Article Text

Abstract
Introduction Applicants to chronic pain medicine fellowship programs often express confusion regarding the importance of various selection criteria. This study sought to elucidate program directors’ considerations in applicant selection for fellowship interviews and ranking and to correlate these criteria with match statistics to provide a guide for prospective candidates.
Methods An electronic survey was sent to all Accreditation Council for Graduate Medical Education-accredited chronic pain fellowship directors. The importance of various applicant characteristics were evaluated and compared with recent match data.
Results Fifty-seven program directors completed the survey. The most important factors involved in applicant interview selection were perceived commitment to the specialty, letters of recommendation from pain faculty, scholarly activities, and leadership experiences. Although completion of a pain rotation was valued highly, experience with procedures was of relatively low importance. There was no preference if rotations were completed within the responders’ department. Variability was noted when considering internal applicants or the applicant’s geographic location. When citing main factors in ranking applicants, interpersonal skills, interview impression and applicant’s fit within the institution were highly ranked by most responders.
Discussion Assessment of an applicant’s commitment to chronic pain is challenging. Most responders prioritize the applicant’s commitment to chronic pain as a specialty, scholarly activity, participation in chronic pain rotations, pain-related conferences and letters of recommendation from pain faculty. Chronic pain medicine fellowship candidates should establish a progressive pattern of genuine interest and involvement within the specialty during residency training to optimize their fellowship match potential.
- chronic pain
- pain medicine
- education
- internship and residency
- analgesia
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Pain medicine fellowship remains competitive, as evidenced by consistent match trends. However, there is limited guidance regarding the importance of various selection criteria for fellowship candidacy.
What this study adds
This study shows that the most important factors involved in applicant interview selection and ranking for chronic pain medicine fellowship are commitment to the specialty, letters of recommendation from pain faculty, peer-reviewed publications and leadership experiences. Prospective applicants should establish a progressive pattern of genuine interest and involvement within the specialty.
How this study might affect research, practice or policy
This study provides a guide to prospective fellowship candidates, improves awareness and fosters self-analysis prior to the application season.
Introduction
Chronic pain medicine fellowships are 1 year, multidisciplinary postgraduate training programs focused on the comprehensive diagnosis and management of chronic pain. The number of programs accredited by the Accreditation Council for Graduate Medical Education (ACGME) increased from 93 to 111 over the past 5 years, currently with 349 potential positions.1 2 There is a trend of more than 96% of positions filled, with the percentage of matched applicants rising from 77.1% to 85.3% over the same period.3–5 National Residency Matching Program (NRMP) 2016 data reported that most programs received around 150 applications and interviewed 29 applicants on average.5
Applicants are frequently drawn to the subspecialty of chronic pain medicine because of interest in procedural skills, multidisciplinary care, personal experiences with pain, guidance by mentors and an interest in helping a population in need of improved quality of life.6 Certification in pain medicine is offered through the American Board of Medical Specialties (ABMS) for multiple specialties including anesthesiology, physical medicine and rehabilitation (PM&R), neurology, psychiatry, family medicine, emergency medicine and radiology. NRMP data reported a 3-year trend of more PM&R applicants matching (16.4%, 19.1% and 19.7%), while neurology applicants remained relatively stable (2%, 3.5% and 3.2%), and anesthesiology fluctuated (80.4%, 65.6%, 74.7%). Of the 337 matches into chronic pain fellowships in 2021, 215 (63.8%) were allopathic medical doctor (MD) graduates, 66 (19.6%) were doctors of osteopathy (DO) graduates, 39 (11.6%) were United States citizens who studied medicine abroad (US-IMG) and 17 (5%) were non-US citizens international medical graduates (non-US IMG). Interestingly, chronic pain medicine is the fourth highest specialty by percentage of positions filled by osteopathic graduates.3–5
Pain medicine continues to be one of the most competitive fellowship programs in the USA.3 A potential reason for such a competitive environment may be the broad pool of applicants, given the unique multidisciplinary nature of the specialty. There is great variability among applicants’ characteristics, such as standardized test scores, medical school transcripts, geographic location, as well as training background and clinical skill set. Therefore, it is beneficial for prospective candidates to understand the key factors used for interview selection when program directors (PDs) analyze a large pool of applicants. The current published literature is helpful to understand trends in pain fellowship matching. However, it does not identify key factors involved in applicant interview selection and ranking by PDs. Some of the earliest studies provided data regarding factors used by PDs to select residents, and both studies affirmed that interpersonal skills during the interview was the most important selection variable.7 8 Limited survey studies analyzing characteristics for residency in orthopedic surgery, ophthalmology, radiology, psychiatry and PM&R have been published. Additionally, fellowship PDs have been surveyed in the fields of sports medicine, hand surgery, obstetrics and gynecology, neuroradiology, pediatric emergency medicine, spine surgery, trauma surgery and sleep medicine.9–22 However, there are no publications to date discussing the key factors involved in fellowship applicants’ interview selection and ranking in the field of chronic pain medicine.
In this study, we surveyed chronic pain medicine fellowship PDs regarding the importance of various applicant characteristics involved in fellowship interview selection and ranking. Since there are no data discussing this in the field of pain medicine, it is our hope that the results of this study will improve applicant’s awareness of the key factors involved in applicant selection and ranking, and foster applicant self-analysis prior to the application season, and most importantly, provide a guide to prospective pain medicine fellowship candidates.
Methods
A succinct anonymous electronic survey (appendix 1) was developed with collaboration from all authors and stored on REDCap secure software. Data were collected from 1 August to 24 August 2021. The survey was distributed electronically to PDs of every ACGME accredited chronic pain fellowship program at the same time, identical to all recipients, who had an equal length of time to respond to the anonymous electronic survey. Questions assessed three main areas of fellowship candidacy, including medical training, academics and experience with leadership and research. Various factors were rated on a scale of importance or preference. Scores of 1–3 (out of 10) were considered lowest importance, 4–6 medium importance, 7–9 high importance and 10 extreme importance. Respondents’ preference of applicant’s primary specialty ranked from highest preference (5) and ‘will not be considered’ (0). The medical training subsection included domains such as medical degree, primary specialty, chief resident appointment and exposure to procedures. The academics subsection domain included letters of recommendation (LORs), elective rotations, personal statement (PS) and others. Leadership and research sections included participation in committees, societies and publications, followed by interview impressions, fit within the institution, etc. Statistical analysis was performed on all of the main factors studied, and results were reported with a weighted mean and SD for each question. It should be noted that the demographics (age, gender, race) of the PD responders were not captured as part of the survey.
Results
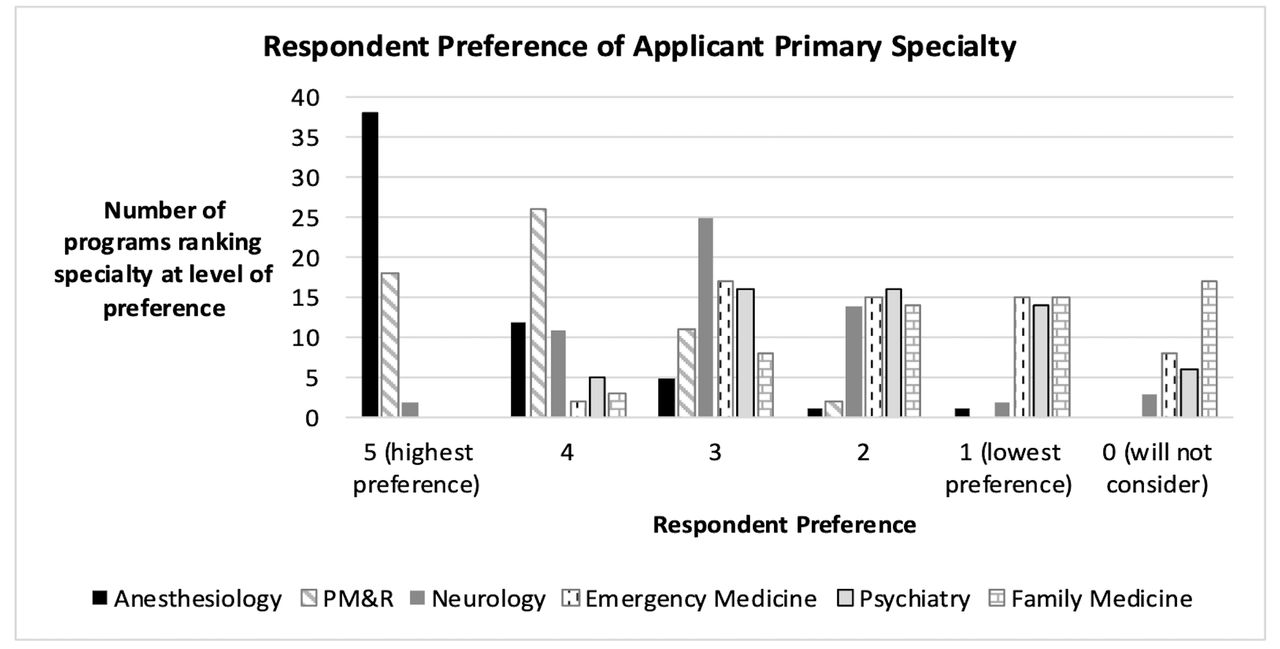
Fifty-seven PDs completed the survey (51.3% of all ACGME accredited fellowships). Most PDs reported consideration for applicants from diverse training backgrounds. All survey responders (100%) reported accepting allopathic (MD) medical degrees, with 93% accepting osteopathic (DO) medical degrees, and 71.9% accepting international medical graduates. The majority of programs (84%) have a screening process that evaluates US Medical Licensure Exam (USMLE) scores. However, 59.6% do not have a predetermined cut-off score, 3.5% screen with score >200 points, 7% with score >210 points, 12.3% with score >220 points and 1.8% filter by a score >240 points. The importance of individual criteria are summarized in table 1. Figure 1 shows a graphic with respondents’ preference of applicant’s primary specialty, while table 2 displays preferred specialty mean averages with SD. Figure 2 displays a graphic with the percentage of programs placing a particular magnitude of importance on applicant qualities, ranked from lowest importance to extreme importance. Figure 3 summarizes this study key findings.
Importance of factors involved in selection of applicants for interview and determination of candidate ranking

Respondent preference of applicant primary specialty. PM&R, physical medicine and rehabilitatation.

Applicant qualities ranked by importance.
{kind=link}
{kind=link}
{kind=link}
Key factors involved in applicant interview selection and ranking for chronic pain medicine fellowship.
Preferred applicant specialties
Perceived commitment to the subspecialty of chronic pain was of high importance to 43.9% of participants and of extreme importance to 47.4% of participants. LORs from pain faculty were reported as extreme importance by 31.6% of participants and of high importance by 56.2% of participants. In contrast, LOR from non-pain faculty were perceived as less impactful. Leadership experiences, such as mentoring students and committee/society involvement, as well as poster presentations at scientific meetings were of medium importance. Peer-reviewed publications were considered of high importance by 64.9% of participants. Many participants (50.9%) reported that chief resident appointment was of highest importance, and 35.1% reported medium importance when selecting applicants to interview. Perceived interest in academic medicine and community medicine were reported of medium importance; however, perceived interest in academic medicine had a higher mean average when compared with perceived interest in community medicine. This study revealed that fellowship programs accept trainees of different backgrounds, including anesthesiology, PM&R and a variety of other ABMS board-eligible specialties. Figure 1 and table 2 show the responders’ preference by specialty.
The data reported the highest preference for anesthesiology applicants at 66.7%, followed by PM&R applicants at 31.6%. However, when data results were analyzed with mean average and SD, including level of preference ranked 0 to 5 with (5) highest preference and (0) will not consider, there was a closer average preference between the two specialties. However, the overall number of applicants and proportionally higher success rate of anesthesiology applicant matches is consistent with PDs stated preference. This is likely attributable to the fact that most pain fellowship programs are affiliated with anesthesiology departments, and there is possibly a preference towards candidates from a similar background. Overall, PDs express variable preference for applicants internal to the program’s department (5.37±2.89) versus external to the department at the institution (4.79±2.37) or from other institutions (3.54±2.18).
When ranking an applicant, 35.1% of PDs considered interview performance of extreme importance and 63.2% of high importance. Interpersonal skills, professionalism and overall impression ranked extreme importance for 56.1% of participants and 42.1% ranked as high importance. The applicant’s fit within the institution was reported as extreme importance by 47.4% of PDs, while the applicant’s geographic proximity to the program was variable. Follow-up thank you notes were considered of low importance.
Discussion
PDs expressed commitment to the specialty of chronic pain as the most important factor in applicant selection. Responders assessed this through participation in chronic pain rotations, knowledge of the field and an understanding of issues facing the specialty. Additionally, responders reported that a record of progressive and genuine interest in the field through pain-related scholarly activity, seeking mentorship and having participation in pain societies, and leadership activities with committees or pain societies were key components of perceived commitment to the specialty. The importance of publications (eg, PubMed indexed studies or book chapters) is clear. Most responders (93%) reported that 1–5 peer-reviewed publications are appropriate, while 7% reported that 6–10 publications are appropriate. These numbers are overall less than NRMP data of matched fellows averaging 6.8 publications for US MD, 5.6 for US DO, 13.4 for US IMGs and 16.4 for non-US IMGs.3–5 Responders cited the importance of longitudinal research in residency as opposed to engagement in these activities within a few months leading to the fellowship application. These findings are similar to studies on residency or fellowship selection criteria in other specialties.9 10
Early commitment to the specialty of chronic pain should not sacrifice a candidate’s engagement within their primary specialty. In fact, responders reported that candidates must demonstrate interest in chronic pain medicine while simultaneously fulfilling core residency requirements. Responders reported that at least one or two rotations in chronic pain are important, which helps support the applicant’s global understanding of the specialty, including procedural skills, clinical experience and the daily issues of a pain practice. There is no consistent preference for where the rotations are performed, whether within the responders’ departments or elsewhere. Geographical bias may play a role in applicant preference for fellowship programs; however, PDs generally consider the applicant’s location of medium importance.
Candidates must prioritize attainment of LOR from pain medicine faculty during chronic pain rotations. Key components in LORs include discussion of applicant teachability, proactivity of the applicant, leadership and research experiences, and discussion of how the applicant exceeded expectations to demonstrate commitment to the field. Survey responders also noted attention to LORs with mention of personal experiences, professionalism, work ethic, adaptability to feedback and assessment of applicant’s reputation in the department. Additionally, PDs also appreciated reports on applicants’ reliability, teamwork abilities, empathy and rapport with patients, humility, knowledge of multidisciplinary concepts in pain care, interpersonal skills and ability to work with others. In particular for applicants of specialties other than anesthesiology, it may be prudent to have LORs that detail the extent of the applicant’s involvement in chronic pain medicine experiences. This may help PDs appreciate the magnitude of pain experiences when less familiar with applicants’ residency curricula. As a core component to the fellowship application, the PS is often mentioned as intimidating to candidates. Survey responders reported that the PS provides another opportunity for the applicant to express their commitment to the specialty. Responders cited interest in applicants’ unique stories, understanding of the specialty and opportunities to note qualifications for the field. PDs often rely on the PS to build familiarity with the applicant and motivations for pursuing fellowship. Postfellowship plans may be included as well.
Overall, this analysis repeatedly returned to perceived commitment to the specialty. Future fellowship candidates may wish to implement a plan to demonstrate a record of progressive genuine interest in chronic pain. In addition to completing the core requirements of their specialty, applicants should focus on completion of chronic pain rotations to broaden their understanding of the field, including exposure to clinical demands, procedural skills and understanding of this unique patient population. Participation in chronic pain rotations also offers opportunities for LOR from pain faculty, which are perceived by PDs as one of the most important factors when selecting applicants to interview. This study found that prospective applicants may wish to focus on scholarly productivity in pain research, participation in pain-related conferences with poster presentations and society leadership engagements. Applicants may seek mentorship from pain faculty and PDs during residency, and such networking may be a factor to facilitate interview selection and ranking. Networking with pain faculty and seeking mentorship from experts is fundamental to recognizing whether the specialty is an appropriate fit for an applicant.
PDs are frequently asked what applicants may do to improve chances of obtaining an interview, usually only a few months prior to application submission. Realistically, there are limited options to significantly alter the application at that point. It is too late to change medical school, residency location, chosen specialty or USMLE scores. Historically, candidates may think there is a bias for residents with high board scores. However, this survey shows that only 40% of programs have a predetermined board score cut-off, which may prompt applicants to focus on other aspects of their application during residency. If time allows, it may be beneficial to broaden exposure with additional chronic pain rotations and complete scholarly activities, such as pain-related publications. The PS and LOR are the main application components that the applicant has the ability to improve shortly before submission. Lastly, it may be wise for an applicant to contact the program directly to express their specific and genuine interest, but excessive persistence may be detrimental.
Once the applicant reaches the interview, the overall impression created during the interview, ‘performance on the interview’ and ‘fit’ within the institution are crucial components of candidate ranking. The candidate’s ‘fit’ within the program is unique to each specific fellowship program. Each fellowship program has unique qualities that may appeal to or support different candidates in different ways. Programs may use multiple interviews to focus on practical medical and non-medical scenarios to assess critical thinking, empathy and communication skills.23 Institutions often also use the feedback from staff, such as coordinators, nurses and ancillary personnel during the application and interview day while interacting with prospective applicants. PDs often have favorable impressions of candidates who demonstrate preparation for and institution-specific knowledge during interviews. Understanding whether a candidate is a good fit is difficult based solely on paper applications, so LOR may help determine whether applicants have qualities that would translate to success in the program.
Limitations
Just over half of the ACGME-accredited chronic pain medicine fellowship PDs participated. The response rate of this study was similar to other published survey studies on the specialty and superior to studies on other fellowship disciplines.9 24–28 However, it is prudent to acknowledge that the overall data may not appropriately represent all PDs preferences, and generalizability of the data cannot be assumed to avoid dogmatic conclusions. As mentioned previously, the demographics (age, gender and race) of the PD responders were not captured as part of the survey. This study also did not explore timing of application submission, which is often a topic of discussion among applicants. Earlier submission for maximal consideration among programs should be considered, although anecdotally most PDs do not review applications until at least February under the current system. Most importantly, it is highly recommended to submit a complete application, including all assigned LOR.
Conclusion
Chronic pain medicine fellowship prospective applicants should prioritize participation in chronic pain rotations to increase their knowledge of the field and an understanding of issues facing the specialty, in addition to participation in peer-reviewed research, and leadership opportunities in committees and societies. LORs from pain faculty describing the candidates’ clinical performance, work ethic and individualized qualifications were ranked as the most important factor when selecting applicants to interview, along with perceived commitment to the specialty. Early commitment in residency training, with networking and mentorship from pain faculty, is essential to build a progressive and cumulative history of genuine interest and involvement within chronic pain medicine.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Institutional review board approval from The University of Kansas Medical Center was obtained for this study, ID #STUDY00147594. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank all the Accreditation Council for Graduate Medical Education accredited chronic pain fellowship program directors who completed this survey.
References
Footnotes
Twitter @VinnyFrancioMD, @benjamin_gill, @jonhagedornmd, @RobertPaganMD, @ScottPritzlaff, @kohanlynn, @dsayed1
Contributors VTF, BG, RPR, JMH and SP contributed to study conception. VTF, BG, JMH, SP, TF, LK and DS contributed to study design. VTF, SP, TF, LK and DS contributed to study conduct. VTF and BG contributed to data analysis. All authors contributed to data interpretation and manuscript preparation. VTF is a guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.