Article Text

Abstract
The medical field has been experiencing numerous drug shortages in recent years. The most recent shortage to impact the field of interventional pain medicine is that of iodinated contrast medium. Pain physicians must adapt to these changes while maintaining quality of care. This position statement offers guidance on adapting to the shortage.
- COVID-19
- Drug-Related Side Effects and Adverse Reactions
- Diagnostic Techniques and Procedures
- Injections, Spinal
- Multimodal Imaging
Data availability statement
No data are available. N/A.
Statistics from Altmetric.com
- COVID-19
- Drug-Related Side Effects and Adverse Reactions
- Diagnostic Techniques and Procedures
- Injections, Spinal
- Multimodal Imaging
Key findings
What is already known on this topic
Medical shortages have been impacting the medical field with increasing frequency impacting patient care.
What this study adds
This paper serves to address the recent iodinated contrast medium shortage and provide guidance to physicians on caring for patients including prioritization of procedures, use of alternative imaging techniques, and risks associated with alternative contrast mediums.
How this study might affect research, practice or policy
This study may help guide physicians’ decision making when caring for patients during the iodinated contrast medium shortage.
Introduction
Contrast medium is frequently used to confirm accurate interventional placement, injectate delivery, and to exclude flow of off-target tissue in interventional pain procedures including but not limited to epidurals, paravertebral, intravertebral (kyphoplasty), joint (eg, facet, sacroiliac, hip, knee), lumbar sympathetic plexus, and visceral sympathetic blocks). These procedures are performed frequently in the USA; with an annual estimate of 2 million in the Medicare population alone from 2008 to 2014.1
In recent years, our world has been impacted by numerous supply chain shortages, including medication shortages. Currently, iohexol is unavailable or in limited supply due to a shutdown of a production facility in Shanghai, China.2 The facility is now open and resuming production of iohexol, however the shortage is expected to last for a few months. The availability of alternative iodinated contrast medium (ICM) such as iopamidol, iopromide, ioversol, and ioxilan may also be impacted secondary to increased use. Shortage of drugs also occur frequently. Medication errors related to drug shortages can be reported to the Medication Error Reporting site (https://www.ismp.org/report-medication-errorsite) on the Institute for Safe Medication Practices (ISMP) website.
Organizations and healthcare systems should provide guidance to clinicians during the shortage. Every attempt to conserve contrast for clinically appropriate interventions should be made. In the field of pain medicine, clinicians should consider minimizing iodinated contrast use, using alternative image guidance (ultrasound (US)) when feasible, delaying interventions that are not clinically urgent, or not safely performed without contrast. Members of the American Society of Regional Anesthesia and Pain Medicine (ASRA Pain Medicine) created an ad hoc working work to create these recommendations. The ASRA Pain Medicine Board of Directors reviewed and approved this document. The recommendations contained herein do not define standard of care. They are not intended to replace clinical judgment. In the imperfect setting of heterogeneity of the data, limited data, controversial topics, and bias inherent to expert opinion, compliance with the recommendations may not result in improved outcomes compared with alternative therapies consistent with personalized medicine.
Discussion
Should interventional pain procedures be delayed during the iohexol or other ICM shortages?
The majority of interventional pain procedures are deemed elective procedures. Injections are not typically performed on an emergency basis since the patient’s pain can be at least partially treated with medication and non-pharmacological approaches until a procedure can be scheduled.
Recommendations
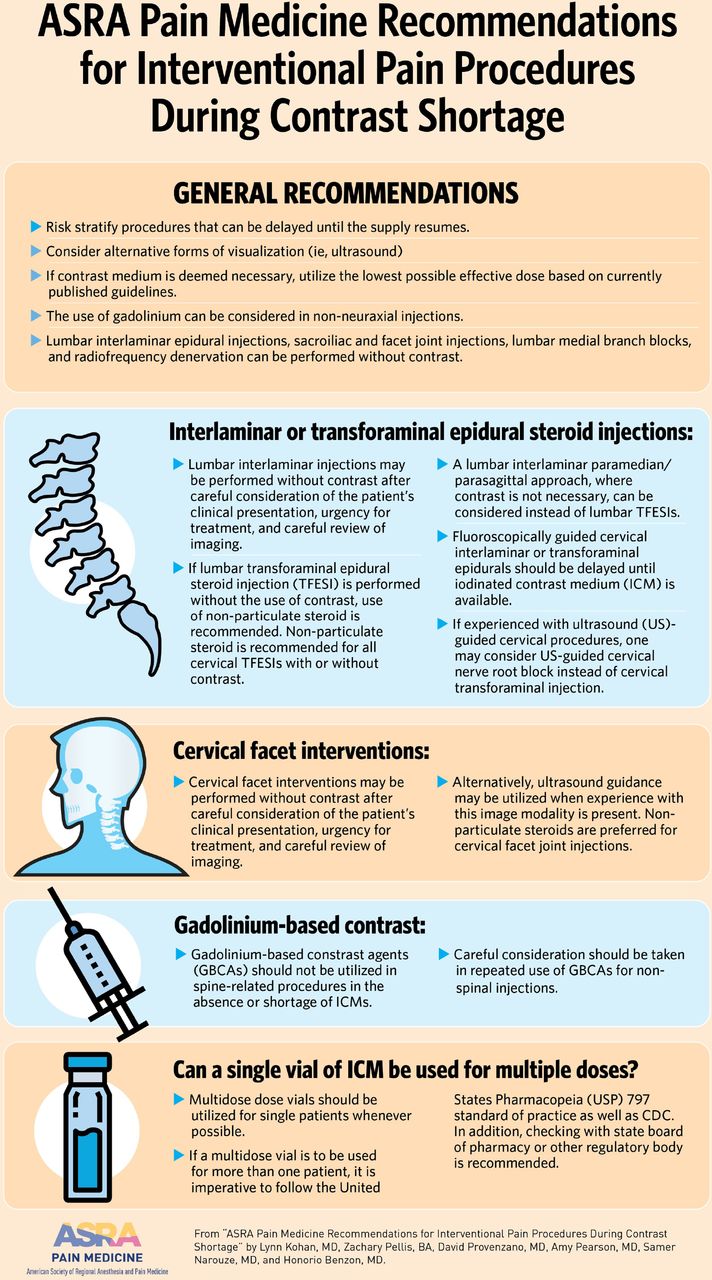
Attempts should be made to risk stratify procedures that can be delayed until the supply resumes. Patients with severe pain and functional impact should be prioritized. Patients at risk of adverse events, such as patients with suspected intrathecal drug delivery system malfunction, who are in need of intrathecal catheter studies, particularly with baclofen intrathecal delivery, should also be prioritized. Consideration should be given to alternative forms of visualization (ie, US) or the exclusion of ICM when nonessential for safety. The use of gadolinium-based contrast agent (GBCA) can be considered in non-neuraxial injections.
Which interventional pain procedures can be performed safely without the use of iohexol or other ICM?
Recommendations
A majority of fluoroscopically-guided interventional pain procedures can be performed without the use of contrast agent. These include but are not limited to lumbar interlaminar (IL) epidural injections, sacroiliac and facet joint injections, lumbar medial branch blocks (MBB), radiofrequency denervation, and peripheral joint injections. When a contrast agent is used, the minimum amount that does not reduce accuracy should be injected. Additionally, many procedures can use US imaging including stellate ganglion blocks, joint injections, and deep soft tissue injections (eg, piriformis muscle). When performing these procedures under US, vascular structures can also be identified and avoided.
Can IL or transforaminal epidural steroid injections be performed without the use of contrast?
The use of contrast agent in epidural steroid injections (ESIs) is typically recommended. Both a multisociety working group and the World Institute of Pain (WIP) Benelux working group recommend the use of contrast in ESIs to ensure the needle is appropriately placed as well as to reduce risk of neurological injury.3 4 Gaps in the ligamentum flavum, particularly in the cervical region, increase risks of false loss or resistance with subsequent spinal cord injury.5 Additional complications associated with ESIs include vascular penetration. Intravascular placement can be associated with seizures, hematoma, and decreased procedure efficacy. Transforaminal ESIs (TFESIs) and cervical procedures are typically associated with a higher risk of vascular complications than IL and lumbar procedures, respectively.6–12 Non-vascular aberrant spread of injectate, including intradiscal, may also occur.13–16
While use of ICM is recommended to lessen the risk of inadvertent intrathecal placement and vascular compromise, both the multisociety working group and the WIP Benelux working group, however make concessions for patients with documented contrast allergies suggesting that both cervical and lumbar IL and transforaminal injections can be performed without contrast.3 4 The use of lateral or contralateral lateral oblique views for IL approaches is recommended as well as the use of dexamethasone for all transforaminal injections in which contrast is not utilized. Thus, ultimately decision to perform these procedures via fluoroscopic guidance without contrast should be considered on a case by case basis after careful consideration.
The clinician should also consider alternative imaging (US) or techniques (parasagittal) to perform epidurals that may be more safely performed without the use of ICM.
In the cervical region, one could consider US-guided cervical nerve root injection instead of cervical TFESI.17 Retrospective comparative studies showed that US-guided cervical selective nerve root block was not inferior to fluoroscopy guided transforaminal or IL injections.18 19
A lumbar parasagittal or paramedian approach, wherein the needle is inserted on the side of the patient’s radicular pain, may be considered in patients with unilateral radicular pain, especially when several levels are involved. In the parasagittal or paramedian approach, the use of contrast is not necessary. A study demonstrated greater incidence of anterior epidural contrast spread, the interface between the herniated disc and the nerve root, when the injection was parasagittal (100%) compared with transforaminal (75%).20 RCTs showed greater incidence of anterior epidural spread (90% vs 32%) and pain relief (68% vs 17%) with the parasagittal approach compared with the midline approach21; better pain relief with either the parasagittal and transforaminal approaches compared with the midline approach22; and, equivalent pain relief between the parasagittal and transforaminal approach (76%–78%).23 One study showed lower VAS scores in the infraneural group compared with the paramedian approach.24
For targeted cervical ESI, the advancement of a catheter to the side and level of pathology may be considered instead of the transforaminal approach. However, studies showed no superiority of the targeted catheter approach over a standard C7-T1 IL ESI. Pain relief and other outcome measures were similar at 1 month, 6 months, and 1 year.25–27 The similar efficacy may be secondary to the small epidural space allowing the injectate to flow from C7-T1 to higher cervical levels. The use of intermittent fluoroscopy imaging is advised in cervical IL ESIs in view of possible gaps in the ligamentum flavum, advancement of the needle through a gap may result in spinal cord injury.28 Additionally, case reports have demonstrated intravascular venous uptake of contrast material despite negative aspiration in the lower cervical/upper thoracic spine from involvement of the posterior internal vertebral venous plexus, which drains the IL space and returns blood to the heart through the paired vertebral veins and bilateral brachicocephalic veins.29 Intravascular uptake can result in decreased efficacy and a theoretical risk for microinfarction.30
Thus, given potential risks of inadvertent spinal cord injury secondary to gaps in the ligamentum flavum, low sensitivity and poor negative predictive values of negative aspiration of blood, consideration to delay cervical IL ESI until ICM is available should be considered. Additionally, the use of paramedian/parasagittal approach in lumbar IL ESIs or use of US guidance to perform cervical TFESIs can be considered.
Recommendations
Given the current contrast shortage clinicians must weigh risks versus benefits of performing these procedures without contrast. Lumbar IL injections may be performed without contrast after careful consideration of the patient’s clinical presentation, urgency for treatment, and careful review of imaging.
Caution should be employed if considering lumbar TFESIs without the use of contrast given the increased risk of vascular compromise in addition to risk of intradiscal spread. If lumbar TFESI is performed without the use of contrast, use of non-particulate steroid is recommended. Non-particulate steroid is recommended for all cervical TFESIs with or without contrast. In addition, a fluoroscopic depth view (lateral or contralateral oblique) is advised.
Fluoroscopically guided cervical IL or transforaminal epidurals should be delayed until ICM contrast is available.
The lumbar paramedian/parasagittal approach, where contrast is not necessary, can be considered instead of TFESIs in patients with lumbar unilateral radicular pain.
If experienced with US-guided cervical procedures, one may consider US-guided cervical nerve root block instead of cervical transforaminal injection.
Can cervical facet interventions be performed without the use of contrast?
The recent international multisociety consensus practice guidelines on cervical facet interventions addressed the role of image guidance. They recommend that fluoroscopy or US (in providers with expertse) be used for cervical MBB. US can be useful in patients in whom radiation exposure may be associated with potential harm (this could apply also to this current contrast shortage).
It should be noted that while contrast agent utilization was recommended, this was not specifically mandated.31–33
If contrast has to be used for facet joint injections, it is recommended, based on studies, to use volumes <1.5 mL of intraarticular lumbar facet joints and <0.5 mL for lumbar MBB.34 For cervical facet joint, injection of <1 mL is recommended for facet joint (capacity of the joint is less than 1 mL) and <0.3 mL for cervical MBB.31
Recommendations
Given the current contrast shortage clinicians must weight risks vs benefits of performing these procedures without contrast. Cervical facet interventions may be performed without contrast after careful consideration of the patient’s clinical presentation, urgency for treatment, and careful review of imaging.
If contrast medium is deemed necessary, use the lowest possible effective dose based on currently published guidelines.
Alternatively, US guidance may be used when experience with this image modality is present. Non-particulate steroids are recommended in cervical facet joint injections.
Can alternatives to iodinated contrast such as gadolinium be used?
GBCAs have been suggested as an off-label alternative in patients with a history of a hypersensitivity reaction (HSR) to the ICM. To date, it is unclear if the use of GBCA have comparable diagnostic accuracy compared with ICM with studies offering conflicting results.35 36 A recent study demonstrated that the overall radiopacity of a majority GBCAs is less than that of iodinated contrast.37 Gadobutrol had the highest radiodensity secondary to its elevated gadolinium molar concentration. In comparison to iodinated radiographic contrast, gadobutrol’s radiographic contrast level was between isohexol 240 and 140 mg/mL in the 70–125 kVp range. However, it must be recognized that GBCAs with high molar concentrations of gadolinium are at increased risk for acute neurotoxicity with intentional or inadvertent intrathecal administration and greater care and smaller volumes should be considered for utilization. GBCAs are either linear or macrocyclic and further subdivided into ionic and nonionic based on their chelate structure11 (see table 1).
Gadolinium based contrast agents
Gadolinium is a toxic lanthanide element, its toxicity is mostly secondary to its interference with calcium ion channel processes.38 Thus, gadolinium is injected in its chelated form when used in medical imaging.39 The chelation is loose with the linear GBCAs while the binding is rigid with the macrocyclic agents. This explains the greater incidence of adverse events secondary to the freed gadolinium ion from intravascular administration of linear agents (nephrogenic systemic fibrosis, gadolinium brain deposition/retention)11 38 40–45 Most important, encephalopathy and death have been reported after unintentional intrathecal administration injection during interventional pain procedures.
Given the reports of adverse events,46 47 a multisociety working group published recommendations regarding the use of GBCAs in interventional pain procedures.48 The working group concluded that GBCAs are contraindicated in intrathecal (IT) injections. GBCAs should not be used in patients at increased risk of IT puncture. GBCAs should not be used in IL or TFESIs. GBCAs may potentially be used in procedures in which there is a low risk of IT injection including lumbar sympathetic blocks, facet joint injections, and MBBs after careful explanation to the patient of the risks and the off-label utilization. The group also recommend using the lowest possible dose of GBCA when necessary to achieve clinical information when necessary.48 A recent meta-analysis reviewed incidences of adverse outcomes following intrathecal administration of GBCA.49 In analyzing 53 studies comprizing 1036 patients, an adverse event rate of 13%, mostly due to postural headache was demonstrated. The review found intrathecal gadolinium to be relatively safe up to doses of 1 mmol, with serious neurotoxic adverse events occurring above 2 mmol. Serious neurological adverse events have been documented in several case studies (table 2).
Previous cases of intrathecal gadolinium neurotoxicity*
In their study of dural leaks, hydrocephalus, and cerebral spinal fluid (CSF) disorders (arachnoid cyst communications, aqueductal stenosis, obstruction of the fourth ventricle), radiologists intentionally inject gadolinium intrathecally. They inject small volumes (0.2–0.5 mL, not exceeding 1 mL), slowly (0.2 mL per second), and/or combine it with either CSF, normal saline or an ICM (eg, iodixanol).50 A prospective feasibility and safety glympathic imaging study in 100 patients concluded that 0.5 mL (1.0 mmol/mL) of gadobutrol (combined with 3 mL iodixanol) was safe.51
In summary, the administration of a GBCA via routes other than intravenous is an off-label use and that significant nervous system-related warnings are listed in the prescribing information.52 53 Second, specific formulations of GBCAs have differing chelating agents and concentrations of gadolinium (gadobutrol has the highest gd concentration per mL), meaning the toxicity profile of one type is not directly applicable to another. Based on published clinical reports of acute GBCA neurotoxicity, prospective safety studies, and reviews, physicians should stay below a gadolinium dose of 1 µmol/g brain (ie, theoretical number based on case reports and published animal data suggesting neurological risks)51 (figure 1).

Neurotoxic gadolinium concentrations in human and rat studies. Numerical values indicate gadolinium concentration in µmol per gram of brain. Human drawings indicate human studies, rat drawings indicate rat studies. Concentrations that did not induce neurological complications are shaded blue, while concentrations that induced neurological complications are shaded red. *A gadolinium concentration of 2.5 µmol/g brain did not induce neurological complications in two publications **But did induce neurological complications in one publication when the gadolinium was not injected over an extended period of time. ***Blue people 50 75–80. Red people 42–44 62–68 70–74. Rats 81–83.
Based on a theoretical dose limit of 1 µmol/g brain, restricted GBCA volumes would be feasible based on the GBCA’s gadolinium molar concentration. Specifically, GBCA volume limits could range between 1.4 mL (1 mol/L of gadolinium) to 5.6 mL (0.25 mol/L of gadolinium). Patel et al recommended similar dosing of no more than 1 mmol/g brain; GBCA concentrations of 0.25, 0.5 and 1.0 mmol/mL which would correspond to volumes of 4, 2, and 1 mL, respectively (table 1).49 An old study in rats showed that macrocyclic agents have lower median lethal dose (LD50) compared with linear agents. In spite of their findings, the authors concluded that the safety factor of the diagnostic dose is 80 when compared with the lethal dose.54 Translational and prospective studies are required to better understand the risk of GBCA neurotoxicity. Until further basic and clinical research is performed, GBCAs should not be considered a safe and viable alternative to iodine-based contrast.
Recommendations
GBCAs should not be used in spine-related procedures (IL ESIs or TFESIs) in the absence or shortage of ICMs.
Careful consideration should be taken in repeated use of GBCAs for non-spinal injections.
Are recommendations different in patients with a history of HSR to ICM?
Because of the above adverse events with a GBCA, especially encephalopathy after unintentional IT injection, physicians should not switch to a GBCA lightly. History of an ‘allergic reaction’ should be investigated. Patients often state that they had an ‘allergic’ or (HSR, the preferred term) when the symptoms are not specific (eg, headache, nausea). The practitioner should therefore ask the details of the patient’s reaction. Most HSRs are anaphylactoid, non-IgE mediated reactions. In patients with documented HSR, switching to another ICM and a premedication may be adequate in mild and moderate reactions. Patients with moderate or severe HRs should be ideally referred to an allergist. Studies showed that changing the ICM is as effective, if not better than premedication.55 Additionally, extravascular injection of the culprit ICM has been shown not to necessarily result in a breakthrough reaction, in patients with documented index reactions.56 57 In one study, none of 20 patients who had 45 extravascular injections (pancreaticobiliary tract, genitourinary, abdominal cavity, CSF, outline of fistula) of the culprit ICM developed a breakthrough reaction.56 In patients in whom the risk of IT injection is great, premedication, injecting a different ICM, vigilant monitoring for 2 hours may be considered instead of using a GBCA.
Recommendations
In perivertebral injections where intrathecal injection of gadolinium is possible and where contrast is absolutely necessary, the use of ICM may be considered in patients who had a history of HSR to an ICM even during the ICM shortage.
Can a single vial of ICM be used for multiple doses?
The Centers for Disease Control and Prevention (CDC) recommends use of single dose vials whenever possible. In cases where single-dose vials are not available or feasible, one can use multidose vials for a single patient that are stored according to manufacturer recommendations, outside of immediate patient care areas, with the initial access date clearly labeled, appropriate aseptic technique used for medication withdrawals as outlined by the CDC58 and US Pharmacopeia (USP).59 The CDC recommends that multidose vials should be dedicated to single patient use whenever possible. Moreover, the CDC states that the medication only be kept in a clean medication preparation area away from immediate patient care areas in order to prevent contamination of the vial through direct or indirect contact with contaminated surfaces or equipment.58 CDC recommends discarding multidose vials that have entered an immediate patient care area. Multidose vials are labeled by the manufacturer and usually contain an antimicrobial preservative to prevent the growth of bacteria.60
During medication shortages, clinicians may wonder about using a multidose vial for more than one patient in order to conserve ICM, however, physicians should avoid using accessing multidose vials for more than one patient. Pharmacists following specific guidelines may at times provide ICM for use in multiple patients during times of critical shortage. Consideration for splitting ICM into patient specific syringes is considered medium risk compounding according to the USP and if performed must follow the USP Pharmaceutical Compounding-Sterile Preparation Guidelines.59 Organizations considering dose splitting/repackaging should be aware of risks including the CDC Morbidity and Mortality Weekly Report report of bacterial infections following the use of a single container of contrast used for multiple patients.61 The ISMP highlights the necessity to handle repackaging/splitting doses in a pharmacy’s clean room61 in concordance with USP 797 standard of practice (USP 797) if a contrast injection system cannot be used.59 61
Recommendations
Multidose dose vials should be used for single patients whenever possible.
If a multidose vial is to be used for more than one patient it is imperative to follow the USP 797 standard of practice as well as CDC.
In addition, checking with state board of pharmacy or other regulatory body is recommended.
Conclusion
In summary, supply chain issues resulting in medications shortages are unlikely to resolve any time soon. Thus, we must be prepared to adapt while continuing to provide quality care to our patients.
A summary of the recommendations is included in figure 2.
{kind=link}
{kind=link}
Summary of ASRA pain medicine recommendations for interventional pain procedures during contrast shortage. ASRA, American Society of Regional Anesthesia; CDC, Centers for Disease Control and Prevention.
Data availability statement
No data are available. N/A.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to acknowledge Ann Snively for her help with the creation of the infographic included here as Figure 2.
References
Footnotes
Twitter @kohanlynn, @daveprovenzanomd, @amypearsonmd, @NarouzeMD
Contributors All authors contributed to the development, writing, and editing of the manuscript. LK is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests DAP is president elect of the ASRA Pain Medicine. He has consulted for Avanos, Boston Scientific, Heron, Medtronic, Nevro, SI Bone, and Wise. Pain Diagnostics and Interventional Care has received research support from Avanos, Boston Scientific, Medtronic, Nevro, Stimgenics, and Abbott. SN is president of the ASRA Pain Medicine.
Provenance and peer review Not commissioned; externally peer reviewed.