Article Text

Abstract
Background The fluoroscopic-guided epidural access is occasionally challenging; therefore, the contralateral oblique (CLO) view has emerged as an alternative approach. The CLO view appears to be optimal for mid-thoracic epidural access; however, evidence on its utility is lacking. Therefore, we aimed to evaluate the clinical usefulness of the CLO view at 60°±5° compared with the lateral (LAT) view using fluoroscopic-guided mid-thoracic epidural access.
Methods Patients were randomly allocated to undergo mid-thoracic epidural access under the fluoroscopic LAT view (LAT group) or CLO view (CLO group). The primary outcome was the first-pass success rate of mid-thoracic epidural access. The secondary outcomes were procedural pain intensity, patient satisfaction, needling time, number of needle passes, and radiation dose.
Results Seventy-nine patients were included. The first-pass success rate was significantly higher in the CLO group than in the LAT group (68.3% vs 34.2%, difference: 34.1%; 95% CI 13.3 to 54.8; p=0.003). Procedural pain intensity was significantly lower in the CLO group than in the LAT group. Patient satisfaction was significantly greater in the CLO group than in the LAT group. The needling time and the number of needle passes were significantly lower in the CLO group than in the LAT group. Radiation dose in the CLO group was significantly reduced compared with that in the LAT group.
Conclusions The fluoroscopic CLO view at 60°±5° increased the success rate and patient satisfaction and reduced the procedural time and patient discomfort compared with the LAT view when performing mid-thoracic epidural access. Therefore, the CLO view at 60°±5° can be considered for mid-thoracic epidural access under fluoroscopic guidance.
Trial registration number KCT0004926.
- analgesia
- chronic pain
- pain management
- pain, postoperative
- technology
Data availability statement
Data are available upon reasonable request.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The fluoroscopic-guided epidural access in the mid-thoracic region is occasionally challenging. The contralateral oblique (CLO) view has emerged as an alternative approach; however, evidence on its utility is lacking.
WHAT THIS STUDY ADDS
The fluoroscopic CLO view at 60°±5° increased the success rate and patient satisfaction and reduced the procedural time and patient discomfort compared with the lateral view when performing mid-thoracic epidural access.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The CLO view at 60°±5° can be considered for mid-thoracic epidural access under fluoroscopic guidance.
Introduction
Fluoroscopic-guided interventions have become a major part of managing acute and chronic pain, which can ensure safety and accuracy in clinical practice.1 2 The anteroposterior view and lateral (LAT) view are primarily obtained to recognize the needle tip position related to the target structures during fluoroscopic-guided interventions.3 A LAT view can present how far the needle is from the target area, such as the epidural space, which helps identify the needle location and secure patient safety.4 However, visualizing the interlaminar space and needle tip in the LAT view is often limited, especially at the mid-thoracic levels due to the prominent spinous processes.5 6
Considering the limitations of fluoroscopic LAT view, the contralateral oblique (CLO) view may be an alternative to the LAT view because it offers clearer visualization of the needle tip and lamina, which provides a reliable and consistent radiological landmark.4 7 CLO view can be obtained by first identifying the target lamina to which the needle tip is related and then focusing the image intensifier away in an oblique contralateral direction from the lamina.4 Compared with the systematically studied ideal angle and advantage of CLO view in the cervical or lumbar region,4 6–8 evidence of the CLO view’s utility in the mid-thoracic region is lacking.
Our previous observational study reported that the CLO view at 60° can provide clearer laminar margin visualization and a more consistent needle tip location than the LAT view in the mid-thoracic epidural access (TEA).9 TEA is mandatory for chronic pain interventions or patient-controlled epidural analgesia after major open surgeries.10 11 However, it is associated with a high failure rate,12 and up to 50% of clinical failure is believed to be related to technical factors.13 We hypothesized that the CLO view could increase the success rate and improve procedural outcomes, such as reduced needling time and decreased patient discomfort. However, no study has reported on the clinical usefulness of the CLO view compared with the conventional LAT view during mid-TEA. Therefore, we aimed to assess the clinical usefulness of the fluoroscopic CLO view at 60°±5° compared with the LAT view when approaching mid-thoracic epidural space.
Methods
Study design and participants
This trial was a single-center randomized controlled clinical trial. The prospective trial was conducted at Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. Before inclusion of the first participant, written informed consent was obtained from each participant, and the trial was registered with the Clinical Research Information Service (https://cris.nih.go.kr/cris/search/detailSearch.do/19207, KCT0004926) on 16 April 2020. Participants were enrolled from 2 June 2020 to 26 March 2021. The methodology of this study was conducted following the approved guidelines. All patients who underwent epidural steroid injection, blood patch, and epidural analgesia in the mid-thoracic (T4–T8) region were assessed for eligibility. Patients aged 20–79 years were included. Patients with allergy to local anesthetics, contrast medium, or steroids; infection at the insertion site; neurological or psychiatric disorders; prior spine instrumentation; significant anatomical variation such as severe scoliosis; pregnant patients; patients with coagulopathy; and those who used antiplatelet or anticoagulant medication were excluded.
Randomization
Patients were randomly allocated to the LAT group (mid-TEA obtained in the LAT view) or the CLO group (mid-TEA obtained in the CLO view) using a computer-generated random numbers table. Randomization was determined with block sizes of 4 and an allocation ratio of 1:1. First investigator kept opaque and sealed envelopes labeled with sequential study numbers, and which were opened just before the procedure. Although the pain physicians could not be blinded to the type of procedure, all patients were blinded to the type of procedure. The second investigator, who was not blinded to the allocation groups, assessed the procedural outcomes in the operating room. After the end of the procedure, in the postanesthetic care unit, the third investigator, who was blinded to the allocation groups, evaluated the subjective outcomes including patient satisfaction and procedural pain intensity.
TEA procedures
All patients were placed in a prone position on the operating table and monitored with pulse oximetry, non-invasive blood pressure, and a three-lead ECG. A pillow was placed under the chest to widen the target interlaminar space. All procedures were performed under fluoroscopic guidance (Ziehm Vision RFD, Ziehm, Nuremberg, Germany). After identification of the target thoracic vertebra between T4 and T8 for mid-TEAs under anteroposterior view, the patient’s skin was sterilized.
The study protocol is described in online supplemental figure 1. We performed three needle passes on each skin puncture, where a needle pass represents one instance of needle advancement without withdrawal. If the needle was readvanced after withdrawal to change the direction, it was considered as another needle pass. A maximum of three skin punctures was allowed. Consequently, up to three skin punctures with up to three needle passes each (up to nine needle passes) were allowed in the allocated view, and if the epidural access failed after the ninth attempt, only one skin puncture using the non-allocated view was allowed (crossover). According to a previous study with some modifications in the paramedian approach,14 the first needle entry point was determined to be at the junction between the mid-pedicular line and the lower endplate of the just inferior body to the target interlaminar space on an anteroposterior view (online supplemental figure 2). If epidural space was not accessed despite three needle passes at the first needle entry point, different needle entry points were determined: (1) second needle entry point was at the junction between the mid-pedicular line and the upper endplate of one vertebral segment below the target interlaminar space, (2) third needle entry point was at the junction between the mid-pedicular line and the inferior pedicle margin of one vertebral segment below the target interlaminar space (online supplemental figure 2). A 22-gauge Tuohy needle (Green Medical Supply, Seoul, Korea) or 18-gauge Tuohy needle (Perifix, B Braun Melsungen, Melsungen, Germany) was used to approach the epidural space. After local infiltration with 1% lidocaine, the Tuohy needle was advanced at an angle of 10°–15° medially and 50°–60° upward until it reached the pedicle level on the vertebral body in an anteroposterior image. The fluoroscopic device was then rotated 90° (LAT group) to visualize the spinolaminar line (an imaginary line connecting the spinolaminar junction; figures 1A and 2A) or at an angle of 60° obliquely to the contralateral direction to the needle tip (CLO group) to visualize the target interlaminar space and ventral interlaminar line (VILL; an imaginary line connecting the ventral laminar margins; figures 1B and 2B). To overcome the limited angle (45°–50° on one side and 90° on another side) of traditional fluoroscopy, the table was tilted when necessary. In addition, to optimize the CLO view, based on 60°, ±5° of adjustment was allowed. The epidural needle was subsequently advanced without using the loss-of-resistance (LOR) technique until before the spinolaminar line in the LAT group or just before the VILL in the CLO group. Needle trajectory was adjusted during advancement to avoid contacting the laminae. If the epidural needle encountered the laminae and could not be advanced, the needle was withdrawn and readvanced at a different angulation of the needle. Immediately before the spinolaminar line or just before VILL, the needle was advanced further cautiously until epidural space was reached using the LOR-to-air technique. After LOR was achieved, correct epidural access was confirmed by the spread of contrast medium injected (Omnipaque 300, GE Healthcare, Little Chalfont, UK) in the LAT view (LAT group) or CLO view at 60°±5° (CLO group) (figure 1C,D) and anteroposterior views (figure 1E,F). The procedure was conducted by two pain physicians with more than 7 years of experience in mid-TEA according to identical protocols.
Supplemental material
Supplemental material
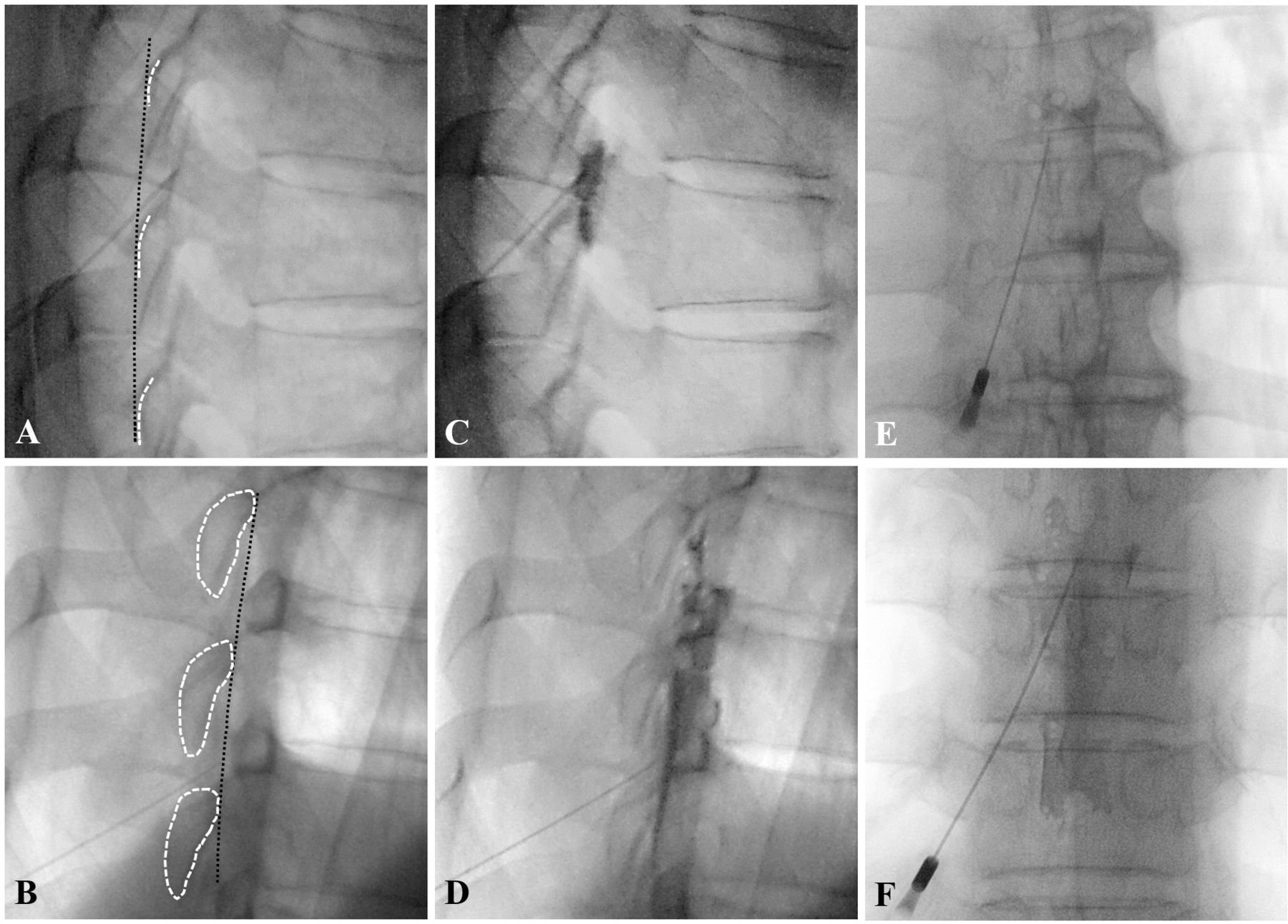
Fluoroscopic views for describing the spinolaminar line (an imaginary line connecting the spinolaminar junction) in the lateral view (A) and the ventral interlaminar line (the imaginary line connecting the ventral laminar margins) in the contralateral oblique view at 60°±5° (B). The white dot lines indicate the spinolaminar junction (A) or the laminar margin (B). The black dot lines indicate the spinolaminar line (A) or ventral interlaminar line (B). The lateral view (C) and the contralateral oblique view (D) after contrast medium administration. Anteroposterior fluoroscopic view with the spread of contrast medium in the lateral group (E) and in the contralateral oblique group (F).

Illustrations for describing the relationship between X-ray beam, the lamina of thoracic spine, and needle tip in lateral view (A) and contralateral oblique view (B).
Outcome assessments
The primary outcome was comparing the first-pass success rate of mid-TEA; achievement of successful epidural access at once without any needle withdrawal and confirmation of contrast dispersion in the epidural space (online supplemental figure 1). Secondary outcomes were as follows: (1) final success rate: achievement of successful epidural access and confirmation of contrast dispersion in the epidural space within the maximal nine needle passes in the allocated trial; (2) needling time: procedural time from the skin puncture to contrast medium administration after reaching the epidural space; (3) total number of needle passes: sum of first needle pass and additional needle passes, which was defined as a readvancement of the needle after any needle withdrawal for changing the direction; (4) number of skin punctures; (5) cross-over success: achieving successful mid-TEA in the cross-over trial; (6) relative location of the needle tip in both groups; it was defined as grade –2 (significantly posterior to the reference line that is VILL in the CLO group or spinolaminar line in the LAT group), grade –1 (just posterior to the reference line), grade 0 (on the reference line), grade +1 (just anterior to the reference line), grade +2 (significantly anterior to the reference line)9; (7) cumulative total radiation dose (cGy×cm2): it was obtained from the fluoroscopic report of each procedure15; (8) patient satisfaction: assessment after the procedure by global perceived effects on a 7-point scale with some modifications (grade 1=very dissatisfied, grade 2=somewhat dissatisfied, grade 3=slightly dissatisfied, grade 4=neither satisfied nor dissatisfied, grade 5=slightly satisfied, grade 6=somewhat satisfied, grade 7=very satisfied)16 17; (9) procedural pain intensity: assessment of a single 11-point numeric rating scale, in which 0=no pain and 10=worst pain imaginable. To obtain valid numeric rating scale and global perceived effects data, all patients were instructed on how to grade their pain using a numeric rating scale and their satisfaction using global perceived effects before the procedure. Additionally, procedure-related complications, including epidural hematoma, vasovagal reaction, dural puncture, pneumothorax, intravascular or intrathecal local anesthetic injection, and spinal cord injury, were also recorded. Clinical success, such as the analgesic efficacy of the procedure, was not evaluated because majority of the study patients underwent thoracic epidural catheter insertion for postoperative analgesia.
Statistical analysis
Data are expressed as means±SD, medians (IQR), numbers (proportion), or relative risk with a 95% CI. We focused on the primary outcome as the first-pass success rate of TEA which was compared using the χ2 test. Other categorical data were compared using the χ2 test or Fisher’s exact test, as appropriate. Normal distribution of continuous data, such as body mass index, was assessed using the Kolmogorov-Smirnov test. Non-normally distributed continuous data, such as the numeric rating scale and patient satisfaction, were compared using the Mann-Whitney U test. The risk difference and its 95% CI were calculated according to the protocol given by Altman et al.18 P<0.05 was considered significant. Data were analyzed using MedCalc (V.11.3.3.0; MedCalc Software, Ostend, Belgium) and the Statistical Package for the Social Sciences (SPSS V.21.0, IBM SPSS Statistics; IBM).
Based on the previous data at our institution, the first-pass success rate using the CLO view at 60°±5° was 80%.9 We assumed the first-pass success rate using the conventional LAT view to be 50%. With a two-sided 80% power and a 5% significance level, a minimum of 39 patients per group were needed. Considering a dropout rate of 5%, we included 42 patients in each group.
Results
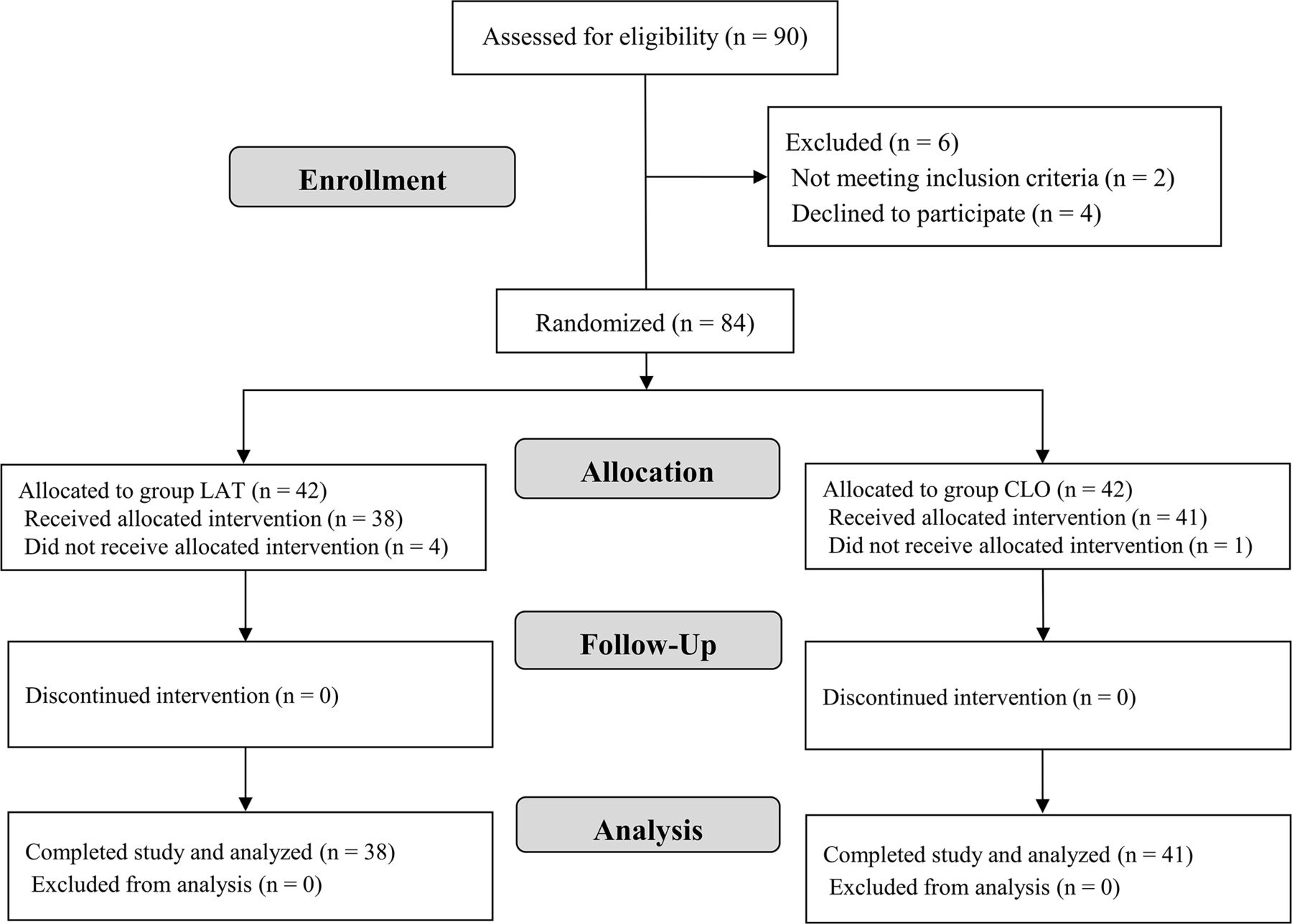
Among the 90 eligible patients, two patients aged >80 years were excluded, and four patients declined to participate in the study. Subsequently, 84 patients were randomized into the allocated groups. After randomization, four patients (two patients: procedure cancellation, one patient: not visiting on the scheduled date, one patient: symptom improvement) in the LAT group and one patient (not visiting on the scheduled date) in the CLO group did not receive the allocated intervention. In total, 79 patients (38 in the LAT group and 41 in the CLO group) were finally analyzed (figure 3).

Consolidated Standards of Reporting Trials (CONSORT) flow diagram of patients included in the study. Lateral (LAT) group comprised patients who underwent mid-thoracic epidural access under the fluoroscopic LAT view. Contralateral oblique (CLO) group comprised patients who underwent mid-thoracic epidural access under the fluoroscopic CLO view.
Clinical characteristics of the patients were not different between both groups (table 1). The most common cause of mid-TEA was the purpose of patient-controlled analgesia. Thus, thoracic epidural catheter placement was the most common intervention. Furthermore, the interlaminar spaces of T7–T8 were the sites where the mid-TEA was most frequently conducted.
Clinical characteristics of the study participants
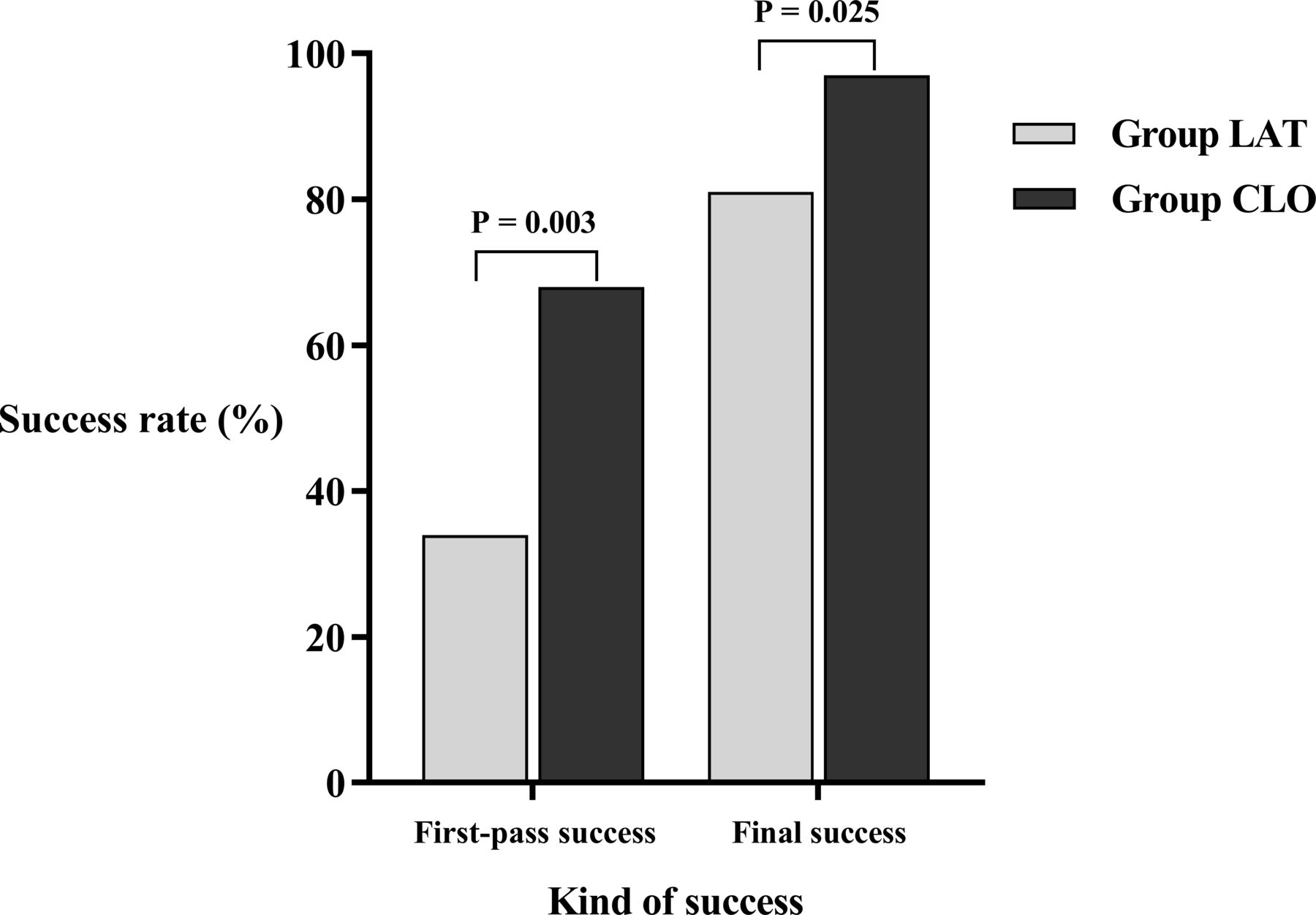
The first-pass success rate was significantly higher in the CLO group than in the LAT group (68.3% vs 34.2%, difference: 34.1%; 95% CI 13.3 to 54.8; p=0.003; figure 4). Mid-TEA was successfully achieved in the CLO group except for one patient. The final success rate was significantly higher in the CLO group than in the LAT group (97.6% vs 81.6%, difference: 16.0%; 95% CI 2.8 to 29.2; p=0.025; figure 4). Procedural pain intensity (numeric rating scale) scores were significantly lower in the CLO group than in the LAT group (2.0 vs 3.3, difference: 1.3%; 95% CI 0.6 to 1.9; p=0.002). Patient satisfaction (global perceived effects) was significantly greater in the CLO group than in the LAT group (6.2 vs 5.0, difference: 1.2%; 95% CI 0.6 to 1.7; p<0.001). The other procedural variables during mid-TEA are shown in table 2. The needling time and number of needle passes were significantly lower in the CLO group compared with the LAT group (95.0 (84.0–142.0) vs 123.0 (107.0–296.0) s, p=0.011; 1.0 (1.0–3.0) vs 2.5 (1.0–5.0), p=0.003, respectively; table 2). The number of skin punctures did not differ between the two groups (p=0.293). Cross-over trials were lower in the CLO group than in the LAT group (2.4% vs 18.4%, p=0.025), and all cross-over trials were completed successfully. The needle tips which were located on the reference line (grade 0) were significantly more frequently seen in the CLO group compared with the LAT view (67.5% vs 9.7%, p<0.001). The distance from the skin to the epidural space identified by LOR was not significantly different between the groups (5.8±0.8 vs 5.6±0.5 cm, p=0.308). Cumulative total radiation dose in the CLO group was also significantly lower than that in the LAT group (59.3±35.0 vs 88.5±71.2 cGy×cm2, p=0.026). One case of the vasovagal reaction occurred in the CLO group, although there were no serious complications in both groups.
Procedural variables during the mid-thoracic epidural access

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of the success rate of first-pass success and final success between the two groups. Lateral (LAT) group comprised patients who underwent mid-thoracic epidural access under the fluoroscopic LAT view. Contralateral oblique (CLO) group comprised patients who underwent mid-thoracic epidural access under the fluoroscopic CLO view.
Discussion
This randomized controlled study is the first to measure the clinical utilities of the fluoroscopic CLO view at 60°±5° in the mid-TEA; the CLO view increased the first-pass and final success rates of mid-TEA under fluoroscopic guidance. Additionally, the CLO view at 60°±5° significantly decreased the needling time and number of needle passes necessary to successfully achieve mid-TEA. These advantages of the CLO view reduced procedural pain, increased patient satisfaction, and decreased total cumulative radiation dose during the mid-TEA.
The thoracic region is the most difficult area to approach the epidural space compared with the cervical or lumbar region.19 20 Although fluoroscopic-guided TEA has several advantages over the landmark approach, mid-TEA remains technically challenging.6 21 The fluoroscopic anteroposterior view and LAT view cannot exactly identify the depth of the needle tip related to the epidural space and discriminate between true and false LOR.22 According to our previous study about mid-TEA, the visualization of needle tips and laminar margins was poor on the LAT view at the mid-thoracic region.9
Although the anteroposterior view and LAT view are widely used as standard practice, recent attention has been directed towards using the CLO view for identifying the needle depth during the fluoroscopic-guided interlaminar epidural access.23 The CLO view appears to be a feasible alternative to the traditional fluoroscopic views for epidural access.4 7 24 Through scientific geometric analyses of the CLO view, Gill et al suggested that fluoroscopic CLO views at 50° and 45° were proper in the cervical and lumbar regions, respectively, to improve needle tip visualization and provide a consistent landmark when accessing the epidural space.4 7 Furthermore, our previous study demonstrated that the fluoroscopic CLO view at 60° may be optimal for mid-TEA; it can provide clear visualization of the needle tip and laminar margin in the mid-thoracic region.9 These properties of the CLO view can make the needle tip avoid the lamina without periosteal contacts, achieving a higher first-pass success rate (68.3%) and improving the accuracy (97.6%) of the fluoroscopic-guided mid-TEA in the present study. Furthermore, it may lead to a decreased needling time, pain intensity, radiation exposure, and increased patient satisfaction in the present results. Despite the needling time being approximately 2 min in our study, it can be much longer, especially for trainees and novices. Thus, the CLO view can be more advantageous in reducing the needling time for beginners, who are not proficient in actual clinical practice. In the previous study, 63.3% of cases presented with poorly visualized needle tips, and 23.3% of cases with poorly or not visualized laminar margin at the LAT view under fluoroscopy.9 This could result in a difficult TEA and be associated with a lower first-pass success rate (34.2%) in the present study.
The catastrophic risks with the fluoroscopic-guided spine interventions in the cervicothoracic region are intrathecal or intramedullary injection.23 This could occur through a false-negative LOR and inappropriate ventral needle advancement. Therefore, for secure mid-TEA using the fluoroscopic CLO view, some safety rules are recommended. First, the LOR portion of the procedure must begin vicinity but not through the VILL. Second, a contrast medium should be administered if the LOR is not obtained despite the needle tip being rather deeply located beyond the VILL because of the need to exclude false-negative LOR. Third, when a needle tip is deeply located on the CLO view, the physician should check the needle tip location on the anteroposterior view. If the needle tip crosses over the midline and is located on the contralateral side, the tip will be deeply located beyond the VILL on the fluoroscopic CLO view for geometric reasons.5 Consequently, the physician should keep in mind that deep needle tip location could cause serious neurological complications and thus should carefully access the epidural space to achieve procedural safety.
There are some limitations to the present study. First, the sample size was relatively small to evaluate the safety and complications related to the procedure. Although no serious complications were noted in this study, the interpretation of the fluoroscopic CLO view safety should be cautiously approached until the evaluation for complications with proper sample size is studied. Second, the LAT group showed a high failure rate (18.4%) compared with the previously reported failure rate under fluoroscopic guidance (1%–2%).13 25 This inconsistency may be explained by the limited epidural access attempts and restricted interventional field (mid-thoracic region) in the present study protocol. Third, the procedure results may vary depending on the individual characteristics and skills of the physicians. However, this study was performed by two physicians with more than 7 years of proficient experience in performing mid-TEA in both fluoroscopic views. To reduce bias, all physicians performed the procedure using both the fluoroscopic views 3 months before beginning the study. Moreover, possible confounding factors, such as the available fluoroscopy technician and equipment, were identical for both physicians. Nevertheless, external validation is required. Fourth, the indications for TEA in this study were heterogeneous and included both acute and chronic pain conditions. Additionally, considering that patients who received patient-controlled epidural analgesia for acute postsurgical pain formed the largest proportion, the findings may not necessarily apply to a special population with difficult anatomy (eg, scoliosis or degenerative thoracic spine). Fifth, although there were no adverse events related to tilting the table, and patients did not complain of anxiety in this study, the use of table tilting might be limited as regards securing patient safety and preventing an increase in patient anxiety. To address this issue, patients could be placed in the semilateral position with a pillow under the abdomen and thorax, or they could be positioned in the opposite direction with their head facing the caudal direction. Finally, other anteroposterior approaches such as the caudal angle approach and different entry points could change our findings to some extent; therefore, further studies with different anteroposterior approaches are required.
Conclusion
The fluoroscopic CLO view at 60°±5° can increase the success rate and patient satisfaction, reduce the procedural time and patient discomfort, and provide the possibility of ensured safety compared with the LAT view when performing mid-TEA. Therefore, we recommend that the CLO view at 60°±5° can be considered as the proper view for achieving successful mid-TEA under fluoroscopic guidance.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Asan Medical Center Institutional Review Board (2020-0535). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
D-HK and H-JK are joint first authors.
Presented at This work was presented at the 71st Annual Meeting of the Korean Pain Society in Daejeon, Korea, 22 May 2021. This work was presented in part as D-HK’s PhD thesis at the University of Ulsan College of Medicine (2021).
Contributors D-HK: conception, design and conduct of the study; analysis and interpretation of data; reporting; writing—original draft preparation. H-JK: conception, design and conduct of the study; interpretation of data; writing—review and editing of the manuscript. BJ and DL: data curation and acquisition. J-WS: planning, conception and design of the study; supervision; project administration. S-SC: planning, conception, design and conduct of the study; writing—review and editing of the manuscript; supervision; project administration. All authors critically revised the manuscript. All authors approved the final version of the manuscript. S-SC (guarantor) accepts full responsibility for the finished work and/or the conduct of the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.