
Abstract
Background
Hallux valgus is a frequent condition of the forefoot, resulting in cosmetic deformity and pain. Chevron osteotomy (CO) is widely employed for the treatment of hallux valgus. Chevron–Akin double osteotomy (CAO) was previously described and superiority over an isolated Chevron procedure was assumed. The objective of this study was to compare the short-to-middle term outcomes of CO and CAO.
Patients and methods
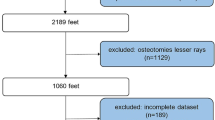
This study included 72 patients with established diagnosis of mild-to-moderate hallux valgus, treated by either isolated CO or CAO. The CO group included 46 patients (mean 51.5 years) with a mean hallux valgus angle of 27°, while the CAO group included 26 subjects (mean 53.1 years) and a mean hallux valgus angle of 32° preoperatively. All patients were reviewed by physical examination, and standardized questionnaire, and pre- and postoperative standing X-rays were performed. Matched group analysis was carried out to analyze statistical differences of both techniques.
Results
The patients were assessed and group matched at a mean of 1.37 years for the CO group and 1.04 years for the CAO group, postoperatively. Mean improvement of HVA (hallux valgus angle) was 10.6° in the CO group and the CAO group improved by 17.5°. DMAA (distal metatarsal articular angle) improved in the CO group by 5.4° and in the CAO by 13.7°. Mean AOFAS score improved by 27.9 (CO) and 21.5 (CAO). Patient satisfaction was high in both groups, with a tendency towards higher values within the CAO group.
Conclusions
These findings indicate that Chevron–Akin double osteotomy is a save and practicable procedure for the treatment of mild-to-moderate hallux valgus. Superiority of combined Chevron–Akin procedure over an isolated Chevron osteotomy might be limited to distinct clinical settings, but should not be generally assumed.


Similar content being viewed by others


References
Hueter C (1879) Klinik der Gelenkerkrankungen mit Einschluss der Orthopädie. Vogel, Leipzig
Dykyj D (1989) Pathological anatomy of hallux abducto valgus. Clin Podiatr Med Surg 6:1–15
Piqué-Vidal C, Solé MT, Antich J (2007) Hallux valgus inheritance: pedigree research in 350 patients with bunion deformity. J Foot Ankle Surg 46(3):149–154
Roddy E, Zhang W, Doherty M (2008) Prevalence and associations of hallux valgus in a primary care population. Arthritis Rheum 59:857–862
Klein C, Groll-Knapp E, Kundi M, Kinz W (2009) Increased hallux angle in children and its association with insufficient length of footwear: a community based cross-sectional study. BMC Musculoskelet Disord 17(10):159
Easley ME, Trnka HJ (2007) Current concepts review: hallux valgus part 1: pathomechanics, clinical assessment, and nonoperative management. Foot Ankle Int 28:654–659
Tinetti ME, Speechley M, Ginter SF (1988) Risk factors for falls among elderly persons living in the community. N Engl J Med 319:1701–1707
Corless JR (1976) A modification of the Mitchell procedure. J Bone Joint Surg 55:138
Schneider W, Aigner N, Pinggera O, Knahr K (2004) Chevron osteotomy in hallux valgus. Ten-year results of 112 cases. J Bone Joint Surg Br 86:1016–1020
Akin O (1925) The treatment of hallux valgus: a new operative procedure and its results. Medical Sentinel 33:678
Mitchell LA, Baxter DE (1991) A Chevron–Akin double osteotomy for correction of moderate hallux valgus. Foot Ankle 12:7–14
Karasick D, Wapner KL (1990) Hallux valgus deformity: preoperative radiologic assessment. AJR Am J Roentgenol 155:119–123
Hardy RH, Clapham JC (1951) Observations on hallux valgus; based on a controlled series. J Bone Joint Surg Br 33:376–391
Hammond EC (1985) Matched groups analysis method. Natl Cancer Inst Monogr 67:157–160
Mann RA (1990) Bunion surgery: decision making. Orthopedics 13:951–957
Pochatko DJ, Schlehr FJ, Murphey MD, Hamilton JJ (1994) Distal chevron osteotomy with lateral release for treatment of hallux valgus deformity. Foot Ankle Int 15:457–461
Resch S, Stenström A, Reynisson K, Jonsson K (1994) Chevron osteotomy for hallux valgus not improved by additional adductor tenotomy. A prospective, randomized study of 84 patients. Acta Orthop Scand 65:541–544
Schneider W, Knahr K (2002) Keller procedure and chevron osteotomy in hallux valgus: five-year results of different surgical philosophies in comparable collectives. Foot Ankle Int 23:321–329
Jones SHA, Al Hussainy F, Ali RP, Betts MJ (2004) FlowersScarf osteotomy for hallux valgus—a prospective clinical and pedobaraographic study. J Bone Joint Surg Br 86:830–836
Crevoisier X, Mouhsin E, Ortolano V, Udin B, Butoit M (2001) The Scarf osteotomy for the treatment of hallux valgus deformity: a review of 84 cases. Foot Ankle Int 22:970–976
Kristen KH, Berger C, Stelzig S, Thalhammer E, Posch M (2002) The Scarf osteotomy for the correction of hallux valgus deformities. Foot Ankle Int 23:221–229
Acknowledgments
PL was supported by the Regensburger Forschungsförderung in der Medizin (ReForM).
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lechler, P., Feldmann, C., Köck, F.X. et al. Clinical outcome after Chevron–Akin double osteotomy versus isolated Chevron procedure: a prospective matched group analysis. Arch Orthop Trauma Surg 132, 9–13 (2012). https://doi.org/10.1007/s00402-011-1385-3
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-011-1385-3