Article Text

Abstract
Background The past two decades have witnessed an epidemic of opioid use disorder (OUD) in the USA, resulting in catastrophic loss of life secondary to opioid overdoses. Medication treatment of opioid use disorder (MOUD) is effective, yet barriers to care continue to result in a large proportion of untreated individuals. Optimal analgesia can be obtained in patients with MOUD within the perioperative period. Anesthesiologists and pain physicians can recommend and consider initiating MOUD in patients with suspected OUD at the point of care; this can serve as a bridge to comprehensive treatment and ultimately save lives.
Methods The Board of Directors of the American Society of Regional Anesthesia and Pain Medicine, American Society of Anesthesiologists, American Academy of Pain Medicine, American Society of Addiction Medicine and American Society of Health System Pharmacists approved the creation of a Multisociety Working Group on Opioid Use Disorder, representing the fields of pain medicine, addiction, and pharmacy health sciences. An extensive literature search was performed by members of the working group. Multiple study types were included and reviewed for quality. A modified Delphi process was used to assess the literature and expert opinion for each topic, with 100% consensus being achieved on the statements and each recommendation. The consensus statements were then graded by the committee members using the United States Preventive Services Task Force grading of evidence guidelines. In addition to the consensus recommendations, a narrative overview of buprenorphine, including pharmacology and legal statutes, was performed.
Results Two core topics were identified for the development of recommendations with >75% consensus as the goal for consensus; however, the working group achieved 100% consensus on both topics. Specific topics included (1) providing recommendations to aid physicians in the management of patients receiving buprenorphine for MOUD in the perioperative setting and (2) providing recommendations to aid physicians in the initiation of buprenorphine in patients with suspected OUD in the perioperative setting.
Conclusions To decrease the risk of OUD recurrence, buprenorphine should not be routinely discontinued in the perioperative setting. Buprenorphine can be initiated in untreated patients with OUD and acute pain in the perioperative setting to decrease the risk of opioid recurrence and death from overdose.
- pain
- postoperative
- analgesics
- opioid
- opioid-related disorders
- pain management
- pharmacology
Data availability statement
All data relevant to the study are included in the article.
Statistics from Altmetric.com
Introduction
Currently, opioid use disorder (OUD), involving both prescription opioid medications and illicit opioids, is a public health crisis in the USA, having reached epidemic proportions in the past several years.1 A recent national survey estimates that at least 2.5 million people in the USA have OUD.2 Previous models of OUD treatment, primarily focused on psychosocial counseling and behavioral treatments, have been strengthened by the addition of pharmacological therapies in association with these psychosocial treatments; this was formerly referred to as medication-assisted treatment (MAT) and is now known as medication treatment of OUD (MOUD).3 MOUD has been studied at length, and there is strong evidence demonstrating improved outcomes, increased retention in treatment, and decreased morbidity and mortality in the OUD population treated with this therapy.4
Given these benefits, expansion of access to MOUD critically decreases morbidity and mortality from OUD and associated medical problems,5 with positive downstream effects on healthcare resources and society. Unfortunately, despite the opioid epidemic having been declared a national emergency in October 2017, a significant treatment gap remains between the number of patients diagnosed with OUD and those receiving MOUD. This reasons for this gap are complex and include multiple barriers, including stigma, an insufficient number of buprenorphine prescribers available to provide outpatient treatment,6 inadequate insurance coverage, and low payor compensation. The COVID-19 pandemic has posed unique and dangerous challenges for patients with OUD, including higher OUD recurrence rates, more overdose fatalities, and worsening barriers to care.7 The US Centers for Disease Control and Prevention (CDC) reported that over 81 000 drug overdose deaths occurred in the 12 months preceding May 2020, representing the highest number of overdose deaths ever recorded in a 12-month period.8
Now more than ever, physicians, including anesthesiologists and acute pain specialists, should consider MOUD for patients with OUD.
The current definition of addiction as stated by the American Society of Addiction Medicine (ASAM) is as follows:
[Addiction is] a treatable, chronic medical disease involving complex interactions among brain circuits, genetics, the environment, and an individual’s life experiences. People with addiction use substances or engage in behaviors that become compulsive and often continue despite harmful consequences.9
Although the definition of ‘addiction’ has evolved over time, the most current clinical nomenclature for a substance-related addictive disorder is ‘substance use disorder’ (SUD), where the term ‘substance’ is replaced by the actual substance of abuse (eg, alcohol use disorder, cocaine use disorder, etc). According to the most recent edition of the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders,10 each SUD is defined by 11 criteria divided into 4 categories. The criteria for OUD are shown in box 1.
American Psychiatric Association criteria for OUD
Impaired control:
Opioids are often taken in larger amounts or over a longer period than was intended.
There is a persistent desire or unsuccessful efforts to cut down or control opioid use.
A great deal of time is spent in activities necessary to obtain the opioid, use the opioid, or recover from its effects.
Craving, or a strong desire or urge to use opioids.
Social impairment:
Recurrent opioid use resulting in a failure to fulfill major role obligations at work, school, or home.
Continued opioid use despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the effects of opioids.
Important social, occupational, or recreational activities are given up or reduced because of opioid use.
Risky use:
Recurrent opioid use in situations in which it is physically hazardous.
Continued opioid use despite knowledge of having a persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by the substance.
Pharmacological criteria:
Exhibits symptoms of tolerance (reducing effect with increasing dose).*
Exhibits symptoms of withdrawal (physiological symptoms due to absence of a substance typically used repeatedly).*
A patient must meet at least one of the pharmacological criteria in addition to at least one other criterion from another category to be diagnosed with an OUD. Meeting two to three criteria constitutes mild OUD, four to five is moderate, and six or more is defined as severe. The severity of the disorder may have implications for treatment.10
Prevention efforts and treatment approaches for SUDs are generally as successful as those for other chronic diseases,11 which is important to highlight when combating stigma. Clinicians are responsible for treating common chronic diseases; unfortunately, despite estimates that SUDs affect >20 million American adults at some point in their lives,2 many clinicians do not have significant training or experience in the treatment of SUDs. In this context, it is critical that more frontline physicians are trained in at least diagnosis (if not basic treatment) of SUDs. Doing so will provide vulnerable individuals with appropriate care and/or expeditious referral to a physician with appropriate credentials and knowledge of ancillary resources. In addition, the chronic and relapsing/remitting nature of OUD indicates that lifelong treatment is often needed to care for patients adequately.
From the standpoint of physicians who specialize in anesthesiology and pain management, some evidence demonstrates that prescription opioid exposure in both the perioperative and chronic pain settings has contributed to increased incidence of both persistent opioid use and possible OUD.12 13 However, recent evidence does not suggest a linkage in opioid-naïve patients undergoing total knee arthroplasty.14 In those who have been diagnosed with OUD, treatment of pain with most full opioid agonists, such as oxycodone or morphine, puts already vulnerable patients at risk for recurrence or worsening of their active OUD.12 13
US Food and Drug Administration (FDA)-approved medications for OUD include methadone, buprenorphine, and naltrexone, all of which have been found to be similar with respect to effectiveness,15 16 with the caveat that the efficacy of naltrexone is comparable (in the short term) only if patients withdraw and abstain from opioid use for 7–10 days prior to initiation of therapy. Of these, only methadone and buprenorphine are opioid agonists, meaning that there is potential for benefit from the standpoints of both craving, withdrawal suppression, and analgesia with both medications.15 A Cochrane meta-analysis found no significant differences in retention in treatment between buprenorphine and methadone at medium or high doses.17 However, a recent National Institute on Drug Abuse study found a higher rate of retention in treatment for methadone, while urine-confirmed abstinence was similar between the two groups.18
Methadone, when prescribed for OUD, is challenging to manage. Methadone for treating OUD must be dosed daily at a specialized facility, referred to as an opioid treatment program or ‘methadone clinic’, and which requires special licensure to operate.19 In addition, methadone may increase the risk of overdose if the dose is raised too quickly or combined with other illicit drugs before tolerance has fully set in.20 On the other hand, for the reasons indicated shortly hereafter, the partial agonist buprenorphine can be safely and effectively prescribed by many physicians in office-based settings.21 Currently, prescription of buprenorphine, unlike methadone, does not require dispensing in a clinic requiring a special regulatory license, alleviating a significant barrier for physicians. However, buprenorphine prescription does require applying for an x-waiver (if treating >30 patients in the first year) or a notice of intent (NOI) to obtain an x-waiver without training, which will be further explained below.3 19 Furthermore, buprenorphine can be prescribed discreetly in an office setting, diminishing the stigma and social barriers that may be associated with methadone clinics.19
In the perioperative setting, where acute pain is more likely, methadone’s long half-life carries additional risk factors, including respiratory depression,22 which weighs against its use as a first-line opioid to be initiated in the setting of acute pain. In addition, while methadone is the primary pharmacological treatment for OUD in the USA, access to methadone is restricted by federal law (The Narcotic Addict Treatment Act of 1974) to highly regulated treatment programs.19 Buprenorphine may also decrease respiratory rate; however, the decrease is usually not clinically significant.23 The pharmacological profile of buprenorphine includes low intrinsic activity toward mu receptors; in addition, buprenorphine is a partial mu agonist at the mu receptor. Because methadone is a full mu agonist, it carries more potential for misuse and less protection from overdose compared with buprenorphine.16 Clinicians should also be aware that QT-interval prolongation and serious cardiac arrhythmias (eg, torsades de pointes) have been reported with methadone.24 The respiratory depressant effects of methadone persist longer than its analgesic effects. The terminal elimination half-life of methadone also has considerable interindividual variability, generally reported as 8–29 hours, but values have ranged from 9 to 87 hours in postoperative patients, from 8.5 to 75 hours in opiate-dependent patients, and up to 120 hours in outpatients receiving therapy for chronic malignant pain.24 Because of its unique pharmacological properties, buprenorphine has potential advantages over methadone for OUD, including less sedation, fewer withdrawal symptoms, and lower risk of toxicity at higher doses.19
Ultimately, the choice to initiate buprenorphine, methadone, or naltrexone for OUD should be made collaboratively with the patient and care team and be consistent with the patient’s goals. This paper does not seek to advocate for one form of MOUD over another. However, while methadone and naltrexone are viable options for MOUD, a full discussion of these medications is beyond the intended scope of this document.
The purpose of this multisociety collaborative document, based on literature review and expert opinion, is to serve as an educational resource for physicians focused on recognizing and managing OUD in the perioperative period. Specifically, the document will provide information on buprenorphine pharmacology, the perioperative management of patients on buprenorphine for OUD, and the advantages of initiation of buprenorphine postoperatively in patients with suspected OUD. This document is not intended to serve as a comprehensive guideline for treatment of OUD. We recognize the many challenges of co-managing pain and OUD in hospitalized patients. Since anesthesiologists and pain physicians knowledgeable about opioid pharmacology and management, we are uniquely poised to lead collaborative efforts to adequately treat OUD and acute pain. After hospital discharge, identification of and collaboration with outpatient providers may permit patients with OUD to receive immediate and sustained treatment in the community from appropriately trained clinicians, enabling services that promote best practice, encourage retention in treatment, and reduce OUD recurrence risk, overdose, and possibly death. Accordingly, trying to establish a ‘hand-off’ to an appropriately trained and experienced outpatient prescriber is preferred. While immediate lack of such services (eg, ‘hand-off’) should not uniformly prohibit the initiation of buprenorphine in patients with OUD experiencing acute pain, lack of prospective trials in this arena necessitates use of clinical judgment and comfort.
Methods
A multisociety working group to develop guidance for anesthesiologists and pain physicians on managing patients with OUD was convened after approval from the American Society of Regional Anesthesia and Pain Medicine Board of Directors in early 2020. Societies with a vested interest in OUD and pain medicine were identified and formal request-for-participation letters were sent to each society, who all approved involvement. Each society selected one or two members to serve on the working group based on their expertize, clinical experience, and academic interests (see online supplemental appendix A for a list of participating societies and representatives). While the majority of the members have backgrounds in anesthesiology and/or pain medicine, 4 members (of the 10-member working group) carry active board certification in addiction medicine, including one representative from the ASAM.
Supplemental material
The multisociety working group, later known as The Substance Use Disorder Ad Hoc Working Group, was tasked with the common goals of (1) identifying the need for perioperative guidance on management of buprenorphine for MOUD for anesthesiologists and pain management physicians; (2) providing an overview of basic pharmacology of buprenorphine and review of legal prescribing requirements; and (3) developing recommendations on the management or initiation of buprenorphine in patients with OUD in the perioperative period. Pertinent questions and a proposed format were developed by the multisociety working group chair based on input from the group members and modified during video conference calls.
Once consensus was reached on a topic, the multisociety working group chair performed edits, and the section was sent to the entire group for further review and correction. At onset, the multisociety working group decided that ≥75% agreement was required for consensus, although 100% consensus was achieved for all recommendations. After the multisociety working group completed the recommendations, the document was sent to the boards of directors of each society for approval. The document was subsequently edited based on feedback from individual societies.
Search engines used during the compilations of literature included PubMed, Google Scholar, MEDLINE, and Cochrane Database of Systematic Reviews, as well as the reference section of certain manuscripts. Search terms included buprenorphine, MOUD, MAT, OUD, perioperative, buprenorphine initiation, and x-waiver. Guidelines from organizations and institutions, such as the Vermont guidelines and ASAM were reviewed. Articles were also evaluated and screened by the multisociety working group for relevance. There were no limitations in the types of articles that were used to develop the recommendations, but the quality of each piece of evidence was evaluated by one or more members of the group.
A modified Delphi process was used to tabulate comments, incorporate recommended changes, and compile the answers towards consensus over a series of nine conference calls. Recommendations were graded on a scale from A to D or as insufficient according to the United States Preventive Services Task Force grading of evidence guidelines with the level of certainty graded as high, medium, or low (tables 1–3).25 This grading system was chosen based on its use in numerous pain management guidelines26–28 and its flexibility, which allows for high-grade recommendations in the absence of level 1 studies and for multiple grades of recommendations.29
Levels of evidence for guidelines and recommendations
What the grades of evidence mean and suggestions for practice
Levels of certainty regarding net benefit
Rationale for OUD treatment
Increased education is warranted for anesthesiologists and pain physicians to recognize and treat OUD
Medical management of OUD saves lives.30 Despite access to effective screening and treatment tools, rates of opioid-related hospitalizations and deaths from opioid overdose continue to rise.31 The National Academies of Sciences, Engineering, and Medicine recently published Medications for Opioid Use Disorder Save Lives, a report on the importance of MOUD. The report emphasized barriers to greater use of MOUD including stigma, inadequate education, and restrictive regulations.30 Stigma against those with OUD is common within the healthcare setting32 and fewer than 10% of physicians have completed the previously required training to prescribe buprenorphine.33
Lack of sufficient clinical training to provide care for patients with OUD is also a significant barrier. Medical schools and residencies often do not provide training in managing OUD. As of 2008, only 12 medical schools required a separate SUD course, while 45 offered it as an elective.34 Studies suggest that early training in evidence-based treatment is associated with higher confidence and willingness to provide OUD treatment.35 Thus, it has been reported that one of the most effective strategies for addressing the treatment gap may be to require healthcare professionals to be trained in the screening, diagnosis, and treatment of OUD and that such training should not be specialty specific.32 The National Academy of Medicine (NAM) therefore recommends that accreditation agencies require clinicians receive training in OUD.32
An additional barrier is insufficient coordination of care among specialists.35 Interprofessional collaboration between practitioners of anesthesiology, chronic pain, surgery, primary care, and addiction medicine, along with frequent communication, are likely to improve both outcomes in care and patient satisfaction.36 The NAM report calls on all clinicians to receive education and training and to work together to combat the devastating consequences of OUD.32 Anesthesiologists can heed this call to action and play a leading role in treating patients with OUD.
Insurance and payor barriers are also significant; insurance plans may not cover or may require preauthorization for coverage of OUD medications.36 Advocacy work needs to continue to reduce these barriers. A full discussion of payor coverage limits is beyond the scope of this article.
Importantly, patients may report an interest in starting MOUD in the hospital setting.31 To be most effective, however, systems promoting ongoing, long-term care with MOUD after hospitalization are needed, and these may be most effectively provided by an outpatient physician experienced in OUD management. Several studies have shown that hospital-based OUD treatment with ongoing treatment after discharge is effective in terms of increasing entry into treatment, improving retention in treatment, increasing completion of hospitalization, and reducing opioid use and readmission.31 37
Hospitalization has been found to provide a teachable moment for initiating OUD care.38 Thus, anesthesiologists and pain physicians are in a unique position to help identify, treat, and/or refer perioperative patients with OUD. While the number of patients with SUD presenting in the perioperative period is unknown, approximately 10%–30% of hospitalized patients have an untreated non-alcohol SUD.39 Untreated SUD often complicates the inpatient course secondary to poor adherence to medical treatment plans, withdrawal, and early cessation of appropriate treatment (as one-third of patients with SUD leave against medical advice).19 40 Additionally, the economic and societal impact of untreated SUD is staggering.41 42 Furthermore, death rates among patients with OUD are highest (31.7 per 1000) within the first month following a hospital discharge.43 Starting buprenorphine has been found to be one of the most effective ways to save lives; the number need to treat to prevent one death with buprenorphine is <3.44 Larochelle et al also reported buprenorphine treatment was associated with a 37% reduction in all-cause mortality during the year following a non-fatal overdose.44 This mortality reduction is larger than the reduction in mortality associated with treatment with any blood-pressure medication, diabetic medication, or statin, and also larger than the reduction associated with aspirin after an ST-segment elevation myocardial infarction.45
Anesthesiologists and pain physicians can help lead efforts to screen, intervene, and initiate MOUD, and refer patients to ongoing community-linked treatment. Given the high mortality and the scarcity of outpatient resources for OUD treatment, it is important to recognize and treat OUD among perioperative patients. Although coordinating adequate outpatient follow-up, insurance coverage, and discharge planning is preferable, these should not be absolute requirements for initiation of this critical medication during a hospitalization, given some evidence that short-term exposure may reduce mortality,46 decrease presence of illicit substances,46 and be beneficial from a harm reduction standpoint,44 even when long-term follow-up is not available. Establishing inpatient collaboration and alliances with community programs and outpatient primary care practices can assist in streamlining care after hospital discharge. The recently reduced barriers to buprenorphine prescribing may assist in this process, as innovative methods to increase the ability to assist patients with OUD are urgently needed. Universal SUD screening can be integrated into the perioperative space, and physicians can be educated in the basics of addiction medicine, diagnosis of SUD, basic pharmacology, and multidisciplinary SUD treatment approaches.32 In addition, barriers to treatment access can be explored and addressed. Education, awareness, and empathy are key to decreasing the stigma of this treatable disease. In addition, physicians play an integral role in decreasing rates of OUD by collaborating with and educating the surgical team and other inpatient colleagues.
Summary
Levels of OUD are high in the USA; thus, anesthesiologists and pain physicians will encounter patients with treated and untreated OUD within the perioperative period. The NAM encourages all physicians to screen for and treat OUD. Anesthesiologists and pain physicians can play an integral role in leading efforts to screen and treat OUD within the perioperative period.
Pharmacology
There are three FDA-approved medications for the treatment of OUD (table 4).47–52 This manuscript will focus on the use of buprenorphine in the treatment of OUD.
Opioid use disorder (OUD) medications39–43 47
Buprenorphine is a long-acting, mixed opioid agonist and antagonist that can lower the potential for misuse of opioids, diminish withdrawal symptoms and cravings, and offer protection in overdose situations.20 Its antagonistic properties provide safeguards against respiratory depression and diminish the euphoric effects of short-acting opioids.53 Buprenorphine is available as a single agent or in combination with naloxone. Naloxone is combined with buprenorphine to serve as a deterrent to injection use; naloxone taken orally or sublingually has low pharmacological activity.54 Buprenorphine is available in multiple dosage forms and requires special consideration when selecting a formulation or transitioning to a different dosage form. When indicated for the treatment of chronic pain, buprenorphine is available in a twice daily buccal film or weekly transdermal patch. When indicated for the treatment of OUD, buprenorphine is approved for use parenterally as an extended-release subcutaneous injection and sublingually as a tablet or film (as a single agent or in fixed combination with naloxone) (tables 5 and 6). While manufacturers and experts historically have preferred the use of buprenorphine alone for induction, comparative evidence is lacking and either formulation (buprenorphine with or without naloxone) may be used.55 Buccal as compared with sublingual administration results in greater bioavailability of naloxone, which may precipitate withdrawal symptoms on induction. Therefore, when the combination of buprenorphine/naloxone is used, sublingual application of the buprenorphine/naloxone film is preferred for minimizing exposure to naloxone and reducing the risk of withdrawal during induction therapy.55
FDA-approved buprenorphine formulations for MOUD and analgesia50
Buprenorphine dosage formulations
Unfortunately, there is often confusion associated with the pharmacological properties of buprenorphine, most notably with regard to its analgesic potential. Specifically, buprenorphine is often mistakenly thought of as a weak analgesic.56 It is also often feared that buprenorphine will reduce the effectiveness of full mu opioids resulting in inadequate analgesia. Buprenorphine was, in fact, originally developed as an analgesic.57 Some clinical studies report that buprenorphine has similar or greater analgesic efficacy and antihyperalgesic effects as full mu-opioid receptor agonists.58–61 With regard to receptor binding, when buprenorphine is administered in maintenance doses typically prescribed for the treatment of OUD, mu-opioid receptors may still be available for binding of full mu agonists, although more pharmacological data and studies are needed.
Summary
Various buprenorphine formulations are FDA-approved for either the treatment of OUD or pain. Buprenorphine formulations that are FDA-approved for the management of OUD are available only in milligram dosing while formulations approved for analgesia are available only in microgram dosing. Buprenorphine is a potent analgesic despite being a partial mu-opioid receptor agonist. While buprenorphine has a strong affinity for the mu-opioid receptor, opioid receptors remain free for binding of full mu agonists even at standard doses of buprenorphine. Thus, although prospective data are lacking, effective analgesia may be obtained both with buprenorphine and with concomitant use of full mu agonists while a patient is also receiving buprenorphine. However, treating acute pain with opioids alone may be challenging for high levels of postsurgical pain; maximizing non-opioid and non-pharmacological agents is essential.
Discussion
Buprenorphine for the perioperative patient
Patients with OUD frequently have high rates of hospitalization and readmission, long lengths of stay, and escalating healthcare costs.31 A subset of patients with OUD may present for surgery and have acute pain. Patients may have active untreated OUD or be in recovery and receiving MOUD. Each of these situations presents different challenges as well as opportunities for the anesthesiologist and acute pain service.62
Perioperative management of a patient on buprenorphine for OUD
In response to the opioid epidemic, increasing numbers of patients with OUD are being transitioned to buprenorphine from schedule II prescriptions or illicit opioids.63 From 2010 to 2016, annual prescriptions of buprenorphine formulations more than doubled.60 Thus, physicians are more frequently encountering patients on buprenorphine (with or without naloxone) who need surgery, necessitating more guidance as to how to care for patients with OUD. The perioperative period is a vulnerable time for patients with OUD. Patients with OUD may fear they will be treated unfairly or be judged by medical professionals during their hospitalization. Shame and stigma are also common.64 Additionally, patients worry about receiving inadequate pain relief, experiencing opioids withdrawal symptoms, and relapsing.65 Patients with OUD are at increased risk of recurrence following discharge from the hospital.43 Thus, a comprehensive preoperative evaluation, discussion of management of care, and communication with the primary inpatient service and/or outpatient prescriber are essential.
Recommended preoperative evaluation guidelines for the management of perioperative pain include obtaining a history, performing a physical examination, identifying medications whose cessation may lead to withdrawal, and assessing for psychiatric and SUD comorbidities.66 Our working group recommends universal SUD screening if possible with validated screening tools for all preoperative patients. An example of easy-to-implement screening tools includes the single question screening test for drug use (National Institute of Drug Abuse (NIDA)-1 quick screen),67 which asks about substance use during the last 12 months. A positive screen can trigger a more detailed assessment tool such as the Drug Abuse Screening Test,68 69 to assist in risk stratifying patients for additional support or referral for treatment when indicated.
Urine toxicology screens specifically testing for methadone, buprenorphine, and fentanyl may be helpful in addition to reviewing the prescription monitoring program if risk factors for OUD are present.66 It is important to note that anxiety about surgery and postoperative pain are significant stressors and may elicit a conditioned response, ultimately resulting in drug cravings.70 Exposure to prescription opioids and undertreated pain can also lead to cravings and OUD recurrence.71 72 Thus, it is imperative to discuss the risks and benefits of perioperative pain management modalities with a focus on OUD recurrence prevention. Careful discussion should ensue for patients receiving MOUD.
During the perioperative period, physicians may have concerns about the ability to treat postoperative pain given that a full mu-opioid agonist (hydromorphone, morphine, hydrocodone) is unable to displace buprenorphine. Buprenorphine has high affinity for the mu-opioid receptor, displaces full mu-opioid agonists, has an extremely long half-life (24–42 hours for sublingual or buccal administration; 26 hours for transdermal administration and 43–60 days for slow-release subcutaneous injection), is highly lipophilic, and slowly dissociates from the receptor.24 As such, oral buprenorphine takes 2–3 days to be eliminated from the body. While peak plasma concentrations increase with buprenorphine dose, the increase is not in direct proportion which results in a ‘leveling off’ of opioid effects, even with further dose increases. Buprenorphine is metabolized completely by the liver to norbuprenorphine, an active metabolite with some weak analgesic activity. Thus, previously published guidelines and expert opinion recommended discontinuing buprenorphine prior to anticipated pain or surgery.73 74 The 2004 Treatment Improvement Protocol released by the US Center for Substance Abuse Treatment stated that the administration of buprenorphine should generally be discontinued while patients are taking full mu-opioid agonist medications.74 This advisory influenced medical practice, leading to the commonplace discontinuation of buprenorphine prior to surgery. However, the recommendation was derived from case reports of difficult-to-treat acute pain in buprenorphine-maintained patients and may possibly reflect the challenge of managing already opioid-tolerant and opioid-dependent patients in need of analgesia as opposed to the consequences of buprenorphine itself.63 Furthermore, additional evidence suggests that buprenorphine in combination with full mu opioids can effectively treat perioperative or other acute pain.75–78
Even though buprenorphine has high affinity at the mu receptor, some receptors remain unoccupied and can continue to bind full mu agonists needed to treat acute pain in the perioperative period.79 Thus, perioperative management of buprenorphine is evolving from the traditional teaching of holding buprenorphine to ‘open up receptors’ to a consensus of continuing buprenorphine with or without naloxone through the perioperative period. Kornfeld et al evaluated the effectiveness of full agonist opioids in patients maintained on buprenorphine while undergoing major surgery.76 Physician assessment and patient self-report revealed adequate pain control with full opioid agonists and in some cases when multimodal treatment options were used.71 Mercadante et al were able to show the efficacy of opioid agonists in patients with cancer who were maintained on transdermal buprenorphine.80 It should be noted however that transdermal buprenorphine is a microgram formulation thus provides an overall lower dose of buprenorphine than are typically used for OUD. Furthermore, The ASAM’s National Practice Guideline for the Treatment of Opioid Use Disorder (2020 focused update) states, ‘Discontinuation of methadone or buprenorphine before surgery is not required. Higher potency intravenous full agonist opioids can be used perioperatively for analgesia’.81 Additionally, it has even been reported that patients continued on maintenance doses postoperatively have a lower patient-controlled opioid analgesia requirement than those whose maintenance pharmacotherapy has been discontinued.82
Table 7 summarizes findings of perioperative management of patients on buprenorphine for MOUD. These studies comprised largely of case reports or series, cohort studies, or retrospective reviews. There were no randomized controlled trials.
Summary of case reports/series, reviews, and published guidelines on management of buprenorphine in the perioperative period
While prospective trials are lacking, review of available literature suggests that buprenorphine (with or without naloxone) can be continued in the perioperative period while maintaining adequate analgesia. In a clinical practice advisory based on a review of evidence, Goel et al state, ‘it is almost always appropriate to continue buprenorphine at the preoperative dose. Furthermore, it is rarely appropriate to reduce the buprenorphine dose’.83 As discussed below, individual considerations on perioperative buprenorphine maintenance dosing are a shared decision between the patient and the perioperative physicians and should be tailored to patient factors, anticipated pain severity, and the availability of regional anesthetic techniques, institutional resources, and professional expertize.
Continuation of buprenorphine in the perioperative period is further supported by evidence to suggest that it is harmful to discontinue buprenorphine. In fact, for some patients, discontinuation may even be fatal.84 Likelihood of harm is increased in patients prescribed buprenorphine for OUD as opposed to chronic pain.76
Bentzley et al determined that patients who discontinued buprenorphine maintenance treatment had a >50% (range 50%–90%) chance of OUD recurrence or, even worse, of death.82 Patients with OUD are also at an increased risk of inadvertent overdose when their maintenance treatment is discontinued due to a decrease in opioid tolerance and concurrent introduction of a full mu agonist.60 In addition, patients are often fearful of discontinuing buprenorphine.82
While there is growing support for the continuation of buprenorphine in the perioperative period, there is less agreement regarding the appropriate dose at which buprenorphine should be maintained.63 In addition to the studies in table 7 suggesting adequate pain postoperative pain control in patients maintained on buprenorphine, it may be beneficial to examine studies on receptor binding to help clarify the issue.
Human [11C]-carfentanil positron emission tomography studies provide information into receptor binding occupancy at different buprenorphine doses. Study results exhibit some variability but consistently demonstrate some degree of opioid receptor availability, even at high buprenorphine doses. Greenwald et al demonstrated that when high doses of buprenorphine are used in heroin-dependent patients, there is a decrease in available mu-opioid receptors, an increase in buprenorphine levels, and a decrease in withdrawal symptoms, but also a decreased hydromorphone response overall.85 However, another study performed by the same group was able to show the percentage of available mu receptors at varying doses of buprenorphine: 71%–85% at 1 mg, 53%–72% at 2 mg, 36%–55% at 4 mg, 20%–35% at 8 mg, 13%–24% at 12 mg, 9%–20% at 16 mg, 4%–15% at 24 mg, and 2%–12% at 32 mg.85 86 The researchers concluded that patients can be maintained on buprenorphine with sufficient pain control from full mu-opioid agonists without worsened outcomes. Zubieta et al accessed mu-opioid receptor availability in three healthy controls, finding buprenorphine-induced dose-dependent opioid receptor availability reductions of 36%–50% at 2 mg and 79%–95% at 16 mg relative to placebo.87 In contrast, Quaye et al demonstrated that high doses (24–32 mg) of buprenorphine, as may be used for maintenance therapy, would result in little-to-no receptor availability, whereas moderate doses (8–12 mg) would result in up to 20% receptor availability, which is still sufficient from an analgesic standpoint.88 Finally, Comer et al estimated that mu-opioid receptor availability was 21%–31%, 11%–22%, and 6%–12% at 2, 8, and 32 mg of buprenorphine, respectively.89 Collectively, these studies suggest that even at high doses (24–32 mg) of buprenorphine, some opioid receptors remain unoccupied. Furthermore, while we are unaware of any studies investigating the degree of analgesia obtained with full mu agonists with various levels of buprenorphine receptor occupancy, Comer et al suggest that buprenorphine 16 mg/day did not fully block the reinforcing efficacy of 12.5 mg and 25 mg intravenous heroin.89 Similarly, Greenwald et al reported that buprenorphine 16 mg/day and 32 mg every other day did not fully block the reinforcing efficacy of 24 mg intravenous hydromorphone.90
In conclusion, buprenorphine may produce similar clinical analgesic efficacy as a full mu agonist.58 There is some evidence that shows a relationship between mu receptor availability and withdrawal symptoms/heroin cravings.86 Unfortunately, the literature is lacking in terms of data that confirms degree of opioid receptor occupancy needed for analgesia for any mu agonist or partial agonist; thus, future studies are needed (eg, it is unknown what per cent of opioid receptors needs to be occupied by full or partial agonists in order to produce clinically noted analgesia and/or if the percent binding needed to produce analgesia differs among individuals).
In addition to understanding receptor occupancy, risk factors for exacerbation of OUD within the perioperative period should also be identified. In a 2019 systematic review, Goel et al suggest the following as potential risk factors: discontinuation of buprenorphine prior to surgery; introduction of a full mu agonist in place of buprenorphine prior to surgery; <20 months duration of buprenorphine for treatment of OUD; a positive urine drug screen within the last 20 months; discharge from the perioperative period without maintenance of buprenorphine and insufficient communication with the patient’s outpatient buprenorphine prescriber.91
Thus, based on pharmacokinetic studies and other available literature, it is our recommendation that buprenorphine should not be routinely discontinued in the perioperative period.76 77 86–89 92–95 We do, however, recognize that there are no prospective clinical trials evaluating the optimal dose of perioperative buprenorphine. Prevailing recommendations based on preclinical data, site-specific experience, and consensus statements suggest adequate pain control in all but one patient taking ≥16 mg sublingual buprenorphine.76 77 93 94 Thus, our recommendation is to continue buprenorphine at the patient’s home dose unless inadequate pain relief necessitates a change in the maintenance dose. With sufficient addiction and/or pain management or consultative expertize, a buprenorphine taper to 16 mg could be considered for patients prescribed higher doses of buprenorphine (eg, ≥16 mg) and anticipated high postsurgical opioid requirements. We are aware, however, that for most healthcare systems, there may be insufficient access to OUD and pain medicine specialty consultations for guidance.63 76 Thus, any needed change to a patient’s outpatient buprenorphine regimen of buprenorphine, similar to other perioperative changes to outpatient medication changes, warrants a thorough discussion with both the patient and the primary buprenorphine prescriber regarding the associated risks and benefits, including the increased cravings or OUD recurrence during and after the hospitalization in conjunction with the need to achieve adequate analgesia.
It is important to understand that a multimodal analgesic regimen incorporating non-pharmacological therapies and non-opioid medications and interventions (eg, regional anesthesia) should be used in all patients continued on buprenorphine.
Pain in patients on maintenance buprenorphine (with our without naloxone) for OUD can be managed using multimodal therapies, similar to patients without OUD. As discussed earlier, a thorough conversation with the patient discussing multimodal treatment options is encouraged. Varying dosing strategies for acute or postoperative pain exist for patients prescribed buprenorphine for chronic pain or OUD. If possible, an acute pain consult should be obtained to help develop a safe perioperative management plan while minimizing OUD recurrence risk.65 Regional anesthesia as well as adjunct non-opioid medications and non-pharmacological alternatives should be used.95 Patient and family education and cognitive-behavioral approaches to manage anxiety, craving, and pain should be considered, particularly if opioid analgesics are prescribed.65 Discharge instructions should include safe use, storage, and disposal of opioids and communication with the surgical or hospitalist service.
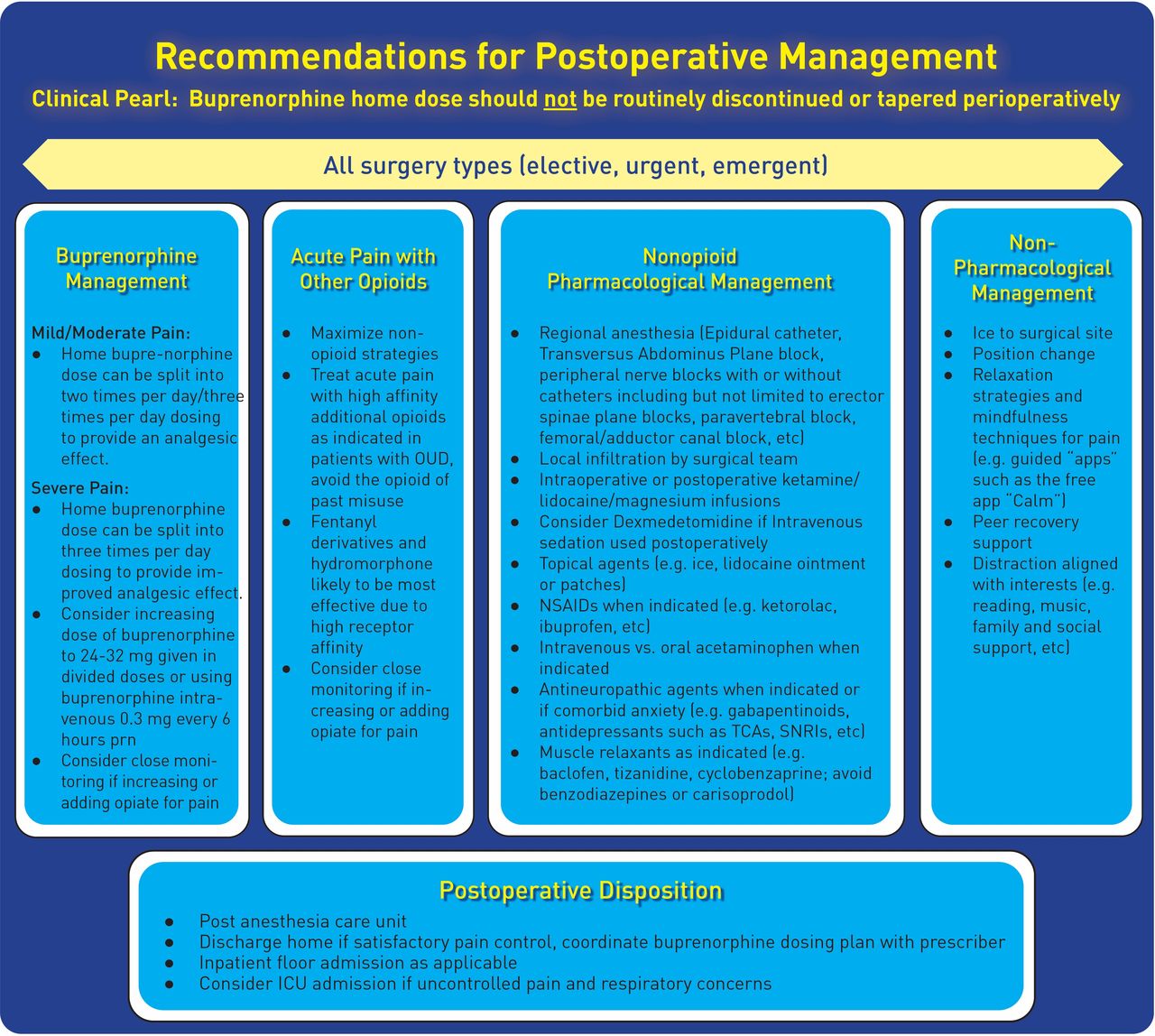
As supported by most experts, we recommend the following strategies for treating acute pain in patients prescribed chronic buprenorphine. Figure 1 provides recommendations on a multimodal analgesic approach for patients taking buprenorphine (with or without naloxone) in the perioperative period. When using full mu agonists as part of the multimodal treatment plan, opioids with high affinity to the mu receptor such as fentanyl or hydromorphone should be used. Any patient treated with an increase or addition of opioids to aid in postoperative pain control needs to be provided a safe postoperative taper with specific instructions. Some evidence suggests that supplemental doses of buprenorphine be given in addition to continuing the patient’s baseline buprenorphine dose to most effectively provide analgesia.76 77 92 Collaboration between the patient’s buprenorphine prescriber and/or addiction medicine team is always encouraged.
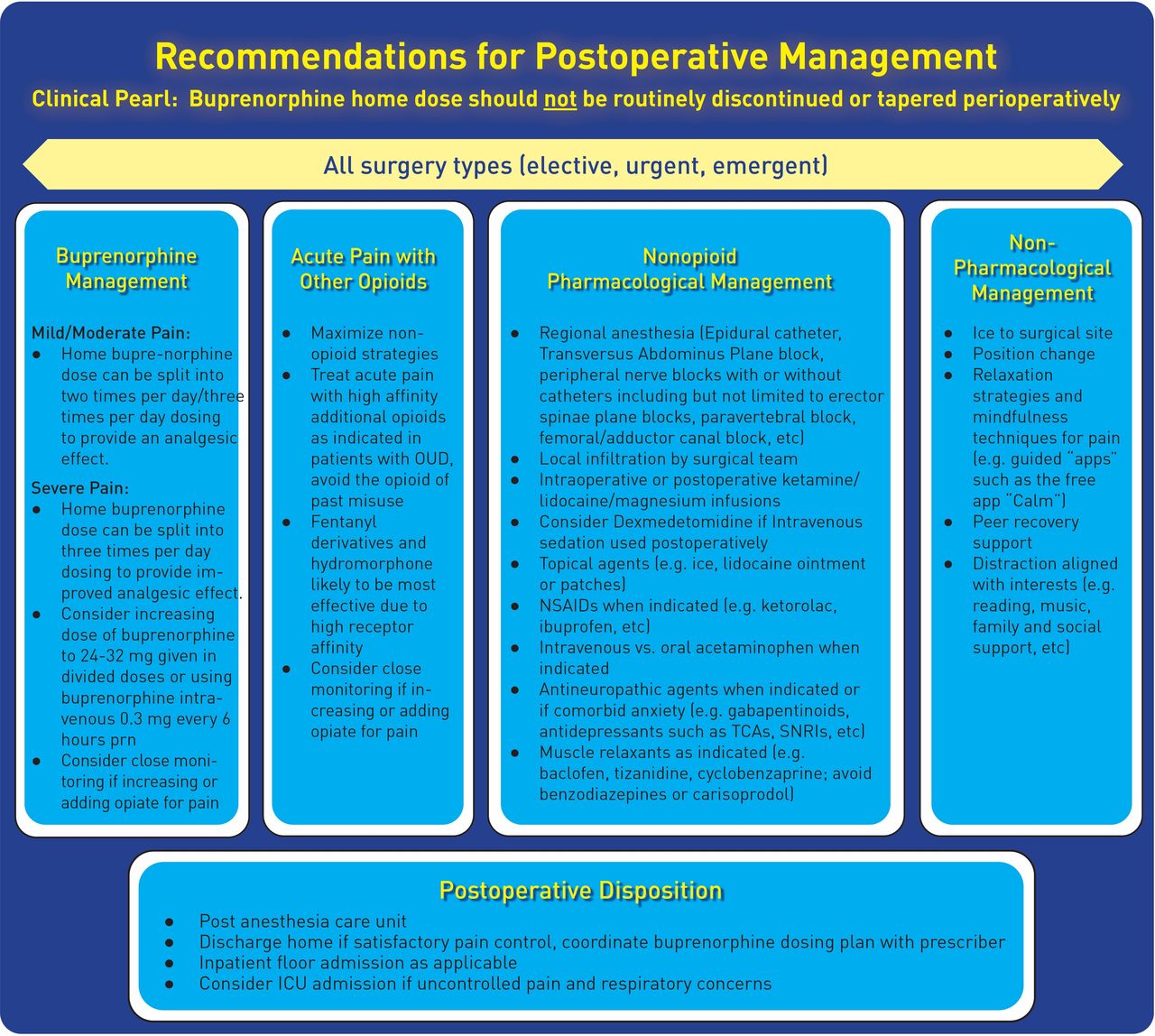
Recommendations for postoperative buprenorphine management. The recommendations above likely apply to the vast majority of healthcare systems, where addiction medicine/psychiatry services are not available to collaborate with anesthesia/acute pain services. In isolated clinical circumstances such as high-level academic medical centers with excellent integration of addiction and acute pain services, it is reasonable to consider a taper of buprenorphine in perioperative situations where extremely high levels of pain are anticipated and the admitting dose of buprenorphine is over 16 mg. If this is undertaken, it must be a shared decision between the patient, the buprenorphine prescriber, and the surgical team. An open discussion with the patient regarding possible drawbacks (including potential increase of craving and possibility of OUD recurrence) is necessary. This discussion should include a clear plan for discharge and follow-up with the primary prescriber. †The committee recognizes that not all clinicians will feel comfortable increasing the patient’s home buprenorphine dose. Thus, increasing the home dose can be done after consulting with the patient’s buprenorphine prescriber, the health system’s addiction services team (if available), and the patient. ICU, intensive care unit; NSAID, non-steroidal anti-inflammatory drug; OUD, opioid use disorder; SNRI, serotonin and norepinephrine reuptake inhibitor; TCA, tricyclic antidepressant.
Summary of recommendations
Preoperative planning
Buprenorphine should not be routinely discontinued as adequate analgesia can be achieved (grade B, moderate level of certainty). Discontinuing buprenorphine can increase the risk of OUD recurrence or harm (grade B, moderate level of evidence). Current evidence suggests variation in recommendations with regard to tapering patients on high dose (>16 mg) of buprenorphine and in situations in which high levels of postoperative pain are anticipated; however, receptor availability studies and case reports suggest adequate analgesia can still be achieved even at high doses of buprenorphine. Thus, the working group recommends that, in addition to not routinely discontinuing buprenorphine prior to surgery, one should avoid tapering it perioperatively as well (grade B, moderate level of certainty).
Postoperative pain
Most available literature recommends the use of multimodal analgesia in the perioperative period in patients receiving buprenorphine for MOUD. Thus, the working group recommends that multimodal analgesia, including adjunctive medications and regional anesthesia techniques, should be used whenever possible (grade B, moderate level of certainty).
Additional evidence from opioid receptor binding studies and other literature review suggests that opioids can be administered in conjunction with buprenorphine to achieve adequate analgesia. Thus, it is the working group’s recommendation to consider administration of full mu agonists (with high affinity for the mu receptor) (grade B, moderate level of certainty) or increased and/or divided doses of buprenorphine (grade C, low level of certainty) with close monitoring for uncontrolled postoperative pain if multimodal analgesia proves inadequate.
Discharge planning
Most studies on postoperative opioid use suggest providing a plan to taper the patient off postoperative opioids once the acute pain resolves. A taper plan can assist in minimizing withdrawal, decreasing postsurgical opioid use, and maximizing successful discontinuation of acute opioids once pain has resolved.96 97 Appropriate surgical prescribing and follow-up may ensure patients have tapered off postoperative opioids and acute pain management has been addressed. Similarly, if a full mu agonist is initiated or if buprenorphine is increased during the perioperative period, the working group recommends a postdischarge plan to taper off the full mu agonist or return to the preoperative maintenance dose of buprenorphine (grade A, moderate level of certainty). Additionally, length of recovery should be considered when prescribing full mu agonists on discharge. While providing full mu agonists with a taper plan may be reasonable for patients in stable recovery, caution is advised in those with active/recent illicit opioid use. Providing multiple daily prescriptions with ‘do not fill’ dates may be one technique to help mitigate the risk on this circumstance.
In addition, evidence from existing literature supports the working group’s recommendation to engage in ongoing collaboration with the patient’s outpatient buprenorphine prescriber (grade A, moderate level of certainty).
Perioperative management of a patient with an untreated active OUD
Substance use is prevalent among hospitalized patients: 36% use tobacco, 20% use alcohol hazardously, and 8% use illicit drugs.98 While researchers have made strides in the development of brief interventions to decrease tobacco99 and alcohol abuse100 101 among hospitalized patients, advancements in the treatment of opioid misuse have been minimal.102 Patients with opioid dependence are at an increased risk of adverse health-related events, and thus, often seek care in emergency departments.103 Between 2004 and 2011, opioid-related emergency department visits increased 183%. Nearly 25% of these visits resulted in hospital admission.104 Patients with OUD are approximately seven times more likely to be hospitalized than patients without OUD.105 These hospitalizations enable interventions to take place. While the number of patients with OUD presenting for surgery is unknown, this may provide an opportunity to initiate buprenorphine.106 Undertreated pain in conjunction with unaddressed OUD may result in less favorable outcomes, including premature discharge, worsening of underlying medical conditions, readmission, OUD recurrence, and overdose, both during the inpatient stay and immediately after discharge. Acute pain management necessitates special considerations and planning for patients with OUDs.65 Opioid withdrawal may also interfere with medical treatment; thus, withdrawal should be managed appropriately using a tapering schedule of opioid agonist substitution with methadone or buprenorphine.106 107 Furthermore, opioid withdrawal is considered a high-risk period that is associated with increased risk of opioid use, overdose, and death.60 108–110
Studies suggest MOUD can be started safely during hospitalization, promoting engagement in outpatient SUD care and increased acceptance of MOUD.102 104 A study by Liebschutz et al and literature from the Substance Abuse and Mental Health Services Administration (SAMHSA) reported lower rates of illicit opioid use at a 6-month follow-up period among hospitalized patients who received buprenorphine induction and linkage to buprenorphine treatment on discharge.102 111 Liebschutz et al compared use of long-term MOUD between opioid-dependent hospitalized patients receiving buprenorphine induction and linkage to treatment versus detoxification.102 The buprenorphine-initiated group was found to have greater long-term use of MOUD compared with the detoxification group. In addition, D’Onofrio et al found emergency department-initiated buprenorphine with coordinated follow-up for continued treatment versus referral, with or without brief intervention, increased engagement in OUD treatment, reduced self-reported illicit opioid use, and decreased the use of inpatient OUD treatment services.101 Initiating buprenorphine must be a shared decision with the patient. Previous needs assessment studies have indicated that 67% of patients with active substance abuse would like to cut back or quit, and 44% are interested in MOUD.31 Thus, given the desire of patients to seek treatment and the apparent efficacy of hospital-initiated treatment, it appears hospitalization may provide a moment for starting addiction treatment.38
It has also been reported that exposure to MOUD for even short periods of time increases survival. Studies report an instantaneous reduction in mortality after buprenorphine-assisted detoxification, even when access to long-term care and follow-up was not available.46 Every day, week, or month that a patient is receiving treatment is a period of time during which they have a reduced risk of overdose.112 Therefore, increasing pressure to make MOUD standard practice exists in some arenas. Leaders within emergency medicine (EM) have been called on by the Surgeon General and the CDC to aid in addressing the opioid epidemic by expanding patients’ access to MOUD with buprenorphine.113 In addition, the state of Massachusetts recently mandated treatment of OUD in emergency departments.114 Furthermore, multiple studies report patients initiated on MOUD within the EM setting remained in long-term engagement of treatment for OUD.115
Unfortunately, many hospitals lack inpatient OUD services and pathways to care for and link patients to timely OUD care after discharge.116 Additional fears and/or limitations include the need for patients to abstain from opioid use for a period of time before starting buprenorphine/naloxone to provide adequate time for the elimination of systemic full mu opioids and avoiding precipitating opioid withdrawal with the use of a partial opioid agonist with high affinity for the opioid receptor.117
Thus, there is a need to create models that can improve care for patients with untreated OUD. One such approach is the induction of buprenorphine without requiring prior withdrawal symptoms, an approach used with increasing frequency in EM.118 Similar to the emerging evidence from EM, buprenorphine may be initiated safely in perioperative patients suspected of having an OUD.
Different approaches to inpatient induction are available and include waiting for opioid withdrawal (eg, Clinical Opioid Withdrawal Scale (COWS) 8 or 12) before giving buprenorphine; however, this is intolerable for some patients. New methods of initiating buprenorphine are evolving including microdosing and a method that describes a protocol essentially midway between the traditional method and the microdosing method. Microdosing, also known as the ‘Bernese method’, attempts to improve patient comfort by avoiding the need for withdrawal and minimizing the risk of precipitated withdrawal.119 Microdosing appears well tolerated by patients in case reports.119 120 The ‘Bernese method’ describes initiating patients on doses of 0.2 mg of buprenorphine (compared with traditional induction doses of ≥2 mg) and slowly escalating while concurrently de-escalating the other opioid; however, a universally recommended protocol does not exist.119 While microdosing is becoming increasingly popular, a recent systematic review confirmed that publications are limited to case studies and no rigorous trials have been conducted.121 A recent study by Moe et al demonstrated that EM department-initiated buprenorphine/naloxone induction is feasible.121 While microdosing may therefore be an option in certain hospitalized patients, microdose initiations may take between 5 and 7 days, which may be longer than a patient’s anticipated length of stay. Faster inductions with standard dosing have also been used successfully; however, there is currently no consensus for the optimal initial buprenorphine dose.122 For uncomplicated opioid withdrawal, most existing algorithms122–126 suggest administering 4–8 mg buprenorphine sublingual and waiting approximately 1 hour. If withdrawal symptoms have improved, the physician may titrate an additional 4–8 mg as needed until cravings are suppressed. Discharge recommendations include documentation of opioid withdrawal and/or OUD as a diagnosis, providing a loading dose of 32 mg if no x-waivered provider is available to provide a prescription, and a <7-day prescription if an x-waivered provider is available.126 If withdrawal symptoms do not improve after the initial dose, the following differential diagnoses should be considered: underlying illness mimicking withdrawal, such as influenza, diabetic ketoacidosis, and thyrotoxicosis; incomplete treatment withdrawal; side effects from buprenorphine itself; or too large a dose started too soon after opioid agonist (precipitated withdrawal).126 Uncomplicated withdrawal can be diagnosed using subjective report and objective signs.
Withdrawal assessment
Subjective
Patient reports feeling unwell: nausea, stomach cramps, body aches, yawning, goose bumps, vomiting, diarrhea, and/or tremor may be reported.99
Objective
At least one of the following symptoms is observed: restlessness, sweating, rhinorrhea, dilated pupils, watery eyes, tachycardia, yawning, goose bumps, diarrhea, or tremor.
Typical withdrawal onset occurs >12 hours after short-acting opioid; >24 hours after long-acting opioid; and >48 hours after methadone (can be up to >72 hours).101
A recent systematic review by Wolff et al assessed the current literature for EM-initiated buprenorphine.127 They identified 215 articles via various search engines. Of these, eight were selected based on relevance to the question ‘In adult patients experiencing opioids withdrawal, is emergency room-administered buprenorphine as effective for the management of opioid withdrawal compared with alternative management therapies’. They concluded that there were no level A recommendations. Buprenorphine or methadone are more effective options compared with non-opioid-based management strategies, such as adrenergic agonists and antiemetics; thus, using these medications for initiating treatment for opioid withdrawal in the emergency department is a level B recommendation. The authors recommended utilization of buprenorphine as opposed to methadone as a level C recommendation (box 2).128
Levels of recommendation as defined by Hatten et al128
Level A recommendation
Generally accepted principles for patient care that reflect a high degree of scientific clinical certainty (eg, based on evidence from one or more class of evidence I or multiple class of evidence II studies demonstrating consistent effects or estimates.
Level B recommendation
Recommendations for patient care that may identify a particular strategy or range of strategies that reflect moderate scientific certainty (eg, based on evidence from one or more class of evidence II studies or multiple class of evidence III studies demonstrating consistent effects or estimates.
Level C recommendation
Recommendations for patient care that are based on evidence from class of evidence III studies, or in absence of any adequate published literature, based on consensus.
In contrast to expert recommendations that advise waiting until mild-to-moderate withdrawal symptoms occur before initiating buprenorphine,129 a recent case series by Patel et al suggests that buprenorphine may be initiated prior to experiencing overt withdrawal.106 Patel et al provide a protocol for initiating buprenorphine for postoperative pain in patients with OUD in the perioperative period.106 Buprenorphine was initiated 4 hours after the last full mu opioid was given to allow for a washout period. The time frame was chosen based on the half-life (close to 4 hours)130 and general prescribing frequency (every 4–6 hours for pain) of oxycodone, the most commonly used full mu agonist at their institution. Intravenous hydromorphone, also commonly used for postoperative pain, has an even shorter half-life,131 with the expectation that initiating buprenorphine would not precipitate acute withdrawal. In the study by Patel et al, patients were provided 2 mg sublingual buprenorphine as needed for pain every 2 hours during the first 24 hours for a maximum of 12 doses (24 mg).106 Additional full mu agonists were not provided. Three patients experienced mild withdrawal symptoms, such as nausea and diarrhea, and two patients had no subjective signs of withdrawal. Two patients were evaluated for the COWS; one had a score of 8 and the other 0. Patients were typically discharged on a dose of 8 mg two times per day or 16 mg daily. Mean pain scores before and after buprenorphine initiation were 5.2±2.9 vs 4.7±2.9 (p=0.4), respectively, suggesting that standard doses of full mu agonists were not essential to achieving adequate pain control. However, pain control cannot be attributed to buprenorphine alone as multimodal analgesia, including ketamine, was provided. On discharge, patients were linked to an outpatient buprenorphine provider. The study assessed the number of patients who filled their buprenorphine prescriptions after discharge (five out of seven); similar to strategies employed by internal medicine physicians and psychiatrists.132 133
Based on available evidence from hospital and EM inductions as well as the working group’s expert opinion, prior to hospital discharge, buprenorphine may be initiated in small doses, similar to those used in the study by Patel et al,106 which should maintain adequate analgesia without precipitating severe opioid withdrawal. Collaboration with the acute pain service or addiction specialist team is recommended if available, but absence of these services should not absolutely prohibit initiation. When considering initiating buprenorphine, it is important to first confirm that buprenorphine therapy is indicated. Many patients will divulge symptoms of OUD if asked. Screening tools such as the Opioid Risk Tool, Screener and Opioid Assessment for Patients with Pain, Current Opioid Misuse Measure, and Addiction Behaviors Checklist have been used successfully in EM134 and thus may be used within the perioperative setting.
It is the working group’s recommendation to initiate buprenorphine at a lower dose than suggested in many EM protocols.122–126 Starting at a lower dose may lessen the risk of precipitated withdrawal and enable initiation within 4–6 hours of the last short-acting full mu-opioid agonist and within 1–2 hours of intravenous full mu agonist opioids. Adjuvant medications may be used, if necessary, to lessen withdrawal symptoms (table 8).
Modalities used to treat opioid withdrawal symptoms
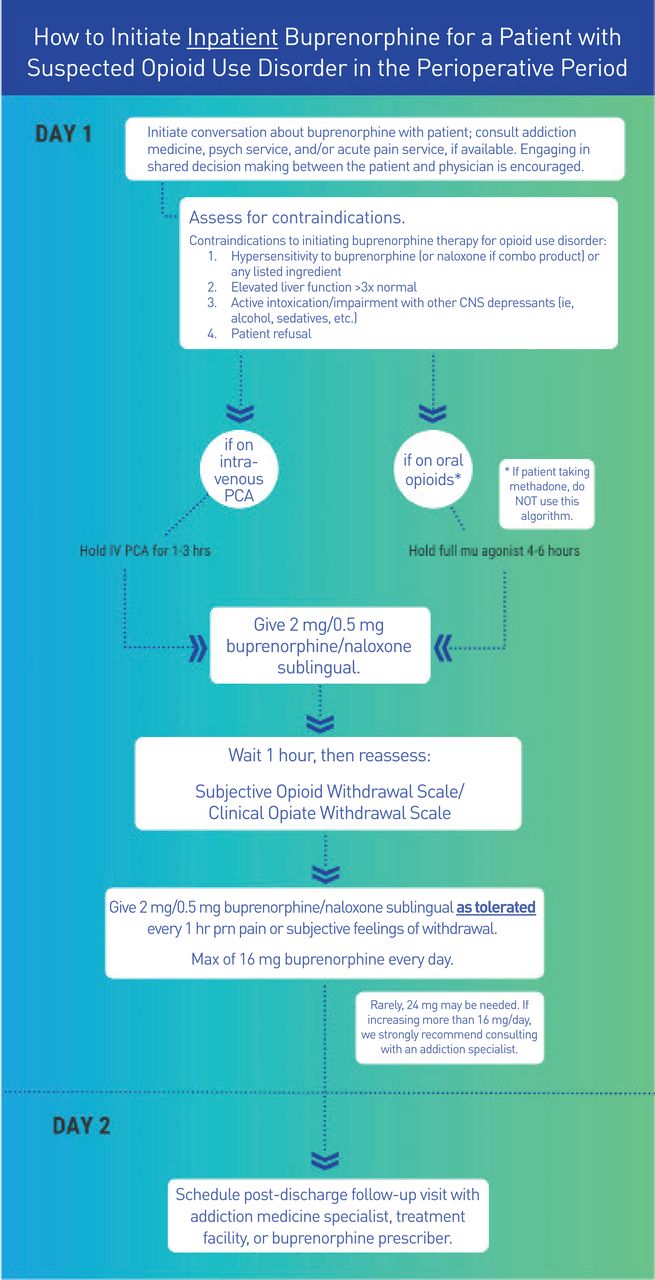
Figure 2 presents the working group’s recommendations on starting buprenorphine in this manner. It is preferable that all patients initiated on buprenorphine be referred to an addiction medicine specialist, primary care provider, or other community resource. Until a relationship with a local provider is established, it has been recommended to call any available community buprenorphine prescriber before starting buprenorphine122 in the hospital if able; however, our group does not recommend delaying necessary treatment if a community provider is unavailable. A buprenorphine prescriber locator is available on the SAMHSA website to facilitate establishing community linkage if needed.135 A needs assessment study within the EM literature highlighted the discordant priorities of the emergency room (rapid and flexible referral process) and the community prescribers offering buprenorphine; this emphasizes the need for increased availability and accessibility to MOUD on demand and the importance of communication between EDs and community prescribers of MOUD.136 To help accomplish this goal, they recommend that a date, time, and follow-up location should be provided whenever possible in order to ensure a smooth transition.136 Patients can alternatively register with an anonymous buprenorphine provider matching system that facilitates patient-provider contact.137 Perioperative physicians can also use lessons learned from the EM literature to help facilitate processes that enable hand-offs of care, including use of social workers to help coordinate outpatient MOUD referrals without increasing physician workload or costs.138 In a retrospective, cohort, single-center study, Kelly et al describe a social work-driven emergency department initiation of buprenorphine program with referral to community MOUD providers. Patients with OUD presenting to the ER were identified by patient self-report, standardized nursing screening, or emergency department provider concern. All patients who were identified in this manner received an urgent social work consult to explore willingness to seek treatment for OUD. The social workers developed individual plans to help link patients to appropriate community prescribers.138
{kind=link}
{kind=link}
How to initiate buprenorphine for a patient with suspected opioid use disorder (OUD) in the perioperative period. *We do not recommend using this algorithm (eg, initiating buprenorphine) in patients with chronic pain who are currently being prescribed long-acting opioids in the perioperative period. Clinical Opioid Withdrawal Scale (COWS): see online supplemental appendix B. Subjective Opioid Withdrawal Scale (SOWS): see online supplemental appendix C. CNS, central nervous system; PCA, patient-controlled opioid analgesia.
Supplemental material
Supplemental material
A recent review by Martin et al further describes models to establish maintenance treatment on discharge; including the Substance Abuse Services and Referral to Treatment model, bridge model, and emergency department-bridge model.139 These models may provide useful guidance in implementation and logistical details to support health systems in better addressing OUD in their communities.
We recognize that barriers may exist due to the patients’ insurance or lack of insurance and difficulty finding a suitable outpatient buprenorphine prescriber, which may prevent handing-off the patient’s care. While a hand-off is preferable and strongly recommended, short-term treatment without follow-up has been demonstrated to reduce mortality,46 decrease presence of illicit substances,140 and increase harm reduction44; thus, lack of such resources should not uniformly prohibit initiation of buprenorphine in this setting. Any physician who decides to prescribe buprenorphine when a ‘hand-off’ is not possible should consider the risks and benefits unique to the clinical situation, including their own comfort level and education, as well as balancing the risks of prescribing a full mu agonist on discharge versus buprenorphine in regard to OUD recurrence prevention and analgesic control.
Tools to aid in the development of protocols for evidence-based treatment of OUD exist, including guidance on screening, medication administration, and preparation for discharge.141 Order sets can be developed to aid physicians in the process. The Ca Bridge to Treatment program issued a Best Practices: Inpatient and Order Set Guideline, which is a useful resource (box 3).142
Strategies for in-hospital management of patients with opioid use disorder (OUD)
Screening
Most patients will disclose their substance use history when asked.
Urine toxicology is generally not required but may be useful, particularly in identifying patients who have recently taken methadone, which may make initiation of buprenorphine more difficult.
Some clinics may require a positive urine toxicology for opioids prior to medication treatment of opioid use disorder (MOUD) treatment, which may be important when linking to community care.
Medication administration
See committee recommended algorithm. Figure 2 (inpatient buprenorphine initiation).
The Clinical Opioid Withdrawal Scale may be a useful tool to help physicians and nurses who are new to diagnosing opioid withdrawal. Use of subjective signs and objective signs of withdrawal is also valid.
May include naloxone for respiratory rate <8 breaths per minute.
Discharge planning
If able, provide buprenorphine prescription for OUD as bridge to community-linked treatment. Requires x-waivered physician.
If an x-waivered provider is not available, ensure immediate linkage to community clinic providing MOUD care.
Provide naloxone prescription or information at discharge.
Provide information for follow-up to community-linked clinic.
Pathways that guide management of patients from hospital to community OUD treatment are likely to be absent in many hospital systems. A recent needs assessment study employed the use of ‘in reach’ liaisons—community SUD treatment staff who perform in-hospital assessments to triage and coordinate care across systems.31 We recognize that these types of ‘in reach’ liaisons may not be feasible; thus, we recommend coordinating with social workers to help facilitate transition to community based-care where possible. It is also important to note that the link to care should include a variety of options, including MOUD, and abstinence programs, office-based treatment, intensive outpatient treatment, and residential levels of care, thereby giving patients many options.31
Recommendation
Patients with suspected OUD can be approached and educated about the benefits of initiating buprenorphine postoperatively. Current literature, largely from the field of EM, has demonstrated that initiation of buprenorphine for patients with OUD results in decreased use of illicit substances and greater retention in OUD treatment programs. Safe initiation of buprenorphine with linkage to a community provider was described in several available EM studies, as well as by an anesthesia-led team in a case series. Thus, based on both review of this literature and expert opinion, it is the working group’s recommendation that, when possible and clinically indicated, anesthesiologists/pain physicians can consider recommending or starting buprenorphine for postoperative analgesia in patients with suspected OUD, using available social work or ancillary services to help facilitate linkage to outpatient buprenorphine prescribers when possible (grade of evidence B, moderate level of certainty). However, per updated Department of Health and Human Services (HHS) guidelines, buprenorphine treatment can now be legally given without concomitant ancillary treatment.143 Thus, one additional recommendation, based on physician expertize/comfort, is that buprenorphine treatment can still be considered in circumstances in which follow-up/insurance coverage has not been fully established (grade of evidence C, low level of certainty). Buprenorphine, with its long half-life and partial agonism, is likely a safer alternative for discharge medication than full mu-opioid receptor agonists in patients with OUD, even without an established connection to an outside buprenorphine prescriber. Thus, in circumstances in which a warm hand-off has not been definitely established, the amount of buprenorphine prescribed can be consistent with appropriate postoperative discharge standards; however, a longer course of treatment could be provided, depending on the prescribing physician’s comfort level. Initiating buprenorphine should always entail a shared decision-making process between the patient and the physician. The patient should also be given whatever resources are available within the local community to encourage continuation of SUD treatment, whether medical or psychosocial.
Legal issues and x-waivers
Rules and regulations regarding the prescription of buprenorphine are confusing and may lead to decreased access to care. However, given recent data showing an increase in opioid-related overdose deaths in the year preceding August 2020,144 there has been a renewed emphasis at the federal level to increase access to MOUD.144 There have also been several recent legal changes and updates related to the x-waiver certification process. On April 28, 2021, the Department of HHS announced that qualified providers who are state-licensed and registered by the DEA are exempt from the current x-waiver certification training requirements.141 To qualify for the exemption, physicians must adhere to a limit of treating to no more than 30 patients at any one time, and they still must submit a NOI to obtain an x-waiver to SAMHSA. These exemptions only apply to the prescribing of schedule III, IV, and V medications and not schedule II medications such as methadone for OUD. Furthermore, physicians can only treat patients under this exemption in states where they hold an active medical license.
Clinicians can order milligram (ie, MOUD) FDA-approved formulations of buprenorphine to hospitalized (perioperative) patients without applying for an NOI and can increase the dose if needed in order to ‘maintain or detoxify a person as an incidental adjunct to medical or surgical treatment of conditions other than addiction, or to administer or dispense narcotic drugs to persons with intractable pain in which no relief or cure is possible or none has been found after reasonable effort’.144 Accordingly, patients admitted for conditions such as endocarditis related to drug use, osteomyelitis, abscess, and trauma related to injection drug use are all eligible for treatment with buprenorphine or methadone in the hospital setting. FDA formulations approved for the treatment of chronic pain, such as buprenorphine transdermal patch (Butrans) and the buccal formulation (Belbuca), cannot be prescribed for the treatment of OUD; however, they can be used for the treatment of analgesia in any setting without obtaining a x-waiver.145
X-waiver certification process
X-waiver certification is still required for physicians who wish to treat >30 patients at a time. The training for physicians involves 8 hours of continuing medical education and can be completed fully online free of charge (box 4).
Steps for obtaining x-waiver certification (if desiring to treat >30 patients)
Complete training.
8 hours hours for physicians.
24 hours for mid-level providers.
Apply to Substance Abuse and Mental Health Services Administration for ‘x-waiver’.
Training available at https://pcssnow.org/medications-for-opioid-use-disorder/
Summary
X-waivers are not required to prescribe/dispense buprenorphine while the patient is in the hospital or emergency department; however, they are required to provide a prescription for buprenorphine that a patient will fill at a pharmacy. The training to obtain an x-waiver is waived when treating <30 patients and submitting an NOI to SAMHSA.
It is the working group’s consensus to advocate for the elimination of barriers to prescribing buprenorphine for patients with OUD. We also advocate that in the interim physicians obtain education in MOUD and submit an NOI to obtain an x-waiver.
Consensus
The presubmission version of these recommendations was sent to participating societies in March 2021, and approved by the American Society of Regional Anesthesia and Pain Medicine, American Academy of Pain Medicine, and the American Society of Health-System Pharmacists. The American Society of Anesthesiologists and the ASAM requested some additional edits which were included by the working group. There was 100% consensus among the committee members (coauthors) for each recommendation. All five societies supported the recommendations in the manuscript. These guidelines were approved en bloc by the American Society of Administrative Council and Committees on Pain Medicine (Acute and Chronic), but were not voted on by their Board of Directors.
Conclusion
OUD is a chronic debilitating disease that results in significant morbidity and mortality. Increasing the use of buprenorphine during the perioperative period is one important way to decrease morbidity and mortality, and anesthesiologists and pain physicians are uniquely qualified to lead this effort. Buprenorphine is an effective FDA-approved medication for the treatment of pain and OUD. While this document addresses numerous issues regarding the use and prescription of buprenorphine in the perioperative period, the overarching goals of this multisociety working group are to educate anesthesiologists and pain physicians and to encourage the use of evidence-based treatment options for OUD. Understanding the significant morbidity and mortality caused by OUD is critical for both individual patient care and our current public health crisis. This is a prime instance where our specialty can and should make a difference. This multisociety working group encourages physicians to learn more about this safe, efficacious, and underused treatment that can save lives. See online supplemental appendix 4 for summary of committee recommendations.
Supplemental material
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Acknowledgments
The authors would like to thank Angie Stengel for her administrative assistance in coordinating conference calls and outreach to participating organizations. We would also like to thank Anne Snively and Athena Ermidis for their help with figure creation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @kohanlynn, @SPotruDO
Correction notice This article has been corrected since it published Online First. The author affiliations have been updated.
Contributors All authors contributed to the development, writing and revision of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer This document is based on literature review and expert opinion. It is not intended to establish standard of care.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.