Article Text

Abstract
Background Dysfunction of the thalamocortical connectivity network is thought to underlie the pathophysiology of the migraine. This current study aimed to explore the thalamocortical connectivity changes during 4 weeks of continuous transcutaneous vagus nerve stimulation (taVNS) treatment on migraine patients.
Methods 70 migraine patients were recruited and randomized in an equal ratio to receive real taVNS or sham taVNS treatments for 4 weeks. Resting-state functional MRI was collected before and after treatment. The thalamus was parceled into functional regions of interest (ROIs) on the basis of six priori-defined cortical ROIs covering the entire cortex. Seed-based functional connectivity analysis between each thalamic subregion and the whole brain was further compared across groups after treatment.
Results Of the 59 patients that finished the study, those in the taVNS group had significantly reduced number of migraine days, pain intensity and migraine attack times after 4 weeks of treatment compared with the sham taVNS. Functional connectivity analysis revealed that taVNS can increase the connectivity between the motor-related thalamus subregion and anterior cingulate cortex/medial prefrontal cortex, and decrease the connectivity between occipital cortex-related thalamus subregion and postcentral gyrus/precuneus.
Conclusion Our findings suggest that taVNS can relieve the symptoms of headache as well as modulate the thalamocortical circuits in migraine patients. The results provide insights into the neural mechanism of taVNS and reveal potential therapeutic targets for migraine patients.
- complementary therapies
- transcutaneous electric nerve stimulation
- treatment outcome
- chronic pain
Statistics from Altmetric.com
Introduction
Migraine is a highly prevalent neurological disorder1 that can impose great personal and socioeconomic burdens.2 Therapeutic strategies for migraine are mainly based on preventive and abortive drug therapy, which are only partially effective and bear unpleasant side effects inevitably.3 Thus, it is necessary to explore a new therapy for migraines with better efficacy and less side effects.
The vagus nerve consists of a complex network that regulates pain, mood, and the neuroendocrine-immune axis.4 5 Accumulating evidence suggests that transcutaneous vagus nerve stimulation (tVNS) at the external ear (auricular branch of vagus nerve, ABVN) or the neck (the cervical branch of vagus nerve) can induce antinociception, which may affect peripheral and central nociception, inflammatory responses and pain-related behavior.4 6–8 Previous studies suggest that cervical tVNS can reduce the number of migraine attacks9–11 and relieve acute pain in migraine patients.12–14
However, there is a relative paucity of literature on auricular tVNS treatment of migraine. In the only randomized, controlled clinical trial that tested the effects of taVNS by stimulating the concha of the outer ear with different frequencies, investigators found that patients in the 1 Hz group had a significantly larger reduction in headache days per 28 days than the patients in the 25 Hz group.15 Nevertheless, the effects of tVNS at ABVN at 1 HZ compared with sham stimulation at the vagus free area of the outer ear in migraine patients remains unclear, as well as the underlying mechanism behind it.
Although still under investigation, literature suggests that the thalamus holds an important position in our understanding of allodynia, central sensitization and photophobia in migraines.16 Further studies indicate that circuits between the thalamus and cortex play important roles in mediating the perception of pain, and that functional and anatomical alterations in the thalamocortical (TC) circuits are involved in the development and maintenance of migraines.17–19
In a recent study, we found that 1 Hz taVNS can produce widespread brain activity changes in brain regions such as the solitary nucleus, the locus coeruleus, the raphe nuclei, and the insula in patients with migraines.20 In addition, investigators found that vagal afferents can activate the ascending antinociceptive pathway from the periaqueductal gray (PAG) and raphe nuclei onto the thalamus.21 Taken together, these findings suggest that taVNS may modulate TC circuits.
In this study, we investigate the modulation effect of taVNS on clinical outcomes, TC circuits, and their association in migraine patients. Specifically, we compare clinical outcome and resting state functional connectivity (rsFC) using a functionally parceled thalamus seed-based approach before and after 4 weeks of taVNS (as compared with sham taVNS) in patients of migraine without aura. We hypothesize that longitudinal treatment with taVNS could significantly modulate the rsFC of the TC network and reduce symptoms in migraine patients.
Methods
Standard protocol approvals, registration and consents
Patients with migraines were recruited between May 2017 and May 2019 from the Second Affiliated Hospital of Guangzhou University of Chinese Medicine. This study protocol was registered on the Chinese Clinical Trial Registry (ChiCTR-INR-17010559, February 7 2017, http://www.chictr.org.cn/hvshowproject.aspx?id=11101). Informed consent was obtained from all participants.
Study population
Migraine diagnosis was based on the International Classification of Headache Disorders, second Edition by licensed neurologists. Episodic migraineurs without aura were recruited for this study, with inclusion criteria as follows: (1) aged 18–45 years old; (2) right-handed; (3) have at least 6 months of migraine duration; (4) have at least two headache attacks per month; (5) have not taken any prophylactic headache medications during the past 1 month and (6) have not taken any psychoactive or vasoactive drugs during the past 3 months.
Excluded criteria includes the following: (1) headache induced by other diseases; (2) headache attack within 48 hours prior to the experiment or during the experiment; (3) pregnancy or lactation; (4) any other chronic pain conditions; (5) severe head deformity or intracranial lesions; (6) score on the Self-Rating Anxiety Scale (SAS) or the Self-Rating Depression Scale (SDS) >50.
Experimental design
A single-blinded, randomized and controlled clinical trial was applied in this study. All patients were recruited from the outpatient unit of the Department of Neurology in the Second Affiliated Hospital of Guangzhou University of Chinese Medicine and prescreened by neurologists between May 2017 and May 2019. After passing the prescreening process, potential eligible patients provided informed consent in the presence of a study physician and were randomly assigned to either the real or the sham taVNS treatment group based on an SPSS generated randomization sequence. All participants were blinded to the treatment (real vs sham) they received.
The study lasted for 8 weeks: 4 weeks before the treatment (the baseline) and 4 weeks during the treatment. Patients were instructed to complete headache diary records after enrollment. The diaries were collected at week four and week eight. The headache diary documented the onset time, duration, pain intensity (measured by Visual Analog Scale (VAS) score), accompanying symptoms, and rescue medication use.
Intervention
The stimulation was applied with an electronic acupuncture treatment instrument (SDZII, Huatuo, Suzhou, China) by trained physicians. Similar to a previous taVNS study on migraine,15 we have chosen the frequency of 1 Hz with the duration of 0.2 ms. The stimulation was continuously applied for 30 min during each session. Stimulation intensity was adjusted to the strongest sensation that the patients could tolerate without pain (approximately 1.5–5 mA). All the patients included in the final analysis completed 12 treatment sessions in total during the 4-week treatment.
Similar to our previous studies,20 real taVNS was applied at the left cymba concha (the real stimulation site).22 The control (sham) stimulation was on the left tail of the helix (figure 1). We chose these stimulation sites based on a previous anatomical dissection study which reported that the cymba concha is innervated by the ABVN in 100% of the exposed auricle, while the tail of helix is free of cutaneous vagal innervation.23
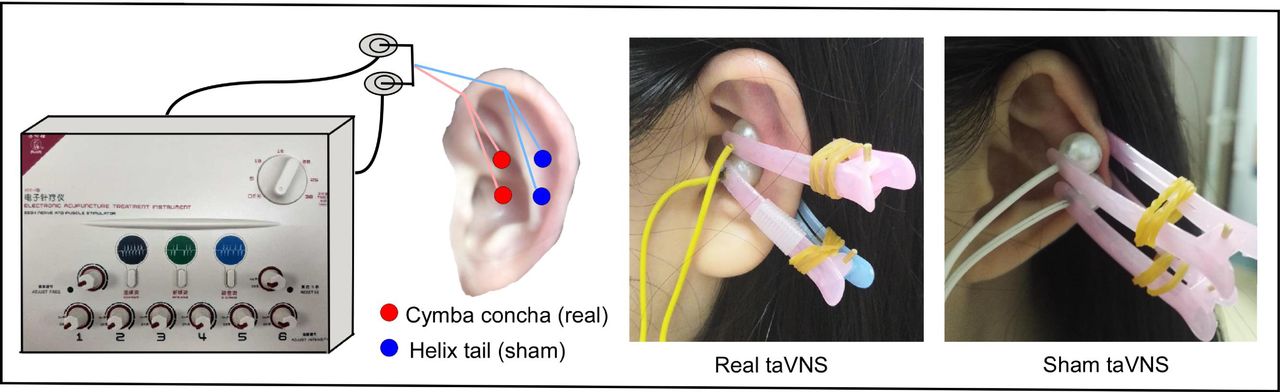
Real and sham taVNS stimulation site on left ear. taVNS, transcutaneous vagus nerve stimulation.
Clinical outcomes
All patients completed the self-recorded headache diaries for the baseline period (week 1–4) and during the treatment period (week 5–8). Similar to a previous study on taVNS treatment of migraine,15 we chose mean reduction in the number of migraine days as the primary outcome.
As for secondary outcomes, we evaluated: (1) mean reduction in pain intensity as measured by the 0–10 VAS of each migraine; (2) mean reduction in migraine attack times; (3) increased scores on the Migraine Specific Quality-of-Life Questionnaire (MSQ); (4) reduction in Zung SDS and Zung SAS. All of the staff who collected clinical measurements were blinded to the treatment distribution of the patients.
Statistical analysis for clinical outcome
The effect of taVNS was estimated by comparing changes of migraine days using a linear mixed model with time, group allocation and interaction between the two as fixed effects, patients as a random effect, and age and gender as covariates. The analysis was performed using R V.3.1.0, with the lme424 and lmerTest.25 We also performed similar analysis on the secondary clinical outcomes including pain intensity, frequency of migraine attack times, MSQ, SDS and SAS.
Functional MRI data acquisition
All patients participated in identical functional MRI (fMRI) scanning sessions before and after 4 weeks of treatment. All MRI/fMRI (MRI/fMRI) scans were conducted on a 3.0 T Siemens MRI scanner (Siemens MAGNETOM Verio 3.0 T, Erlangen, Germany) with a 24-channel phased-array head coil.
Resting state fMRI encompassing the whole brain was acquired with the following parameters: repetition time (TR)=2000 ms, echo time (TE)=30 ms, field of view (FOV)=224 mm×224 mm, matrix=64×64, flip angle=90°, slice thickness=3.5 mm, interslice gap=0.7 mm, 31 axial slices paralleled and 240 time points. Subjects were told to stay awake, remain motionless, and keep their eyes closed during the 8 min resting-state fMRI scan. T1-weighted high-resolution structural images were applied with the following parameters: TR=1900 ms, TE=2.27 ms, flip angle=9°, FOV=256 mm×256 mm, matrix=256×256 and slice thickness=1.0 mm.
Data preprocessing
Functional images were preprocessed using CONN18.a.26 The preprocessing steps included slice timing correction, realignment, segmentation of structural data, spatial and functional normalization into standard stereotactic MNI space, and reslicing into 2×2×2 mm voxels.
To minimize the effects of head motion, subjects whose mean frame displacement (FD) exceeded 0.2 mm were excluded27 28 (no subjects were excluded in the data analysis). We identified outlier time points in the motion parameters and global signal intensity using ART implemented in CONN toolbox (https://www.nitrc.org/projects/artifact_detect/). Linear regression using white matter (WM) and cerebrospinal fluid (CSF) signals, linear trend, subject motion (six rotation/translation motion parameters and six first-order temporal derivatives), and outliers (scrubbing) was conducted to remove any confounding factors. After that, the residual BOLD time series was band-pass filtered with a frequency window of 0.008–0.09 Hz. Preprocessed data remained unsmoothed for further winner-take-all thalamic functional parcellation. Data were smoothed at a Gaussian kernel of 6 mm Full Width at Half Maximun (FWHM) for seed-based analysis.
Parcellation of thalamus
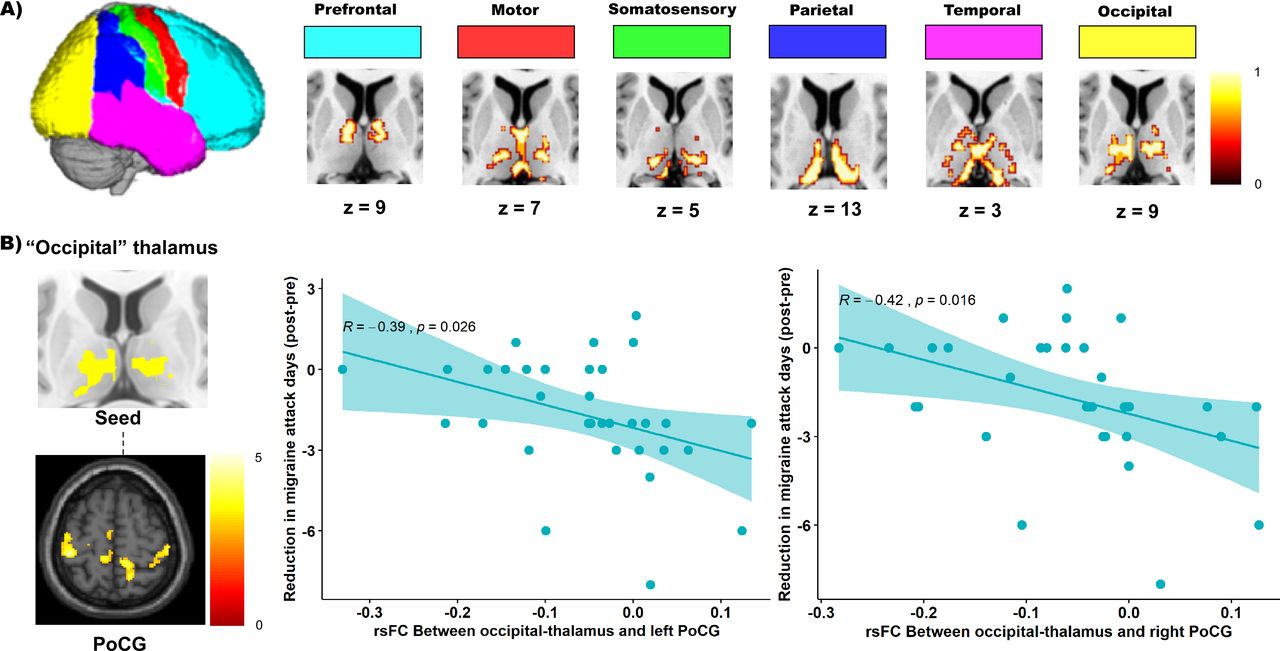
Similar to the procedure in previous studies,29 30 the cortex of the whole brain was partitioned into six bilateral cortical subregions: the prefrontal, motor, somatosensory, parietal, temporal and occipital cortex (figure 2A, see online supplemental table e1 for detailed region components) based on a priori-defined nonoverlapping Harvard-Oxford probabilistic cortical atlas threshold at 25% (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/Atlases). We also localized the entire thalamus based on the Harvard-Oxford subcortical atlas.
Supplemental material
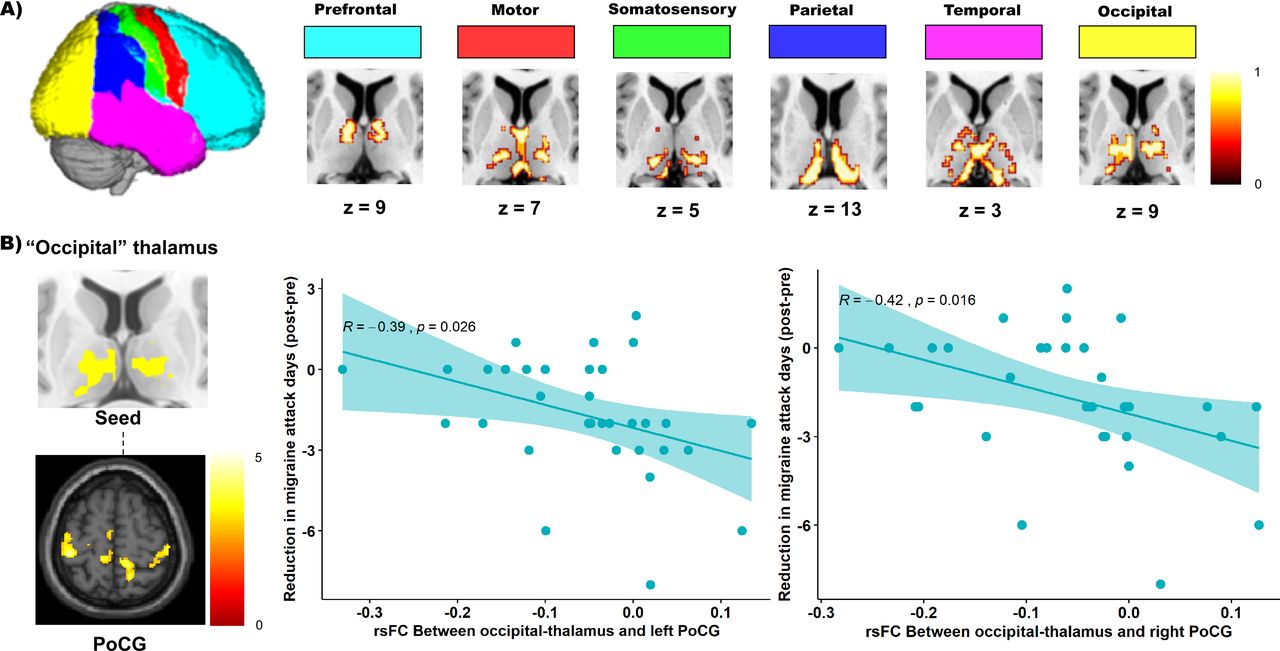
Functional parcellation map of the thalamus and seed-based analysis result of the thalamic motor seed. (A) Left: demonstration of the six bilateral cortical brain regions. Right: six parceled thalamus subregions corresponding to prefrontal, motor, somatosensory, parietal, temporal and occipital cortex presented in the axial view of the brain. (B) Left: seed-based functional connectivity result of the ‘occipital’ thalamic seed showed decreased connectivity with bilateral postcentral gyrus in the real taVNS group after treatment compared with the sham taVNS; right: correlation between the rsFC change (post >pre) of ‘occipital‘ thalamic seed-bilateral POG and the mean reduction of migraine days in the real taVNS group. PoG, postcentral gyrus; rsFC, resting state functional connectivity; taVNS, transcutaneous vagus nerve stimulation.
Then, the BOLD signals of six bilateral cortical subregions and the entire thalamus were extracted. Partial correlations between the mean BOLD signal of each cortical subregion and the signal in each thalamic voxel were applied, adjusting the signal variance from other cortical subregions. After that, custom winner-take-all strategy31–33 was applied, that is, partial correlations were averaged across all patients and each thalamic voxel was labeled according to the cortical subregion with the highest partial correlation value. Thus, we functionally parceled the thalamus into six regions corresponding to the predefined cortical regions. The six thalamic subregions were used as seeds (regions of interest) in the following seed-based rsFC analysis.
Seed-based functional connectivity analysis
The functional connectivity analysis was performed using the CONN toolbox. In the first-level analysis, we produced a correlation map for each patient by extracting the BOLD time series from each thalamic seed and computing Pearson’s correlation coefficients between the time series in every thalamic seed and all other voxels of the whole brain, respectively. Correlation coefficients were Fisher transformed into ‘Z’ scores to increase normality. Seed-to-voxel second-level analyses were performed using a mixed-designed analysis of variance with treatment (real taVNS vs sham taVNS) entered as the between-subject factor, time (pretreatment vs post-treatment) as the within-subject factor, and age and gender as covariates. A threshold of voxel-wise p<0.005 uncorrected and cluster-level p<0.05 false discovery rate (FDR) corrected was applied for comparison.
Results
Participants and baseline characteristics
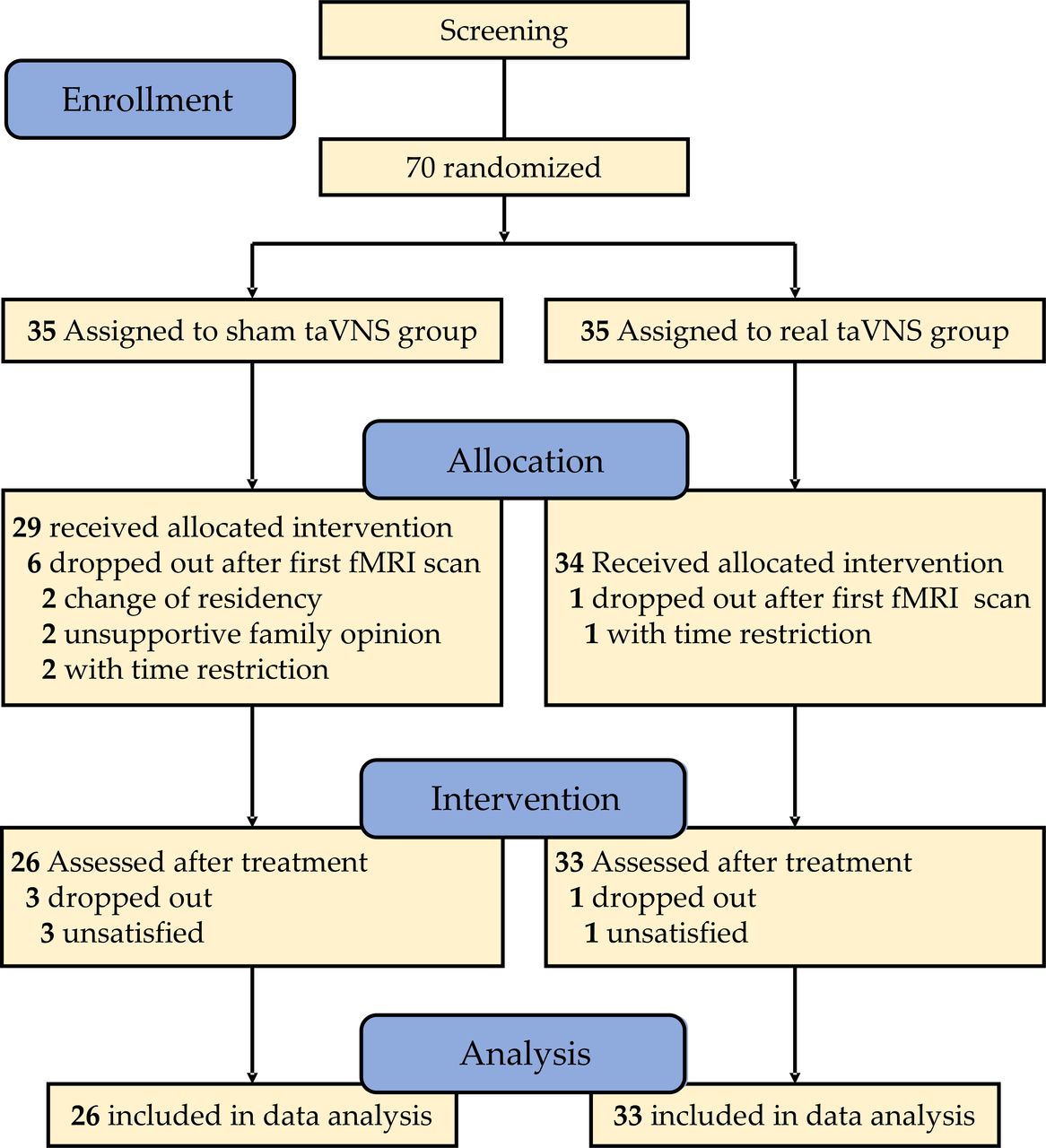
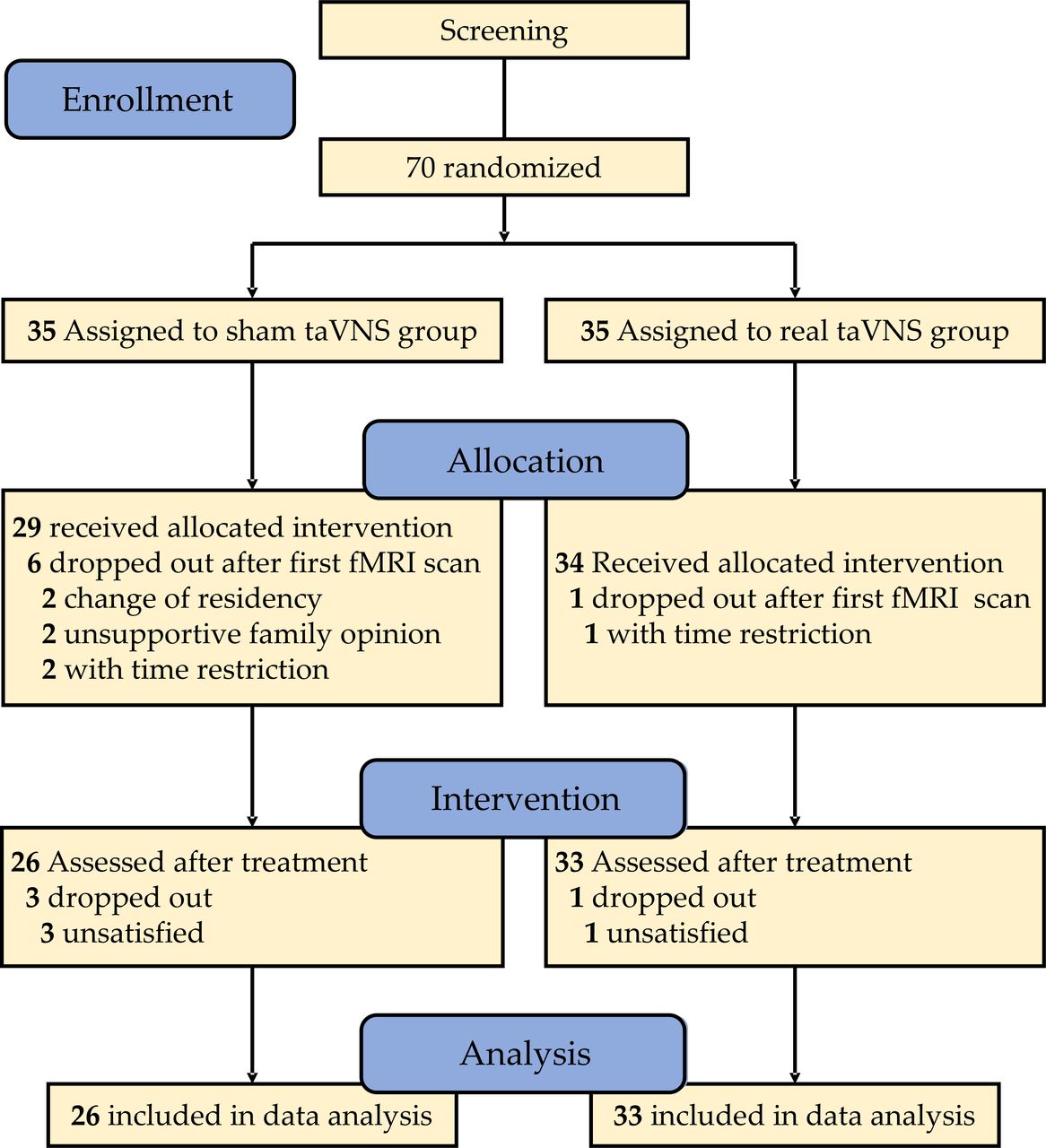
Seventy patients were randomized after screening and baseline assessment (35 in the taVNS group, 35 in the sham taVNS group). Fifty-nine patients (33 in the taVNS group, 26 in the sham taVNS group) completed the two fMRI scans (baseline and after 4-week treatment). See figure 3 for reasons for dropping out in each group. No patients were excluded due to head motion under the previously defined standard.
{kind=link}
{kind=link}
{kind=link}
Flow chart of screening, randomization and intervention. fMRI, functional MRI; taVNS, transcutaneous vagus nerve stimulation.
Baseline characteristics of the two groups were shown in online supplemental table e2. There was no significant difference between the real and sham group in age, gender, number of migraine days, pain intensity, MSQ, SAS and SDS at baseline.
Clinical outcome
The clinical outcome measurements and corresponding statistics are summarized in table 1. Significant time ×group interaction effects were found in the primary outcome variable (mean reduction in numbers of migraine days [F (1,57)=5.41, p=0.024]), two of the secondary outcome variables (mean reduction in headache pain intensity [F (1,57)=7.52, p=0.008], and migraine attack times [F (1,57)=6.29, p=0.015]). For the primary outcome measure, the intra-group difference was an absolute reduction of −2.5 days (95% CI −3.3 to −1.6; p<0.001) in the group treated with real taVNS compared with −0.7 days (95% CI −2.1 to 0.6; p=0.267) in the sham group. There were no significant interactions or between-group effects on other clinical outcome measurements (MSQ, SAS, SDS).
Clinical outcome measurements in the real and sham taVNS groups
Functional connectivity results
Six functionally parceled thalamic subregions corresponding to the prefrontal, motor, somatosensory, parietal, temporal and occipital cortex were shown in figure 2A (see online supplemental figure e1 for details). Functional subdivisions of the thalamus were similar to the previous studies using the winner-take-all parcellation strategy.31 34
The result of seed-based analysis using six functionally parceled thalamic subregions is shown in online supplemental table e3. Compared with the sham group, the real taVNS group showed increased connections between ‘motor’ thalamic seed with the rostral anterior cingulate cortex/medial prefrontal cortex (rACC/mPFC) after treatment. Also, real taVNS, compared with sham taVNS, showed decreased connectivity between (1) the ‘parietal’ thalamic seed and the right supramarginal gyrus (SMG); (2) the ‘temporal’ thalamic seed and the right superior parietal lobule (SPL); (3) the ‘occipital’ thalamic seed and the bilateral postcentral gyrus (PoG), right SMG and right precuneus (PCu)/SPL.
Given the important role of the rACC/mPFC and somatosensory cortex in the TC network of vagus nerve stimulation,35 we extracted the Fisher z value of the connectivity between the rACC/mPFC-‘motor’ thalamic seed and the connectivity between the PoG-‘occipital’ thalamic seed, and explored the association between the functional connectivity change and corresponding clinical improvement (reduction of number of days, pain intensity, and attack times).
Pearson’s correlation showed that the FC change of the ‘occipital’ thalamic seed and the bilateral PoG is significantly correlated with the reduction of the migraine days (left: R=−0.39, p=0.026; right: R=−0.42, p=0.016) in the real taVNS group after treatment (figure 2B), and no significant correlations were found in sham group (left: R=−0.2, p=0.33; right: R=−0.19, p=0.36). There is no significant correlation between the FC change of rACC/mPFC and the corresponding clinical improvements in both real and sham groups.
Discussion
In this study, we investigated the modulation effect of taVNS in migraine patients. We found significant alleviation in the number of migraine days, pain intensity and attack times after real taVNS treatment when compared with sham taVNS treatment. The taVNS significantly modulated the TC functional connectivity. In particular, we found that the thalamic subregions associated with the motor and occipital cortex had a significant functional connectivity change with two important cortical regions in the vagus afferent network- the rACC/mPFC and somatosensory cortex respectively. When compared with the sham group, the real taVNS group showed increased connectivity between the ‘motor’ thalamic subregion and the rACC/mPFC, and decreased connectivity of the ‘occipital’ thalamic subregion with bilateral PoG. Furthermore, this decreased connectivity is significantly associated with the primary variable (mean reduction of migraine days) in the taVNS group.
Consistent with the previous studies, we found that 1 Hz taVNS can significantly relieve the symptoms of migraine when compared with sham taVNS. Straube et al15 showed that patients who had received 1 Hz taVNS had a significant reduction in headache days compared with patients who had received 25 Hz after 3 months of treatment, highlighting the potential of 1 Hz taVNS for migraine treatment. Our findings are also in line with studies using other non-invasive vagus nerve stimulation (at the neck), which demonstrated the potential of VNS for migraine treatment. For instance, two multicenter clinical trials have shown that self-administered neck VNS three times per day may reduce the number of migraine days in chronic migraine patients.9 10
The role of the thalamus in migraine pathology has been well documented. A previous positron emission tomographic study showed posterior/lateral thalamus activation during a migraine attack.36 Hodkinson et al found increased low-frequency oscillations (as measured by fractional amplitude of low frequency fluctuation, fALFF) in the TC network of patients with migraines during their interictal phase. This increased fALFF in the thalamus was selectively associated with headache frequency.37 More recently, investigators found alteration of thalamic functional connectivity in brain regions associated with pain modulating and pain encoding networks during migraine attacks when compared with their interictal period.18 These findings demonstrate the important role of the TC circuits in the pathophysiology of migraines.
In this study, we found that taVNS can significantly modulate the TC circuits. Specifically, real 4-week taVNS treatment produced increased rsFC between the ‘motor’ thalamic subregion with the rACC/mPFC when compared with sham taVNS treatment.
Literature suggests that the motor cortex may play an important role in pain modulation. For instance, motor cortex stimulation has shown particular promise in the treatment of refractory pain.38 39 Non-invasive motor cortex stimulation has been used to treat different chronic pain disorders.40 41 Timothy et al showed anodal M1 tDCS enhanced activation in brain regions such as the mPFC, ACC and PAG, leading to the descending inhibition of pain.42
The rACC/mPFC are key regions in the descending pain modulation system.43 In previous studies, we found that compared with healthy controls, migraine patients showed reduced rsFC between the rACC/mPFC and PAG, another key region in the descending pain modulatory system.44 We also found that the rACC/mPFC had decreased functional connectivity with brain regions within the default mode network and increased rsFC with sensorimotor and salience networks in chronic low back pain patients.45
The rACC/mPFC are also important targets for the antinociceptive effects of opioids. A human positron emission tomography study demonstrated that the opioid receptors were enriched in cortical projections of the medial pain system in the cingulate and prefrontal cortex.46 Alexandre et al found that migraine patients had abnormal activation of opioid receptors in the prefrontal cortex during migraine attacks.47 Taken together, our findings suggest that the descending pain modulation system may be involved in the modulation effect produced by taVNS.
We also found that taVNS could significantly decrease the connectivity between the ‘occipital’ thalamic seed and the bilateral PoG as well as the right PCu after taVNS treatment. Specifically, the decreased functional connectivity between the ‘occipital’ thalamic seed and the bilateral PoG is significantly associated with the reduction of migraine days.
The anatomical profile of the functionally parceled ‘occipital’ thalamic subregions located in an area around the medial and posterior group of thalamic nuclei. In particular, pulvinar nucleus from the posterior group of the thalamus has a strong connection with the visual cortex and is recognized as a prototypic association nucleus involved in reciprocal cortico–cortical interactions.48 A neural anatomy study showed that the pulvinar nuclei in this region send projections to V1, V2, auditory and somatosensory cortices, and that these projections are implicated in the clinical features of migraines.49 In a previous study, we found abnormal posterior thalamic (pulvinar nuclei) dynamic functional network connectivity with the visual cortex and PCu in migraine patients.50 In a more recent study, we found that the occipital cortex may play an important role in the pathophysiology of migraines.51 We speculate that this may indicate that taVNS can modulate the interaction among key sensory regions, including the somatosensory cortex and the visual cortex through the thalamus.
There are several limitations in this study. First, the sample size is relatively small, so a randomized and sham-controlled clinical trial/study with a large sample size is needed to validate our findings of taVNS. Second, this is a single-blinded study. The physicians who administered the taVNS were not blinded to the treatment modality. Thus, there may be some potential bias. Nevertheless, the patients and staff members involved in clinical and imaging data collection were blinded to the randomization. In addition, we are not able to report the magnitude to which the blinding is maintained during the study course as we did not perform a blinding assessment.52 A further study with a double-blinded design and a blindness assessment is needed to further validate our findings. Third, three multicenter, double-blinded, randomized, sham-controlled studies using non-invasive vagus nerve stimulation at the neck included migraine patients with or without aura.9 10 14 One reported a greater therapeutic gain in migraine patients with aura than those without aura.10 In the current study, we only recruited migraine patients without aura. It remains an interesting topic to investigate/compare the effects of taVNS in migraine patients with and without aura. Future studies regarding this topic are needed.
Conclusion
In summary, in this single-blinded placebo controlled clinical study, we investigated the modulation effect of taVNS and its underlying mechanism. We found that real taVNS can significantly improve clinical outcomes compared with sham taVNS after 4 weeks of treatment. Using functionally parceled methods, we found that taVNS can increase the connectivity between the motor-related thalamic subregion and rACC/mPFC, and decrease the connectivity between the ‘occipital’ thalamic subregion and brain regions associated with pain sensitivity (postcentral gyrus/PCu). Furthermore, the rsFC change between the occipital related thalamic subregion and the bilateral postcentral gyrus was significantly correlated with the reduction of migraine days in the real taVNS treatment group. The current study may further our understanding of migraine pathophysiology and identify potential new targets for intervention in the form of electrical stimulation for migraine patients.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
YZ and YH contributed equally.
Contributors Design and conceptualized study: YZ, BL and JK; Analyze and interpret the data: YH, JK and YT; Acquisition of data: YZ, HL, ZY, YZ, XL, XYH and WC; Manuscript preparation: YH, SH, HC and JK; Funding acquisition: YZ and BL.
Funding This study was supported by the Medical Scientific Research Foundation of Guangdong Province of China (A2017234) and the Administration of Traditional Chinese Medicine of Guangdong Province of China (20182047).
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval This study protocol was approved by the Institutional Review Board of the Second Affiliated Hospital of Guangzhou University of Chinese Medicine.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. Data are available on reasonable request, contact email: liubogzcm@163.com