Article Text

Abstract
Objective It is uncertain whether persons with chronic widespread pain (CWP) experience premature mortality. Using the largest study conducted, we determine whether such a relationship exists, estimate its magnitude and establish what factors mediate any relationship.
Methods UK Biobank, a cohort study of 0.5 million people aged 40–69 years, recruited throughout Great Britain in 2006–2010. Participants reporting ‘pain all over the body’ for >3 months were compared with persons without chronic pain. Information on death (with cause) was available until mid-2015. We incorporated these results in a meta-analysis with other published reports to calculate a pooled estimate of excess risk.
Results 7130 participants reported CWP and they experienced excess mortality (mortality risk ratio 2.43, 95%CI 2.17 to 2.72). Specific causes of death in excess were cancer (1.73adjusted age and sex, 95% CI 1.46 to 2.05), cardiovascular (3.24adjusted age and sex, 95% CI 2.55 to 4.11), respiratory (5.66adjusted age and sex, 95% CI 4.00 to 8.03) and other disease-related causes (4.04adjusted age and sex, 95% CI 3.05 to 5.34). Excess risk was substantially reduced after adjustment for low levels of physical activity, high body mass index, poor quality diet and smoking. In meta-analysis, all studies showed significant excess all-cause (combined estimate 1.59 (95% CI 1.05 to 2.42)), cardiovascular and cancer mortality.
Conclusions Evidence is now clear that persons with CWP experience excess mortality. UK Biobank results considerably reduce uncertainty around the magnitude of excess risk and are consistent with the excess being explained by adverse lifestyle factors, which could be targeted in the management of such patients.
- epidemiology
- fibromyalgis/Pain syndromes
- outcomes research
Statistics from Altmetric.com
Introduction
Persons with CWP, the characteristic symptom of fibromyalgia (FM), have been reported to experience premature mortality. The original observation, in a UK study, found 30% excess mortality was explained primarily by increased cancer incidence and reduced survival.1 2 A subsequent UK study confirmed the 30% excess mortality was primarily from increased cancer and cardiovascular deaths.3
Studies to identify the mediators of such a relationship have focused on low levels of physical activity, since the specific cancers contributing to excess mortality (female breast, prostate and colon) have been linked to low physical activity.4 5 It has been hypothesised that CWP may lead to low levels of physical activity and this was confirmed by a longitudinal study.6 Further studies have suggested additional lifestyle mediators of excess mortality: overweight has been shown to predict CWP onset and persistence7 8; persons with CWP have been reported as more likely to smoke, and women with CWP have been shown to have poorer quality diet.9
However not all studies conducted have found an excess mortality among persons with CWP. Meta-analyses have reported considerable heterogeneity, which has been attributed to differences in study populations, follow-up time, pain phenotype, methods of analysis and use of confounding factors.10 11 Currently there is considerable uncertainty as to whether there is an excess mortality risk. It is important to determine whether an excess risk exists and if so to quantify it, since there remains the potential, as part of managing patients with CWP or FM, to modify the mediators of any excess risk.
We therefore now report on the largest study to examine the relationship between chronic widespread pain (CWP) and mortality experience, and with considerably more detailed information on potential mediators of any excess risk. Further we include these results in a meta-analysis, with other published reports, to evaluate the coherence of evidence.
Methods
UK Biobank
Detailed methods used by UK Biobank have been published previously,12 and we provide only summary details of relevance to the current analysis. The study aimed to recruit around half a million persons aged 40–69 years who were registered with a general practitioner within the National Health Service. Approximately 9.2 million invitations were issued, between 2006 and 2010, to people living within 25 miles of one of 22 assessment centres throughout Great Britain.
At the assessment centre, participants completed questionnaires including items on lifestyle and environment. Information on pain was collected by means of a touchscreen questionnaire. Participants were asked ‘In the last month have you experienced any of the following that interfered with your usual activities?’ If they answered positively, they were then provided with a list that included individual regional pain sites, or alternatively they could choose the response ‘pain all over the body’. Subjects who reported ‘pain all over the body’ were not offered the option of choosing any further regional sites. Respondents were asked whether the reported pain had lasted at least 3 months, and those with ‘pain all over the body’ which had lasted 3 months were defined as having CWP. Participants were identified on the Office for National Statistics (ONS) records. ONS collects information on cause of death from civil registration records. For registered deaths, the underlying cause of death is derived from the sequence of conditions leading directly to the death and is recorded on the death certificate. The current analysis uses data on vital status up to August 2015.
The exposures that we considered in terms of mediating any relationship between CWP and mortality were focused on factors potentially modifiable as part of the management of CWP:
Body mass index (BMI), derived from measured height and weight, categorised according to standard cut-offs of the WHO.
Physical activity: minutes of walking per week (‘In a typical week, on how many days did you walk for at least 10 mins at a time’ and ‘How many minutes did you usually spend walking on a typical day?’); minutes of moderate activity per week (‘In a typical week, on how many days did you do 10 mins or more of moderate physical activities like carrying light loads, cycling at a normal pace (do not include walking)’ and ‘How many minutes did you usually spend doing moderate activities on a typical day?’); minutes of vigorous activity per week (as before but vigorous defined as ‘activities that make you sweat or breathe had such as fast cycling, aerobics, heavy lifting’). These were categorised as nil and then by quartiles.
Diet: participants were asked: (1) ‘On average how many heaped tablespoons of cooked vegetables would you eat per day? (Do not include potatoes.)’ (2) ‘On average how many heaped tablespoons of salad or raw vegetables would you eat per day? (Include lettuce and tomato in sandwiches)’ (3) ‘About how many pieces of fresh fruit would you eat per day?’ (4) ‘About how many pieces of dried fruit would you eat per day?’ Total daily ‘portions’ of cooked vegetables, raw vegetables and salad consumption were calculated and recoded as quintiles. Frequency of alcohol consumption was determined with response categories: never, daily or almost daily, three or four times a week, once or twice a week, one to three times a month, special occasions only. The latter two categories were combined into ‘Less frequently than once or twice per week’.
Smoking status: a history of smoking was recorded, which allowed us to classify respondents as current, never (or very rare) or ex-smokers, the latter group being divided into ex-regular and ex-occasional smokers.
UK Biobank analysis
We used Poisson regression models with robust estimation of SEs to model the relationship between CWP and all-cause mortality, adjusted for age group and sex. We tested and confirmed that the mediating variables were not collinear. We compared persons with CWP to persons who did not report any chronic pain. We additionally examined specific major causes of death as outcomes, including cardiovascular disease, respiratory disease and cancer. We report the mortality risk ratio (MRiR) including all deaths in the follow-up period, but excluding deaths in the first 2 years of follow-up from all subsequent analyses, since CWP may be a manifestation of an existing illness. Starting with a basic model containing CWP, age group and sex, we added, individually, lifestyle factors or markers that could possibly mediate any observed relationship. We then added all such potential mediators to a final model. Associations are expressed MRiR with 95% CI.
Meta-analysis
We used (in a modified way) and updated a search conducted by Smith et al,10 which identified studies examining the relationship between chronic pain and/or widespread pain (WP) and mortality. Although their review focused generally on chronic pain, our update focused only on studies examining WP or CWP. A second difference is that although previous meta-analyses extracted effect measures that were maximally adjusted for potential confounding factors, we have extracted data that are (as close as possible) only adjusted for age and sex. The difference is that we are answering the question ‘Do persons with CWP experience excess mortality (in comparison to those without chronic pain)’, whereas using fully adjusted effect measures is answering the question of whether the report of pain (per se) is associated with excess mortality. Thus the data on effect measures extracted from studies which they identified as eligible may be different.
We reran the published search strategy (in the appendix S1 of the original meta-analysis) from January 2014 (in order to ensure that articles published close to the time of the previous search were not missed) to January 2017.
Studies were eligible for the current meta-analysis provided that they:
were observational studies
sampled from a population sampling frame (or an approximation to such)
identified persons with WP or CWP (including FM) and a comparison group of persons without such pain; the definition of WP should involve recognised criteria or the reporting of pain all over the body
provided either a mortality rate ratio (MRtR) or MRiR quantifying the relationship between WP or CWP and mortality
were published as a manuscript in English in a peer-reviewed journal.
Identified abstracts were screened by two authors and any disagreement resolved by discussion. We also checked studies included in the meta-analysis by Smith et al10 to determine that they met the above eligibility criteria. Meta-analysis was conducted using a random effects model to reflect known differences in studies including geographical location, phenotypes and follow-up. The effect measures extracted from the eligible studies (MRrR or MRiR) were as closely as possible only adjusted for age and sex. In the meta-analysis, conducted using RevMan software, mortality risk ratio (MRR) has been used to signify the combined estimates using MRtR and MRiR. Sources of heterogeneity in effect measures were explored, specifically in relation to the geographical area in which the study was conducted and prevalence estimate of the phenotype studied.
Results
UK Biobank
From 502 627 UK Biobank participants, 2193 (0.4%) did not answer the pain questions and are therefore excluded from this analysis. Among the remaining 500 434 persons, 7130 reported CWP (prevalence 1.4%), while 281 718 reported that they did not have any chronic pain. These two subcohorts are the study population for the current analysis, and their characteristics are shown in table 1. The CWP and the ‘no chronic pain’ groups had the same median age (58 years). Persons with CWP were less likely to be male (36.3% vs 50%); were more likely to be heavier than normal weight (80.4% vs 63.5%); be a current smoker (18.6% vs 9.3%); and not to drink any alcohol (22.7% vs 6.7%). They also undertook physical activity less often. In total there were 12 799 deaths in the study population within the period of observation: 7486 (58%) classified as being due to cancer, 2691 (21%) cardiovascular disease, 728 (6%) respiratory disease, 436 (3%) due to external causes and 1458 (11%) were classified as ‘other’.
Characteristics of persons with chronic widespread pain (CWP) and no chronic pain in UK Biobank study
After adjusting for age and sex, participants with CWP had a more than twofold risk of dying in the follow-up period (MRiR 2.56, 95% CI 2.32 to 2.82), an excess that remained largely unchanged when deaths occurring in the first 2 years of follow-up were excluded (2.43, 95% CI 2.17 to 2.72). Deaths occurring in the first 2 years are excluded from all further analyses. Specific causes of death in excess were cancer (1.73 adjusted age and sex, 95% CI 1.46 to 2.05), cardiovascular (3.24adjusted age and sex, 95% CI 2.55 to 4.11), respiratory (5.66adjusted age and sex, 95% CI 4.00 to 8.03) and other disease-related causes (4.04adjusted age and sex, 95% CI 3.05 to 5.34), while the excess of deaths from external causes was not statistically significant (1.55adjusted age and sex, 95% CI 0.68 to 3.49).
We then examined to what extent the factors that were identified as being associated with pain status also predicted death in the period of follow-up (table 2). Age-adjusted risk of death was lower in women (MRiR 0.58 (95% CI 0.56 to 0.60). Age and gender adjusted risk was higher in obese participants (35–39 kg/m2 vs normal weight 5.54 (95% CI 5.08 to 6.03), ≥40 kg/m2 9.02 (95% CI 8.23 to 9.89)), and those who reported no walking (vs 1–100 min/week: 4.15 (95% CI 3.77 to 4.57)) or no moderate physical activity (vs 1–60 min/week: 2.95 (95% CI 2.74 to 3.19)). Risk of death was also higher in smokers (current smokers 2.54 (95% CI 2.39 to2.70), ex-smokers 1.44 (95% CI 1.36 to 1.52)) and persons who reported never drinking alcohol (vs daily drinkers 6.18 (95% CI 5.68 to 6.73)).
Relationship between demographic and lifestyle factors and risk of death
Finally, we tested to what extent adjusting the risk models for these measured lifestyle variables attenuated the relationship between CWP and excess mortality (table 3). Such attenuation would be consistent with the effects being mediated through such variable(s). When we did this, each class of variable (physical activity, BMI, smoking, diet including alcohol) when added to the model containing only pain status (CWP/no chronic pain), age group and sex resulted in a small attenuation of effect from an MRiR of 2.4 to MiRRs in the range of 2.0–2.2. However when all such potentially mediating variables were entered into the model, the MiRR reduced to 1.47 (95% CI 1.24 to 1.73). In cause-of-death-specific models with potential mediating variables, there remained an excess risk of cardiovascular 1.99 (95% CI 1.41 to 2.80), respiratory 1.91 (95% CI 1.08 to 3.36) and ‘other disease’ deaths 2.14 (95% CI 1.42 to 3.21), but the there was no longer an excess risk of cancer death 1.06 (95% CI 0.82 to 1.38) and external deaths 1.01 (95% CI 0.30 to 3.40).
Relationship between pain status and risk of death, adjusting for potential mediating variables
Meta-analysis
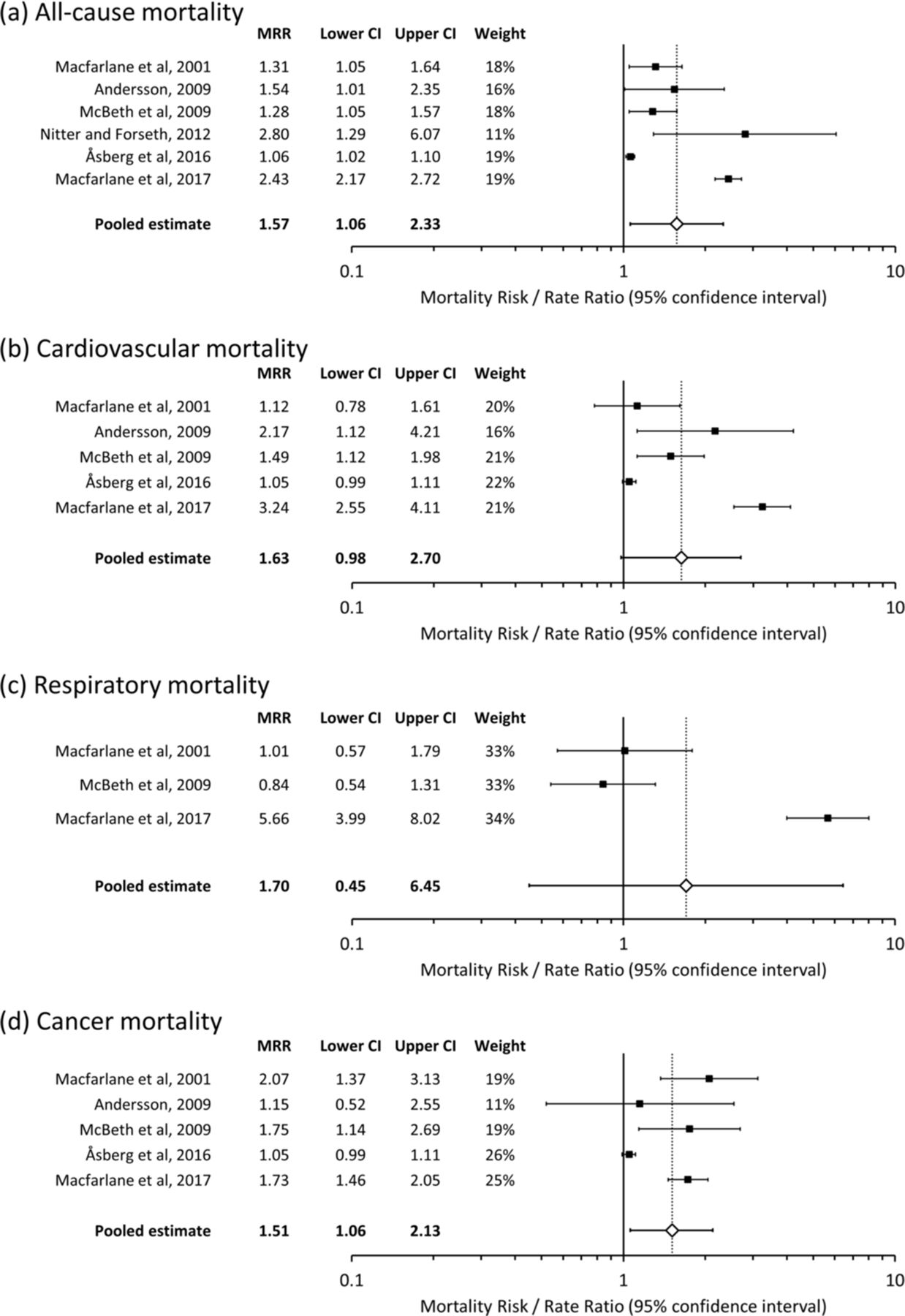
Our search identified 3171 unique publications, of which 15 proceeded to abstract screening and 1 to full-text screening and subsequent inclusion.12 Of the five studies included in the meta-analysis of Smith et al,10 one did not meet eligibility criteria for the current meta-analysis,13 since the pain phenotype did not include any measure of ‘widespreadness’. Instead the phenotype examined was multiple joint pain. Thus a total of six studies (including the current analysis) were eligible for the current meta-analysis.1 3 12 14 15 Characteristics of studies identified as eligible are given in table 4. One study presented data only to one decimal place and thus in the meta-analysis was identified as having a non-symmetrical log-transformed CI.3 We therefore contacted the first author of the publication and they provided more precise data (for analyses only adjusted for age and sex). Eligible studies included 580 020 participants from three European countries (Norway, Sweden and the UK). There was significant heterogeneity between studies: I2=98% for all-cause mortality, 95% for cardiovascular, 96% for respiratory and 91% for cancer (all p<0.001). All studies showed significant excess of all-cause mortality and the combined estimate of this was 57% (MRR 1.57; 95% CI 1.06 to 2.33). For cardiovascular mortality, three out of five studies showed a significant association and the combined estimate of this was 63% (1.63; 95% CI 0.98 to 2.70). For respiratory mortality, only one out of three studies showed a significant excess mortality, and there was considerable uncertainty around the pooled estimate of excess risk (1.70; 95% CI 0.45 to 6.45). For cancer, three out of five studies showed significant excess mortality and the pooled estimate was 51% (1.51; 95% CI 1.06 to 2.13) (figure 1).
Studies eligible for meta-analysis of CWP and mortality
{kind=link}
Forest plots of pain and all-cause and disease-specific mortality. MRR, mortality risk ratio.
We investigated the source of heterogeneity with respect to the relationship between CWP and all-cause mortality. When restricted by geographical area, the meta-analysis showed that considerable heterogeneity was present in studies conducted in Great Britain (I2=90%) (MRR 1.60; 95% CI 1.06 to 2.42) but not in studies conducted in Scandinavia (I2=0%) (MRR 1.06; 95% CI 1.02 to 1.10). Similarly when analysis was restricted to those studies with prevalence of CWP in the 10%–20% mid-range, that is, excluding those with the extreme prevalence estimates, there was no evidence of heterogeneity (I2=0%) (MRR 1.30; 95% CI 1.07 to 1.58).
Discussion
Using data from UK Biobank, involving over half a million study participants, we have demonstrated that persons with CWP have an important excess of risk of dying in the medium and long term. This excess risk was evident across all disease and non-disease categories. The meta-analysis of this relationship shows that all six studies conducted find excess mortality and estimate the excess risk across all studies at 59%, although there is significant heterogeneity. Similar excesses of cancer and cardiovascular mortality are observed. In UK Biobank, adjustment for lifestyle factors substantially reduced the excess risk, and this observation is consistent with them mediating the relationship between CWP and mortality.
Methodological issues
The main strengths of UK Biobank in addressing this question include that it uses a sampling frame that is considered to have almost complete population coverage. Although the participation rate was low (5.5%), we have previously published an analysis that demonstrates that the prevalence of regional pains in UK Biobank is very similar to more traditional pain epidemiological studies with higher participation, and that the study reproduces known relationships with aetiological factors.16 The large sample has allowed us to examine specific causes of death to exclude deaths within 2 years of the assessment (since WP may be a manifestation of a disease linked to death, eg, metastatic cancer) and consider the role of mediating factors.
The phenotype used in studies that have examined the relationship with mortality has varied considerably. They have included WP according to the definition within the American College of Rheumatology (ACR) criteria (1990) for FM,1 3 and modifications of the ACR 1990 FM criteria in terms of pain timing and distribution12 15 or bespoke definitions to capture ‘widespreadness’.14 The comparison populations also differ: persons who are free of pain,1 3 14 free of chronic pain15 or who simply do not meet the phenotype12 are variously used. Some studies had an additional criterion that WP is required to be chronic, although studies of WP have shown that the vast majority of persons with WP report chronic symptoms (81% in UK Biobank). These have resulted in prevalence proportions within population-based studies of between 1.4% and 23.1% and suggest important differences in the symptomatic populations studied. Interestingly the study with the highest prevalence12 reported a markedly lower excess risk of mortality. UK Biobank has used the most stringent definition, which has resulted in a prevalence similar to that of FM,17 and across all-cause and disease-specific mortality reports some of the highest excess mortality. This is consistent with the hypothesis that the greatest excess mortality is among those with more severe symptoms. Sensitivity analyses confirmed that heterogeneity in risk estimates was indeed partly explained by differences in prevalence, as well as by geographical area.
We have approached the analysis in a different way to some previous studies on this topic. We adjusted for the confounding factors of age and sex. Given that the question we are asking is ‘Do patients with CWP experience prematurely mortality?’ we believed that no further adjustment should be made. However when excess mortality is observed, it is of relevance to examine mediators — since these can become targets for intervention. Previous studies have identified lack of physical activity and poor quality diet as the variables that may explain a relationship. UK Biobank has a rich source of data to allow the assessment of these potential mediators. They nevertheless represent markers of these lifestyle factors rather than comprehensive assessments. Despite this, adjustment for these lifestyle markers almost completely explained cancer and ‘non-disease’ excess mortality and explained 56%, 80% and 62% of the excess mortality for cardiovascular, respiratory and ‘other-disease’, respectively.
Comparison with other studies and coherence of evidence
UK Biobank has provided results that are generally consistent with previously conducted studies. For cardiovascular mortality it has provided the largest estimate for excess mortality. It is the first study to suggest a relationship between CWP and excess mortality from respiratory disease.
The meta-analysis of Smith et al10 conducted on this topic chose to extract the most fully adjusted model available in included studies, which means that this examines a subtly different question of whether pain directly increases mortality risk (independent of any lifestyle, psychosocial or clinical factors). We believe that the most clinically relevant question for clinicians managing patients with WP/CWP or FM is what factors can be modified that could reduce any excess mortality which such patients experience. We also excluded one study included in the previous meta-analysis. The study of Macfarlane et al13 was not eligible for this analysis as it examined the mortality consequences of multijoint pain (at least four joints). There was no requirement for pain to be widespread. All included studies had some requirement for the pain to be widespread or for the participant to endorse that the pain was all over their body. Even if the study of Macfarlane et al,13 which did not find any excess mortality MRiR (0.86; 0.74,1.01), had been included in the meta-analysis, the combined estimate would still have suggested an important excess. Exclusion of a phenotype that excludes a measure of ‘widespreadness’ is supported by a proposed modification to the 2011 research criteria for FM, which requires that multisite pain is also widespread across the body.18 The meta-analysis of Åsberg et al19 concluded that ‘pooled data gave no evidence for a higher mortality rate among individuals with chronic widespread musculoskeletal complaints’. This put emphasis on a pooled unadjusted MRR of 1.69, which was not statistically significant, and a markedly reduced excess (MRR 1.13) after full adjustment. The inclusion of UK Biobank, considering age-adjusted and sex-adjusted risks, has provided a similar pooled estimate of excess risk (MRR 1.59) and is now statistically significant.
We conclude that the evidence is now clear that persons with CWP experience excess mortality. UK Biobank results considerably reduce uncertainty around the magnitude of excess risk, and demonstrate that the risk is unlikely to be due to the experience of pain per se, but is substantially explained by lifestyle factors associated with having pain (poor diet, low levels of physical activity, smoking, high BMI). These provide important targets for intervention in managing patients with CWP. Optimal management of FM should include exercise, but this is often not provided in a structured and supported way to facilitate long-term behaviour change. Few patients with CWP or FM receive specific supported care in improving diet or stopping smoking. The data from this study show that changing the habits of persons with CWP to be similar to persons without CWP could reduce mortality by around 35%. Such approaches should have high priority in the routine care of such patients.
Acknowledgments
This manuscript uses the UK Biobank resource (Application 1144). We acknowledge the authors of a previous meta-analysis on this topic (Diane Smith, Ross Wilkie, Olalekan Uthman, Joanne L Jordan, John McBeth) whose published search strategy we used as the basis for our meta-analysis, although our meta-analysis had a more restricted focus and the criteria for determining eligibility and the data we extracted from eligible studies were not identical and resulted in selection of a different group of studies. We thank John McBeth (University of Manchester) for providing additional data relating to one of the studies, to allow it be included in the meta-analysis.
References
Footnotes
Contributors GJM had the idea for the study and together with GTJ designed the analysis plan for UK Biobank. GTJ undertook the UK Biobank analysis. MSB conducted the updated systematic review, and all authors participated in undertaking the meta-analysis. GJM drafted the manuscript, but all authors made an important intellectual contribution to the text.
Competing interests None declared.
Ethics approval North West Multi-centre Research Ethics Committee (MREC).
Provenance and peer review Not commissioned; externally peer reviewed.