Article Text

Abstract
Point-of-care ultrasound (POCUS) is a critical skill for all regional anesthesiologists and pain physicians to help diagnose relevant complications related to routine practice and guide perioperative management. In an effort to inform the regional anesthesia and pain community as well as address a need for structured education and training, the American Society of Regional Anesthesia and Pain Medicine (ASRA) commissioned this narrative review to provide recommendations for POCUS. The guidelines were written by content and educational experts and approved by the Guidelines Committee and the Board of Directors of the ASRA. In part I of this two-part series, clinical indications for POCUS in the perioperative and chronic pain setting are described. The clinical review addresses airway ultrasound, lung ultrasound, gastric ultrasound, the focus assessment with sonography for trauma examination and focused cardiac ultrasound for the regional anesthesiologist and pain physician. It also provides foundational knowledge regarding ultrasound physics, discusses the impact of handheld devices and finally, offers insight into the role of POCUS in the pediatric population.
- pain management
- ultrasonography
- critical care
- education
- technology
Statistics from Altmetric.com
Introduction
Point-of-care ultrasound (POCUS) has become a powerful tool at the bedside because of the potential for improving patient management. Modern ultrasound (US) equipment provides excellent image quality, portability, simplicity and availability in various clinical settings. Although ultrasound and echocardiography have historically been within the purview of radiologists and cardiologists, the emergence of POCUS as a bedside tool to supplement the physical examination has resulted in tremendous expansion into other subspecialties. Although there is overlap, there are unique subspecialty clinical applications. For example, ultrasound visualization of peripheral nerves for procedural purposes has a significant benefit to regional anesthesiologists and chronic pain physicians despite having separate indications in radiology.1–3 It is this diversity in clinical ultrasound practice among subspecialties that underlies the American Medical Association’s recommendation that ‘policy on ultrasound imaging…(and) criteria for granting ultrasound privileges (be) based upon background and training for the use of ultrasound technology and strongly recommends that these criteria are in accordance with recommended training and education standards developed by each physician’s respective specialty’.4 Based on these recommendations, there exist guidelines for training, competency and credentialing in POCUS in emergency medicine5 and critical care medicine,6 7 and there is currently a work product for POCUS available through the American Society of Anesthesiologists (ASA).8 Despite the availability of significant resources in the form of numerous live courses9 and an educational review series on POCUS,10–15 no specific guidelines or recommendations exist on the use of POCUS for regional anesthesiologists and pain physicians. Given ASRA’s early leadership in providing recommendations for procedural-based bedside ultrasound in the form of ultrasound-guided regional anesthesia and ultrasound-guided interventional pain procedures, there was a call to address the need for formal POCUS recommendations.2 3
The American Society of Regional Anesthesia and Pain Medicine (ASRA) Guidelines Committee appointed a task force to develop recommendations for the clinical indications for POCUS as a foundation for education and training in POCUS. The task force aims to provide alignment between regional anesthesiologists and acute and chronic pain physicians for training recommendations in the perioperative and/or chronic pain setting. The recommendations are based on the current best evidence and will consider each clinical setting’s commonalities and uniqueness.
In part I of a two-part review article series, we will discuss the clinical indications for POCUS for the regional anesthesiologist and pain physician. The skills discussed are airway ultrasound, lung ultrasound (LUS), gastric ultrasound, the focused assessment with sonography for trauma (FAST) examination and focused cardiac ultrasound (FoCUS). The authors acknowledge that musculoskeletal ultrasound and neurosonography are other emerging diagnostic skills but are outside the scope of this POCUS article.
We also provide foundational knowledge regarding ultrasound physics, the impact of handheld devices and finally, insight into the role of POCUS in the pediatric population.15 Ultimately, these task force recommendations will outline the clinical indications of POCUS and lay the foundation for defining criteria for education, training, competency and credentialing for the regional anesthesia and pain physician.
Methods
An expert panel was assembled for this project based on the recommendations from the ASRA’s Guidelines Committee and Board of Directors. This panel consists of national and international experts in POCUS. Specifically, the qualifications for panel selection involved multiple publications in POCUS, leadership through participation in and/or development of POCUS education and expertise and leadership in regional anesthesia and pain medicine to ensure all topics are accurately covered and appropriate for education and training recommendations. To define areas of competency, a systematic literature search (MEDLINE, PubMed and Ovid) was performed, looking at clinical indications and utilization of POCUS for anesthesiologists, regional anesthesiologists and pain physicians. Findings were not filtered by risk of bias or Grading of Recommendations, Assessment, Development and Evaluations (GRADE) of evidence. When appropriate, recommendations were drawn from other subspecialties such as critical care, cardiology, emergency medicine, surgery and radiology. Keywords used included: point-of-care ultrasound, ultrasound, regional anesthesiology, perioperative point-of-care ultrasound, chronic pain, acute pain, ultrasonography/standards, clinical competency/standards, ultrasound physics, curriculum, education, training, barriers to education, barriers to training, airway ultrasound, lung ultrasound, pulmonary ultrasound, focused cardiac ultrasound, gastric ultrasound, pediatric point-of-care ultrasound and handheld ultrasound. Based on these relevant clinical skills (airway ultrasound, lung ultrasound, focused cardiac ultrasound, gastric ultrasound, abdominal/pelvic ultrasound), corresponding groups were tasked with describing educational goals and requirements for competency for regional anesthesiologists and pain physicians. The writing process was then conducted in leader-facilitated groups. Contributing authors were granted access to review the document in its entirety and gave final approval to the recommendations.
Ultrasound physics and equipment requirements for POCUS
Ultrasound imaging is a user-dependent tool that requires knowledge of the fundamental principles of ultrasound and the technical skills for acquisition, optimization and accurate interpretation of images.16 Most regional anesthesiologists and pain physicians are familiar with linear and curvilinear transducers for ultrasound-guided procedures and the general principles of ultrasound image generation, common artifacts and the sonoanatomy of neurovascular structures. To perform an organ-based ultrasound, such as echocardiography, clinicians will need to familiarize themselves with lower frequency transducers, such as the phased array, as well as the wide dynamic range capacitive micromachined ultrasound transducers (CMUTs). The artifacts associated with phased array processing, such as ghosting, and Doppler measurements, such as aliasing, are unique and require advanced understanding.17 18
Medical ultrasound is mechanical energy in the form of high frequency (>20 kHz) sound waves emitted from a piezoelectric transducer or a CMUT. The majority of the waves pass through tissue with different densities and resistance to sound (acoustic impedance), and a small fraction is reflected toward the transducer. Returned ultrasound signals alter the shape of the piezoelectric crystals or flexible plates of the CMUT, creating an electrical current proportional to the signal’s strength, which is then processed to form a two-dimensional image.19 Concepts such as reflection, refraction, scattering and attenuation play an essential role in ultrasound image interpretation; however, given the scope of this article, we suggest learners reference other fundamentals of ultrasound text to explore these topics further.
Ultrasound artifacts play an important role in POCUS imaging and interpretation. With POCUS, navigating through acoustic barriers such as aerated lungs and the bony framework of the chest wall results in artifacts that can either contribute to misdiagnosis or be used as diagnostic aids.20 For example, A-lines and B-lines, discussed in detail in the LUS section, can be used to guide management in focused LUS. See table 1 for a list of common ultrasound artifacts.
Knowledge of ultrasound physics and equipment21
For POCUS, transducer selection ensures optimal axial and lateral resolution. High-frequency linear (HFL) transducers provide a rectangular image; however, due to increased attenuation, imaging depth is limited. Therefore, HFL probes are ideal for superficial structures such as the pleura and the airway. Convex (curvilinear) sequential array transducers are arranged in a curved fashion producing a fan-shaped image. Convex transducers have a lower frequency and thereby provide improved image resolution of deeper structures (penetration), a wider image in the far field and are best for imaging intraperitoneal and retroperitoneal organs. For intrathoracic structures such as the heart and large vessels, low-frequency phased array transducers with a small footprint that use electronic field steering to image beyond acoustic barriers, such as ribs, produce a cone-shaped image of the heart. When comparing capacitive transducers (CMUT) to traditional piezoelectric transducers, the CMUT transducer’s advantages are a larger bandwidth and lower production cost.21 CMUT arrays can be manufactured with different operating frequencies and geometries from a single silicon wafer, allowing full-body imaging with a single transducer.22 The disadvantage is that CMUT technology is relatively new compared with piezoelectric transducers; therefore, the imaging quality and applications do not match traditional transducers.
Clinical indications and evidence for POCUS
We will focus on the clinical indications and evidence for airway ultrasound, LUS, gastric ultrasound, the FAST examination and FoCUS for the regional anesthesiologist and pain physician.
Although the clinical benefits of POCUS have been widely advocated by many medical specialties,6 23–27 the apparent positive impact of POCUS on patient outcomes has not consistently been demonstrated in a randomized, controlled trial for many reasons.28 29 First, POCUS is used as a diagnostic or monitoring tool. It is not a procedural intervention that can be easily randomized and directly attributed to improved patient outcomes. Second, POCUS is only one part of the complex sequence of medical care. As such, it is challenging to show that a single intervention can either lead to a meaningful outcome or overtreatment, overdiagnosis or potential iatrogenic injury. Finally, POCUS findings as an extension of the physical examination are heavily dependent on proper education and training, maintenance of competency, personal skills and experience and individual interpretation of the operator. With that said, what follows is the current best evidence supporting the clinical indications for POCUS.
Airway ultrasound
Point-of-care airway ultrasound can aid in the assessment and planning of perioperative or periprocedural airway management. Airway US can be used to predict potential difficult airway management. The measurement of the anterior neck has shown that the distance from the skin to the hyoid bone is highly predictive of difficult mask ventilation and intubation.30 In a patient with a concern for a ‘cannot intubate, cannot ventilate’ scenario, front of neck airway sonographic identification of the cricothyroid membrane is more accurate than palpation alone31–34 and more rapid for emergency airway access.35 36 Of note, the cricothyroid membrane is highly dependent on neck position; therefore, one must maintain the same position or (following any movement of the neck) rescan to confirm location before attempting an emergency airway.
Airway ultrasound assessment of the cricoid cartilage compared with palpation has improved accuracy, facilitating the correct application of cricoid pressure.37 38 Additionally, the efficacy of cricoid pressure can be assessed by visualization of esophageal compression.
Confirmation of endotracheal intubation compared with endobronchial intubation with airway ultrasound was more sensitive and specific than chest auscultation when tracheal cuff dilation and bilateral pleural sliding was seen.39 40 In the event of decreased or absent end-tidal carbon dioxide, as seen in cardiac arrest or other low output states, lung sliding can be used as a surrogate for endotracheal tube confirmation.41 And finally, it can facilitate nasogastric tube placement.30–40 Multiple studies have shown the benefit of ultrasound imaging in the correct placement of nasogastric tubes.42–44 See figure 1 for an example of airway ultrasound probe placement, anatomy and sonoanatomy.

Airway ultrasound (US) probe placement, anatomy and sonoanatomy. (A) Probe placement for airway US scanning. (B) Anatomy of the thyroid cartilage, cricoid cartilage and tracheal rings with corresponding sonoanatomy in transverse and sagittal planes. CC, cricoid cartilage; TC, tracheal cartilage. *Cricothyroid membrane.
There are advanced procedural applications of point-of-care airway ultrasound that we will briefly mention as they are beyond this document’s scope. Ultrasound-guided nerve blocks for airway anesthetization should be reserved for those with expertise in their performance.45 Landmark-based glossopharyngeal and superior laryngeal nerve blocks have been associated with higher plasma concentrations of local anesthesia, a higher incidence of local anesthetic systemic toxicity (LAST) and lower patient comfort than less invasive techniques.45 While ultrasound-guided techniques may provide more favorable results over traditional landmark-based approaches, the current evidence is insufficient to recommend them over non-invasive mucosal topicalization.
Additionally, a thorough ultrasound assessment of the neck for pathologies such as esophageal (Zenker) diverticulum or an aberrant vertebral artery before performing a stellate ganglion block can avoid potential complications.46 47
The Indication, Acquisition, Interpretation, and Medical Decision-Making (I-AIM) Framework is a standardized, step-by-step guide for clinicians learning a new POCUS skill to identify the appropriate clinical scenarios where it can be used.48 49 As airway ultrasound is an emerging skill for the regional anesthesiologists and pain physicians, table 2 provides a review of clinical case examples in the I-AIM Framework to facilitate knowledge comprehension, integration and translation into the clinical arena.
Examples of cases in airway POCUS following an I-AIM Framework
Lung ultrasound
Point-of-care LUS can be used to assess an acute or critically ill patient with respiratory distress as an extension to physical examination.50 LUS has superior diagnostic accuracy (both sensitivity and specificity) over many traditional imaging. Furthermore, LUS is faster to execute and allows repeated dynamic bedside assessment to monitor disease progression or regression (response to treatment) without radiation exposure.
Overall, LUS excels in its accuracy in detecting lung pathologies such as pneumothorax and pleural effusion (table 3). Additionally, LUS has the advantage of differentiating pleural effusion from lung consolidation, which is not always possible with a chest radiograph.51
Comparison of sensitivity and specificity between LUS versus CXR
Two large meta-analyses found the sensitivity and specificity of LUS for diagnosis of pneumonia to range between 85%–93% and 72%–93%, respectively.52 53 For diagnosis of lung contusion, LUS has a higher degree of diagnostic accuracy than chest radiography with greater sensitivity (95% vs 27%) but similar specificity (96% vs 100%).54 55 LUS is also superior to auscultation in confirming tracheal versus bronchial intubations with higher sensitivity (93% vs 66%) and higher specificity (96% vs 59%).40 A recent meta-analysis suggests a higher sensitivity (94%) and specificity (92.4%) with LUS to diagnose heart failure than routine clinical workup, including chest radiography and natriuretic peptides.56 B-lines are consistently accurate in the diagnosis and monitoring of pulmonary edema and other lung conditions such as acute respiratory distress syndrome, lung infection,57 connective-tissue disorders and lung fibrosis.58
LUS has been used for decades as a means to assess diaphragmatic function.59 The most common methods image the right and left hemidiaphragm by using the liver and spleen as acoustic windows to record diaphragmatic movement in motion mode. The subcostal method, however, can be challenging, particularly on patients with large body habitus. An alternate approach is to assess diaphragmatic function at the zone of apposition by observing diaphragm muscle thickening during the respiratory cycle.60 61 The zone of apposition is defined as the area of the diaphragm close to the lower rib cage where the diaphragm separates from the rib cage.
LUS is based predominantly on the interpretation of artifacts derived by air/tissue interface (eg, pleural line) and real anatomical images in the absence of air/tissue interface (eg, effusion and consolidation). Several lung artifacts (A-lines and B-lines) and signs (lung sliding and pulse) are commonly observed and are highlighted in figure 2.11 Interpretation of lung and pleural artifacts or ‘signs’ has led to the development of standardized protocols to evaluate the lung. These diagnostic protocols follow a step-by-step approach based on particular US profiles.62 In the bedside LUS in emergency protocol,62 profiles have been designed to assess pneumonia, congestive heart failure, chronic obstructive pulmonary disease (COPD), asthma, pulmonary embolism (PE) and pneumothorax with an accuracy >90%. The fluid administration limited by lung sonography protocol63 sequentially rules out an obstructive, cardiogenic, hypovolemic and distributive (usually septic) shock.64
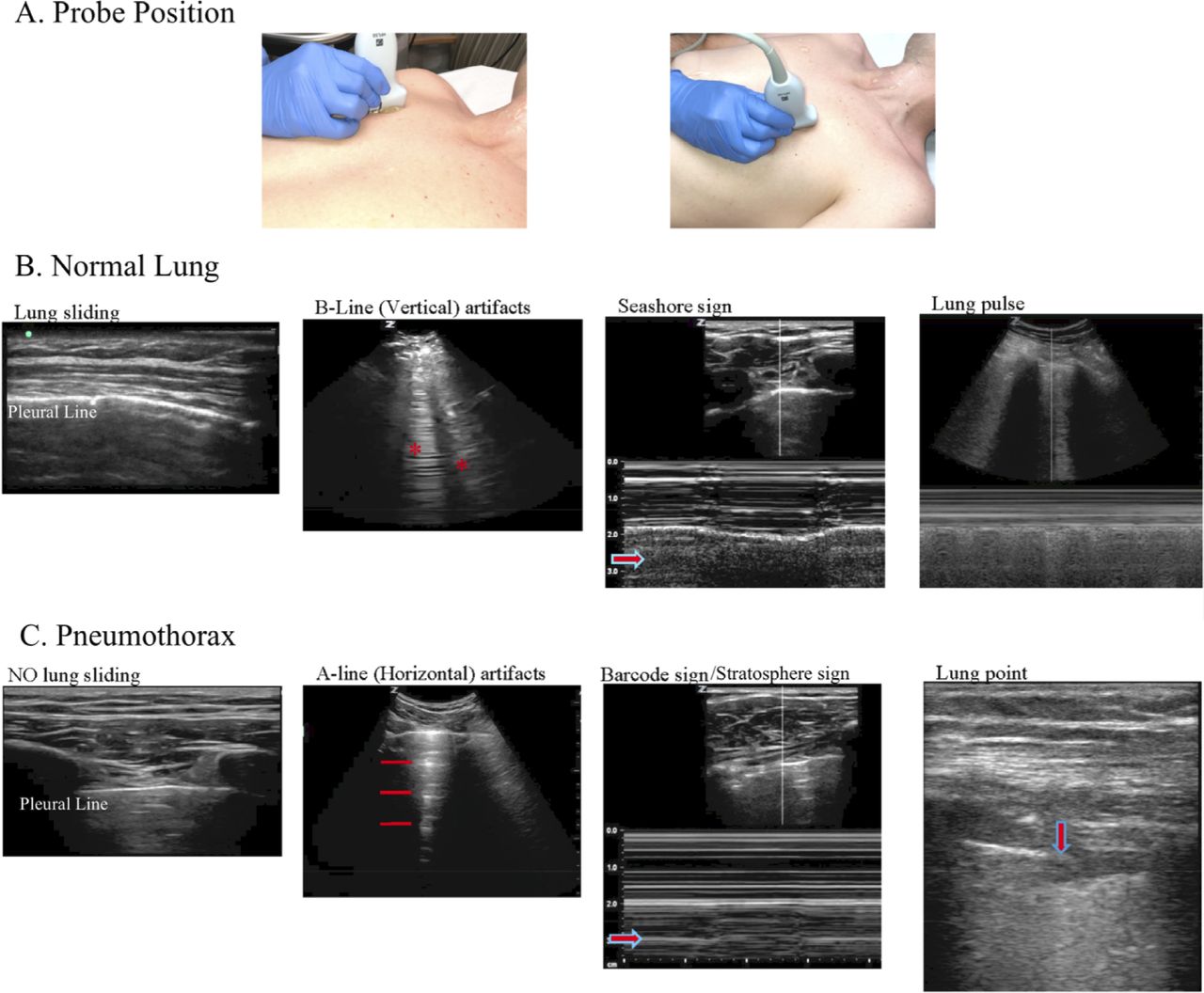
Lung ultrasound (LUS) with normal findings and pathology to rule out and diagnose a pneumothorax. (A) Probe placement for LUS scanning. (B) Normal lung sonoanatomy to rule out a pneumothorax, including lung sliding, B-lines (red asterisks) vertical reverberation artifacts, the seashore sign with arrow pointing to the ‘sandy beach’ visible with normal lung sliding and lung pulse with asterisk showing intermittent movement synchronous with the cardiac rhythm. (C) Sonoanatomy with LUS to diagnose a pneumothorax, including absence of lung sliding, A-lines (red lines) horizontal artifact pattern seen with absence of lung sliding, a barcode sign or stratosphere sign with the arrow pointing to the pattern of parallel horizontal lines continuing beyond the pleural line visible with lack of movement and a lung point.
LUS is a valuable tool for diagnosing and monitoring a variety of pulmonary and pleural complications after regional anesthesia and interventional pain procedures. Pneumothorax54 has been reported as a potential complication of regional anesthesia procedures such as interscalene65 and supraclavicular66 brachial plexus block, erector spinae plane block,67 thoracic paravertebral block68 and pain procedures such as trigger point injection,69 intercostal nerve block,70 thoracic facet joint injection, radio-frequency lesioning71 and celiac plexus block.72 Respiratory symptoms may develop within minutes following these procedures but more commonly develop over several hours. Hemidiaphragmatic paresis is a known complication of above the clavicle brachial plexus blocks (interscalene and supraclavicular) due to a secondary phrenic nerve block.59 73 LUS can be used to help determine pre/post block diaphragmatic function, monitor the return of diaphragmatic function and differentiate between a block complication versus another potential cause of respiratory insufficiency. Also, pleural effusion and hemothorax have been described after supraclavicular block74 and thoracic epidural75 and during interscalene brachial plexus infusion.76 77 Diagnostic LUS can also guide management in acute respiratory failure,78 circulatory shock and cardiac arrest states,79 interstitial syndrome,80 lung consolidation,52 acute decompensated heart failure81 and endobronchial intubation.40 82
FAST examination
The FAST is a well-validated POCUS examination with broad applications in the fields of regional anesthesiology and chronic pain medicine.83 See figure 3 for the four FAST views—subcostal, right upper quadrant, left upper quadrant (LUQ) and pelvic views.
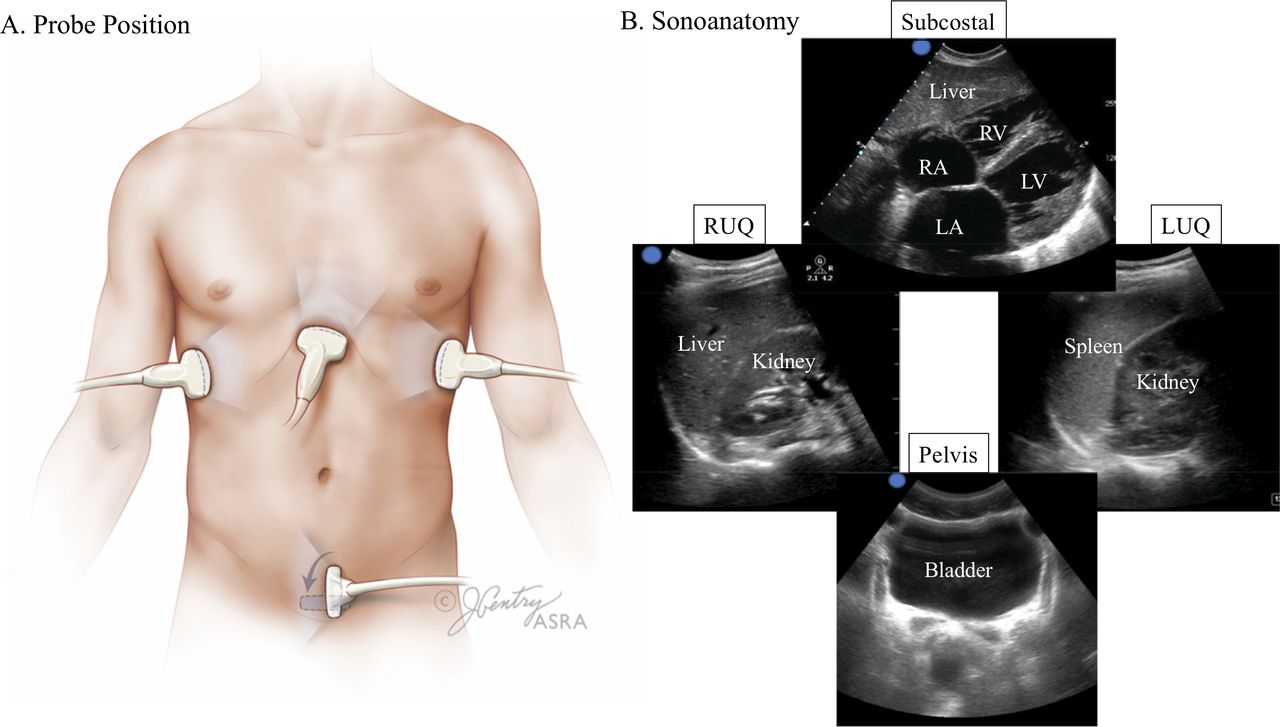
FAST examination probe placement and corresponding sonoanatomy. (A) Probe placement. (B) Sonoanatomy for FAST views including subcostal four-chamber view, RUQ (Morison’s pouch/hepatorenal space), LUQ (perisplenic space) and pelvic view (transverse view). FAST, focused assessment with sonography for trauma; LA, left atrium; LUQ, left upper quadrant; LV, left ventricle; RA, right atrium; RUQ, right upper quadrant; RV, right ventricle.
Initially, the FAST examination was intended to rapidly identify trauma patients who need surgical intervention.82 In the perioperative setting, the indications are an ongoing assessment of trauma patients, critical patients recovering postoperatively, hip arthroscopy patients with severe postoperative pain or showing signs of hemodynamical instability, patients with ascites, patients with peritoneal dialysis and patients following any abdominal surgery.14 84 Additionally, there is a role in gynecologic and obstetrics procedures in the form of the focused assessment with sonography for obstetrics examination.85 86 A positive examination indicates that the patient has at least 300–500 mL of free fluid in the peritoneal space.87 This amount of fluid following abdominal surgery is rarely benign and almost always indicates ongoing hemorrhage. An exception to this situation is intra-abdominal fluid extravasation (IAFE) following hip arthroscopy. IAFE occurs in up to 15% of hip arthroscopy cases and is highly associated with increased pain.84
Chronic pain procedures, such as celiac plexus block, have a risk for bleeding and intra-abdominal hemorrhage.88 Additionally, patients will rarely have a positive FAST examination except in cases of chronic pathology. It is essential to recognize that cirrhotic patients will commonly accumulate enough ascites to produce a positive FAST examination. The same applies to end-stage renal patients treated with peritoneal dialysis.
Gastric ultrasound
Gastric POCUS is used to evaluate stomach contents as they relate to aspiration risk.13 89 Pulmonary aspiration of gastric contents has significant perioperative morbidity and mortality.90 Regional anesthesia and pain management procedures are commonly performed under various degrees of sedation. Chronic pain patients frequently require sedation because of increased sensitivity to needling, opioid-induced hyperalgesia and anxiety. Additionally, deep sedation can be crucial for interventions where patient movement during the procedure may lead to devastating complications, including, for example, inadvertent administration of brain stem injection with trigeminal nerve block or radiofrequency ablation, or pneumothorax with intercostal, or paravertebral nerve blocks.91
The ASA’s recommendations for nil per os (NPO) status are routinely observed in anesthesia and pain medicine practice.92 However, the guidelines are for healthy patients undergoing elective procedures and does not apply to the many complex patients receiving anesthesia or sedation. Opioid dependency, labor, diabetic gastroparesis, advanced renal or liver dysfunction, neuromuscular disorders, ileus, trauma or urgent surgery may prolong gastric emptying, leading to a ‘full stomach’ despite prolonged periods of fasting.93 94 Morbidly obese, pregnant and pediatric patients may also be at increased risk of aspiration.93 94 Additionally, the prandial status may be difficult to assess in patients with a language barrier, altered cognition (such as delirium or dementia) and inconsistent clinical history. Therefore, gastric US should be considered before sedation to verify gastric content for patients with these conditions or when fasting status is unclear.95
Gastric POCUS is most useful when there is clinical uncertainty regarding the status of stomach contents, in other words, when the pretest probability of a ‘full stomach’ is close to 50%.13 96 97 In a prospective study with a simulated clinical scenario with a pretest probability of ‘full stomach’ of 50%, a positive gastric ultrasound examination increased the post-test probability of a full stomach to over 95%, and a negative test decreased the post-test probability to 0.1%.98 Additionally, bedside gastric ultrasound has been shown to change anesthetic management in two-thirds of patients who have not followed fasting instructions before elective surgery99 100 and in pediatric patients undergoing urgent surgery.101 102
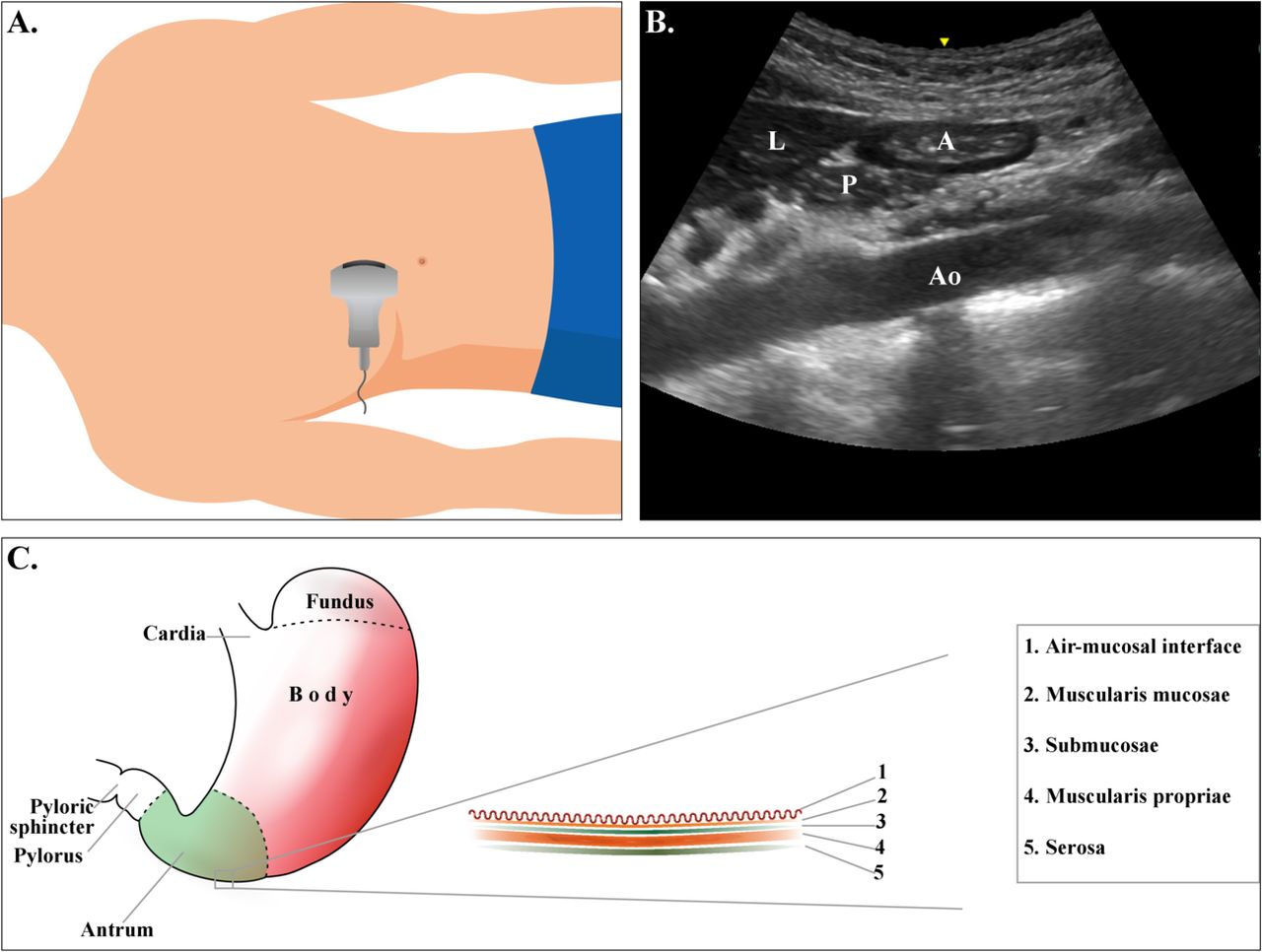
Gastric ultrasound has been studied in adult,103–105 pediatric,101 106 107 obstetric108 109 and morbidly obese110 111 patients. A systematic assessment of the gastric antrum provides information about the entire organ’s contents (figure 4).103 104 112 113 Based on qualitative and quantitative findings, the results of a gastric ultrasound examination may be summarized in a binary manner as an ‘empty’ or a ‘full’ stomach.13 89 96 97 103 104 114 An ‘empty’ stomach has no appreciable content or there is a low volume (<1.5 mL/kg) of hypoechoic fluid consistent with baseline gastric secretions.13 89 96 97 103 104 114 A ‘full’ or ‘not empty’ stomach has evidence of solid particulate content (mixed echogenicity), thick (hyperechoic) fluid or a volume of clear fluid in excess of normal baseline gastric secretions (>1.5 mL/kg) (figure 5).13 96 97 103 104 114
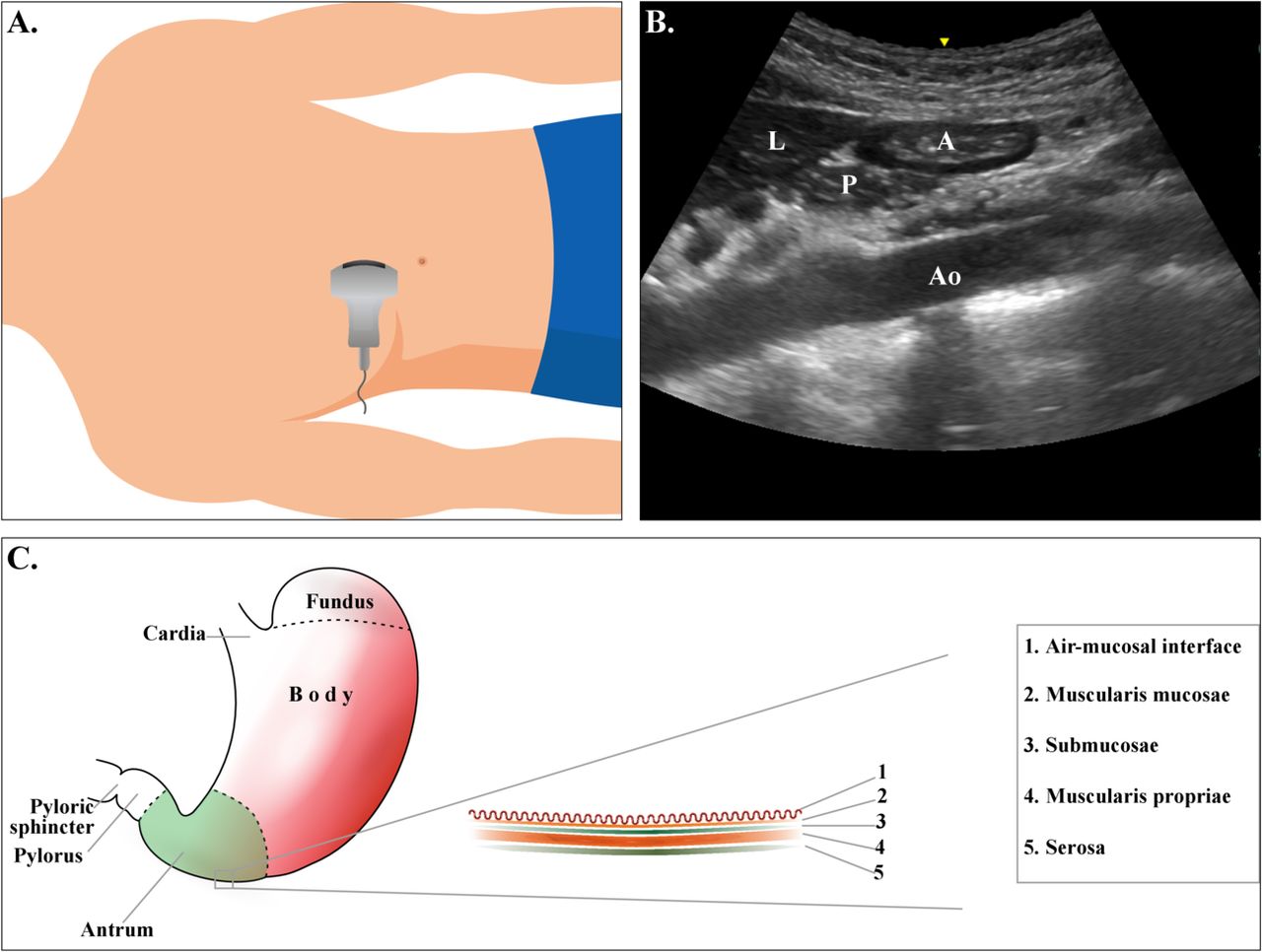
Gastric ultrasound probe placement and anatomy: (A) Probe placement for gastric ultrasound. (B) Basic sonoanatomy of the gastric ultrasound view at the level of the gastric antrum. (C) The five sonographic layers of the gastric wall. Note that with a low-frequency curvilinear transducer, the resolution is decreased and only the muscularis propria is evident. A, antrum; Ao, aorta; L, liver; P, pancreas.

Gastric ultrasound sonoanatomy. (A) Sonographic appearance of the antrum in an empty stomach. (B) Appearance with clear fluid. (C) Appearance soon after a solid meal (early stage solid) with significant air content. (D) Appearance with mixed solid and fluid content (late stage solid). A, antrum; Ao, aorta; L, liver.
Patient position affects antral size as the stomach’s contents pool in the most dependent areas. A more accurate evaluation of the antrum and gastric content is obtained in the right lateral decubitus (RLD) or the semirecumbent position with the head elevated at 45°, as the supine position can underestimate gastric content.103 104 112 115 Given these positional differences, a semiquantitative three-point grading system can be used to assess the presence or absence of clear fluid in the supine and/or RLD positions.104 112 In a grade 0 antrum (empty stomach), fluid is absent in both positions. A grade 1 antrum only has visible fluid in the RLD position, consistent with baseline gastric secretions. Grade 0 and 1 antrums are commonly seen in the fasting state. Alternatively, a grade 2 antrum appears distended with clear fluid in both the supine and RLD positions, and it correlates with gastric volumes>100 mL.104 112 A grade 2 antrum is uncommonly seen in the fasting state. Gastric ultrasound has been shown to be reliable and accurate to identify a ‘full stomach’.98 116
Quantification of gastric antrum volume has been validated against endoscopically guided gastric suctioning110 112 for a wide range of gastric volumes (0–500 mL), patient’s body mass index (19–60) and ages (18–85 years). By placing the patient in the RLD position and measuring the cross-sectional area (CSA) of the gastric antrum at the level of the aorta, the following statistical model can be used to measure gastric volume. Gastric volume (mL)=27.0+14.6×RLD CSA−1.28×age.112 This statistically robust model has the benefit of only one covariate (age) and has been shown to have high intrarater and inter-rater reliability.
Focused cardiac ultrasound
FoCUS has been used in critical care for over 25 years, with the earliest example being the focus assessed transthoracic echocardiography (FATE) protocol.117 While echocardiography was, for decades, the exclusive domain of the cardiologist, those days have passed. Both the American Society of Echocardiography118 and the World Interactive Network Focused on Critical UltraSound119 have published recommendations for the utility of FoCUS at the bedside for specific clinical indications. With the availability of high-quality, hand-carried devices, as well as the expansion of training and expertise, the perioperative setting has been ushered into a new era of bedside ultrasound. Specifically, this evidence has been supplemented by several review articles describing the value of FoCUS in the broad practice of anesthesiology,120 121 regional anesthesia and pain medicine.12 122 Although there are no controlled studies on the utilization of FoCUS in pain practice at this time, there are several scenarios where it could be clinically relevant.
FoCUS aids with patient assessment and clinical optimization, and it can help guide the management of procedural complications. Patients presenting urgently or emergently in the perioperative or periprocedural setting can have undiagnosed and potentially significant cardiac comorbidities. FoCUS can be used to screen high-risk patient populations for undiagnosed cardiac disease when formal echocardiography is not promptly available.118 One clinical example is the elderly patient presenting with a hip fracture.123 In a prospective study, hip fracture patients who received routine bedside cardiac ultrasound screening found that 31% of patients with no audible murmur had aortic stenosis (AS).124 Diagnosis of significant pathologies, such as AS, should alter anesthetic technique, monitoring and postoperative care.125Additionally, bedside cardiac ultrasound on high-risk hip fracture patients did not delay entry into the operating room and may have improved short-term and long-term mortality.123
FoCUS can differentiate among intraoperative and periprocedural complications. In the setting of refractory hypotension following a procedure, FoCUS can differentiate among decreased preload seen with a high spinal, poor contractility related to LAST to the myocardium and other complications associated with more complex cardiac pathologies (eg, myocardial infarction (MI), PE, undiagnosed pericardial effusion).126
FoCUS can also provide repeated evaluation of volume status and ventricular function, which is often not logistically feasible with formal echocardiography118 127–129; additionally, FoCUS may prompt further testing or consultation. For example, although FoCUS has a low sensitivity for PE,130 131 when there is a high level of clinical suspicion and visualization of a dilated right ventricle (RV), it might lead to a more urgent pursuit of definitive imaging like CT angiography (CTA).118 Similarly, while FoCUS should not be used to detect wall motion abnormalities,118 119 global left ventricle (LV) systolic dysfunction in a patient with ECG changes and other supportive symptoms may prompt more rapid cardiology consultation. Of note, negative findings with FoCUS in a clinical situation suspicious for the above pathologies should not discourage pursuing more conclusive investigations, such as ordering advanced imaging, for example, CTA or a complete transthoracic echocardiogram.
There are several clinical scenarios where the utilization of FoCUS can be considered for the chronic pain or interventional pain physician. Radiographic contrast is routinely used in interventional pain management to help detect an intravascular spread of the injectate. While adverse reactions are rare, they can be life-threatening.132 Therefore, pain physicians should be equipped with tools allowing timely management of an anaphylactic reaction or other complications. FoCUS can be potentially used to treat other rare complications of pain management procedures, including hypotension after sympathetic blocks or respiratory and cardiovascular collapse resulting from brainstem anesthesia after trigeminal blocks.133 134
Cardiac arrest
FoCUS is emerging as an important tool to assist with diagnosing and managing patients in cardiac arrest.135 FoCUS plays a role in the asystole and pulseless electrical activity (PEA) pathway in the advanced cardiac life support (ACLS) algorithm. FoCUS can help diagnose treatable pathologies such as hypovolemia, PE, LV failure and pericardial tamponade. FoCUS can also provide insight into prognosis and survivability based on the presence or absence of LV wall motion.126 The focused echocardiographic evaluation in life support protocol describes the optimal timing and FoCUS views to assist in diagnosis and management during ACLS while avoiding interference with other essential treatments.126
FoCUS views
The fundamental FoCUS views are the parasternal long axis, parasternal short axis, apical four-chamber, subcostal four-chamber and the subcostal-inferior vena cava view. These views are sufficient to obtain the qualitative information needed to diagnose gross and potentially life-threatening pathology. This article will not detail view acquisition as there are multiple resources available in publications and online.12 121 136 However, figure 6 highlights the basic views as initially described with the FATE protocol.

Probe placement for a focus cardiac ultrasound examination and modified basic FATE card to Include subcostal IVC view. (A) Probe placement for each FATE view with arrow demonstrating orientation marker direction. (B) Modified basic FATE card with IVC view. 4-C, four-chamber; Ao, ascending aorta; IVC, inferior vena cava view; L, left; LA, left atrium; LV, left ventricle; R, right; RA, right atrium; RV, right ventricle; PS LAX, parasternal long axis, PS SAX, parasternal short axis.
Relevant pathology
FoCUS can identify specific gross pathologies, and the following section will highlight some of the most pertinent pathologies for regional anesthesiologists and pain medicine physicians. Before implementing a new clinical skill, it is essential to understand the indications and subsequent steps required to practice this skill both safely and correctly. The I-AIM Framework is a standardized, step-by-step guide for clinicians learning a new POCUS skill to identify the appropriate clinical scenarios where it can be used.48 49 table 4 has a summary of each cardiac pathology using the I-AIM Framework.
FoCUS I-AIM framework for the regional anesthesiologist
Local anesthetic systemic toxicity
Although LAST is a rare complication for regional anesthesiologists and pain specialists, it is one of the most critical complications to assess and manage appropriately. LAST resulting from peripheral nerve blocks or neuraxial anesthesia can be devastating, causing severe ventricular arrhythmias, myocardial depression and cardiovascular collapse. There is a complex algorithm for the assessment and management of LAST,137 which is particularly relevant when LAST is detected immediately following local anesthetic injection. However, FoCUS can be essential with a delayed presentation of LAST, which can mimic other cardiac pathologies such as MI138 and cardiogenic shock.139 For example, in an otherwise healthy patient presenting with delayed hemodynamic instability following either neuraxial or peripheral nerve block, FoCUS can reveal new-onset myocardial dysfunction suggesting LAST.
Aortic stenosis
AS is often of concern for a patient presenting for urgent or emergent surgery (for example, hip fracture surgery) without a recent medical workup and an audible systolic murmur on auscultation. Hip fracture patients can benefit significantly from neuraxial technique depending on their comorbidities; however, a patient with severe AS is at risk for significant hemodynamic changes and potential complications following induction with neuraxial technique. Although the definitive diagnosis and grading of valvular AS require advanced technical skill and knowledge, FoCUS can be used to detect morphologic signs that suggest AS and prompt additional diagnostic imaging as well as changes in management.118 119 125 140
Hypovolemia
Assessment for hypovolemia before a neuraxial blockade can add considerable value and help guide management. For example, a trauma patient presenting for emergent surgery with an occult bleed or a patient with end-stage renal disease who has recently undergone dialysis may have inadequate preload at baseline, resulting in significant hemodynamic changes and potential cardiac arrest following induction with neuraxial technique. Alternatively, hypovolemia may result from low vascular resistance and reduced afterload, as seen in pathologies such as sepsis or septic shock.
Pulmonary embolism
PE is a relatively common complication following orthopedic procedures (~1.7%)141 and is a significant cause of death following trauma surgery (~1.6%).142 Regional anesthesiologists routinely manage patients at risk for this complication, and it should be high on our differential diagnosis in the perioperative setting of hemodynamic instability and cardiovascular collapse. PE is a time-sensitive emergency that requires a rapid diagnosis to ensure adequate intervention and management. Although FoCUS has a low sensitivity for PE,130 131 it has been shown to have high specificity in the setting of massive PE, particularly in patients without any known preexisting cardiovascular disease.143 144 Occlusion of the pulmonary vasculature, as seen with massive PE, causes an acute elevation in RV pressure resulting in RV dilation and failure. Although emboli are not always visible, multiple FoCUS findings significantly increase suspicion for PE and should direct further evaluation and/or management.
Summary of clinical indications
Based on the evidence presented, there are multiple clinical applications for POCUS; however, to provide additional examples to guide training, this group has provided several educational case-based clinical scenarios (online supplemental file 1 part I—Case-Based Clinical Scenarios) for review that can be implemented into a training program.
Supplemental material
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplementary video
Supplemental material
Supplemental material
Supplemental material
Pediatric POCUS
POCUS is becoming an essential tool for diagnostic and procedural purposes in pediatric acute care medicine, similar to its use in adult populations.145–149 Evidence documents the benefits of gastric,106 150 151 cardiac,147 148 airway and lung152–156 ultrasound use in children. While there are many similarities between POCUS imaging for adults and children, the differing size, physiology, common injury patterns and distribution of comorbidities in children create aspects of POCUS that are unique to pediatric patients.15
When considering the various categories of the I-AIM model, most of the technical aspects of image acquisition are quite similar between children and adults. In general, smaller footprint, higher frequency transducers are used on children, and the depth and focus settings need to be adjusted to size. Otherwise, the views are acquired through the same windows with similar transducer orientations. Obtaining intraoperative images can be easier given that there is a shorter distance to the target structures. However, when infants and children are draped and positioned for surgery, their smaller size limits access to sonographic windows. Indications, interpretation and directed medical management differ due to the pathophysiologic characteristics of pediatric patients. The following sections summarize the distinct aspects of POCUS applications in children to supplement the didactic information already included in the previous sections.
Airway and LUS
Infants and children have an increased risk of endobronchial intubation due to relatively short tracheal length.157 The ASA Closed Claims Project shows that bronchial intubations account for 4% of respiratory claims in children compared with 2% in adults.158 Point-of-care LUS correctly identifies endobronchial intubation in 95%–100% of children.153 159 160 Diagnosis of an interstitial syndrome and pneumothorax is similar to adult data.
The proportionally large head, small mouth opening, bigger tongue and anterior position of the larynx in infants157 predisposes them to accidental esophageal intubation, which occurs in up to 21% of infants.161 Those patients with esophageal intubation have a 4% incidence of hypotension and a 3% incidence of initiation of chest compression.161 Real-time tracheal ultrasound imaging using a high-frequency linear transducer placed transversely just above the sternal notch has a sensitivity and specificity of 98.5%–100% and 75%–100%, respectively, for correctly diagnosing esophageal intubation.153 159 160 Airway ultrasound has the potential to eliminate the need for test ventilation and speed the diagnosis of esophageal intubation.
Abdominal ultrasound
In response to hypovolemia, children have greater hemodynamic compensatory mechanisms to maintain blood pressure until 40% of the blood volume is lost, making a timely diagnosis of intra-abdominal bleeding via abdominal ultrasound advantageous.162–164 The smaller caliber of Foley catheters makes kinking and plugging common, and ultrasound of the bladder can help to differentiate causes of anuria.
Gastric ultrasound
The gastric volume is measured in pediatric patients in mL/kg with a volume greater than 1.5 mL/kg suggesting greater than baseline secretions.107 Children may not understand the importance of remaining NPO and may violate NPO guidelines when not directly observed. Comorbidities placing them at risk for delayed gastric emptying are short gut syndrome and pyloric stenosis. In infants presenting for a repair of pyloric stenosis, pre gastric and post gastric suctioning imaging can be used to direct the anesthetic induction technique.150 Gastric imaging is ideally performed pre induction, but children may not cooperate, making imaging difficult. Clinical applications of gastric ultrasound imaging in children are sparse.101 150
Focused cardiac ultrasound
Given the prevalence of congenital heart disease in children, it is important to realize that bedside cardiac ultrasound has very limited applications in children with congenital heart disease and should not be used to delineate structural abnormalities.118 147 165 Ultrasound imaging of the heart adds important information to the physical examination in children and is most commonly indicated in the setting of undifferentiated hypotension or tachycardia.147 148 166 167 The use of cardiac ultrasound in the setting of pediatric cardiac arrest is distinct from adult practice. While insufficient evidence exists to recommend for or against the routine use of FoCUS during pediatric cardiopulmonary resuscitation (CPR), the 2010 International Pediatric Basic and Advanced Life Support guidelines recommend that ‘bedside cardiac echocardiography may be considered to identify potentially treatable causes of a cardiac arrest when appropriately skilled personnel are available, but the benefits must be carefully weighed against the known deleterious consequences of interrupting chest compression’.168 Ultrasound can be used to identify reversible causes of cardiac arrest, including cardiac tamponade, severe hypovolemia and pulmonary air embolus.126 169–172 The diagnosis of cardiac standstill or PEA in children carries a different prognosis and algorithmic sequence compared with adults. Forty per cent of intraoperative cardiac arrests in children occur from a respiratory etiology, and restoration of oxygen delivery alone may lead to a return of spontaneous circulation.173 Extracorporeal membrane oxygenation for cardiac resuscitation (E-CPR) as a rescue strategy in children in cardiac arrest is not uncommon.174 There is evidence that E-CPR for pediatric patients with in-hospital arrest requiring >10 min of standard CPR is associated with improved survival and neurologic outcomes. There is also evidence that prolonged conventional CPR with ongoing use of epinephrine every 3–5 min (as recommended by pediatric advanced life support protocol) and resultant elevated systemic vascular resistance may have deleterious effects when implementing E-CPR by limiting extracorporeal membrane oxygenation pump flows.175 More rapid determination of myocardial standstill using cardiac ultrasound may facilitate more rapid progression to E-CPR with improvement in outcomes.
Handheld devices in POCUS applications
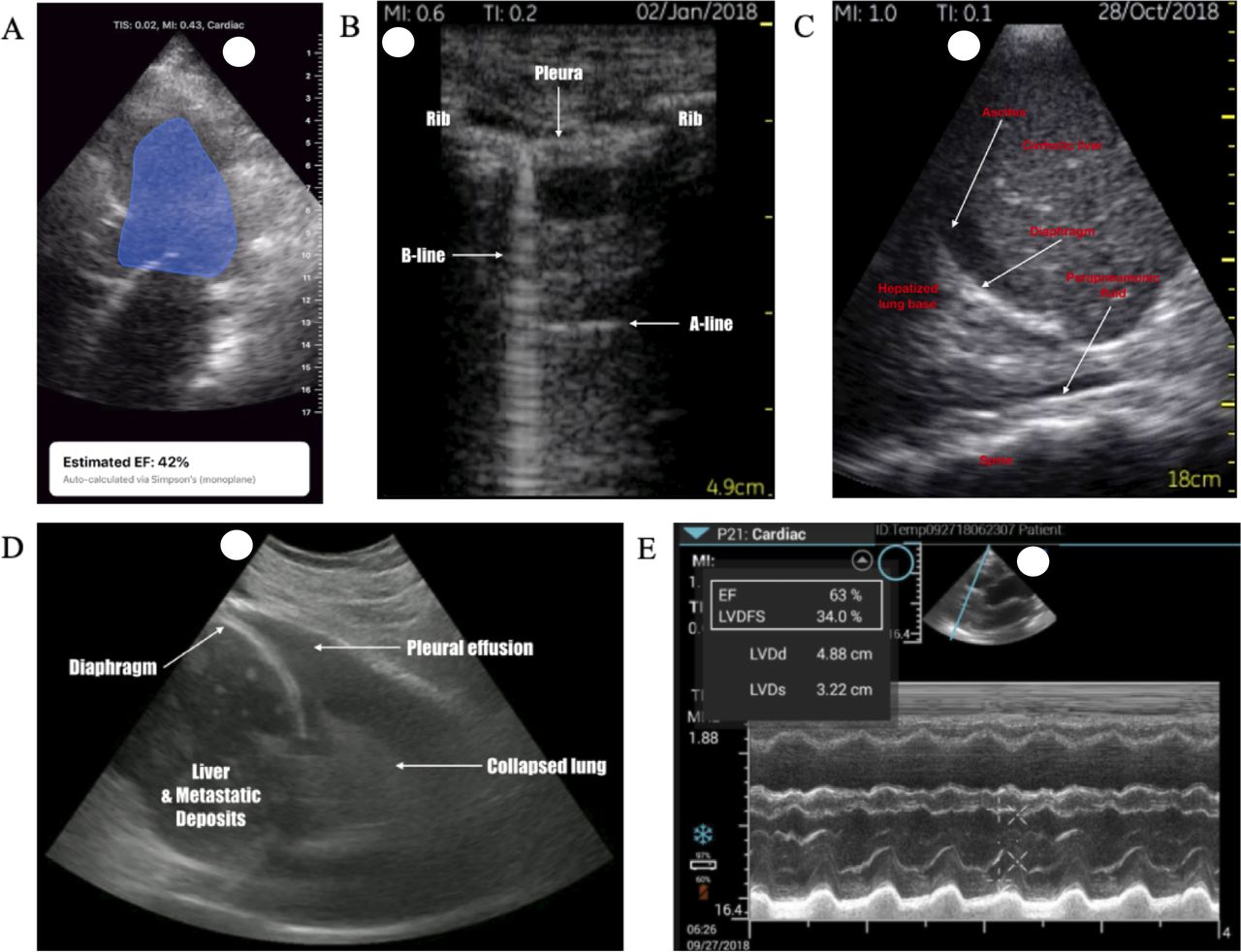
Increasingly portable ultrasound machines have led to an exponential uptake in utilization and discussion in the literature176 with some devices priced for individual purchase.177 178 Traditional ultrasound machines have many barriers to use, including size, cost and difficulty to operate. Therefore, handheld devices can be an introductory device before becoming competent in advanced ultrasound applications.179 For example, the introduction of handheld ultrasound devices in medical schools aids with teaching functional anatomy and with implementing a clinical POCUS curriculum.180 181 Examples of basic images obtained from a selection of these devices are shown in figure 7.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Various images obtained from a range of portable handheld devices. (A) Apical four-chamber view with auto-ejection fraction calculation. (B) LUS—upper zone view demonstrating anatomy and pathology. (C) Right lung base/right upper quadrant view showing cirrhotic liver, ascites and parapneumonic fluid. (D) Right upper quadrant abdominal scan with lung base view, demonstrating metastatic cancer in liver with pleural effusion. (E) Parasternal long axis of the heart, demonstrating calculation of fractional area change. EF, ejection fraction; LUS, lung ultrasound; LVDd; left ventricular end-diastolic diameter; LVDFS, left ventricular dimension fraction shortening; LVDs, left ventricular end-systolic diameter.
Limitations in image quality, screen size, available memory and data encryption make handheld ultrasound devices better used to extend the physical examination rather than comprehensive diagnostics tools. Sterility is of utmost importance given the potential for frequent use and the ability to attach to personal devices.
Critics of POCUS often express concern that it deprioritizes patient contact during the physical examination; however, handheld ultrasound can bridge the gap between the clinician and diagnostic tests while facilitating communication with visual confirmation of findings in real time.182 The presentation of pathology can aid compliance and buy-in for additional testing/imaging.
To offer a balanced approach to handheld devices, some of the advantages and disadvantages are shown in box 1.
Summary of advantages and disadvantages to handheld devices using an I-AIM Framework.
Advantages and disadvantages of handheld devices in POCUS applications:
Advantages
Portability/convenience.
Increased teaching and training opportunities due to portability/affordability.
App-based software upgrades offering AI and other increased functionality.
Ease of transport.
Minimal boot-up time.
Practical in confined spaces.
Simple and less intimidating to beginners.
Cloud-based storage available.
WiFi image upload possible with DICOM linkage to existing institution systems.
Potential to use existing electronic equipment (Android-based/Apple-based devices).
Limitations and pitfalls
Poorer image quality than higher-end systems:
More prone to artifacts.
Greater risk for image misinterpretation.
Small screen size:
Limits image acquisition.
Prevents multiple functionalities on the screen.
Increased phantom scanning (scanning without image capture/record).
Limited compatibility with existing image storage system.
Limited advanced functionality (ie, pulsed or continuous wave Doppler).
Potential for overuse and misinterpretation of incidental findings.
Misplacement, theft or loss of the device.
Scanning time limited by battery life.
Transducer selection is device dependent.
Probes overheat.
Cloud security/governance challenges
Wireless devices prone to drop-out/‘jumpy images’/limited image quality on probe movement.
Sterility concerns.
AI, artificial intelligence; DICOM, Digital Imaging and Communications in Medicine; POCUS, point-of-care ultrasound; WiFi, wireless fidelity.
Summary
POCUS is an essential skill for all regional anesthesiologists and pain physicians to help diagnose relevant complications related to routine practice and guide perioperative management. The growing evidence supporting the clinical utility of POCUS has been outlined to lay the foundation for part II of the recommendations. Part II will provide structured guidelines and strategies for the education of the trainee and postgraduate learner.
The expert panel acknowledges that clinical evidence supporting POCUS is evolving, and certain endpoints, such as improved survival during CPR, require additional validation.181 182 All interventions have risks or downsides, including potential false-negative findings, higher rates of interventions or delayed bedside management due to the performance of an examination.181 182 Because of these concerns, adequate training and future investigation into applications are essential for the adaptation of POCUS into the perioperative and periprocedural setting.
Regarding POCUS skills that fall outside of the traditional scope of regional anesthesiologists and pain specialists, such as the FAST examination, the expert panel emphasizes learning to perform these skills as well. As these skills are introduced into new clinical practice realms, there is great potential to illuminate novel clinical scenarios in the perioperative and periprocedural setting that can aid in patient assessment and management.
Acknowledgments
The authors would like to thank the American Society of Regional Anesthesia and Pain Medicine’s (ASRA) Guidelines Committee and Board of Directors for their feedback and support in the design of the recommendations. The authors would also like to thank Professor Erik Sloth, MD, PhD, for his ongoing inspiration as well as permission to present an adaptation of the focus assessed transthoracic echo card.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @shaskinsMD, @PerlasAnahi, @elboghdadly, @janboublik MDPhD, @hariharan_shank, @NarouzeMD
Contributors All authors are responsible for the content and have read and approved the manuscript for submission to the American Society of Regional Anesthesia and Pain Medicine.
Funding Anahi Perlas, MD receives funding from a Merit Award, Department of Anesthesiology and Pain Medicine, University of Toronto.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement There are no data in this work.