Article Text

Abstract
Background and objectives Documentation is important for quality improvement, education, and research. There is currently a lack of recommendations regarding key aspects of documentation in regional anesthesia. The aim of this study was to establish recommendations for documentation in regional anesthesia.
Methods Following the formation of the executive committee and a directed literature review, a long list of potential documentation components was created. A modified Delphi process was then employed to achieve consensus amongst a group of international experts in regional anesthesia. This consisted of 2 rounds of anonymous electronic voting and a final virtual round table discussion with live polling on items not yet excluded or accepted from previous rounds. Progression or exclusion of potential components through the rounds was based on the achievement of strong consensus. Strong consensus was defined as ≥75% agreement and weak consensus as 50%–74% agreement.
Results Seventy-seven collaborators participated in both rounds 1 and 2, while 50 collaborators took part in round 3. In total, experts voted on 83 items and achieved a strong consensus on 51 items, weak consensus on 3 and rejected 29.
Conclusion By means of a modified Delphi process, we have established expert consensus on documentation in regional anesthesia.
- nerve block
- regional anesthesia
- anesthesia
- neuraxial
- documentation
- minimum standards
- Delphi process
- international consensus
Data availability statement
Data are available on reasonable request. Any data not in the online supplemental information are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- nerve block
- regional anesthesia
- anesthesia
- neuraxial
- documentation
- minimum standards
- Delphi process
- international consensus
Introduction
Accurate and concise documentation is important for both healthcare delivery and medicolegal protection. Several international medical governing bodies place accurate record keeping as one of the fundamental requirements for good clinical care.1 2
Despite the increase in use of regional anesthesia, there is limited information regarding characteristics of effective documentation. This is in contrast to the wealth of documentation standards which exist for general anesthesia.3
The aim of this study was to establish a consensus opinion among a panel of international experts regarding the recommended components of documentation in regional anesthesia.
The recommendations contained herein do not define standard of care. They are not intended to replace clinical judgment. In the imperfect setting of heterogeneity of the data, limited data, controversial topics, and bias inherent to expert opinion, compliance with the recommendations may not result in improved outcomes compared with alternative therapies consistent with personalized medicine.
Methods
An international executive committee consisting of JLB, MJ, HMA, EMLM, and EV was created to design the format of the study. A modified Delphi methodology was chosen as it is a widely used systematic process for achieving consensus amongst a group of experts.4 For this study it was decided that a 3 round, prospective Delphi process would be used with 2 rounds of electronic voting and a final round consisting of a round-table discussion and live polling. A steering committee consisting of BPA and GCC was formed to facilitate the management of the Delphi process as well as analyze the results of the voting and communicate with the panel of experts.
Collaborator selection
One-hundred and three experts from North America (n=37), Europe (n=53), and Australasia (n=13) were invited to participate. All those invited were known to have extensive clinical, educational or research experience in the field of regional anesthesia. In addition, a medicolegal expert from the USA was included to advise on any legal implications arising from the consensus document but did not participate in the voting process.
Generation of the long list
A directed literature review was performed to create an exhaustive list of documentation components for performing a regional anesthetic. A MEDLINE search was conducted using the following terms: ‘regional anaesthesia documentation’, ‘peripheral nerve block documentation’, ‘consent for regional anaesthesia’, ‘regional anaesthesia litigation’, ‘documentation’, and ‘anaesthesia records’ yielding 63 potential documentation components. Following review and discussion by the executive committee, an additional 12 items were added to produce the final long list (online supplemental appendix 1).
Supplemental material
Modified Delphi process
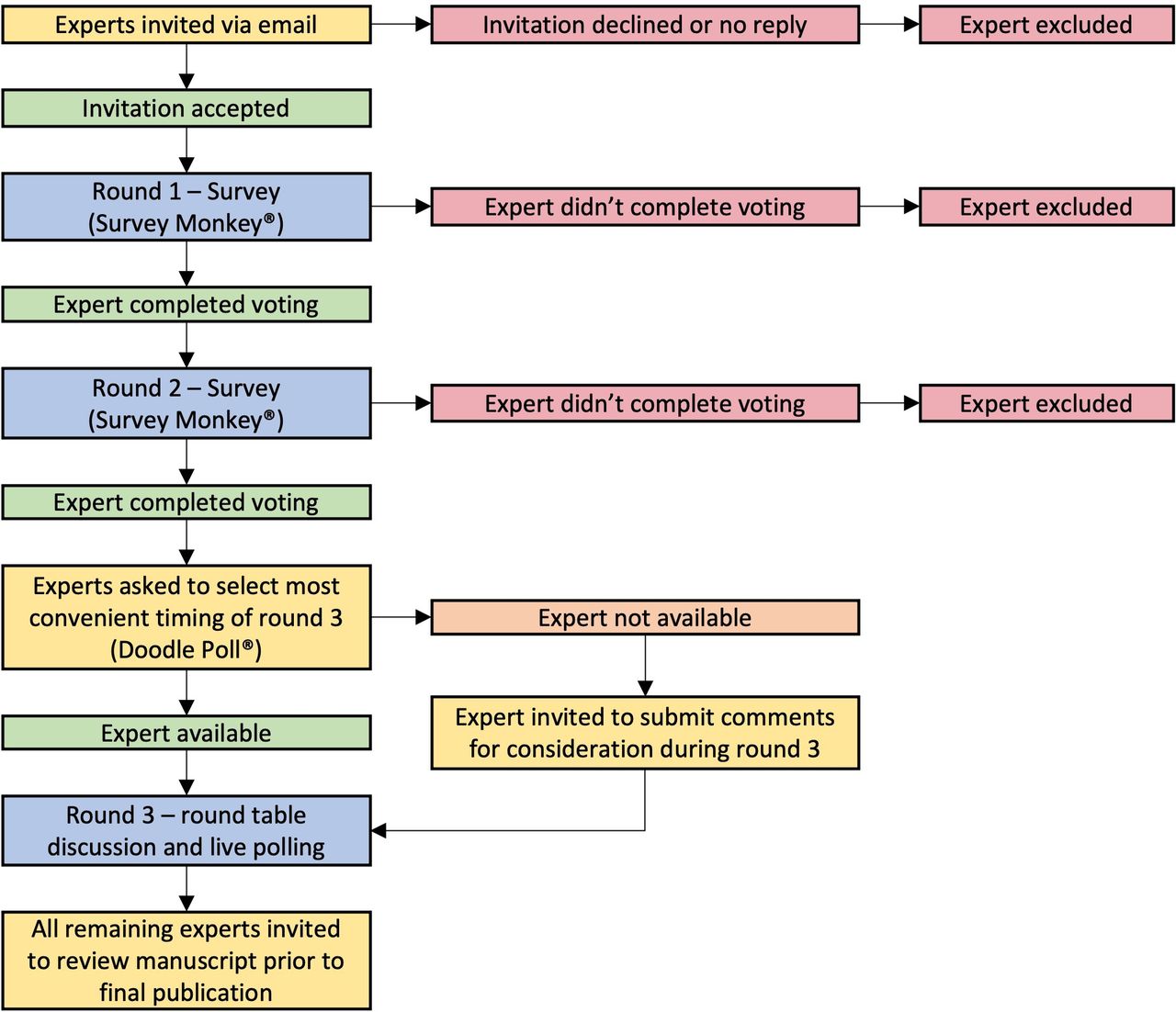
A modified Delphi methodology was chosen as it is a widely used systematic process for achieving consensus among a group of experts. It is characterized by the generation of a long list of items followed by multiple rounds of anonymous voting and feedback. For this study, all experts who had agreed to take part were invited to participate in 2 electronic voting rounds and a third virtual round table discussion with live polling (figure 1). Strict deadlines were imposed on collaborators to complete each round of the Delphi process within a prescribed timeline. Any collaborators who did not vote within the timeline were excluded from all subsequent rounds and were not included as an author on final publication.

Flowchart showing structure of Delphi process and progress of experts throughout the project.
In previous Delphi studies consensus has been defined as ≥75% agreement between collaborators.5 In this study, 50%–74% was deemed to be weak consensus, while ≥75% was agreed to be strong consensus. These ranges were used throughout the Delphi rounds to decide on each item’s progression and ultimate inclusion in the final list of suggested documentation components.
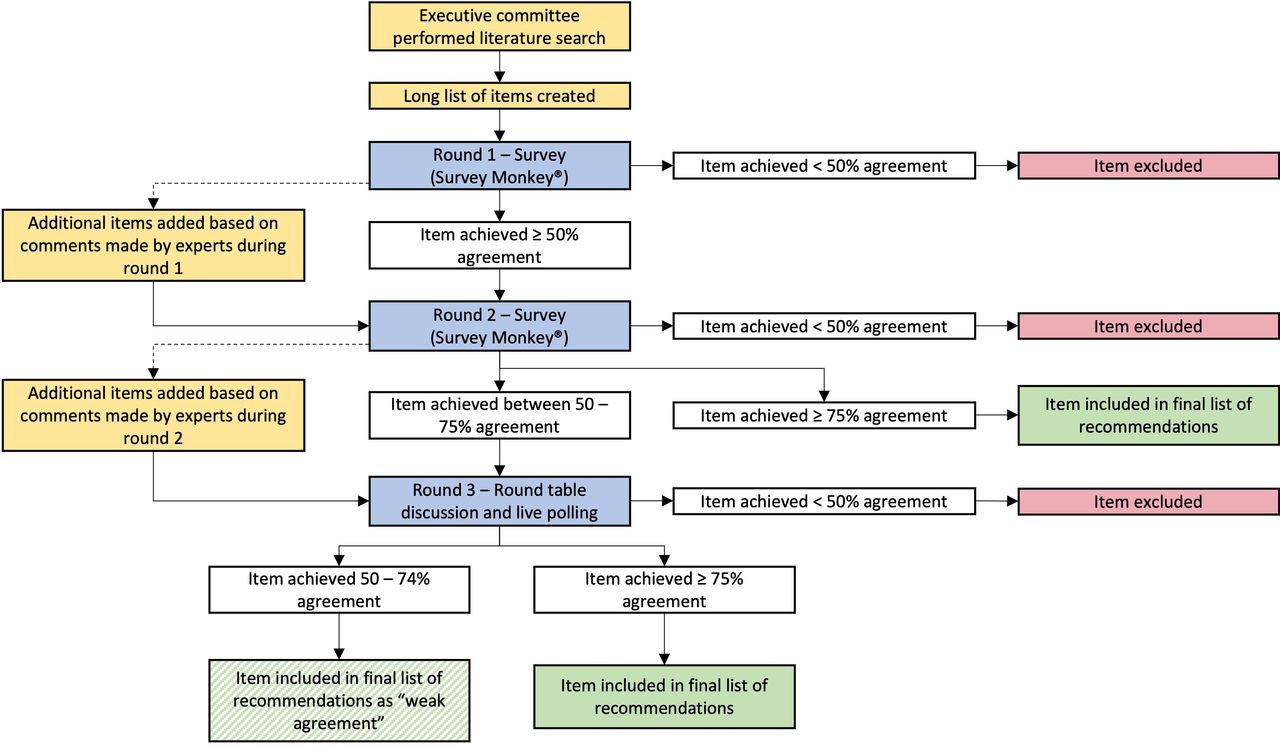
Rounds 1 and 2 were conducted using an online survey tool (Survey Monkey, Momentive, San Mateo, California, USA) distributed via email. Collaborators were asked to ‘agree’ or ‘disagree’ with each of the potential documentation components included in the long list. Commentary and suggestions for additional items were encouraged and were recorded via the same online tool. In round 1, potential documentation components achieving ≥50% agreement proceeded to round 2, while those with<50% agreement were excluded (figure 2). Following review of the comments made by the collaborators in round 1, some items were reworded or clarified, and any suggested additional items were included for round 2 voting.

{kind=link}
{kind=link}
Flowchart showing structure of Delphi process and progress of items throughout the project.
In round 2, items achieving ≥75% agreement were accepted into the final list of suggested documentation components, while those achieving <50% were excluded. Items with 50%–74% agreement proceeded to round 3 for further discussion. Based on comments made by collaborators in round 2, some items were reworded or clarified. Any suggested additional items were included for consideration in the round 3 live discussion.
Round 3 was conducted via online videoconferencing software with polling capabilities (Zoom, Zoom Video Communications, San Jose, California, USA). The study included collaborators from multiple countries spanning different time zones, therefore it was unlikely that all collaborators would be available at the same time to take part in the discussion. To decide on a time for round 3 to take place we used online meeting-scheduling software (Doodle, Zurich, Switzerland) to allow collaborators to pick preselected times which would suit their schedule. The most mutually convenient time was picked and circulated to the collaborators via email. Those collaborators unable to attend the live third round were invited to submit comments in advance of the meeting via another survey (Survey Monkey, Momentive, San Mateo, California, USA). A summary of the outcomes of rounds 1 and 2 was also distributed to all collaborators prior to the virtual discussion to avoid confusion about items previously excluded and allow for a more productive discussion. The meeting was co-chaired by EMLM and JLB, who facilitated discussion amongst collaborators via both electronic messaging and oral discourse. Strict adherence to time limits on discussion (5 minutes) and voting (1 minute) were enforced. All comments made by collaborators in absentia were displayed on-screen for participants during the discussion to ensure all opinions were considered prior to live polling. Items achieving ≥75% agreement were accepted into the final list of suggested documentation components. Those achieving 50%–74% were accepted as weak agreement, and those achieving<50% were excluded.
Results
One-hundred and three experts in regional anesthesia were invited to take part in the Delphi process. In total 79 agreed to participate (77%); 26 from North America (26/37, 70%), 40 from Europe (40/53, 75%) and 13 from Australasia (13/13, 100%). Seventy-seven collaborators who agreed to take part in the study (97%) completed both rounds 1 and 2. Fifty of the collaborators who originally agreed to take part in the study (65%) were available and took part in the round 3 virtual discussion. The median number of voters for each item in round 3 was 48 (range: 46–50).
Seventy-five potential items were included in round 1 of which 67 achieved ≥50% agreement and progressed to round 2. Eight items achieved <50% agreement and were excluded (table 1). Responses and collaborator commentary were collected, anonymized, and summarized by the steering committee and reviewed by the executive committee.
Items rejected from round 1
Following review, 15 of the items were reworded or clarified and an additional 6 items were added for round 2 (box 1).
Additional items added during rounds 1, 2 and 3
Items added for round 2
Grade of block performer (e.g. Consultant, Fellow, Resident, Registrar)
Name of supervisor (if applicable)
Name of assistant (if applicable)
Method used to secure catheter
Ultrasound image included in patient record (if ultrasound used)
Post block monitoring completed by ____ / handed over/off to ____ (e.g. Recovery, Post Anesthetic Care Unit (PACU))
Items added for round 3
Presence / absence of nerve swelling
Items added during round 3
Aseptic technique used as per local policy
All responses from round 2 were collected and summarized by the steering committee as in round 1. Seventy-three items were included in round 2, of which four did not achieve consensus and were excluded (table 2). Forty-five items achieved ≥75% agreement and progressed to the final list of suggested documentation components. The remaining 24 items achieved 50%–74% agreement and were therefore included in round 3 for further discussion. A single additional item was added for round 3 following review of the comments made by the collaborators during round 2 (box 1).
Items rejected from round 2
Twenty-five potential items were discussed and voted on in round 3. Five items achieved ≥75% agreement and were accepted to the final list of documentation components. Following an ad hoc vote by the collaborators, 4 items pertaining to the use of sterile technique (‘sterile gloves used’, ‘mask used’, ‘sterile ultrasound transducer cover used’ and ‘sterile drape used’), were combined into a single all-encompassing item: ‘aseptic technique used as per local policy’. This was added to the list of items to be voted on during round 3 and achieved 75% consensus and was duly accepted to the final list of suggested documentation components. Three potential components achieved only 50%–74% agreement and were included in the final list as weak agreement. Thirteen failed to achieve >50% agreement and were therefore excluded. It is worth noting that 4 of these were the individual items subsequently grouped together into a single documentation component relating to the use of sterile technique which was accepted.
In total 51 items achieved strong consensus (≥75% agreement), 3 achieved weak consensus (50%–74% agreement) and 29 were rejected (<50% agreement). A final list of the suggested documentation components for regional anesthesia is shown in table 3. A summary of all rounds of voting is provided in online supplemental appendix 2.
Supplemental material
Final list of recommendations
Discussion
This study is, to our knowledge, the first to attempt and to achieve an international expert consensus recommendation on documentation in regional anesthesia. Important work has been conducted previously in this area, however only at a national level.6 7 It is hoped that our work will facilitate local institutions in their efforts to support physicians with their documentation and quality improvement needs.
While the majority of the potential documentation components were identified in the literature review, several items were added for consideration due to their necessity in billing processes in privately funded healthcare systems. The significant variation in current documentation practices in different countries, in particular between privately and publicly funded healthcare systems, was a theme throughout the study. We encountered commentary in all Delphi rounds that some items required inclusion in certain countries to ensure payment for the performing anesthesiologist. These same items were deemed unnecessary by collaborators from health systems where documentation does not directly impact an individual clinician’s reimbursement. This issue is reflected in the voting patterns between the USA versus non-USA anesthesiologists (for full list of USA vs non-USA voting, see online supplemental appendix 3). Taking ‘surgeon request for regional anesthesia’ as an example, 78% of USA anesthesiologists agreed in round 1 that this item should be included as a documentation component versus just 22% of anesthesiologists located outside of the USA. Ultimately surgeon request for regional anesthesia was rejected in round 1 with only 38% agreement.
Supplemental material
We anticipated that collaborators might vote according to individual or local standards of practice rather than specifically the documentation thereof. This was an issue in round 1 and was reflected in the collaborator commentary which contained many comments to the effect of ‘I don’t use X technique’ or ‘X technique should no longer be used’ or ‘X piece of equipment is not available in my hospital’. An example which highlights this issue is the use of nerve stimulators. An item included in round 1 was ‘No Evoked Motor Response (EMR) <___mA (when applicable)’ which received numerous comments stating that collaborators were not clear what this meant, no longer use nerve stimulators or that the use of nerve stimulators does not improve the safety of nerve blocks. These comments were associated with collaborators voting ‘disagree’. Despite these comments and votes this item received sufficient agreement (71%) to progress to round 2. To clarify the item in round 2, we changed the wording to ‘No EMR <___mA (when applicable i.e. when nerve stimulator used)’. This item subsequently received 81% agreement in round 2. We clarified several other items with the phrase ‘if applicable’ or ‘if used’ and reiterated to the collaborators that the purpose of the study was to define recommended documentation components and not their personal practice.
It was found that a number of collaborators had voted against items being included as they would be found elsewhere in the medical record (e.g. patient date of birth, name, vital signs) and therefore would be an unnecessary duplication. This was mentioned particularly in the context of electronic medical records where a good deal of data entry is automatic rather than by direct human input. These systems, however, are by no means universally used. The executive committee agreed that for the purpose of creating an exhaustive list of suggested documentation components the issue of duplication should be ignored and addressed later by individuals or governing bodies designing documentation guidelines. To this end, we asked collaborators to visualize the regional anesthesia record document as a stand-alone ‘blank page’ in the absence of the rest of the patient’s record and other anesthesia documentation. Ultimately a significant number of the suggested items in the finalized list are documented elsewhere in the patient’s record independent of a regional anesthesia procedure. Thus, every item may not need to be included on the dedicated regional anesthesia record should it be documented elsewhere.
We have broadly divided our long list and the subsequent finalized list of suggested documentation components into 6 sections.
Patient information
The majority of items relating to patient information were accepted in the early stages of the Delphi process. ‘Patient age’ was excluded in round 1 on the grounds that ‘Patient date of birth’ is preferable as, unlike age, it is a unique patient identifier and can be easily used to calculate age if required. ‘Patient body mass index’ was excluded in round 2 for similar reasons in that it can also be easily calculated.
Procedure preparation
Identification of the block performer by name was accepted to the final list however the grade of the block performer, which was added for round 2, achieved only weak agreement (68%). Many collaborators felt that the name of the block performer would be sufficient information to identify the individual. The name of the supervisor (in the context of a trainee performing a procedure) was added and accepted to the final list in round 2. ‘Name of assistant’ was added and excluded in round 2 as it was felt that ultimate responsibility lay with the performing or supervising anesthesiologist and therefore the name of any assistants was not essential.
In response to numerous collaborator comments ‘Patient consent’ and ‘Individual risks of procedure discussed/documented’ were reworded in round 2 as ‘Documentation of patient consent as per local standards’ and ‘Documentation of individual risks of procedure discussed (as per local standards)’. It was felt it would be impossible to accurately capture the nuanced aspects of consent internationally, and therefore an open approach was applied to allow scope for local interpretation based on pre-existing standards and legal frameworks. Consent and risks, if discussed, should be documented.
Pre-anesthetic/block evaluation was reworded (from pre-anesthetic evaluation) as collaborators felt that this would be separate to a routine pre-anesthetic assessment and might include pre-existing neurology or deficits. ‘Pre-procedure diagnosis (post-operative pain management/surgical diagnosis)’ and ‘Indication for regional anesthesia (surgical anesthesia or analgesia)’ were considered by many collaborators to be interchangeable and as such only ‘Pre-procedure diagnosis (post-operative pain management/surgical diagnosis)’ was accepted following discussion in round 3. The recording of the patient’s pre-procedure and post-procedure Visual Analog Score (VAS) were rejected in round 1 as collaborators felt that while they might be of research interest, they were of limited clinical relevance.
There was detailed discussion around the inclusion of ‘Stop Before You Block (SBYB)’ and the World Health Organisation (WHO) Surgical Safety Checklist/time out. The SBYB campaign8 originated in the UK and has gained some international acceptance, however, as reported by many collaborators, it is not globally recognized and thus not used in all countries. While the WHO checklist is more widely used, the argument was made that this is performed prior to surgery and not necessarily prior to a block. This is important when regional anesthesia is not performed for surgical anesthesia e.g. labor epidural, or is performed outside the theater e.g. in a dedicated block bay. It was generally agreed that should a ‘stop’ moment occur it should be documented, however the precise format of this remains unclear and should be determined by local practices.
Consideration of the patient’s coagulation status (‘Coagulation considered’) was accepted with weak agreement. Many collaborators commented that while it should be considered, it was not necessary to document it separately as it forms part of the routine pre-anesthetic/block assessment.
Procedure performance
As previously discussed, 4 items in the original long list relating to aseptic technique were combined into a single item, ‘aseptic technique as per local guidelines’, which was accepted.
Documentation specific to peripheral nerve block procedures
‘Side of Block’ was accepted to the final list, however, documentation of ‘Block side marked’ was excluded in the final round-table discussion, as it was felt to be repetitive and was adequately addressed elsewhere fe.g. by SBYB or a similar stop-moment.
The commentary surrounding the documentation of nerve stimulator technique is perhaps a reflection of changes in regional anesthesia practice; a number of collaborators stated they were not familiar with, or no longer used, several of the techniques described. ‘No EMR <____mA (when applicable i.e. when nerve stimulator used)’ and ‘Minimum current and current duration (when applicable i.e. when nerve stimulator used)’ progressed to the final list. ‘Description of quality of paresthesia’ and ‘Description of motor response’ were rejected on the basis that if a nerve locating method was used and a defined end point reached such as paresthesia or muscle contraction, that a description of this was too much detail. ‘Catheter tip location confirmed by ultrasound/nerve stimulator’ and ‘Technique of injection (via needle or catheter)’ were also rejected due to perceived excessive detail without providing additional information. ‘Note on incremental injection’ was rejected on the basis that while incremental injection techniques are advocated, it need not be documented. ‘Extra neural spread visualized’ and ‘Presence/absence of nerve swelling’ were also discussed and ultimately rejected, with several collaborators making the point that nerve swelling/extraneural spread themselves were not reliable signs relating to nerve injury. ‘Note on resistance to injection<15 psi’ was rejected on the basis that the majority of the expert panel did not have manometry available nor routinely measure injection pressures with some citing a lack of evidence for its benefit.
Documentation specific to neuraxial nerve block procedures
All but one of the items specific to neuraxial anesthesia were accepted to the final list. ‘Method used to secure catheter’ was added for round 2 following review of commentary and was rejected. ‘Epidural test dose given’ and ‘Dermatomal level of spinal or epidural block achieved’ were clarified in round 2 with ‘if applicable’, acknowledging that many anesthesiologists choose not to give a test dose, and that dermatomal levels may not be tested prior to the start of surgery or general anesthesia.
Post procedure
‘Inclusion of ultrasound image in block note’ was added for round 2 based on comments made during round 1. This proved to be somewhat contentious with many remarking that while it would be ideal to have ultrasound images in the patient’s record this comes with significant logistical issues, offers no safety benefit and even in medicolegal situations a single static image is of little use. There was a significant divide between USA and non-USA votes on this item, with 82% of USA voters agreeing to this standard in round 2 versus just 25% of non-USA voters. It was ultimately rejected however it will be interesting to see how this evolves in the future; the inclusion of images in the patient’s notes has become common practice among laparoscopic surgeons and endoscopists amongst others.
With regard to adequacy of the block for surgery, it was acknowledged that not all blocks are used for surgical anesthesia, and perhaps this item should have been altered to reflect this. Other collaborators made the point that a partial block requiring supplementation is not necessarily a failed block. ‘Post-block monitoring completed by ______/ handed over/off to ______(eg, recovery, PACU)’ was rejected as it was felt that this was beyond the scope of the project.
This study has several strengths. Seventy-seven international experts participated in the study exceeding the median number of 17 participants in other Delphi studies reported in the literature.4 A large number of experts were deliberately sought to minimize individual bias and provide a broad international perspective on this nuanced area. There was an excellent response rate with all 77 collaborators participating fully in the first 2 rounds and 50 taking part in round 3 despite the scheduling challenges associated with timezones. Voting anonymity was maintained throughout all rounds reducing the impact of dominant individuals, peer pressure, bias and to allow consideration of all opinions in a non-adversarial manner. Collaborator commentary was permitted and encouraged throughout the project allowing for a dynamic long list of suggested documentation components. Items could be added and/or revised based on collaborator commentary; this was well demonstrated during the round 3 live discussion where 4 items were consolidated into a single all-encompassing item in response to real-time collaborator discussion. This flexibility yielded a more comprehensive final long list of suggested documentation components that reflects the varied practice of regional anesthesia world-wide.
This study also has a number of limitations. While the expert panel was international, the majority of the collaborators were from Europe, followed by North America, and with a small number from Australia, New Zealand and Singapore. Our panel did not include any collaborators from South America, the Middle East, Asia or Africa, nor were there representatives from low- and middle-income countries. Thus, our suggested documentation components may not be applicable in these contexts. A limitation of all Delphi studies is that any expert panel will be influenced by their own experience and personal practice, however as previously mentioned, the large number of experts in this project should minimize this effect. Another potential limitation arises from the small number of prior studies in this area. As a result, the long list formulation required significant input from the executive committee to generate what was felt to be complete list of documentation components. Twelve additional items were added to the long list originally derived from the literature review, and a further 8 were added during the Delphi process, which could represent a source of bias.
The practice of regional anesthesia is constantly evolving and as such this list of suggested documentation components requires regular review to remain current. It is hoped that this list might provide a framework for international regional anesthesia societies to produce guidelines for documentation standards in the near future. There is no single global standard of care. The practice of medicine and regional anesthesia vary dramatically across the world and documentation should rightly reflect local best practice.
Concerning areas for future research, these may include the formation of a standard block procedure note template for both electronic and paper medical records and standardizing post-block monitoring and follow-up documentation for regional anesthesia procedures including inpatient and ambulatory nerve catheters. Another evolving area that warrants future study is the utility of including digital ultrasound media within the patient’s record should this practice become more widespread.
The authors acknowledge that while attempts to improve documentation standards are necessary and well-intended, an excessive burden of notes may distract from patient care and can even lead to physician burnout.9 Although the final list of recommendations may seem extensive the majority will already be included in the routine documentation practice of most anesthesiologists. This is not intended to be an exhaustive list nor a legal standard of documentation but rather a consensus of useful items to document patient care.
Conclusion
By means of a modified Delphi process we have established an expert panel consensus on documentation in regional anesthesia. We hope adoption of our recommendations will facilitate physician workflow, education, quality improvement and research.
Data availability statement
Data are available on reasonable request. Any data not in the online supplemental information are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Institutional ethics committee approval was deemed unnecessary by Letterkenny University Hospital Ethics Committee in December, 2020.
Acknowledgments
This paper is supported by the ASRA Pain Medicine and the ESRA board of directors.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
HMA, BPA and GGC are joint first authors.
Twitter @HassanM31118046, @sanjibadhikary, @DrEAlbrecht, @janboublik MDPhD, @AlwinChuan, @DanDirzu, @dr_rajgupta, @hdhardman_david, @HlasnyJakub, @rljohnsonmd, @TheLansdowns, @claralexlobo, @ajrmacfarlane, @PeterMerjavy, @PetermoranPeter, @amit_pawa, @PerlasAnahi, @KristopherSchr6, @garyschwartzmd, @ESchwenkMD, @LouiseMoran75
Contributors Study conception and design: HMA, BPA, GGC, JLB, MJ, EV, EMLM and AKW. Study conduct: HMA, BPA, GGC, JLB, MJ, EV and EMLM. Data analysis: BPA and GGC. Manuscript preparation: HMA, BPA, GGC, JLB, MJ, EV and EMLM. Manuscript revision: all authors. Manuscript approval: all authors. Manuscript guarantor: EMLM
Funding The authors received a grant towards the cost of open access from The European Society of Regional Anaesthesia and Pain Therapy
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.