Article Text

Abstract
Background Variability in anatomy in the knees supports the use of aggressive lesioning techniques such as bipolar-radiofrequency ablation (RFA) to treat knee osteoarthritis (KOA). There are no randomized controlled trials evaluating the efficacy of bipolar-RFA.
Methods Sixty-four patients with KOA who experienced >50% pain relief from prognostic superomedial, superolateral and inferomedial genicular nerve blocks were randomly assigned to receive either genicular nerve local anesthetic and steroid injections with sham-RFA or local anesthetic and steroid plus bipolar-RFA. Participants and outcome adjudicators were blinded to allocation. The primary outcome was Visual Analog Scale pain score 12 months postprocedure. Secondary outcome measures included Western Ontario and McMaster Universities Arthritis (WOMAC) and Patient Global Improvement-Indexes (PGI-I).
Results Both groups experienced significant reductions in pain, with no significant differences observed at 12 months (reduction from 5.7±1.9 to 3.2±2.6 in the RFA-group vs from 5.0±1.4 to 2.6±2.4 in the control-group (p=0.40)) or any other time point. No significant changes were observed between groups for WOMAC and PGI-I at the primary endpoint, with only the control group experiencing a significant improvement in function at 12-month follow-up (mean reduction from 91.2±38.2 to 67.1±51.9 in the RFA-group (p=0.06) vs from 95.8±41.1 to 60.6±42.8 in the control group (p=0.001); p=0.85 between groups).
Conclusion Our failure to find efficacy for genicular nerve RFA, coupled with evidence showing that a plenitude of nerves supply the knee joint and preliminary studies indicating superiority of lesioning strategies targeting more than three nerves, suggest controlled trials using more aggressive lesioning strategies are warranted.
Trial registration number TCTR20170130003.
- chronic pain
- pain measurement
- treatment outcome
Data availability statement
Data are available on reasonable request. Contact coresponding author to request the data sharing.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Evidence regarding genicular nerves radiofrequency ablation (RFA) in patients with knee osteoarthritis (OA) knee pain is conflicting. Two possible reasons for negative outcomes are failure to capture the target nerves, which may be reduced by the use of bipolar radiofrequency lesioning, and the need to target more than three target nerves, which may be identified by the use of prognostic genicular nerve blocks.
WHAT THIS STUDY ADDS
This study found that a substantial proportion of individuals experienced meaningful pain relief with RFA or sham RFA coupled with local anesthetic and steroid injections at 12 months, with no statistically significant or clinically important differences between groups.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our negative study, in conjunction with recent evidence suggesting that ablating three nerves may not be sufficient to treat knee OA and that targeting more than three nerves provides better outcomes, suggests randomized controlled trials evaluating more aggressive lesioning strategies are needed to determine the efficacy of genicular nerve RFA.
Introduction
Chronic knee pain related to osteoarthritis (OA) is a common cause of disability in older patients.1 Pharmacological and physical modalities are often advocated as first-line treatments; however, these are often ineffective or poorly tolerated in many individuals.2 Surgical options such as total knee arthroplasty (TKA) can be effective in severe cases, but up to 40% may experience persistent pain, with 15% reporting severe, debilitating pain following joint replacement.3–5
Genicular nerve radiofrequency ablation (RFA) has been touted as a safe and effective minimally invasive surgical alternative in patients with refractory knee OA (KOA),6 though several well-designed sham-controlled trials failed to demonstrate benefit post-TKA using conventional RFA7 8 and a recent large, multicenter database review reported only modest benefit in non-operated knees.9 In this latter study, the use of cooled RFA and performing multiple lesions per targeted nerve were associated with improved outcomes, suggesting more aggressive lesioning strategies may be necessary to optimize treatment outcomes. This finding is supported by anatomical studies demonstrating significant variability in the course and ideal RF targeting points of the genicular nerves,10–12 and a cadaveric study showing better nerve capture rates when cooled RFA is used than when conventional RFA is employed, which was attributed to the larger lesions created amidst anatomical variations.13
Bipolar RFA uses symmetrically placed active electrodes that serve as a conduit for electrical current, resulting in larger lesions than conventional monopolar RFA. Similar to cooled RFA, given the significant variability in genicular nerve location, bipolar RFA should theoretically be ideal for genicular nerve RFA. In one study performed in bovine liver, Cosman et al found that bipolar RF lesions between parallel cannulae resulted in ‘rounded brick-shaped’ lesions comparable in size to three sequential monopolar lesions generated using the same cannulae and generator settings.14 However, there are certain differences between bipolar and monopolar that require an understanding of electrical and thermal conductivity to optimize lesion size. For example, interelectrode distances <5 mm or >15 mm have detrimental effects on lesion formation, placing electrodes parallel to bone reduces the expected lesion size because of heat propagation into bone at the expense of soft tissue, and the effect of fluid modulation is dependent on interelectrode distance.15 Despite the conceptual appeal of bipolar RFA, to date only anecdotal evidence supports its utilization.16 The objective of this randomized, double-blind study was to examine the efficacy of genicular nerve bipolar (GNB) RFA for chronic KOA compared with GNB performed with local anesthetic and steroid plus sham RFA.
Patients and methods
This study was registered with the WHO International Clinical Trials Registry Platform (TCTR20170130003) in January 2017. All participants were recruited between March 2017 to March 2018 and provided written, informed consent; the delay in publication was due to unexpected logistical delays in preparation (ie, from the pandemic, related personnel changes in translation services). Inclusion criteria were 18–85 years of age, severe OA (Kellgren-Lawrence grade III or IV), chronic knee pain greater than 3 months, failure of previous conservative treatments, and a positive prognostic GNB.
Exclusion criteria included acute knee pain, active, non-stable inflammation, any type of knee surgery, previous RF treatment (none screened) or intra-articular injection with steroids or hyaluronic acid in the previous 6 months, prolonged pain relief from prognostic block obviating the need for RFA, known allergy to any study medication, uncontrolled psychiatric or neurological diseases, documented radiculopathy, and the presence of connective tissue diseases affecting the knees.
Study design
Participants were randomized into two equal groups using a computer-generated randomization table and sealed envelope system. Participants, outcome assessors, and statisticians were all blinded to treatment allocation through 12-month follow-up. The proceduralists included two board-certified pain physicians with >7 years of experiences in pain management (NT, RS) and two second year pain fellows who performed parts of procedures under close supervision (eg, WM). The control group (C-group) received a genicular block at three target sites with local anesthetic and corticosteroid plus sham RFA while the RF group underwent bipolar RFA following injection with the same dose of local anesthetic and corticosteroid. Patients were permitted to continue stable analgesic therapies (eg, pharmacotherapy, exercise), with non-steroidal anti-inflammatory drugs used as rescue medications, or in the case of a contraindication or failed prior therapy, codeine or tramadol if deemed necessary.
Procedures
Prognostic GNB
The procedures were performed with patients lying supine with their knees flexed forward using fluoroscopic guidance and superficial anesthesia with <5 mL of lidocaine 1% injected through 25-gage needles, without sedation. A true anteroposterior image of the targeted knee was obtained to identify the injection points as described in previous studies.17 The three targeted nerves were the superomedial, superolateral and inferomedial genicular nerves, which were accessed through 22-gage spinal needles on the medial and the lateral diaphyseal-metaphyseal transition points of the femur, and the medial diaphyseal-metaphyseal transition point of the tibia, respectively, at 60%–75% depths from the posterior borders in lateral views. After negative aspiration, 1 mL of lidocaine 2% was injected at each site. A positive response was defined as >50% pain reduction at rest and with movement lasting at least 2 hours based on patient pain report via a telephone interview performed by a coinvestigator 24 hours postprocedure.
Bipolar RFA
Superficial anesthesia was administered for all ablative procedures, with light sedation administered as indicated. 10 cm 18-gage RF cannulas with 10 mm, curved active tips (Diros technologies, Toronto, Canada) were inserted in a slightly oblique (ie, near-parallel) fashion using coaxial views, similar to the approach used for prognostic blocks. The two cannulas were placed under fluoroscopic guidance with intermittent anteroposterior and lateral images, 3–6 mm above and below the anticipated location for each targeted nerve (ie, 6–12 mm apart), <5 mm from bone at about two-thirds depth from the posterior borders of the femur and tibia18 19 (figure 1).
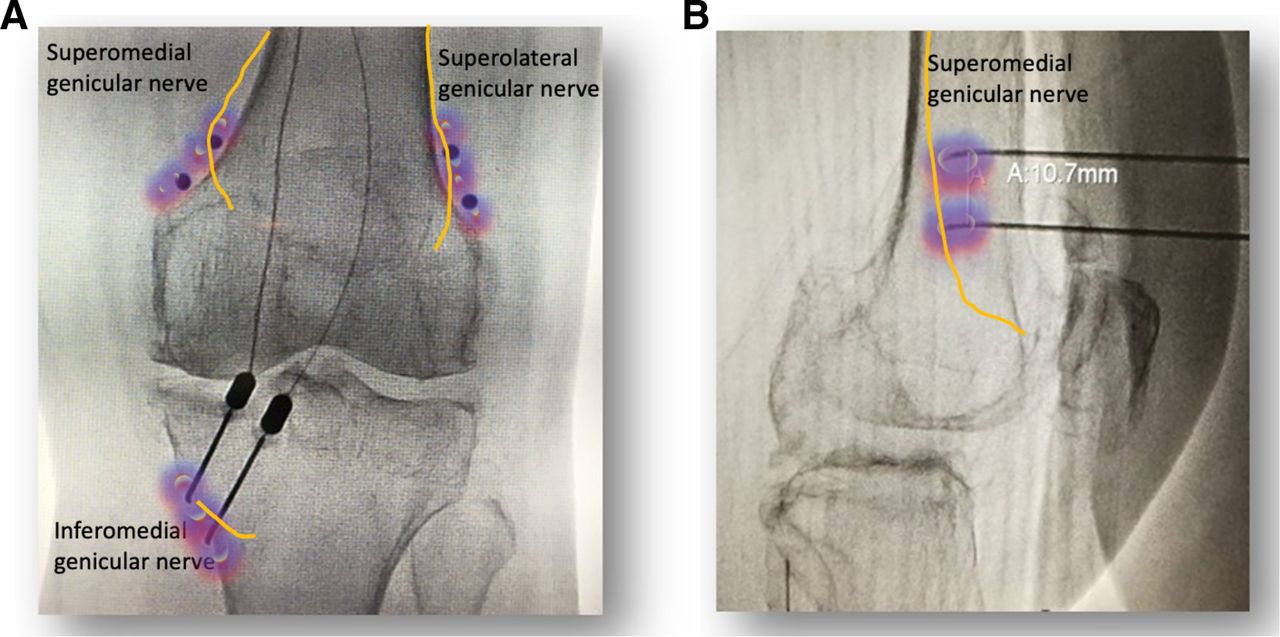
Bipolar needle positioning in the AP and lateral views. Needle distance was based on computerized measurements. Purple luminosities signify schematic representation of bipolar radiofrequency lesions, yellow lines indicate anticipated trajectory of target nerves at site of lesioning. (A) Demonstrates anticipated placement (black dots indicate electrode target sites) for the superomedial and superolateral genicular nerves and actual placement for the inferomedial genicular nerve. (B) Demonstrates actual needle placement for the superomedial genicular nerve.
Sensory stimulation at 50 Hz was performed to confirm sufficient electrode proximity to the nerves, with concordant stimulation ideally obtained at less than 0.6 V. To avoid motor nerve damage, the absence of distal leg movement was verified using stimulation of 2 Hz at up to 2.0 V. Prior to activating the bipolar RF generator, 2 mL of lidocaine 2% mixed with 2.5 mg dexamethasone was injected at each of three target nerves, with steroid added to prevent neuritis.20 21 After waiting for 2 min, RF lesioning was initiated at 90°C for 180 s, simultaneously generating three large contiguous lesions (URF-3AP, Diros technologies, Toronto, Canada).
Sham RFA
For the control group, 10 cm 22-gage RF cannulas with 5 mm active tip were placed in the same manner as for the verum RFA group. Smaller cannulas were employed to minimize tissue damage, but provide the same simulated experience. Sensory and motor stimulation were performed as above, ideally obtaining concordant sensory stimulation at a threshold below 0.6 V. Once the physician was satisfied with electrode placement, the same lidocaine and dexamethasone mixture was injected. This was followed by a 2 min waiting period, after which sham RFA was accomplished using low-grade sensory stimulation at 50 Hz at 1.0 V for 180 s.
Follow-up visits and outcome measures
Baseline data were recorded after randomization in the week prior to treatment. Demographic and clinical data were documented, with outcome measures recorded at 1, 2, 4, 6, 8, 10 and 12 months in-person visits, with telephone follow-ups permitted for those with logistical obstacles for in-person visits. No contact was permitted between study investigators and patients, with any medication adjustments performed by disinterested providers.
The primary outcome was the 0–10 Visual Analog Scale (VAS; 0=no pain, 10=worst pain) recorded at 1, 2, 4, 6, 8, 10, 12 months follow ups, with 12 months designated as the primary endpoint. Secondary outcomes measures included the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)22 and the 7-point Patient Global Impression of Improvement (PGI-I) Likert scale, for which lower scores indicate less functional limitations and greater satisfaction. Analgesic requirements were measured using the WHO analgesic stepladder, in which first-line treatments include non-steroidal anti-inflammatory drugs and adjuvants, second-line treatments include weak (eg, codeine, tramadol) or low-dose (< 30 oral morphine equivalents/d) opioids and third-line treatments include higher doses of opioids. In addition to the outcome measures described above, a positive categorical outcome (ie, responder) was designated as >2 points decrease in VAS pain score coupled with a score <3 on PGI-I (very much, much, or a little better) and the absence of any significant increases in analgesic medications, defined as an increase in the WHO stepladder tier (eg, starting a new analgesic or an increase in opioid dose). Procedural complications including hematoma, infection, and neurological complications (eg, abnormal proprioception, numbness, paresthesia, neuralgia, and motor weakness) were also recorded.
Sample size justification and statistical analysis
Choi et al reported a VAS pain score difference of 35.5 mm at their primary endpoint.17 We hypothesized that RFA would provide greater VAS pain score reduction than nerve block alone and that a difference of 20 mm between groups on the VAS would represent a clinically meaningful effect consistent with clinical studies performed for major joint OA.23 We calculated that achieving this robust effect size of 0.79 would require 27 patients per group using an alpha error of 0.05 and a beta error of 0.8 on Student’s t-test. To account for possible drop-outs, we anticipating enrolling 32 patients per group.
Statistical analyses were conducted using STATA/IC Software, V.17.0 with a p<0.05 being considered statistically significant. We described categorical variables using frequency and percentage and continuous variables with mean and SD.
The normality of continuous data was assessed using the Kolmogorov-Smirnov test. Comparisons of repeated measurements included log transformation on data that were non-normally distribution, and data analyses were performed using repeated measures analysis of variance with baseline pain scores adjusted for between-group differences and the Sidak test for intragroup comparisons. The generalized estimating equation (GEE) method was used for investigating interactions between treatment groups and time for the primary outcome measure.
For head-to-head comparisons at each time point, non-normally distributed continuous data and ordinal data were analyzed using the Mann-Whitney U test (for between-group comparisons) and Wilcoxon signed ranks test (for intragroup comparisons). Categorical data were analyzed using the χ2 test or Fisher’s exact test, as appropriate.
Results
One hundred and ninety-eight patients were screened, with 150 patients deemed eligible for a prognostic GNB. 36.7% experienced prolonged pain relief obviating the need for RFA treatment, 12% experienced a negative block and 8% elected to undergo alternative, non-RFA treatments, leaving 64 patients who were enrolled (figure 2). The average age of participants was 66.7±9.8 years, with 81% being female. They reported moderate pain at baseline (mean VAS score; 6.5±1.7) for an average duration of 5.1±3.6 years. None were on high-dose opioids. Among 32 patients in each group, there were no statistical differences in demographic or clinical variables (table 1).
Baseline demographic data stratified by treatment group (n=64)
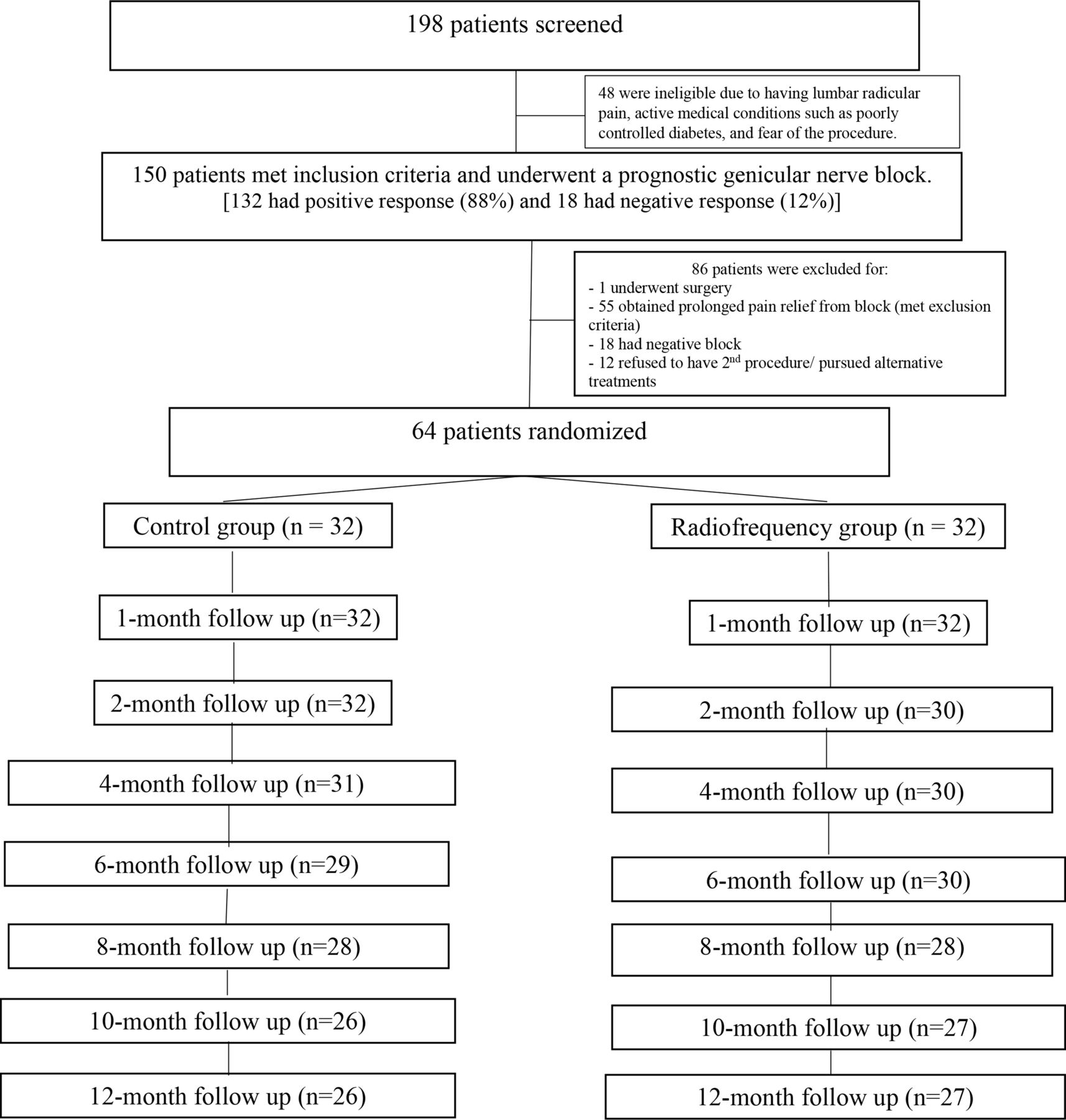
CONSORT patient flow diagram demonstrating study progression. CONSORT, Consolidated Standards of Reporting Trials.
Group differences
After log transformation data adjustment, analyses of repeated measurements were conducted. There were no significant differences between groups for VAS pain score (p=0.38), WOMAC-total score (p=0.83), WOMAC-subscale scores (pain: p=0.45, stiffness: p=0.32 and function: p=0.34), or PGI-I (p=0.73) as similar in intragroup comparison in both groups. The interaction effect between treatment groups and time for pain scores was statistically insignificant (p=0.40).
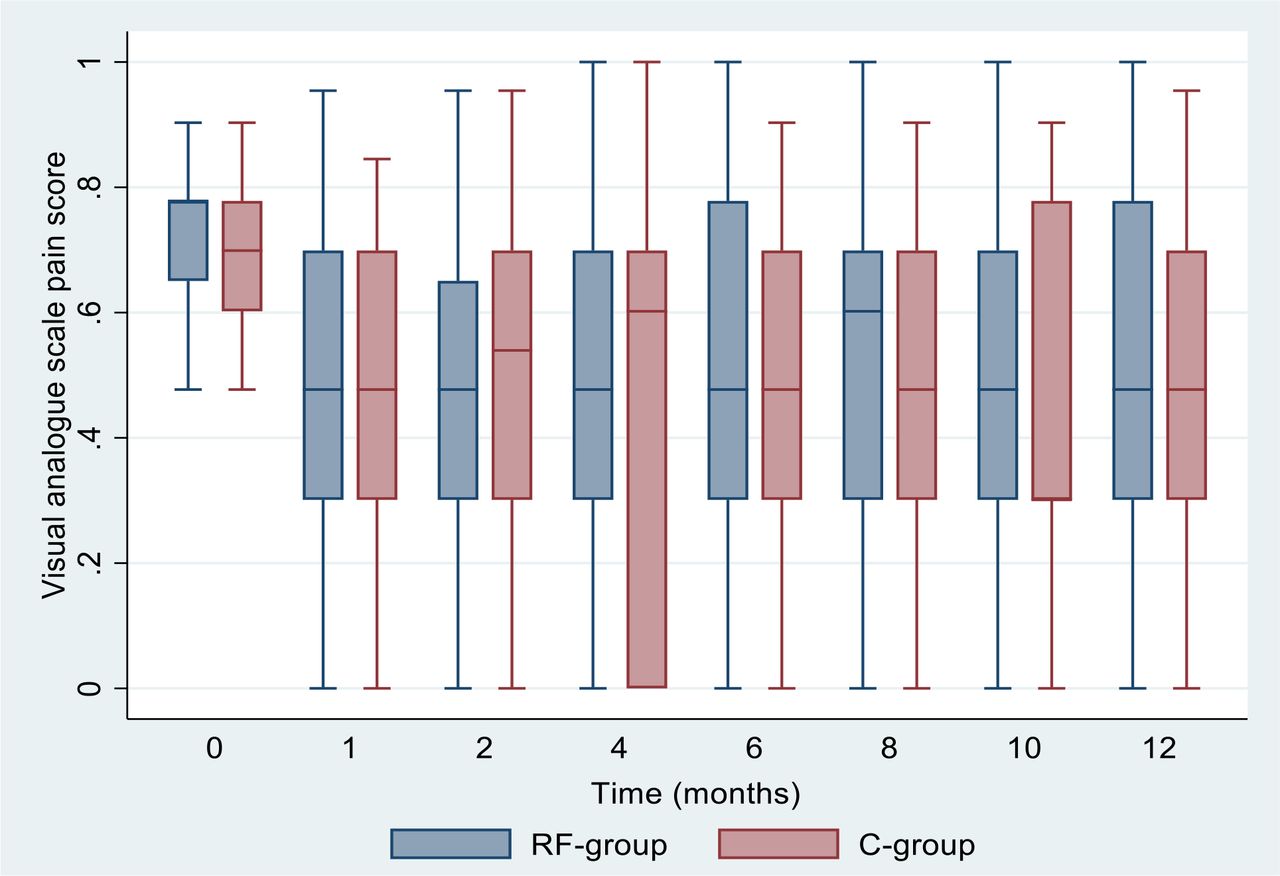
At the 12-month primary endpoint, there were no statistical differences in the primary outcome measure, average VAS pain score (in RFA group 3.2±2.6 vs 2.6±2.4 in control group; p=0.40), or at any other time point (figure 3). The mean difference from baseline in average VAS score also failed to reach statistical significance (2.3±2.8 in the RFA group vs 2.2±2.4 in the sham group; p=0.73). The difference between the control and RFA group for this outcome measure was significant only at the 4-month time point (mean difference from baseline 2.5±2.5 in the RFA group vs 1.1±2.7 in the control group; p=0.04). However, the mean reduction in pain score was not significant at either the 2 month (p=0.82) or 6-month (p=0.29) time point, or at the 4-month time point for mean reduction in WOMAC pain score (p=0.95).
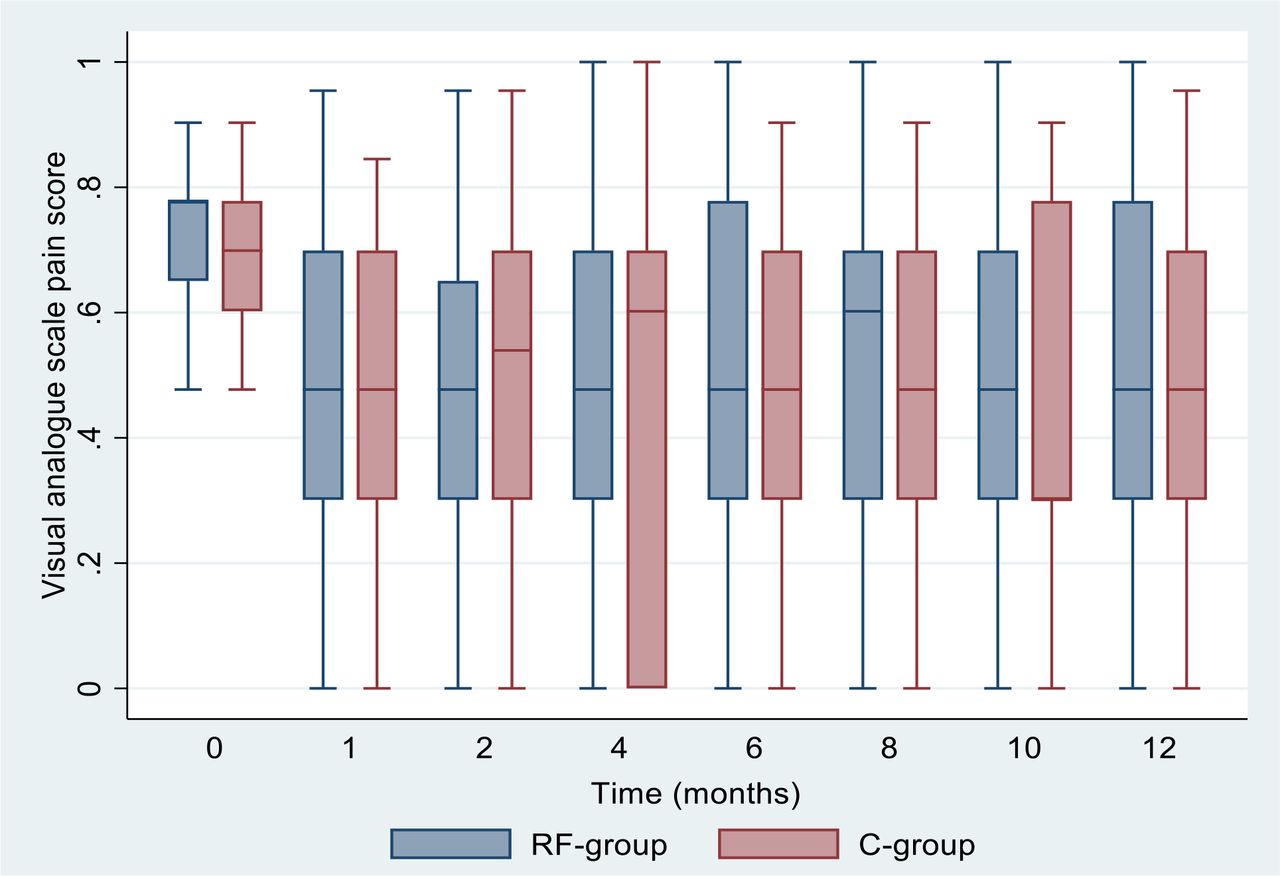
Comparison of pain intensity between treatment groups. RF, radiofrequency.
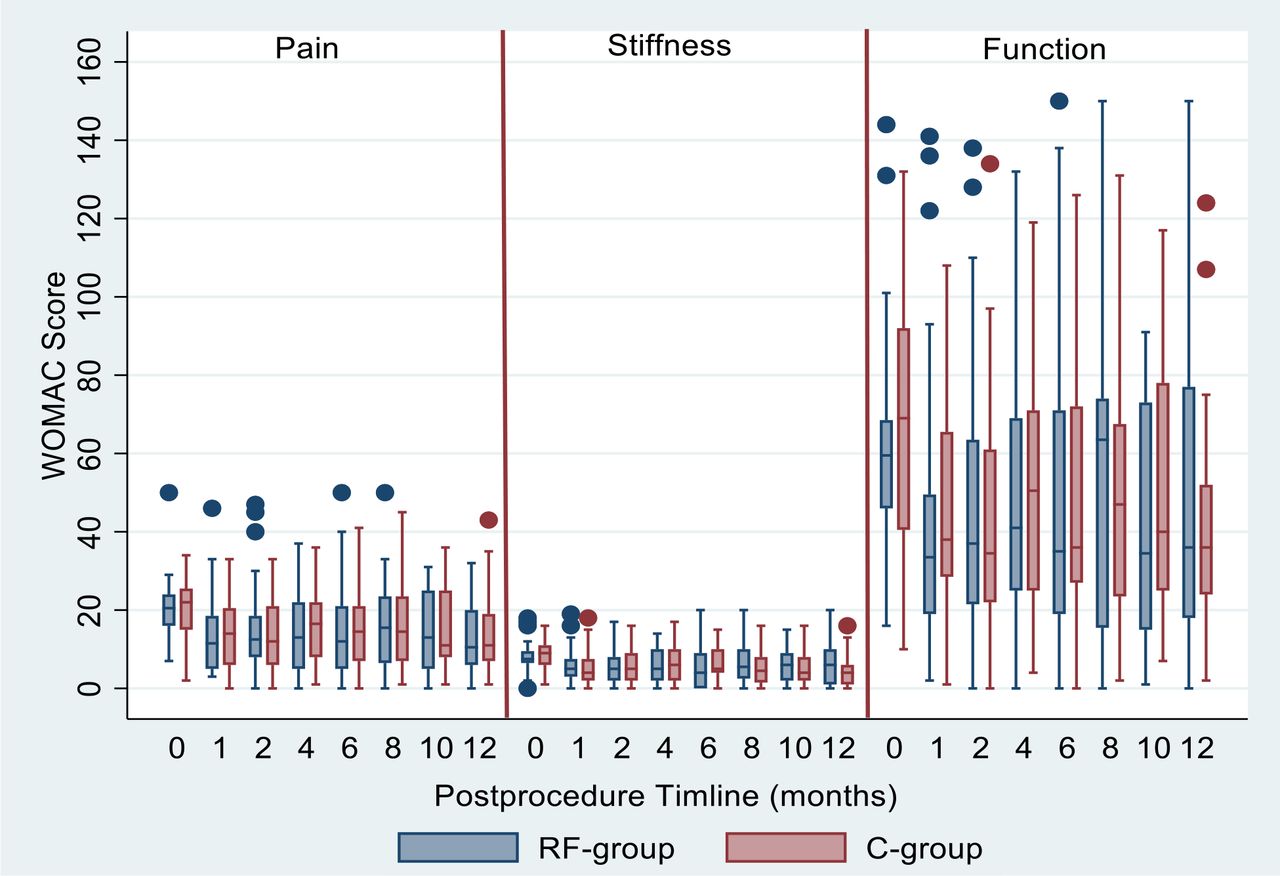
Neither the difference between groups in the overall WOMAC score (67.1±51.9 in the RFA group vs 60.6±42.8 in the control group; p=0.85) nor the mean reduction from baseline in the overall WOMAC score (17.7±49.2 in the RFA group vs 24.6±38.5 in the control group; p=0.70) reached statistical significance at the 12 month primary endpoint, or any other time point. For individual WOMAC subscales, there were no differences in mean scores or mean reductions from baseline in any subscore at 12 months or other follow-up periods (table 2, figure 4).
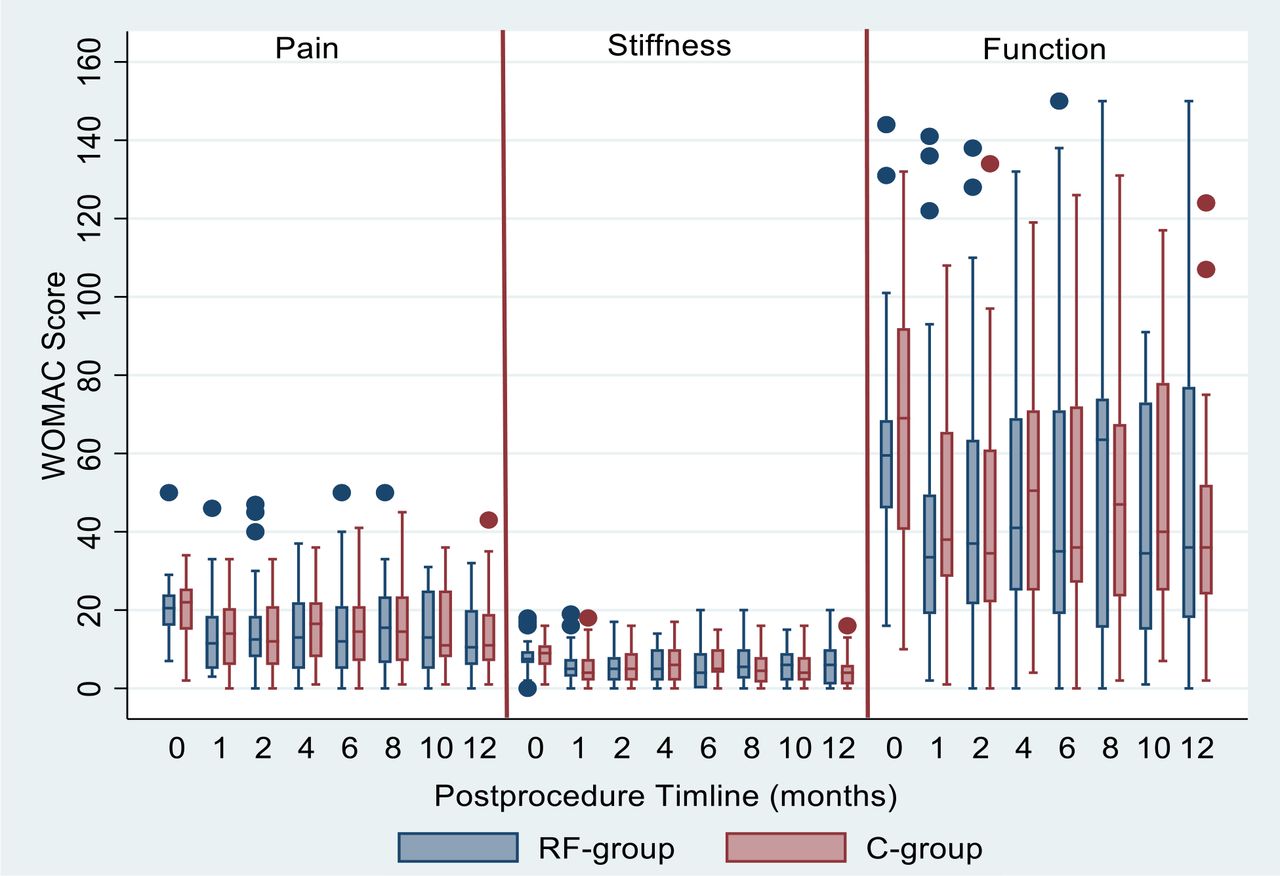
Comparison of Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores between treatment groups. RF, radiofrequency.
Comparison of outcome data through 12-month follow-up
Mean PGI-I scores did not significantly differ between groups at 12 months (2.8±1.3 in the RFA group vs 2.6±1.3 in sham group; p=0.56) or other time points (table 2). There were also no between-group differences in analgesic consumption at any time point, with slight reductions in analgesic consumption observed over the course of the study. At baseline, 16 (50%) and 17 (53%) patients in the RFA and control groups were on non-opioid analgesics, which declined slightly to 13 (44%) and 13 participants (43%), respectively, at 12 months. There was a slight reduction in participants receiving either codeine or tramadol, which declined from 50% (n=16) to 41% (n=12) in the RFA group, and from 47% (n=15) to 37% (n=11) in the sham RFA group. Two patients in RFA group and one patient in sham RFA group who failed to derive benefit from their procedure were started on tramadol or codeine as rescue therapy.
Within-group changes
Within-group differences revealed statistically significant reductions in VAS pain score (mean reduction from baseline of 2.3±2.8 in the RFA group (p=0.001) vs 2.2±2.4 in the control group (p<0.001) at 12 months.
For WOMAC-total score, at 12-month, there was a significant reduction from baseline only in control group (From 95.8±41.1 to 60.6±42.8; p=0.01 vs. from 91.2±38.2 to 67.1±51.9 in the RF-group; p=0.06). For WOMAC-subscale, every subscale was significant difference when compared with baseline in both groups through 6 months, but at the 12-month primary endpoint, there was a significance only in the sham group as shown in table 2.
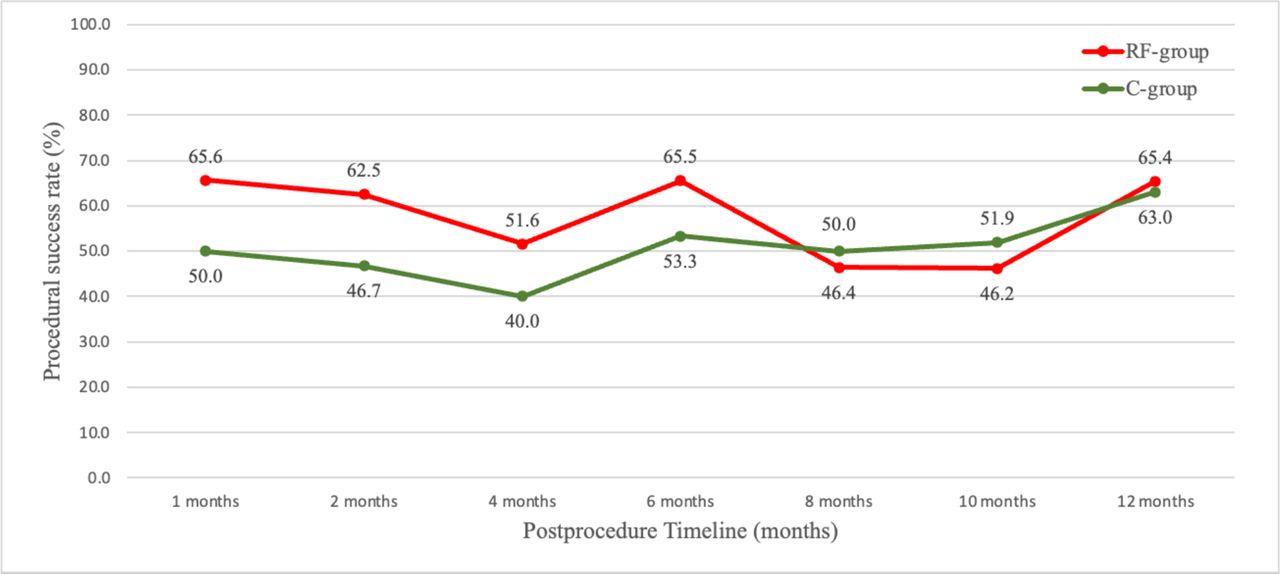
For the binary composite outcome measure, the procedural success rates at 1, 2, 4, 6, 8, 10 and 12 months were 67%, 63%, 52%, 66%, 46%, 46% and 65% in the RFA group, and 50%, 47%, 40%, 53%, 50%, 52% and 63% in the control group, respectively (p=0.86 at 12 months, figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Procedural success rate stratified by study timeline. RF, radiofrequency.
There was no participant withdrawal due to adverse effects. One patient developed significant swelling after the RF procedure which returned to normal within 4 weeks. An MRI of the knee performed 3 weeks after procedure showed quadriceps tendonitis without a fluid collection.
Discussion
In this first double-blind placebo-controlled trial assessing the efficacy of bipolar RF ablation of genicular nerve in chronic KOA. We found significant improvements in pain and function at varying time points for both verum RFA and GNB with local anesthetic and steroid, with no significant differences between groups for any primary or secondary outcome measure.
Comparison to other studies
Although the intermediate-term efficacy of genicular nerve RFA has been shown in comparative-effectiveness and placebo-controlled studies,17 24–27 these studies suffered from numerous methodological and technical flaws including small numbers, suboptimal RF technique including targeting only a small proportion of pain-transmitting nerves, suspect blinding and failure to control for concurrent treatments. More recent well-designed sham-controlled studies have failed to demonstrate efficacy compared with sham RFA, though these studies were performed in individuals scheduled to undergo TKR, which might dwarf any effect of RFA and may result in persistent soft-tissue pain that is not amenable to RFA.7 8 There is little pathophysiological basis for nerve blocks with short-acting local anesthetic and steroids to provide long-term relief for non-neuropathic pain,20 21 though randomized trials evaluating the effectiveness of GNB with local anesthetic and steroids have consistently reported intermediate-term benefit.28–30 The fact that an early placebo-controlled trial that compared RFA to local anesthetic alone accompanied by sham RFA failed to demonstrate any meaningful benefit for the ‘control’ group,17 but that this study demonstrated benefit for both RFA and sham RFA with local anesthetic and steroid, raises questions concerning whether the effects of bias, a stronger placebo effect when nerve blocks are marketed as treatments rather than prognostic tests, or possible nerve inflammation (which might respond to steroids) in a subset of patients contributed to sustained benefit in the control group. At present, there is no evidence to support genicular neuritis as a contributing factor in patients with KOA, and reviews have demonstrated the influence ‘bias’ has on the outcomes of interventional pain procedures.31 For diagnostic medial branch blocks, some guidelines assert that pain relief which lasts longer than 7 hours from lidocaine or 24 hours from bupivacaine is more likely to indicate a placebo response than a true response.20 21 Possible physiological reasons why one might observe long-term benefit from a short-acting nerve block include the reversal central sensitization, breaking the cycle of pain, providing a therapeutic window during which activity can be increased and deconditioning reversed, prolonged neural blockade, and improving sleep in individuals with sleep dysfunction, which raises pain sensitivity thresholds.20 21 Regarding a possible robust and prolonged placebo effect, reviews have found that the placebo response is especially strong for interventional procedures containing elaborate rituals such as real or sham RFA, may endure for months depending on expectations, and may be higher in some ethnic populations (eg, Asian) secondary to culture and possibly even genetics.32 33
Explanation of findings
There are several possible reasons for our failure to detect a significant difference between the RFA and control groups. Perhaps the main contributing factor in our inability to detect a difference between the RFA and sham RFA groups was the high response rate in the latter. For the subjective outcome of pain, the placebo effect is indubitably stronger than the intrinsic effect of even some efficacious treatments, is higher for invasive, ritualistic procedures such as RFA than it is for medications, and may endure for months or even years depending on the anticipated duration of benefit.34 35 This may be why unblinded, comparative-effectiveness studies have consistently demonstrated superiority for RFA36 37 compared with less invasive treatments. Second, studies have consistently found a positive rate of ‘prognostic’ GNB exceeding 80%, with one randomized study failing to demonstrate a difference in genicular nerve RFA outcomes between patients who experienced >50% relief from prognostic GNB and those who underwent RFA without receiving a GNB.11 38 Whereas some might interpret this as evidence against performing prognostic blocks, one large retrospective study found that individuals who experienced >80% relief on GNB obtained better outcomes than those who received between 50% and 79% relief9; this suggests that our 50% cut-off threshold may have been too low. Third, we failed to exclude patients with secondary gain, mild psychopathology, sleep dysfunction, high degrees of disease burden, and the substantial proportion of subjects with possible nociplastic overlay to their KOA, all of whom are more likely to fail interventional treatments.11 28 30 39–44 We also included individuals within a wide age spectrum, as inclusivity enhances generalization. Fourth, it is possible that bipolar lesioning may have missed the targeted nerves, which may be more likely to occur with electrodes oriented parallel immediately adjacent to bone (as is typical for the nerves we targeted) or interelectrode distances that are too small or too large. But the most likely reason for our inability to demonstrate efficacy for genicular nerve RFA is that the nerves we targeted supply only a small percentage of the nociceptive input in KOA, and given the neuroanatomical variations in knee innervation, some nerves may have been missed despite creating large, bipolar lesions and using sensory stimulation to identify neural targets. Whereas bipolar lesions can enhance lesion size under optimal conditions when the electrodes are placed in tissues with similar impedance and conductive properties, when suboptimal conditions exist, two asymmetrical monopolar lesions may ensue. The hypothesis that more than 3 nerves need to be targeted is supported by anatomical studies and reviews demonstrating over 10 pain-transmitted nerves amenable to RFA,10 12 45 46 and 2 clinical studies showing superior outcomes for RFA and GNB when greater than 3 nerves are treated.9 29 Future studies could address this issue by using a more aggressive lesioning strategy, as one large National Institutes of Health study is currently doing (A Sequenced Strategy for Improving Outcomes in People with Knee Osteoarthritis Pain, Clinicaltrials.gov Identifier: NCT04504812).
Strengths
This is the first study to evaluate genicular nerve RFA using sensory stimulation with bipolar electrodes, which create large lesions ideally suited to treat KOA. Unlike many previous studies which failed to use prognostic blocks to select patients,7 8 27 47 we used low-volume lidocaine blocks, and studied a unique population underrepresented in clinical trials. Although the use of prognostic blocks that contain no diagnostic value and have a positive rate exceeding 80%—as we observed in this trial—is controversial, excluding non-responders may enhance statistical power. Finally, our long, 12-month follow-up under blinded conditions without crossover is extremely unusual in clinical interventional trials and bolsters our findings that RFA is not superior to GNB with sham RFA (ie, patients do not over-report pain in a control group to crossover at an early time point). However, a blinded 12-month follow-up also makes it more likely than usual that patients may pursue unrecorded interventions outside of the study.
Limitations
There are several limitations of our study that warrant mentioning. First, we permitted concurrent analgesic therapies in an elderly population that may have had concomitant pain conditions. Although these therapies were equally distributed and no patient received high-dose opioids, this may have dampened a small signal of efficacy. Second, we did not exclude patients with secondary gain, diffuse pain phenotypes, which may indicate central sensitization, minor psychopathology and sleep abnormalities that may nevertheless affect treatment response, and high degrees of disease burden including opioid use and multiple prior unsuccessful interventional treatments. Whereas our inclusive selection criteria enhance generalization, all of these factors may predispose patients to treatment failure, thus undermining our ability to detect small treatment effects. Third, we added steroids to both groups to prevent neuritis in the RFA group, though some studies have found intermediate-term benefit from GNB with steroids48; and to blind participants we performed sensory stimulation for 180 s on the sham group, which could theoretically also have an analgesic effect or enhance the placebo effect. In addition, depo-steroids injected before monopolar RFA were shown in one study to decrease lesion size, though the effects of soluble steroids before bipolar RFA are unknown.49 Fourth, the proportion of females in our study was greater than the typical female predominance in KOA studies, and may reflect unique cultural issues.50 Larger numbers of participants may have reduced non-significant baseline differences in demographic data and outcome measures (eg, sex and baseline pain scores). Finally, our study may have been underpowered as the effect sizes were estimated based on an older controlled study,17 which was published before more recent negative placebo-controlled studies emerged in patients scheduled to undergo TKR,7 8 which is a suboptimal population when the goal is to establish efficacy. This effect may have been amplified by the addition of steroids to the sham group (ie, a comparative-effectiveness study). Consequently, the lower starting point for our primary outcome measure (ie, lower baseline pain scores) in the control group reduced the likelihood of finding a lower mean score at our primary endpoint.
Conclusions
In conclusion, we found that a substantial proportion of individuals experienced meaningful pain relief with RFA or sham RFA coupled with local anesthetic and steroid injections, with no statistically significant or clinically important differences between groups. In conjunction with recent evidence suggesting that ablating three nerves may not be sufficient to treat KOA and that targeting more than three nerves provides better outcomes, we recommend randomized controlled trials evaluating more aggressive lesioning strategies, including with bipolar RFA which has the theoretical potential to increase the nerve capture rate.
Supplemental material
Supplemental material
Data availability statement
Data are available on reasonable request. Contact coresponding author to request the data sharing.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics Committees at Faculty of Medicine Ramathibodi hospital, Mahidol University, Bangkok, ThailandEC ID; 12-59-06. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors gratefully acknowledge the assistance of Mrs.Supak Ukritchon for statistical analysis. Also, we want to thank pain nurses at Ramathibodi hospital, including Mrs. Juthamas Jarupongsa for hard-working during 12 months of consecutive follow-up data gathering.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors WM, NT and RS contributed to the conception and design of the study. WM, NT, RS and SW were involved in data acquisition. WM, NT and SPC analyzed and interpreted data, drafting the article and revising it critically for important intellectual content. All authors approved the final version of the manuscript and agreed to be accountable for all aspects of the work in ensuring that questions related to the integrity of any part of the work were appropriately investigated and resolved. NT accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding Internal funding was used to conduct this study. SPC receives funding from the US Dept. of Defense (MIRROR, HU0001-15-2-0003; Congressionally Directed Medical Research Program, 105637007) and National Institutes of Health (GR101558, R01DA048206-01, U24NS115708, 1UH3135804).
Competing interests SPC is a consultant for Avanos (which makes radiofrequency equipment) and receives institutional research funding. WM, NT, RS and SW have no conflicts of interest to declare. Currently, SPC is the editorial board member of RAPM.FundingInternal funding was used to conduct this study. SPC receives funding from the U.S. Dept. of Defense (MIRROR, HU0001-15-2-0003; Congressionally Directed Medical Research Program, 105637007) and National Institutes of Health (GR101558, R01DA048206-01, U24NS115708, 1UH3135804).
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.