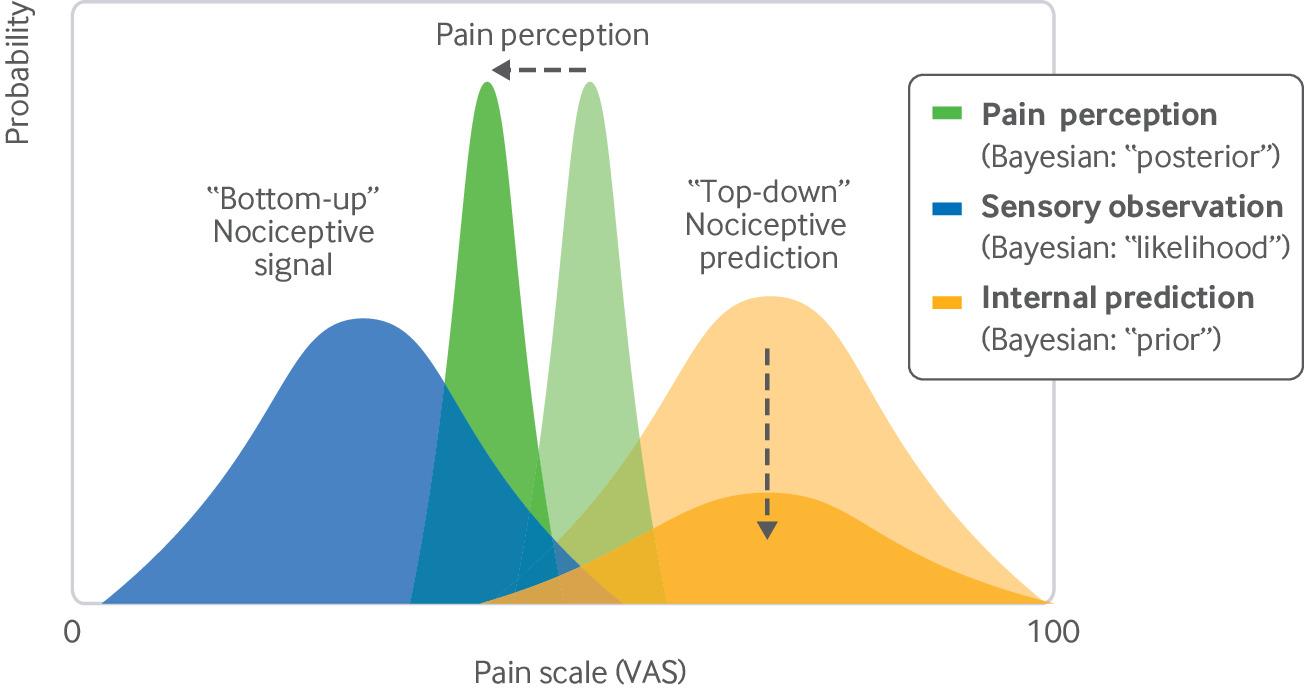
Patients with chronic pain are physiologically different from healthy people. Chronic pain is accompanied by changes in structural and functional architecture in the sensory and limbic processing pathways. Predictive coding/bayesian brain posits that central sensitization amplifies and shifts the top-down predictions such that the brain may now continuously bias sensory data toward painful perception,69104105123124 as depicted in figure 5. These “painful predictions” could be perpetuated by diminishing bottom-up sensory precision weighing so as to reduce prediction errors. This situation could be analogized as a chronic negative placebo (nocebo) effect. For example, in many chronic pain conditions, the injury has already begun to heal biologically but the brain dismisses or interprets healing signals as “mere ‘noise’ and adheres to a hypothesis of ongoing pain.”6 This process helps to explain the low correlation often found between objective pathophysiology and subjective experience.6 This maladaptive positive feedback loop relies on internal top-down predictions that are now relatively divorced from sensory feedback (fig 5). Because of these pathophysiological differences, not surprisingly, evidence suggests that the “chronic pain brain,” compared with the brains of healthy volunteers in acute pain experiments, also responds to placebos through a different set of neurotransmitters and neuroanatomical substrates.5053125

Bayesian account of chronic pain, characterized by up regulated prior (orange) prediction of incoming sensory (blue) signals. The bayesian summation of these two signals yields a perception in between the two. VAS=visual analog scale
{kind=link}
Most patients with chronic pain have not responded to previous treatment; this is especially true of those joining RCTs.69 These patients have often seen multiple practitioners and generally talk about “hope,” a tragic optimism linked to despair, frustration, and uncertainty. Such patients have already had a high dose of therapeutic failure. From a bayesian standpoint, a novel therapeutic intervention in chronic pain necessarily and automatically injects new uncertainty and imprecision into the top-down predictions. A proffered medical treatment presents a situation of “can happen” and creates opportunities to recalibrate entrenched aberrant predictive precision and therefore potentially shift the bayesian computation of pain perception, as depicted in figure 6. At their essence, placebo effects in chronic pain are best conceptualized as modifications of bayesian predictions/biases. Note that our hypothesis would not exclude other previously described psychological mechanisms of pain relief, including reassurance, decreased catastrophizing, increased emotional regulation, change in motivational state, conditioning “dose extension,” or even an effect of a non-conscious expectation, which are forms of high level predictions as well.104126 Although conscious expectations do not seem to play a role in mediating placebo effects in chronic pain, non-conscious predictive processes, such as those potentially subserving medical ritual, physician-patient relationships, and conditioning “dose extension,” could also alter bayesian priors without affecting precision, via shifting predictions toward a less painful state, as illustrated in figure 7.
Placebo effects in chronic pain. Hypoalgesia can be achieved through decreased precision (eg, increased uncertainty) of the (high level) prior, a mechanism that would not rely on expectation. VAS=visual analog scale
{kind=link}

Placebo effects in chronic pain. Hypoalgesia could also be achieved by shifting top-down predictions to more benign intensities, while maintaining similar precision. VAS=visual analog scale
{kind=link}
OLP trials explicitly provide a simple demonstration of how placebos may weaken and decrease the precision of top-down predictions through the explicit accentuation of patients’ uncertainty in the context of a paradoxical if not implausible intervention (fig 6). The entire encounter has inescapable uncertainty: “placebos are substances that have no active ingredients; maybe they can help you—let’s see what happens.” The main difference between OLP and concealed placebo in a double blind RCT is the manner in which each frames the inherent uncertainty of treatment; OLP’s uncertainty is more radical and diffuse than that of double blind placebo. In either treatment context, when patients inhabit the rituals and drama ingrained in the care of chronic pain, including the conscious and non-conscious knowledge of the possibility of relief, complex and subtle healing cues seem to be simultaneously and constantly interpreted, felt, and experienced. For some patients, some of the time, the brain’s high level prediction, “I am in pain,” is automatically challenged and weakened.
Importantly, a predictive coding/bayesian brain account of chronic pain and placebo is compatible with and empirically supported by a set of preliminary observations in multiple RCTs: patients with chronic pain who report higher within person baseline variability have higher responses to placebo treatment. Although conclusions are premature, and further confirmations are necessary, such evidence is notable given the inability, to date, to find reliable predictors of placebo responses. A summary of chronic pain studies that included this assessment can be found in table 7.
Baseline variability and placebo responses
From a predictive coding/bayesian brain perspective, this baseline variability seems to be equivalent to the amount of “noise,” “uncertainty,” or “instability” within the pain perceptual system. To explain these findings, prediction coding/bayesian brain theory draws from machine learning and artificial intelligence. Artificial learning systems may get “stuck” at a non-optimal solution (“local minimum”) during bayesian inferential learning processes. In these cases, an algorithm can benefit from the addition of (stochastic) randomness (“noise”) or resetting (“reconsideration”) of optimization parameters. In other words, variability, imprecision, and noise can sometimes create opportunities for improved bayesian inferences; strong, “stuck,” “top-down” predictions can be undermined with the creation of uncertainty. In accordance with predictive coding/bayesian brain theory, this machine learning perspective provides an intriguing explanation for how stochastic imprecision/randomness/noise can counterintuitively eliminate suboptimal predictions.132133
Further supporting this theory, recent evidence suggests that the source of this perceptual variance in patients with chronic pain may localize to the sensory afferent system. One study randomized patients (n=61) with painful diabetic neuropathy to training in the laboratory designed to allow for accurate rating of evoked pain (increase precision of pain perception) or no training. Both groups were subsequently randomized to either pregabalin or placebo. Patients without sensory precision training had significantly higher placebo responses.134 A subsequent replication study in patients with knee osteoarthritis (n=55) found analogous results.135
Such sensory training involves learning to experience sensory bottom-up sensations with increased precision—a bottom-up mechanism inherently connected to that of placebo through bayesian computation. Rather than decreasing top-down central sensitization directly through the introduction of uncertainty/imprecision, sensory training explicitly increases, via attentional mechanisms, the precision/certainty of the bottom-up sensory signal; this increased the precision of the sensory signal and creates new prediction errors, and it may ultimately force revision and normalization of the overly precise predictions and consequently decrease placebo effects. In chronic pain, decreased precision of sensory input is associated with increased placebo effects. It seems that, “somatosensory experiences that are ambiguous are more malleable to … [top-down predictions] than experiences with clear perceptual characteristics.”119136137
Summary
A summary of this complex, though still simplified, section on predictive coding/bayesian brain may be helpful. Placebo treatments have little influence on bottom-up objective trauma and pathophysiology.123138 Placebos do not directly release nerve entrapments; they modulate how the pain is experiences and perceived. Clinical engagement including actual treatment—whether with placebos or effective medication—automatically triggers neurocomputational re-evaluation of predictions embedded in functional and structural (mal)adaptions of the nervous system (that is, central sensitization/nociplastic revisions), allowing for the possibility for automatic symptom de-amplification. In patients with chronic pain, conscious positive beliefs about treatments will probably not enhance outcomes, but we hypothesize that patients may benefit from awareness that new circumstances could potentially bring possibilities of relief—that is, have something called “hope” within a therapeutic context. The immersion in medical rituals itself alleviates pain in some patients some of the time. This process is automatic and involves little conscious agency. Predictive coding/bayesian brain offers a unified neurobiological construct to interpret placebo evidence.
Practice, ethics, and guidelines
In this section, we review seven ways in which placebos are used in clinical practice and research in light of biomedical perspectives and formal medical guidelines.
Placebo responses in clinical practice
Most commonly, placebo responses arise in clinical practice as a component of prescribed pharmaceuticals or procedures. Evidence from RCTs, summarized earlier in figure 1, clearly shows that placebo responses contribute to the observed responses. For some conditions, most of observed benefit associated with drugs is attributable to placebo responses (including placebo effects) (table 1). How can clinicians promote placebo effects? Reasonable evidence suggests that patient centered care augments placebo effects in chronic pain (table 5). Unfortunately, we have seen no RCT evidence that upgrading the quality of the relationship improves clinical outcomes connected with effective drugs or procedures in a chronic pain RCT. The largest and most important test of clinician augmentation involved a chronic non-pain condition (asthma; n=601), using an elaborate 2×2+1 (placebogenic interaction versus neutral interactions crossed over to medication (a leukotriene antagonist) versus placebo + no-treatment control) design. This study found that enhanced interaction boosted the placebo intervention only on the subjective outcome of symptomatic improvement and not on the objective forced expiratory volume, and it had no effect on medication for either measure.139 Rigorous studies of clinical augmentation of therapeutic benefit of drugs would be desirable for chronic pain. Ethically speaking, however, developing an optimal patient centered relationship is important regardless of whether it improves clinical outcomes. Patient centered relationships based on trust, concern, and acts of kindness are an ethical imperative whether or not they heighten the therapeutic effect of pharmaceuticals.
Placebo treatment
Survey research provides strong evidence that deceptively administering placebo pills and saline injections—as if they were medications—has become rare in medical practice (<4% of US physicians; higher in other countries).140141142 No ethical rationale exists for administering such deceptive “pure” placebos.
“Impure” placebo treatment
“Impure” placebo refers to the practice of physicians prescribing drugs or supplements that they know (or suspect) have no effect on patients’ pathophysiological condition (for example, sub-therapeutic doses of phenytoin for chronic pain or magnesium for chronic headaches).143 A US national randomized survey found that more than 50% of 1200 internists and rheumatologists reported regularly prescribing such impure placebos.140 Other surveys in Europe have found similar or higher rates.141142144 The practice seems to be widespread in chronic pain conditions.144 However, prescribing impure placebos is ethically problematic because it, at least, seems to transgress ethical norms of transparency and informed consent regarding the nature and rationale of prescribed treatment.
Placebo treatment for diagnostics
Physicians sometimes administer placebo treatments as diagnostic tools. For example, placebo injections are sometimes used to determine whether patients qualify for denervation of the zygapophyseal joints; if they respond to placebos, they are often denied the real treatment.145 More generally, the practice involves determining whether pain is “psychogenic” or “greatly exaggerated.”146 One recent systematic review found that the rates of physicians/nurses in a lifetime of work using placebo diagnostic procedures pre-2000 versus post-2000 have shrunk sharply (from between 60% and 97% to between 4% and 37%).144 A consensus exists in most professional organizations that use of placebo diagnostics is unethical without informed consent and generally “does not provide any useful information about the genesis or severity of pain.”146
Open label placebo treatment
If research in OLP continues to be positive (table 3), OLP has the potential to become an ethical option in clinical practice. This is important in so far as OLP adds meaningful benefits beyond usual or even optimal biomedical care (most studies added OLP to ongoing stable regimens), given that patients in OLP RCTs generally are refractory and have a lengthy history with multiple physicians and allied health providers.69
In terms of ethical analysis, OLP adheres to ethical norms of transparency, respect for persons, and informed consent.147 The American Medical Association’s code of ethics stipulates that placebo treatment is allowed when physicians “obtain the patient’s general consent,”148 suggesting that no ethical barrier to OLP exists. (In the UK, the General Medical Council has no explicit guidelines on placebos.)
Importantly, evidence from surveys and focus groups suggests that patients are willing to try OLP. For example, a survey of US patients (n=853) indicated that 62% of patients would probably or definitely take OLP in the context of a recommendation by a doctor.149 This finding was replicated in a focus group in the UK (n=58).150 No data are available on physicians’ attitudes, and we speculate that OLP may not be as acceptable for physicians whose professional identify is connected with offering interventions that are known to be effective by virtue of their pharmacological or physiological properties.
Placebo controls in clinical research
Double blind, concealed placebos are indispensable methodological tools in RCTs. OLP is not a substitute. Besides controlling for placebo effects, placebo arms in RCTs also prevent confounding from potential biases involving allocation, attention, detection, performance, and attrition.151152153 Although some concern exists about denying patients the benefits of treatments already deemed effective,154 placebos are generally accepted as being ethical with informed consent in cases in which potential harm to patients from delayed treatment is minor.155 Use of sham invasive procedures as control interventions is also ethically justifiable when they are methodologically necessary to produce valid results and the risks from the sham procedure are not excessive.156 One serious ethical problem with RCTs, as currently practiced, is that participants often do not receive accurate and transparent descriptions of potential benefits and harms (nocebo effects) detected in previous placebo arms of RCTs for their condition.157
Placebo controls in laboratory experiments
Laboratory studies aimed at elucidating the nature and mechanisms of placebo effects still typically use deception. These experiments remain especially important for neuroimaging of placebo effects on acute nociceptive pain.158 To promote respect for persons in deceptive placebo research, we advocate the use of “authorized deception.” Prospective participants are informed that aspects of the research are not being described accurately and that they will receive a full account during a debriefing after participation in the study and given an opportunity to withdraw their data during this process.159 An RCT investigating authorized deception randomly assigned healthy volunteers to a deceptive placebo intervention in an experiment involving experimental pain with either an authorized deception disclosure or a standard deceptive disclosure; no difference was observed.160 (One of the authors (TJK) has adopted authorized deception for hundreds of patients and has never had a single person withdraw data.)
Conclusion
Placebo responses in chronic pain are pervasive. Although placebo responses in RCTs occasionally produce large effects, on average they provide modest to moderate changes that are nevertheless clinically meaningful. The patient-physician relationship can augment outcomes of placebo treatments. OLP studies are provocative. Placebo effects in chronic pain can be understood as non-conscious bayesian prediction processes engaged by non-conscious and conscious informational cues that arise when patients participate in the rituals and behaviors of medicine. Just as chronic pain involves important components of central sensitization or sensory biases, in a parallel reverse fashion, placebo effects involve sensory biases in the opposite direction. Importantly, our model is provisional and inevitably will need correction as scientific discovery advances. Medicine should abandon its historic denigration of placebo effects and consider accepting them as an intrinsic and valuable component of clinical care. More research is needed to understand how clinicians can optimally and ethically use placebo effects to alleviate pain.
How patients were involved in the creation of this article
We invited four patients—one participating in an ongoing double blind randomized controlled trial (RCT) in chronic pain, one who had completed an open label placebo (OLP) RCT, and two in routine clinical care—to review an advance version of this review. We asked them to read the manuscript in its entirety and to focus especially on sections that were most relevant to their experiences. Their input helped us to add patients’ perspectives in the sections on patient-physician relationship, double blind RCTs, and OLP RCTs. All four patients urged us to continue in our research efforts to understand how placebo effects could be helpful in the treatment of pain. Importantly, the original impetus for this “rethinking placebos” review originally came from exit interviews with patients in RCTs performed by one of the authors (TJK) and from the anthropological patient interview research cited in this paper.
Questions for future research
Patient-physician relationship
Does the patient-physician relationship affect medical outcomes associated with effective drugs and procedures?
If so, what are the key ingredients of this relationship?
Can physicians acquire them through training?
What is the relative importance of clinical outcomes, patient satisfaction, medicolegal factors, fiscal concerns, bureaucratic demands, and ethical duty for adoption of high quality patient-physician engagement?
Open label placebo
Will the results of small, proof of concept trials be replicated in larger and longer duration randomized controlled trials in specific conditions?
If so, what are best practices and circumstances for optimal utilization?
Conditioning placebo paradigms
Can placebo conditioning paradigms that intersperse active ingredients (unconditioned stimuli) with inert pills (conditioned stimuli) be used to lower dosages of powerful analgesics without reducing pain relief?
Predictive coding/bayesian brain
What are the neuroanatomical (or functional network level) substrates of the hypothesized, up regulated bayesian (prior) predictions of pain?
Can the predictive coding/bayesian brain hypotheses be tested quantitatively using calibrated sensory stimuli (bayesian: likelihood), functional magnetic resonance imaging readouts of neural activity (bayesian: prior), and patient reported pain perception (bayesian: posterior)?
Acknowledgments
We thank Gabriel Kaptchuk, Liron Rozenkrantz, Karin Jensen, Kathryn Hall, Adriane Fugh-Berman, Sarah Ballou, and Deborah Grose for feedback on the manuscript.
Footnotes
Series explanation: State of the Art Reviews are commissioned on the basis of their relevance to academics and specialists in the US and internationally. For this reason they are written predominantly by US authors
Contributors: All authors contributed and provided input to the entire manuscript. TJK drafted the first outline of the manuscript, did primary literature reviews, and provided the first draft of the sections on different types of placebo interventions and evidence/theory. CCH wrote the first draft of the predictive coding/bayesian brain portion of the manuscript. FGM wrote the first draft of the practice and ethics section. All authors reviewed all sections of the manuscript, engaged in interactive discussions, and made suggestion for content and references. TJK is the guarantor.
Funding: TJK is partially funded by NIH/NCCIH grants #R01AT008573 and #R61/33AT009306 and the Foundation for the Science of the Therapeutic Encounter.
Competing interests: We have read and understood the BMJ policy on declaration of interests and declare the following interests: none.
Provenance and peer review: Commissioned; externally peer reviewed.