Article Text

Abstract
Background Smoking adversely impacts pain-related outcomes of spinal cord stimulation (SCS). However, the proportion of SCS patients at risk of worse outcomes is limited by an incomplete knowledge of smoking prevalence in this population. Thus, the primary aim of this systematic review is to determine the prevalence of smoking in adults with chronic pain treated with SCS.
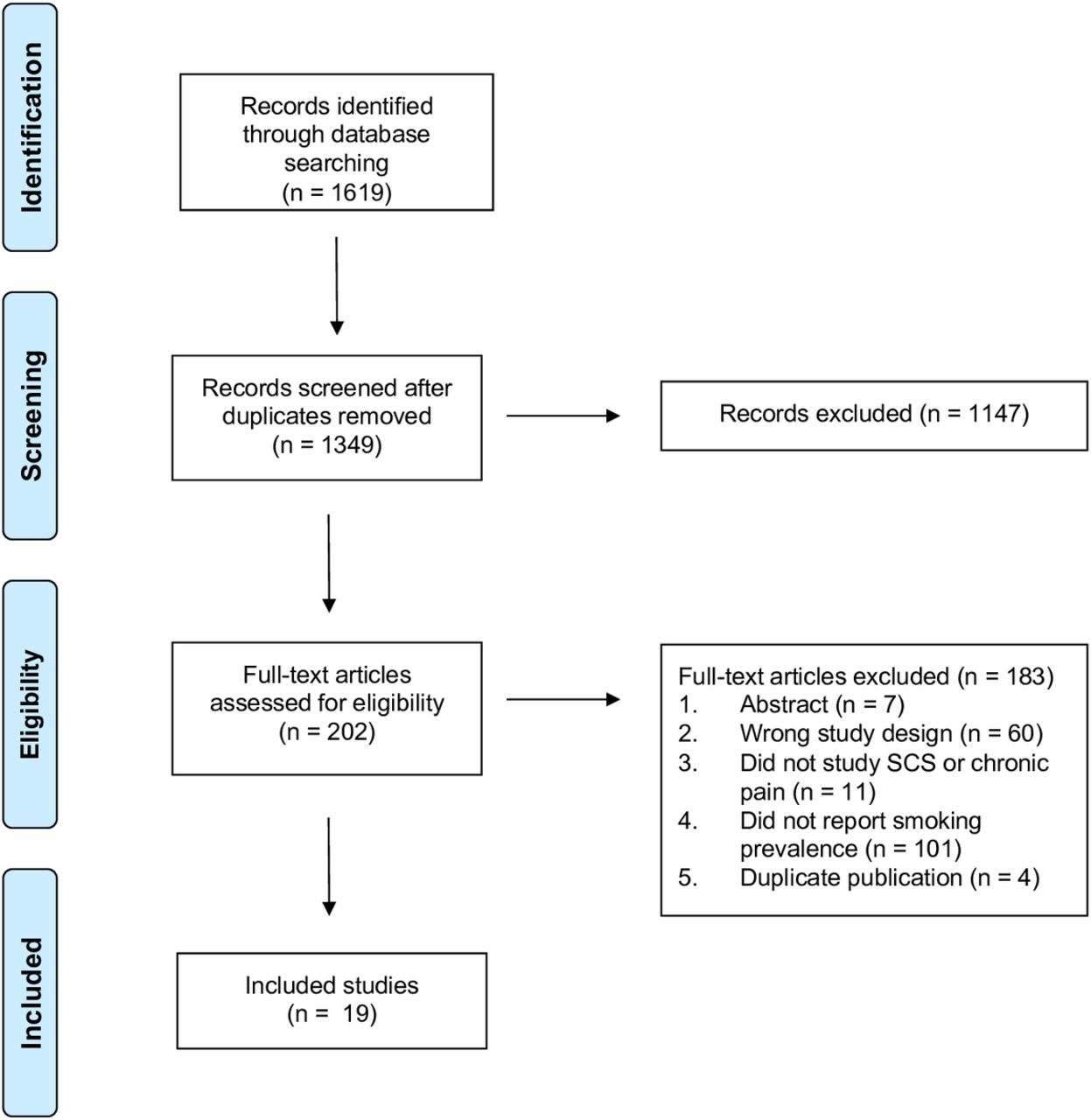
Methods A comprehensive search of databases from 1 January 1980 to 3 January 2019 was conducted. Eligible study designs included (1) randomized trials; (2) prospective and retrospective cohort studies; and (3) cross-sectional studies. The risk of bias was assessed using a tool specifically developed for prevalence studies. A total of 1619 records were screened, 19 studies met inclusion criteria, and the total number of participants was 10 838.
Results Thirteen studies had low or moderate risk of bias, and six had a high risk of bias. All 19 studies reported smoking status and the pooled prevalence was 38% (95% CI 30% to 47%). The pooled prevalence in 6 studies of peripheral vascular diseases was 56% (95% CI 42% to 69%), the pooled prevalence of smoking in 11 studies of lumbar spine diagnoses was 28% (95% CI 20% to 36%) and the pooled prevalence in 2 studies of refractory angina was 44% (95% CI 31% to 58%).
Conclusions The estimated prevalence of smoking in SCS patients is 2.5 times greater than the general population. Future research should focus on development, testing and deployment of tailored smoking cessation treatments for SCS patients.
- chronic pain: back pain
- neuromodulation: spinal cord stimulation
- pain medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Over the past 25 years, technological and surgical advances have revolutionized the use of spinal cord stimulation (SCS) for a broad range of chronic pain conditions1; however, not all patients experience optimal long-term benefits. One recently identified subgroup that may be at risk of poor outcomes are smokers treated with SCS. In a retrospective study that involved 213 patients with chronic spine-related pain treated with SCS, smokers reported greater pain intensity and consumed greater quantities of opioids compared with nonsmokers at 1 year following SCS implant.2 More specifically, the pain scores of smokers were 37% greater compared with never smokers, and the median morphine equivalent dose of smokers was 40 mg compared with 23 mg in never smokers.2 3 This is critically important because SCS is one of the few treatments associated with sustained and durable pain relief, and low risk of adverse effects.1
The proportion of SCS patients impacted by the adverse influence of smoking is limited, in part, by an incomplete knowledge of smoking prevalence in adults with SCS. Thus, the primary aim of this systematic review is to determine the prevalence of smoking in adults with chronic pain treated with SCS. A secondary aim includes determining the prevalence of smoking in adults with chronic pain based on the indication for SCS including lumbar spine diagnoses, ischemic pain related to peripheral vascular diseases and refractory angina.
Methods
Study protocol
Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines4 were followed. An a priori protocol was followed. The trial was registered in the PROSPERO database (CRD42018117004).5
Search strategy
A comprehensive search of databases from 1 January 1980 to 3 January 2019 was conducted. The databases included MEDLINE Epub Ahead of Print, Medline In-Process and Other Non-Indexed Citations, MEDLINE, EMBASE and Scopus. The search strategy was designed and conducted by a medical reference librarian with input from the principal investigator. No language restrictions were employed. Controlled vocabulary supplemented with keywords was used to search for studies on the prevalence of smoking in patients with SCSs. The search strategy is provided in online supplementary appendix A.
Supplemental material
Study selection process
Study inclusion criteria included (1) randomized, cross-over and parallel-designed clinical trials; (2) prospective and retrospective cohort studies; (3) cross-sectional design; (4) age 18 years or older; (5) publication years 1980 to present; (6) any publication language; (7) studies of patients with SCSs and (8) study results that included data on smoking prevalence. Exclusion criteria included (1) studies that involved patients without chronic pain and (2) studies of adults with acute or subacute pain.
In the first phase, two independent pairs of reviewers screened all titles and abstracts identified by our search strategy. In the second phase, the two pairs of independent reviewers screened the bibliography of each full-text article to identify additional relevant citations for inclusion. In the third phase, all full-text articles were screened for inclusion and exclusion criteria and the reason for exclusion of each full text was noted.
Data extraction
Data were extracted by four independent reviewers using a templated electronic database.
Based on the a priori protocol, abstracted data included study design, number of subjects, indication for SCS placement, demographics (mean age, percent female sex) and prevalence of smoking. Smoking status was categorized as current smoker, non-smoker or former smoker. In individual studies, participants described as ‘smokers’, ‘history of smoking’ and ‘tobacco use’ were considered to be current smokers. At least two attempts were made to contact investigators for incompletely reported outcomes.
Risk of bias assessment
The risk of bias in the included studies was assessed by two independent reviewers using a tool specifically developed to assess risk in prevalence studies.6 A summary risk of bias was reported for each manuscript included in the study. Reviewer discrepancy was resolved by consensus or by a third reviewer.
Evidence synthesis
For each trial, the prevalence and SE were recorded. If the SE was not reported, it was calculated from the prevalence data. A random-effects model was used and results were reported with 95% CIs. Statistical analyses were performed using Stata V.15 (StataCorp. 2017. Stata Statistical Software: Release 15).
Results
Characteristics of included studies
A flow diagram of the study selection process is depicted in figure 1. A total of 19 studies met inclusion criteria (online supplementary file 1).2 7–24 All 19 studies reported current smoking and 2 studies2 21 reported former smoking. Three studies were randomized controlled trials (RCTs),13 21 24 six studies were prospective cohort studies,7–9 11 15 16 nine studies were retrospective cohort studies2 10 12 14 17–20 23 and one study was a cross-sectional study.22 Demographic and smoking information were available for 10 838 SCS patients. The general indication for SCS placement in 11 studies was lumbar spine diagnoses including chronic low back pain, radiculopathy, failed back surgery syndrome, degenerative disc disease and spinal stenosis.2 8–11 14 17 19 20 22 23 The indication for SCS placement in six studies was peripheral vascular diseases and, in all studies, pain was an inclusion criterion or a key outcome measure.7 12 16 18 21 24 The indication for SCS in two studies was refractory angina.13 15
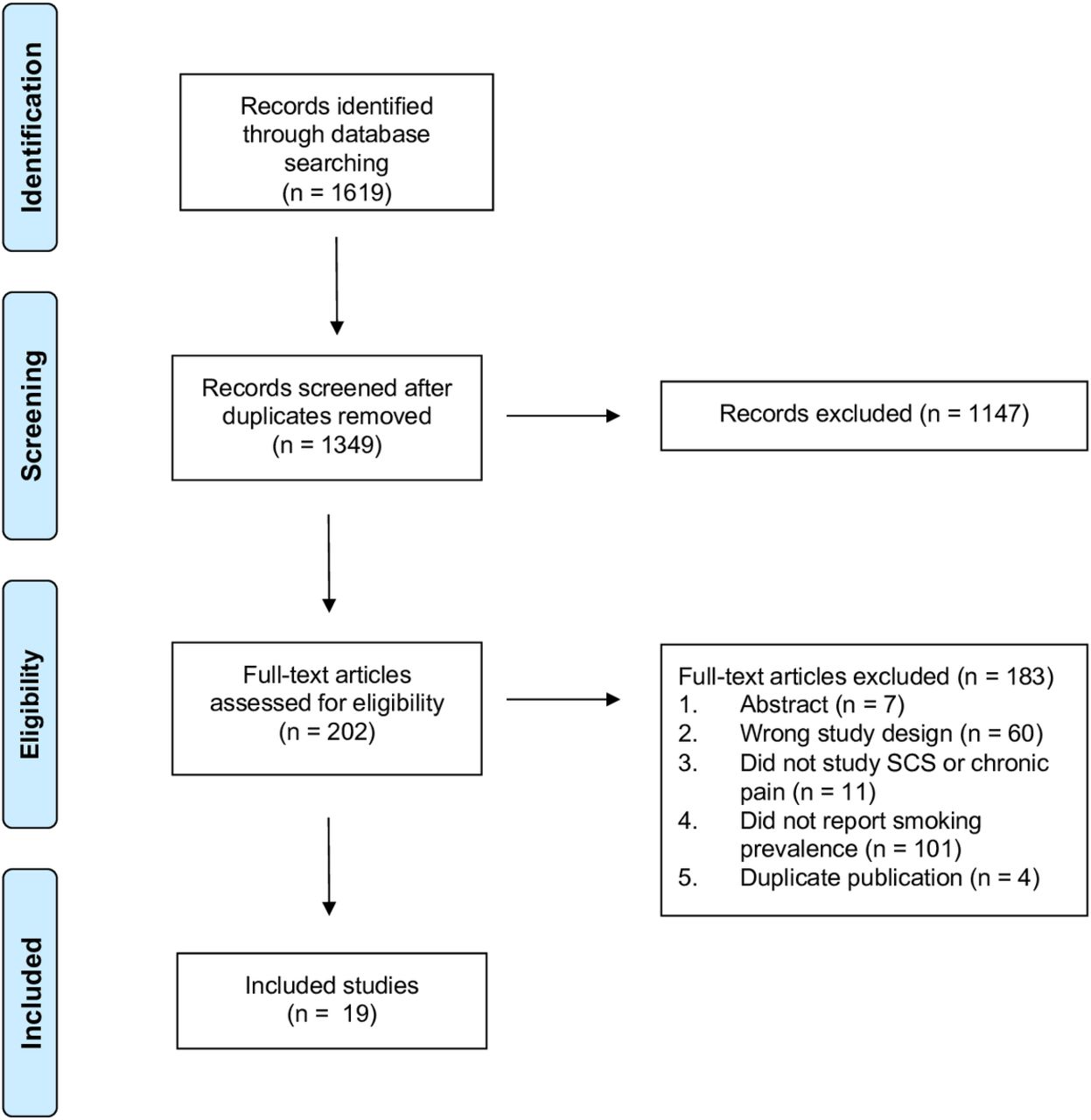
Preferred Reporting items for Systematic Reviews and Meta-Analyses flow chart of the study selection process.3
Risk of bias and level of certainty
The summary results of the risk of bias evaluation are listed in online supplementary file. Thirteen studies were found to have a low or moderate risk of bias2 8–12 14 17–21 24 and six were found to have a high risk of bias.7 13 15 16 22 23 The majority of differences in the risk of bias centered around the first two questions: (1) Is the study population a close representation of the national population? and (2) Is the sampling frame a true or close representation of the target population?
Prevalence of smoking based on study design
All 19 studies (n=10 838 patients) reported current smoking and the prevalence ranged from 14% to 90% (figure 2). The pooled prevalence of smoking in these studies was 38% (95% CI 30% to 47%) with high heterogeneity (I2=97.6%). When one large study that used administrative claims data was excluded from the meta-analysis,14 the pooled prevalence increased to 41% (95% CI 33% to 48%).
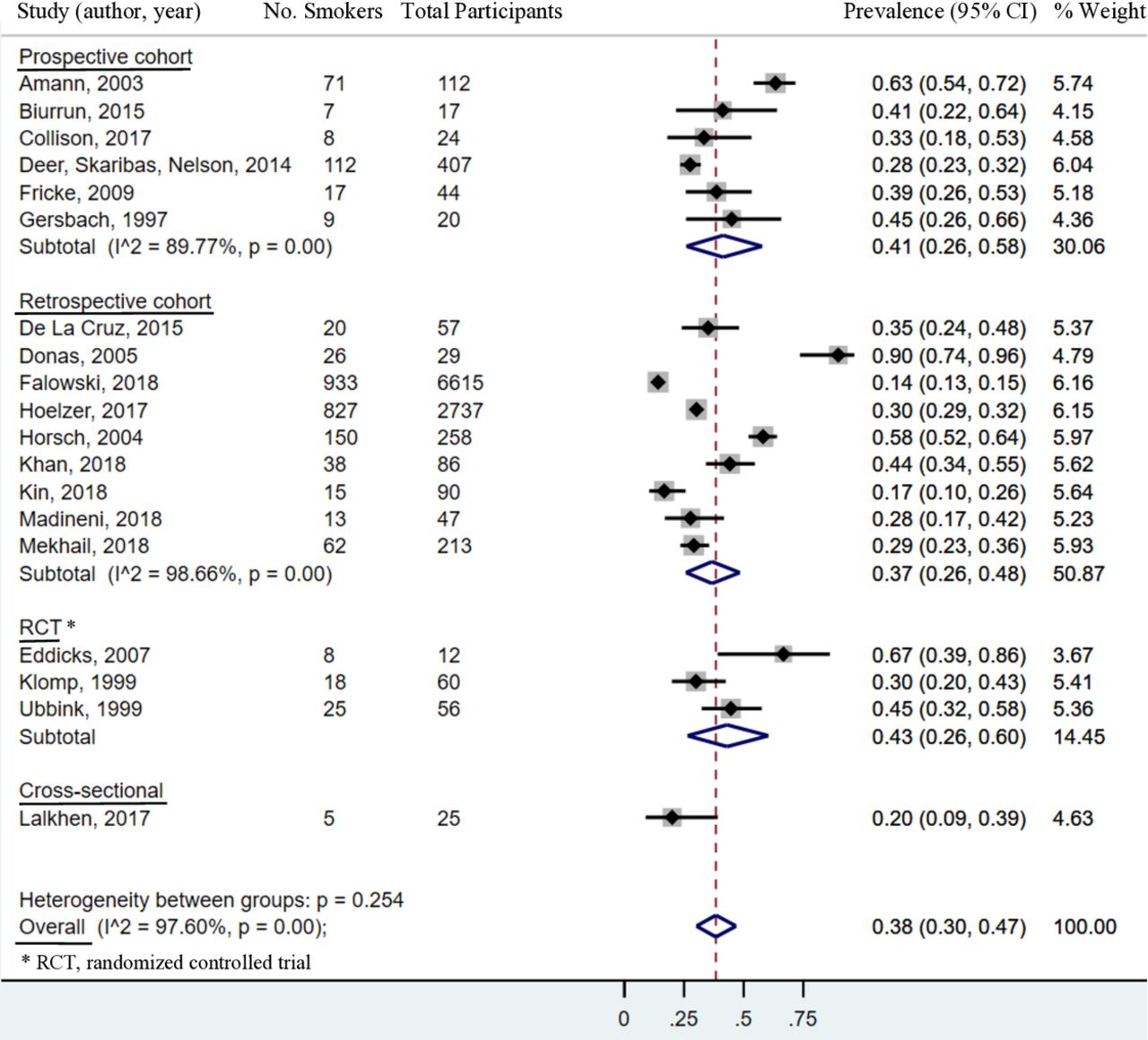
Prevalence of smoking in adults treated with spinal cord stimulation based on study design.
The prevalence of smoking in six prospective cohort studies ranged from 28% to 63% (figure 2). The pooled prevalence of smoking in these studies was 41% (95% CI 26% to 58%) with high heterogeneity (I2=89.8%).
The prevalence of smoking in nine retrospective studies ranged from 14% to 90% (figure 2). The pooled prevalence in these studies was 37% (95% CI 26% to 48%) with high heterogeneity (I2=98.7%).
The prevalence of smoking in three RCTs ranged from 30% to 67% (figure 2). The pooled prevalence of smoking in these studies was 43% (95% CI 26% to 60%). In meta-analyses with three or fewer studies, the I2 estimation becomes unreliable; thus, it was not calculated.
In a single cross-sectional study, the prevalence of smoking was 20% (figure 2).
Prevalence of smoking based on indication for SCS
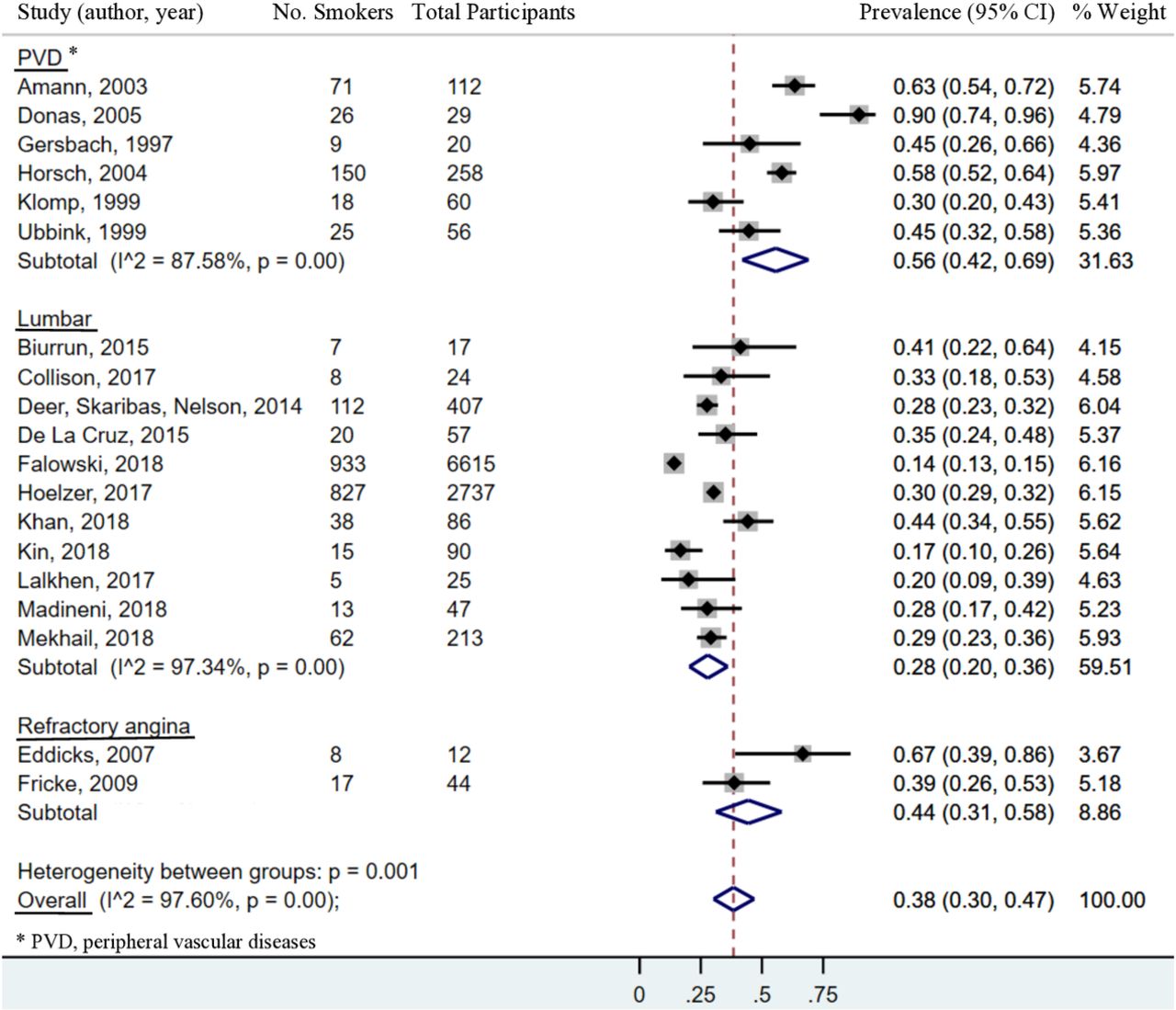
The indication for SCS placement was categorized into three groups including (1) lumbar spine diagnoses (n=11 studies); (2) peripheral vascular diseases (n=6 studies) and (3) refractory angina (n=2 studies).
The prevalence of smoking in six studies of patients with peripheral vascular diseases ranged from 30% to 90% (figure 3). The pooled prevalence of smoking in these studies was 56% (95% CI 42% to 69%) with high heterogeneity (I2=87.6%).
{kind=link}
{kind=link}
{kind=link}
Prevalence of smoking based on the indication for spinal cord stimulation.
The prevalence of smoking in 11 studies of patients with lumbar spine diagnoses ranged from 14% to 44% (figure 3). The pooled prevalence of smoking in these studies was 28% (95% CI 20% to 36%) with high heterogeneity (I2=97.3%).
The prevalence of smoking in two studies of patients with refractory angina ranged from 39% to 67% (figure 3). The pooled prevalence of current smoking in these studies was 44% (95% CI 31% to 58%). In meta-analyses with three or fewer studies, the I2 estimation becomes unreliable; thus, it was not calculated.
Discussion
The main finding of this systematic review and meta-analysis was that the pooled prevalence of smoking in adults with chronic pain treated with SCS was 38%. When the meta-analysis was restricted to prospective studies, the prevalence increased to 41%. The greatest prevalence was observed among adults with peripheral vascular diseases (56%) and refractory angina (44%) compared with individuals with lumbar spine diagnoses (28%).
The estimated prevalence of smoking in the general population has declined over the past 20 years to approximately 15%.25 However, the prevalence of smoking among individuals with chronic pain remains greater than the general population.26–30 More specifically, in a retrospective study that involved 5350 adults with chronic pain admitted to an outpatient functional restoration programme from 1998 to 2012, the prevalence of smoking during the 15-year study period was 23.5%.30 In this previous study, the overall prevalence of smoking in patients with commonly occurring pain conditions including fibromyalgia, low back pain and headache was 25.2%, 22.8% and 21.2%, respectively.30 In comparison, the observations from this meta-analysis suggest that the prevalence of smoking in adults treated with SCS is approximately 1.6 times greater than non-SCS treated adults with chronic pain and 2.5 times greater than the general population.
The high prevalence of smoking in adults with chronic pain could be due, in part, to clinical factors unique to this patient population. Adult smokers with chronic pain report greater pain intensity,31 32 which is partly mediated by greater levels of depression33 and positively associated with the desire to smoke.34 Smokers with chronic pain also experience greater levels of functional impairment35 and negative affect,36 37 are more likely to use opioids,38 39 and report that smoking is an important coping strategy for pain and distress.40 41 These characteristics could have contributed to the observations reported by Mekhail et al2 where smokers treated with SCS reported greater pain scores and consumed greater quantities of opioids compared with nonsmokers.
The results of this study highlight that smoking is a substantial problem in SCS patients which suggests barriers to smoking cessation exist in this population of patients. Although studies suggest that many smokers with chronic pain are willing to consider cessation, it may be difficult for them to quit for several reasons.35 42 Acute nicotine deprivation for 12–24 hours is associated with increased pain intensity and alterations in pain perception.43 44 In addition, greater levels of pain-related anxiety are associated with early relapse,45 which is particularly important because smokers with chronic pain are less likely to tolerate adverse psychological states.41 Thus, smokers with chronic pain, including those treated with SCS, may require tailored interventions that address smoking cessation in the context of chronic pain.42 46
This study has limitations including high levels of observed heterogeneity. Although 13 of 19 studies were assessed as being at low to moderate risk of bias, the majority of differences in the risk of bias were related to selection bias in that the study cohorts were not representative of the targeted population. This sources of heterogeneity could have influenced the reported prevalence of smoking. Other potential sources of heterogeneity include variations in how smoking status was assessed in the different study designs. For example, the pooled prevalence of smoking in the retrospective studies was 37% compared with 41% in the prospective cohort studies and 43% in the RCTs. The lower prevalence in the retrospective studies, including the study that used administrative claims data,14 could be due to inaccurate or incomplete assessment of smoking status compared with the assessment of smoking in the prospective cohort and RCT designed studies.
In summary, the estimated prevalence of smoking in adults treated with SCS is 2.5 times greater than the general population and 1.6 times greater than non-SCS treated adults with chronic pain. These findings also support the assertion that smoking status should be assessed in future neuromodulation trials. The long-term goal of this area of research is to develop, test, deploy and disseminate effective smoking cessation treatments for adults treated with SCS. It is anticipated that the outcomes of future studies will demonstrate the need for preimplant and postimplant smoking cessation interventions in order to effectively mitigate the deleterious effects of smoking on SCS outcomes.
Supplemental material
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at The study findings have not been previously presented at a scientific meeting.
Contributors WMH took part in design of this project, interpretation of data and writing the manuscript. RNM took part in design of this project, acquisition of data, analysis and interpretation of data, and writing the manuscript. JD, EMP and RW took part in acquisition of data. MHM took part in conception and design of this project, and analysis and interpretation of data.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplementary information.