Article Text

Abstract
Background Spinal cord stimulation (SCS) has emerged as an important treatment for chronic pain disorders. While there is evidence supporting improvement in pain intensity with SCS therapy, efforts to synthesize the evidence on physical functioning are lacking.
Objective The primary objective of this meta-analysis was to assess long-term physical function following 12 months of SCS for chronic back pain.
Evidence review PubMed, EMBASE, Scopus, and CENTRAL databases were searched for original peer-reviewed publications investigating physical function following SCS. The primary outcome was physical function at 12 months following SCS therapy for chronic back pain compared with baseline. A random effects model with an inverse variable method was used. The Grading of Recommendation, Assessment, Development, and Evaluation (GRADE) framework was used to determine the certainty of evidence.
Findings A total of 518 studies were screened, of which 36 were included. Twenty-two studies were pooled in the meta-analysis. There was a significant reduction in Oswestry Disability Index (ODI) scores at all time frames up to 24 months following implantation. Pooled results revealed significant improvement in ODI scores at 12 months with a mean difference of −17.00% (95% CI −23.07 to −10.94, p<0.001). There was a very low certainty of evidence in this finding as per the GRADE framework. There was no significant difference in subgroup analyses based on study design (randomised controlled trials (RCTs) vs non-RCTs), study funding, or stimulation type.
Conclusion This meta-analysis highlights significant improvements in physical function after SCS therapy. However, this finding was limited by a very low GRADE certainty of evidence and high heterogeneity.
- Spinal Cord Stimulation
- Back Pain
- Outcome Assessment, Health Care
- Pain Management
Statistics from Altmetric.com
Introduction
Chronic low back pain is recognized as the leading cause of disability worldwide. Disability and poor physical functioning can negatively impact all aspects of life ranging from work-related disability to loss of ability to perform activities of daily living.1–3 The management of chronic low back pain has been extensively studied and a multifaceted approach including physical therapy, psychological therapy, pharmacological therapy, interventional pain procedures or surgeries is critical.4–8 Despite advancements in treatment, low back pain continues to be the leading global cause of years lost to disability and future investigation to mitigate this increasing burden is a priority in chronic pain research.9
Spinal cord stimulation (SCS) has emerged as an important treatment for chronic pain disorders and is currently approved by the Food and Drug Administration for the treatment of refractory chronic pain disorders including failed back surgery syndrome (FBSS), complex regional pain syndrome, painful diabetic neuropathy (PDN), and non-surgical refractory back pain.10–17 Although the mechanism behind SCS is not completely elucidated, a common referenced theory is the gate control theory of pain. Through stimulating A-β neuron fibers, it is proposed that the pain impulses carried by A-δ fibers and smaller C-fibers can be attenuated and intercepted from transmission via ascending spinal and supraspinal tracts.18 In addition to improving pain outcomes, quality of life (QoL), and patient satisfaction, several randomized controlled trials (RCTs) and systematic reviews have reported an association between SCS therapy and improvement in physical functioning outcomes in patients with FBSS and chronic axial low back pain without previous spine surgery.16 19–21 However, other studies have reported no change in measures of physical function after SCS therapy compared with placebo or spine reoperation.22 Evidence review and appraisal are currently lacking in the literature on change in physical function after SCS therapy.23
The primary objective of this systematic review and meta-analysis was to assess the long-term physical function and disability outcomes following neuromodulation with SCS for patients with chronic back pain.
Materials and methods
The study protocol was registered and approved with the International Prospective Register of Systematic Reviews (PROSPERO ID: CRD42022337076).24 Studies were sought that evaluated functional outcomes after SCS therapy using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.25
Search strategy
A systematic search strategy was created for several databases, from database inception to May 31, 2022. The databases included Ovid Medical Literature Analysis and Retrieval System Online (MEDLINE) and Epub Ahead of Print, In-Process & Other Non-Indexed Citations, and Daily, Ovid Excerpta Medica Database (EMBASE), Ovid Cochrane Central Register of Controlled Trials, and Scopus. The search strategy was designed and conducted by an experienced librarian with input from the study’s principal investigator (RSD’S). Controlled vocabulary supplemented with keywords were used to search for studies describing the change in disability and physical functioning outcomes after SCS for patients with chronic pain. The complete search strategy is available in online supplemental file S1.
Supplemental material
Study selection criteria
Peer-reviewed original research publications were considered for inclusion based on the following PICOT criteria: Patient population (P): Adult patients with chronic pain indications including non-surgical or postsurgical back pain. Intervention (I): Dorsal column SCS implants. Studies with only SCS trials and dorsal root ganglion stimulation were excluded. Control/Comparator (C): Physical function measures at baseline prior to SCS implantation. Outcome (O): Physical function outcomes as measured by any of the following physical function assessment questionnaires: Oswestry Disability Index (ODI), Roland-Morris disability questionnaire (RMDQ), or the physical component scale of the Short Form-36 Survey (SF-36). Time (T): Although we did not restrict study eligibility criteria based on follow-up time, the time point of the primary outcome was 12 months after SCS implantation.
Studies were not restricted to a specific waveform paradigm, type of lead (paddle lead, cylindrical lead), or type of pulse generator (external or internal). To facilitate a comprehensive capture of studies, we did not mandate physical function to be a primary outcome from studies.
Outcomes assessed
The primary outcome of this systematic review was change in physical function from baseline to 12 months after SCS implantation. The 12-month time point was chosen a priori as the primary time point based on clinical and research experience from the author team where it was deemed as sufficient time for the primary outcome to manifest. Improvements in pain intensity occur first and after achieving adequate analgesia, patients can increase mobility, exercise, and participate in physical therapy. Secondary outcomes included change in physical function metrics at 1, 3, 6, 18, and 24 months.
Physical function outcomes
Developed by Fairbank et al with multiple versions since, the Oswestry low back pain disability questionnaire has become a commonly used tool for assessing physical function in patients with back pain.26–28 Higher ODI scores indicate increasing disability. Studies predict the ODI’s Minimum clinically important difference (MCID) to be an improvement of 10% or 12.8%.29 30 The SF-36 survey is another validated tool exploring eight domains of health including physical functioning.31 32 The RMDQ is another modality to assess physical disability due to low back pain.28 33 Online supplemental table S2 expands on questionnaires exploring physical function.
Study selection
Two authors (DJK and ME) independently screened the results generated by the search strategy by title and abstract alone. Following this, potentially eligible citations had their full-text version retrieved for assessment of inclusion. Any discrepancies were resolved by a third investigator (RSD’S).
Data extraction
Two groups of paired authors: DJK and ME, and GAMA and EK independently performed data extraction. The following information was extracted and stored on Excel: (1) study characteristics (study design, interventions, funding, country(s), intervention, study subgroups, waveform information, and follow-up duration), (2) participant demographics (sample size, mean age), and (3) outcomes of interest (ODI, RMDQ, SF-36 scores at baseline and at 1, 3, 6, 12, 18 and, 24 months).
Assessment of risk of bias
The quality of the included studies was independently assessed by two authors using the Cochrane Collaboration guidelines.34 Disagreements were adjudicated by a third author (RSD’S). The RCT studies were assessed for bias with the Risk of Bias 2 tool.35 Each of the five domains were graded based on the risk of bias as either: low risk, high risk or some concerns of bias. For cross-over trials, an additional domain (DS) was assessed to look for bias arising from period and carryover effects. For observational studies including cohort and case control studies, the Newcastle-Ottawa scale (NOS) was used.36 The NOS scale was implemented by using this star grading system to appraise the studies across three categories of (1) study group selection, (2) comparability of the groups, and (3) ascertainment of exposure or outcome. Ratings are between 0–9 with studies rated between 0–2, 3–5, 6–9 are classified as having poor, fair, high quality, respectively.36
The GRADEpro software (Evidence Prime) was used by two reviewers (ME and EK) to independently assess the evidence for each outcome across the included studies using the GRADE (Grading of Recommendations, Assessment, Development and Evaluations) quality assessment criteria.37
Statistical analysis
The analysis was conducted with Review Manager software (RevMan) V.5.4.1. Quantitative variables (eg, ODI and SF-36 scores) were extracted and reported as mean and SDs. For studies reporting median and IQRs, the Cochrane Collaboration Guidelines were used to obtain SD from SE or CI, to approximate the median to be equal the mean, and SD was calculated by dividing the IQR by 1.35.38 39 Statistical pooling was performed for those outcomes with more than three studies reporting data. Qualitative reporting summarized outcomes not statistically pooled. An inverse variable statistical method was utilized with a random effects model to generate a pooled effect estimate and the 95% CIs. Statistical heterogeneity between studies was assessed using the I2 statistic with a designation of >50% signifying high heterogeneity. A p<0.05 was set as the level of significance. Publication bias was assessed with funnel plot asymmetry and the Egger’s test. A sensitivity analysis was conducted with the leave-one-out method to assess the robustness of the data.
Subgroup analysis
In the presence of high heterogeneity in the primary outcome, subgroup analysis was performed for those covariates that had three or more studies. For the subgroup analysis based on funding, studies receiving industry-supported funding were classified as industry-funded studies; studies receiving funding from a non-industry source were classified as funded (non-industry); studies receiving no funding or those where no funding statement was reported were classified as non-funded studies. We also performed two post-hoc subgroup analyses stratifying the studies based on study design (RCTs vs observational studies) and stimulation type (paresthesia-based vs non-paresthesia-based stimulation).
Results
Study characteristics
Figure 1 depicts the PRISMA flow chart of the study selection and inclusion process. A total of 36 studies met the inclusion criteria and were included for the qualitative analysis.22 40–74 Table 1 describes the characteristics of the included studies. There were 7 included RCTs,22 40 50 55 61 63 69 17 prospective studies,41–44 46 47 51 56 59 60 62 64 65 68 70–72 11 retrospective studies,45 48 49 52–54 57 58 66 67 73 and 1 ambispective observational study.74 Thirteen studies were conducted in multiple centers.41–43 46 51 55 56 61 63 68 69 72–74 Eight studies were conducted in multiple countries.41 43 52 55 56 63 69 72 Most studies (22/36) were funded by industry.40 41 43 44 46 47 49 51 53 55 56 58 59 61 63 64 68 69 71–74 Seven studies had participants undergoing high-frequency SCS,41 44 50 53 59 61 72 four studies with high-density SCS,43 51 56 64 and two studies with burst SCS.22 40 The duration of follow-up for physical function outcomes varied from 1 month to 5 years. Twenty-two articles were included in the quantitative analysis and were meta-analyzed.22 40–42 44–48 50 51 55–57 60 63 65–67 69 73 74 Five studies40 48 50 67 73 had multiple study arms where the groups were analyzed and presented separately in the forest plot. Specific details of each arm from these studies are presented in online supplemental table S4. Of included studies, the range of mean scores on physical outcome measures at baseline were as follows: SF-36: minimum of 24.08 (6.73)69 to a maximum of 36.67 (21.17).73 RMDQ: 13.9 (4.5)53 to 16.9 (3.5).71 ODI: 24.32 (7.4)45 to 85 (8.9).57
Included study characteristics
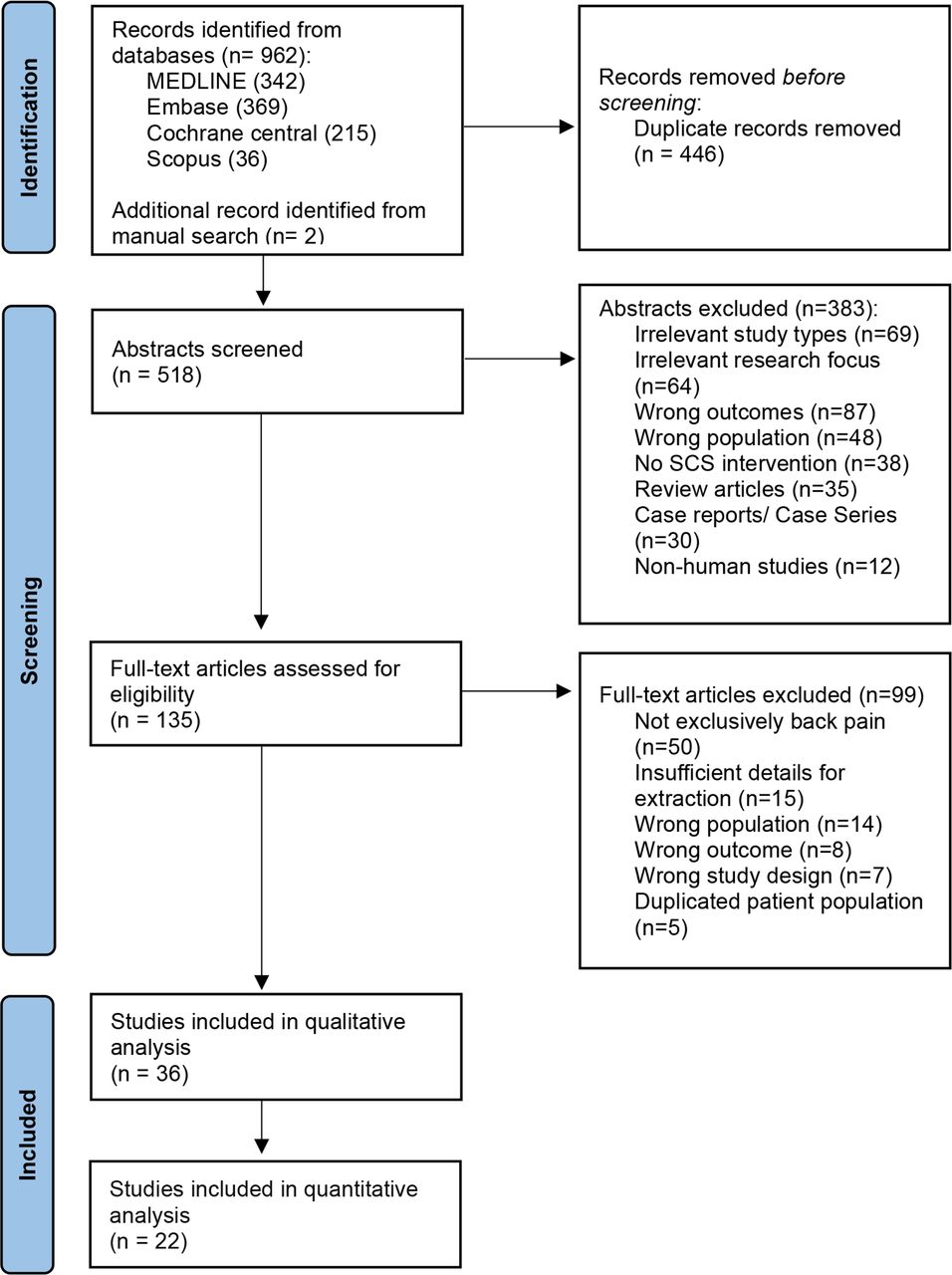
PRISMA diagram. Flow chart for study selection process including identification of studies from multiple databases and sources, screening process, assessment of eligibility and final study inclusion. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Quality assessment
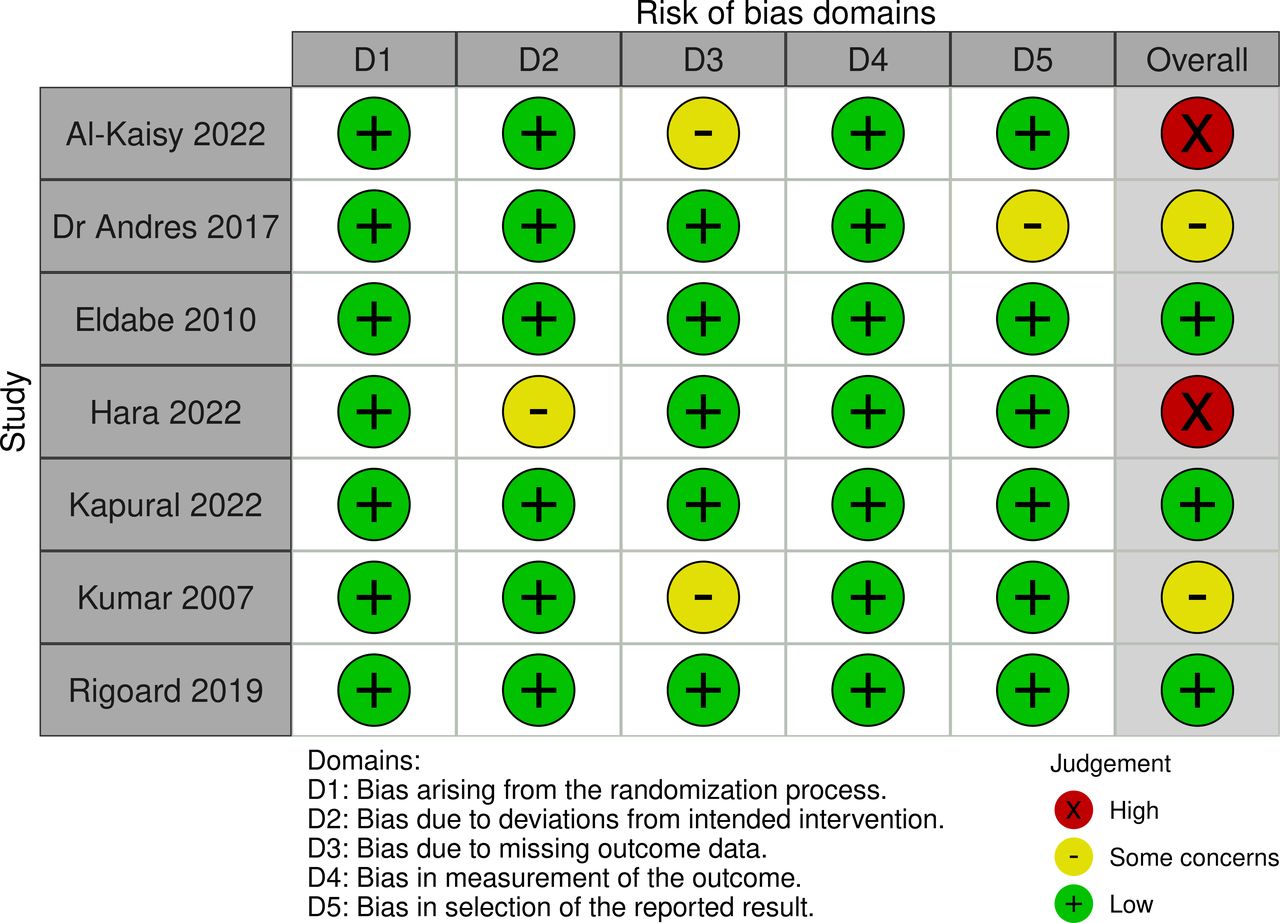
The methodological quality of the included studies are summarized in figure 2 and online supplemental table S3. Overall, three RCTs had low risk of bias and two with some concerns of bias. The two RCTs22 40 with cross-over design had high concern of bias. Both had high bias in Domain S (DS) due to the risk of bias from period and carryover effects. Additionally, Al-Kaisy et al 40 had concerns in domain 3 due to loss of follow-up, while Hara et al 22 had concerns in domain 2 owing to deficiencies in the use of an appropriate analysis plan. Based on NOS, most of the observational studies fell in the category of fair quality, particularly owing to the lack of comparability description, lack of control groups and confounders adjustments. The GRADE assessment is displayed in tables 2 and 3. Most of the included studies were observational in design and only seven were RCTs, thus downgrading the quality of evidence. The ODI score at 12 months had an overall certainty of ‘very low’ due to the presence of risk of bias, and inconsistency. Egger’s test revealed a p value of 0.076. However, based on visual assessment of the Funnel plot (online supplemental figure S5), there may be presence of small-study effects. Sensitivity analysis with the leave-one-out method found no significant changes in effect sizes.

Risk of Bias assessment for included RCT studies. Green circle indicates a ‘low risk of bias’, red circle indicates a ‘high risk of bias’, yellow circle indicates ‘some concerns of bias’. Al-Kaisy et al40 and Hara et al22 were RCTs with cross-over design and were assessed for an additional domain (DS: Risk of bias arising from period and carryover effects) which was judged as high bias. RCT, randomised controlled trial.
GRADE Evidence profile: physical functioning outcomes as per Oswestry Disability Index (ODI) for patients with chronic pain following spinal cord stimulation
Summary of findings table: physical functioning outcomes as per Oswestry Disability Index (ODI) for patients with chronic pain following spinal cord stimulation
Primary outcome
Ten studies40 42 45 46 48 50 56 57 73 74 with 852 patients (at baseline) reported ODI scores at 12 months. Pooled results revealed that ODI scores improved significantly from baseline to 12 months with a mean difference of −17.00% (95% CI −23.07 to −10.94, p<0.001; 852 patients in 10 studies40 42 45 46 48 50 56 57 73 74, figure 3). This finding had high statistical heterogeneity (χ 2=294.04, df=13 (p<0.001), I2=96%). The decrease in ODI scores ranged from a minimum decrease of 4% (95% CI–7.37 to −0.63) to a maximum decrease of 69% (95% CI −78.09 to −59.91). Only one study73 reported on mean SF-36 score at 12 months with after a baseline (36.67±21.17) compared with follow-up of (52.14±26.30; p<0.001). Online supplemental table S6 shows a qualitative summary of study outcomes.

{kind=link}
{kind=link}
{kind=link}
Forest plot of (Oswestry Disability Index) ODI scores before and after (spinal cord stimulator) SCS implantation at 12 months follow-up. Mean difference scores after 12 months of follow-up after SCS implantation are presented. An inverse variable statistical method was used with a random effects model to generate a pooled effect estimate and the 95% CI. The diamond represents the pooled estimated effect size, and the width of the diamond reflects the 95% CI of this estimate. Al-Kaisy 2022 Group 1: Anatomic placement group. Al-Kaisy 2022 Group 2: Paresthesia mapping group. Campwala 2021 Group 1: SCS for patients with no previous spine surgery. Campwala 2021 Group 2: SCS with history of previous spine surgery. De Andres 2017 Group 1: Conventional frequency SCS. De Andres 2017 Group 2: High Frequency SCS. Van Heteren 2022 Group 1: SCS. Van Heteren 2022 Group 2: SCS+PNFS. PNFS, peripheral nerve field stimulation.
Secondary outcomes
Compared with baseline, pooled analysis revealed a mean difference of −19.90 (–28.24,–11.57), p<0.0001; 534 patients in eight studies22 40 46 47 50 51 56 60 in ODI scores at 3 months; −11.20% (95% CI −14.85% to −7.55%, p<0.0001); 490 patients in 9 studies40 42 50 63 65–67 69 74 at 6 months; and −17.11% (95% CI −20.88% to −13.34%, p<0.0001); 202 patients in 3 studies41 46 74 at 24 months. Additionally, pooled analysis revealed a mean difference of 10.06 (95% CI 5.91 to 14.22, p<0.0001); 289 patients in 4 studies55 63 69 73 for the SF-36 scores at 6 months. All secondary outcomes are presented in online supplemental figures S7–S10.
Subgroup analysis
Subgroup analysis based on study design (RCT vs observational studies) revealed no statistically significant difference (χ2=1.71, df=1 (p=0.19), I2=41.4%; online supplemental figure S11) in change of ODI scores at 1 year with a mean difference of −12.22% (95% CI −18.06% to −6.38%, p<0.0001) in RCTs compared with a mean difference of −20.05% (95% CI –30.26% to –9.85%, p<0.0001) in non-RCTs.
There was no significant difference in ODI scores at 12 months between industry-funded studies versus non-funded studies (χ2=0.71, df=1 (p=0.40), I2 0%; online supplemental figure S12). Industry-funded studies had a mean difference of −19.13% (95% CI −22.49% to −15.77%, p<0.0001) whereas non-funded studies had a mean difference of −15.12% (95% CI −23.84% to −6.40%, p<0.0001).
Subgroup analysis based on stimulation waveform (paresthesia-based vs non-paresthesia-based) revealed no statistically significant difference in the primary outcome between the two modes of stimulation (χ2=0.09, df=1 (p=0.76), I2=0%; online supplemental figure S13).
Discussion
This meta-analysis revealed statistical and clinically meaningful improvements in ODI at 12 months after SCS therapy for patients with chronic back pain. Specifically, an improvement in ODI scores of 17% was reported after SCS therapy, which surpasses the threshold for substantial improvement in ODI score (MCID of 10% or 12.8% based on prior studies).29 30 However, these results should be interpreted with caution due to a very low certainty of evidence as per the GRADE framework and substantial statistical, clinical, and methodological heterogeneity. Further, this meta-analysis also revealed statistical and clinically meaningful improvements in SF-36 scores at 6 months and ODI scores that persisted across all time points up to 24 months, highlighting long-term efficacy of this therapy. These findings are important because low back pain continues to be the leading cause of years lost to disability per the Global Burden of Disease Study.75 By alleviating pain severity, SCS therapy may enable patients to resume daily activities and engage in physical therapy, further accelerating their recovery and functionality. These positive benefits also compliment other benefits from SCS therapy including superior analgesia, satisfaction, QoL and reduced analgesic use.1 2 10–17 19 76
The subgroup analysis based on funding source did not reveal any difference in ODI improvement between industry-funded studies versus non-funded studies. In general, the literature has highlighted that industry-funded studies tend to report larger therapeutic effect sizes.77 78 Of note, even among the non-funded studies, some authors reported conflicts of interests with industry. One study received funding from a non-industry source, although there were insufficient studies in this category to pool in the subgroup analysis.22 Further, we observed no subgroup differences based on waveform paradigms (paresthesia-based vs non-paresthesia-based stimulation), indicating that SCS may provide similar functional benefits regardless of waveform.
The improvement in physical function may be an ancillary benefit of SCS therapy. Improvements in pain intensity usually precede improvements in physical function. After achieving adequate analgesia, patients can subsequently increase mobility, exercise, and participate in physical therapy, thus enabling patients to regain functionality as an ancillary benefit. Some studies have also reported improvements in neurological function after SCS therapy, which may also facilitate functionality. Rowald et al reported that activity-dependent SCS can restore motor function in the trunk and lower extremities in patients with complete paralysis.79 Another study investigating SCS therapy in patients with PDN reported improvement in neurological physical exam after SCS therapy.17 The promotion of neural plasticity from neuromodulation is a leading theory, although the exact mechanism is yet to be fully elucidated.80
This meta-analysis has several strengths. First, our search strategy was comprehensive of multiple databases to capture as many studies as possible. Second, we adhered to the PRISMA guidelines while conducting this review. Third, the study abstracts quantitative data of ODI which is a well-established and validated questionnaire with good reliability for low back pain.81 82 Forth, the study attempted to address heterogeneity by performing multiple subgroup analyses.
The study’s results should be interpreted with the following limitations taken into consideration. First, most of the studies were observational in design with only seven RCTs, which was a primary contributor to the very low GRADE quality rating. Second, there was high statistical heterogeneity between studies in the pooled outcomes as highlighted by an I2 statistic >50% among outcomes. This statistical heterogeneity is likely a reflection of substantial methodological and clinical heterogeneity between included studies. Possible sources of methodological heterogeneity included duration of follow-up, study design, and type of outcome measure tool used. Possible sources of clinical heterogeneity included variable patients’ characteristics and demographics, severity of chronic pain conditions and disability, and differences in methods of the studies in patients’ inclusion, type of interventional procedure, SCS settings and waveforms, and geographical location and associated practice variation. Third, discrepancies between the final systematic review and the initial registered protocol were due to the lack of subgroup analysis based on implantation types (eg, paddle vs percutaneous) or publication decade because studies did not stratify based on these parameters and a majority of high-quality studies on neuromodulation have been performed within the last decade.
Fourth, it would be an oversimplification to only depend on a score to describe the complex and multilayered outcome of physical functioning. While ODI, SF-36 and other scores have been well validated and reliable metrics, we understand that these metrics alone do not capture the whole clinical picture and a comprehensive approach to describing outcomes is still needed. Fifth, there was an abundance of funded studies, which reflect the heavy presence of funded neuromodulation and pain medicine literature with potential for industry bias. Sixth, while we attempted to discern and exclude duplicated patient populations that overlapped between different studies, there is a possibility that this was not completely accounted for in the analysis. Finally, although the Egger’s test did not reveal a significant p value, visual inspection of the funnel plot revealed asymmetry indicating the possibility of small-study effects; as a conservative approach, we rated down the GRADE domain for publication bias based on this visual assessment of the funnel plot.
Future research and reviews should highlight physical functioning outcomes and investigate changes in not only numerical score changes but also categories of physical functioning. Observational studies should increasingly adhere to STROBE guidelines to improve the quality of research. The authors of this study encourage the clinical emphasis on physical function goals during patients’ recovery.
Conclusion
The results of this meta-analysis suggest that there may be clinically relevant improvements in physical functioning as measured by ODI and SF-36 scores following SCS therapy. However, these findings should be interpreted with caution due to the very low certainty of evidence as per the GRADE framework as well as high heterogeneity.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors thank Larry Prokop MLS from Mayo Library System, Mayo Clinic, Rochester, MN for his contribution with the literature search.
References
Footnotes
Contributors All authors contributed to the manuscript, revised the manuscript critically for intellectual content, and approved the final version. RSD'S, corresponding author, accepts full responsibility for the finished work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests RSD'S receives funding from investigator-initiated grants with Nevro Corp and Saol Therapeutics. RSD'S is an associate editor for Regional Anesthesia & Pain Medicine. The rest of the authors report no conflicts of interest.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.