Article Text

Abstract
Background and objectives Cervical plexus blocks are commonly used to facilitate carotid endarterectomy (CEA) in the awake patient. These blocks can be divided into superficial, intermediate, and deep blocks by their relation to the fasciae of the neck. We hypothesized that the depth of block would have a significant impact on phrenic nerve blockade and consequently hemi-diaphragmatic motion.
Methods We enrolled 45 patients in an observer blinded randomized controlled trial, scheduled for elective, awake CEA. Patients received either deep, intermediate, or superficial cervical plexus blocks, using 20 mL of 0.5% ropivacaine mixed with an MRI contrast agent. Before and after placement of the block, transabdominal ultrasound measurements of diaphragmatic movement were performed. Patients underwent MRI of the neck to evaluate spread of the injectate, as well as lung function measurements. The primary outcome was ipsilateral difference of hemi-diaphragmatic motion during forced inspiration between study groups.
Results Postoperatively, forced inspiration movement of the ipsilateral diaphragm (4.34±1.06, 3.86±1.24, 2.04±1.20 (mean in cm±SD for superficial, intermediate and deep, respectively)) was statistically different between block groups (p<0.001). Differences were also seen during normal inspiration. Lung function, oxygen saturation, complication rates, and patient satisfaction did not differ. MRI studies indicated pronounced permeation across the superficial fascia, but nevertheless easily distinguishable spread of injectate within the targeted compartments.
Conclusions We studied the characteristics and side effects of cervical plexus blocks by depth of injection. Diaphragmatic dysfunction was most pronounced in the deep cervical plexus block group.
Trial registration number EudraCT 2017-001300-30.
- regional anesthesia
- nerve block
- multimodal imaging
Data availability statement
Data are available upon reasonable request. Study protocols and raw data are available upon reasonable request from the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Introduction
The cervical plexus is located laterally of the transverse cervical processes beneath the sternocleidomastoid muscle. Its main sensory branches penetrate the deep prevertebral and superficial fasciae of the neck, the latter at a common nerve point known as Erb’s point at the dorsal border of the sternocleidomastoid muscle. Its muscular branches supply innervation to the infrahyoid muscles, the anterior and middle scalenes as well as the diaphragm via the phrenic nerve.1
Cervical plexus blocks have been widely used to facilitate various procedures such as carotid endarterectomy (CEA), auricular, clavicular, or thyroid surgery. Different techniques and levels of depths for these blocks have been proposed and can be roughly divided into superficial, intermediate, and deep cervical plexus blocks.2 3 In general it is thought that the relation of the block to the superficial fascia marks the border between superficial and intermediate block, while the deep prevertebral fascia delineates the intermediate and deep block (figure 1). These relations can either be visualized by ultrasound or determined by resistance (intermediate) or after contact with bone, that is, the transverse process (deep). Anatomical and functional details concerning ideal spread and potential permeation of fasciae in the cervical tissue are still largely unknown,4 but might explain similar reported efficacy of these blocks at different levels of injection.5 Deeper infiltration of the cervical plexus has been repeatedly linked to higher complication rates,6 phrenic nerve blockade,7 and wider craniocaudal spread,8 but is still widely performed. The postero-lateral approach to the deep block may be even more dangerous regarding its orientation towards the vertebral arteries.9
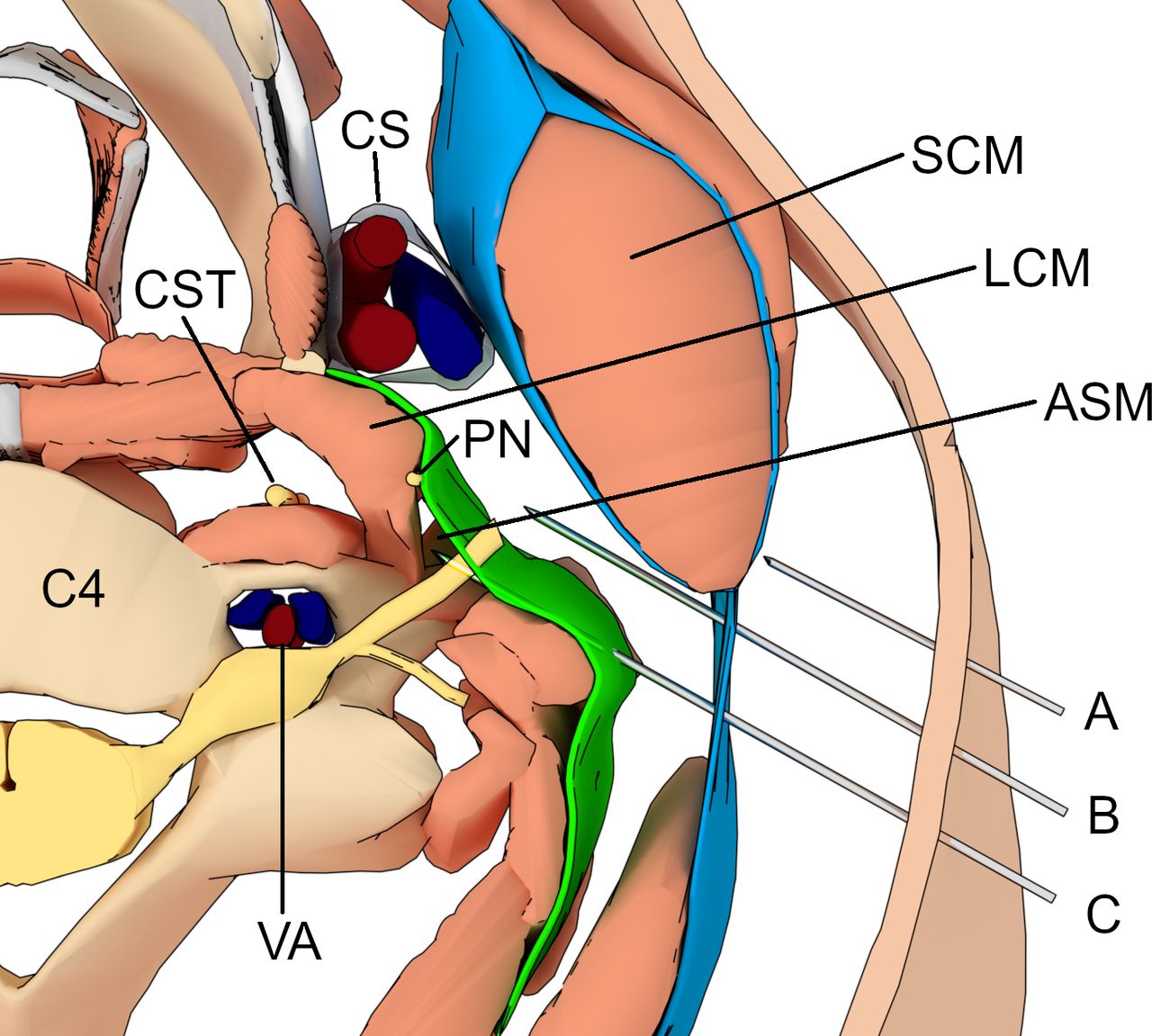
Artistic representation of needle positions for superficial (A), intermediate (B), and deep (C) cervical plexus block at the fourth cervical vertebra (C4). Major structures of interest are labeled: the carotid sheath (CS) encompassing internal and external carotid artery and internal jugular vein; phrenic nerve (PN), cervical sympathetic trunk (CST), longus colli muscle (LCM), anterior scalene muscle (ASM), sternocleidomastoid muscle (SCM), and the vertebral artery (VA). The fascial layers of the neck are colored blue (superficial) and green (deep).
In previous studies, we focused on ideal concentrations of local anesthetics for brachial and cervical plexus blockade and observed hints of substantial phrenic nerve blockade.10 11 Other authors have linked respiratory impairment to tissue distribution of the local anesthetic.12 Therefore, we aimed to study the involvement of the phrenic nerve when comparing these different depths of cervical plexus block. We hypothesized that the depth of block, due to spread within the vertebral fasciae and therefore anatomical vicinity, could have a significant impact on the blockade of the phrenic nerve and consequently hemi-diaphragmatic motion measured by a standardized ultrasound method.13 As all depths of block have been described as feasible methods to achieve sufficient perioperative anesthesia we further hypothesized possible spread of injectate across the fasciae of the neck. We aimed to visualize the spread of the injectate in-vivo by performing contrast agent enhanced MRI after each block.
Methods
Study design
The study is a prospective, randomized, and observer blinded study. We aimed to assess whether unilateral diaphragmatic excursion was affected by the type of cervical plexus block performed. Our primary outcome metric is the difference in ipsilateral diaphragmatic movement (measured in cm during forced inspiration) between our study groups.
It was registered as a clinical trial with the European Medicine agency on August 17, 2017 (https://www.clinicaltrialsregister.eu/ctr-search/trial/2017-001300-30/AT) before start of enrollment on October 4, 2017 and yearly development safety update reports were filed. A mandatory insurance coverage was arranged for all patients included in the study. We adhered to the Consolidated Standards of Reporting Trials (CONSORT) guidelines in reporting this study.
Enrollment
We prospectively enrolled 45 patients scheduled for elective, awake CEA with regional anesthesia. Inclusion criteria were defined as all planned, elective endarterectomies for symptomatic or asymptomatic stenosis of the extra-cranial internal carotid artery under regional anesthesia. Exclusion criteria were: age under 18 years, patients unable to consent, pregnancy, lactation period, contraindications for MRI study and/or contrast agent, implants or incorporated material, for example, cardiac pacemakers, prohibiting MRI study, claustrophobia, inability to remain inside of an MRI due to physical restriction, kidney impairment (glomerular filtration rate below 30 mL/min), liver failure (Child-Pugh class greater A), contraindications to regional anesthesia and/or study medication, severe lung dysfunction (prohibiting supine positioning or chronic obstructive pulmonary disease ≥ GOLD IV), language or communications barrier prohibiting surgery under regional anesthesia.
These patients were randomly assigned to receive either deep, intermediate, or superficial cervical plexus blocks by a computer-generated list. This information was prepared in sealed opaque envelopes and only opened by the anesthesiologist performing the block. Patients, observers, and statisticians remained blinded to the method until after completion of analysis.
Regional anesthesia
Before block placement in the MRI scanner anteroom all patients were routinely monitored via continuous pulse oximetry, ECG, and non-invasive blood pressure measurements. Bilateral hemi-diaphragmatic motion was assessed during normal inspiration and forced inspiration by two otherwise blinded observers (AK, MO) using M-mode on the SonoSite X-Porte and a 5–2 MHz curvilinear probe (Fujifilm SonoSite, USA). This technique has been previously validated and reported to demonstrate good reproducibility.13
Lung function that is, forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC), was assessed in a half-sitting position by a spirometer (EasyOne Spirometer, ndd Medical Technologies, Zurich, CH). Mild sedation was achieved by administering 0.05 mg fentanyl (Fentanyl 0.05 mg/mL, Janssen-Cilag Pharma GmbH, Austria). Arterial cannulation to facilitate invasive blood pressure monitoring during the procedure and the intermediate care unit was performed either in the radial or brachial artery and an arterial blood gas was drawn.
After skin disinfection and sterile draping, all blocks were performed by a single experienced anesthesiologist (JN). In plane visualization of the cannula (SonoTap 22G×80 mm with Facet Tip, Pajunk GmbH, Germany) at the level of the fourth cervical vertebrae (C4) was achieved utilizing a SonoSite X-Porte (Fujifilm SonoSite, USA) with a 15–6 MHz linear probe and the needle advanced from dorsal and lateral of the sternocleidomastoid muscle.
Superficial block was defined as subcutaneous injection above the nerve point of the neck at the dorsal border of the sternocleidomastoid muscle; intermediate block was defined as injection beneath the fascia of the sternocleidomastoid muscle and deep block as injection within 1–2 mm distance of the posterior tubercle of the transverse process. All patients received 20 mL ropivacaine 0.5% (Naropin, AstraZeneca Austria GmbH, Vienna, Austria) mixed with 0.05 mmol of the MRI contrast agent gadopentetate dimeglumine (Dotarem, 0.5 mmol/mL; Guerbet, Villepinte, France).
MRI and surgery
Following block placement magnetic resonance examinations were performed on a Philips Ingenia 1.5 Tesla system (Philips, Best, The Netherlands) using a digital head and anterior coil. After MRI patients were transferred to the holding area, where lung function tests and arterial blood gas samples were repeated. Immediately before surgery, 10 mL of Prilocaine 1% (Xylonest, Aspen Germany GmbH, Munich, Germany) was subcutaneously injected along the presumed line of incision. Standardized CEA techniques were performed with an oblique incision along the medial edge of the sternocleidomastoid muscle to expose the carotid bifurcation. Before arterial clamping 5000 units of unfractionated heparin were administered systemically. The majority of carotid artery lesions were treated with eversion endarterectomy and selective shunting depending on neurological changes of the patients.14 15 In cases with extensive atherosclerotic plaques and high carotid bifurcations conventional endarterectomy with bovine pericardium patch closure was performed at the attending surgeons discretion. Protamine reversal of heparin anticoagulation was not regularly used in this study.16 The amount of supplemental local anesthetic as used by the surgeon, intravenous analgesics, as well as conversion rates to general anesthesia, pain levels, narcotic consumption, complication rates, hemodynamic changes, oxygen saturation, postoperative hoarseness, and paresis of the recurrent laryngeal nerve served as secondary outcome measures. Assessment of the motor function of the recurrent laryngeal nerve that is, function of the vocal cords, was routinely performed via flexible laryngoscopy by an otorhinolaryngologist prior to surgery and on the first postoperative day.
Radiographic analysis
Radiographic analysis was performed independently by two radiologists with extensive experience in MRI analyses (MM and RK). Preliminary results were compared and diverging results jointly reviewed to achieve consensus. Image analysis was blinded to any clinical information and the depth of infiltration was unknown to the radiologists interpreting the images. Intellispace Portal (Philips, Best, The Netherlands) was used to measure infiltration diameters (longitudinal, transverse, craniocaudal) and volume (mL) using manual segmentation. Field of view of the MR examination covered the entire neck region from the level of the foramen magnum down to the first thoracic vertebra. After recording standard survey images, we registered trans-axial T2-weighted images (TR 2500–3500 ms, TE 90, slice thickness 3 mm, FOV 300×250×158) and 3D T1-weighted FFE 1×1 (chemical-shift imaging, Dixon ALL, TR 6.7 ms, TE1 1.9 ms, TE2 4.6 ms, FOV 300×252×158) with multiplanar reformations were prepared. Imaging evaluation included infiltration depth in groups of superficial, intermediate, and deep, passage through Erb’s point, passage through the cervical fascia, vicinity to the phrenic nerve, proximity to the nerve roots C1–C4, diffusion around the carotid artery, location of the carotid bifurcation related to the cervical vertebral bodies and epidural spread.
Statistical analysis
Sample size calculations determined a requirement of 45 patients to detect a 20% difference of diaphragmatic movement during forced inspiration as measured by transabdominal sonography in cm (mean 4.66 cm, SD 0.87 cm, power 80%, accepting an alpha of 5%) in 3 groups of 15 patients for each depth of block. Data were screened and cleaned for incomplete, incorrect, and missing data. Continuous normally distributed variables (height, weight, mean surgery and clamping time, fentanyl, supplemental local anesthetic, diaphragmatic motion, FEV1, FVC, peripheral oxygen saturation, supplemental oxygen, local anesthetic spread, and volume) were analyzed across the groups by analysis of variance (ANOVA), non-normally distributed continuous variables (age) by Kruskal-Wallis test. Pearson’s χ2 tests was used to analyze categorical parameters (ie, American Society of Anesthesiologists score, height of carotid bifurcation, paresis of recurrent nerve, postoperative hoarseness, sex, bradycardia, tachycardia, hypertension, hypotension, shunting, conversion to general anesthesia, Visual Analogue Scale score, patient satisfaction, neurological complications, vicinity to phrenic nerve, proximity to nerve roots, circumferential spread around carotid artery). Pairwise comparisons were performed after ANOVA with Fisher’s least significant difference (LSD) test as post hoc test for the primary outcome metric and where crosstabulation analysis reached statistical significance. FEV1 and FVC were further analyzed by repeated measures ANOVA with superficial, intermediate, and deep block as group variable and time as repeated factor and corresponding LSD tests as post hoc tests. Data were analyzed using STATA/IC V.12.1 for Windows (Stata Corp) and PASW 24 (IBM SPSS Statistics for Windows, V.21.0).
Results
The CONSORT flowchart of this study is represented in figure 2. All 45 enrolled patients completed the study protocol, and no data were lost during analysis. Table 1 summarizes patient and intervention characteristics as well as general outcome parameters.
Patient and intervention characteristics and general outcome parameters
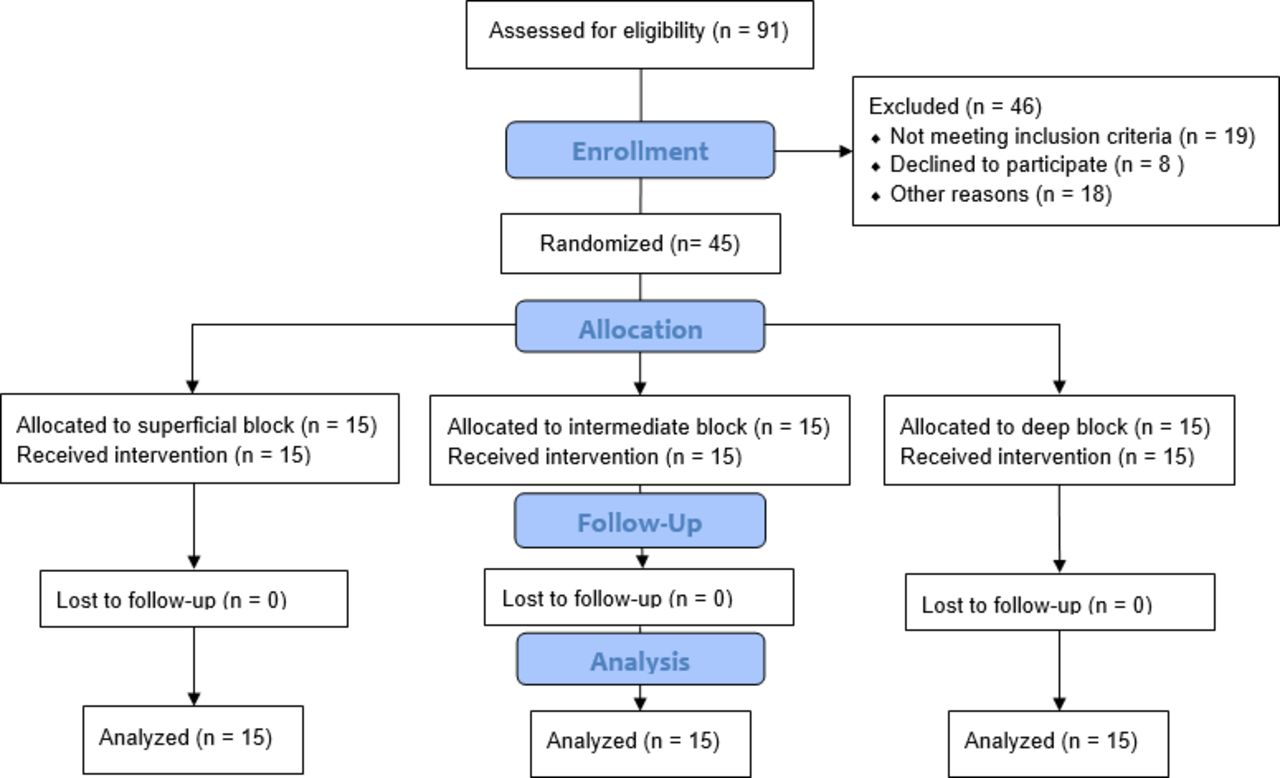
CONSORT flow chart representing enrollment, intervention allocation, follow-up, and data analysis for this study.
Primary outcome measurements
The primary outcome parameter, that is, ipsilateral transabdominal measurements of diaphragmatic movement in centimeter during forced inspiration, did not differ before the block (deep group 4.73±1.00 cm, intermediate group 4.94±1.91 cm and superficial group 5.10±1.29 cm, p=0.78). After block placement we could detect a marked difference of ipsilateral diaphragmatic movement during forced inspiration between the study groups (deep group 2.04±1.20 cm, intermediate group 3.86±1.24 and superficial group 4.34±1.06 cm, p<0.001). Post hoc analysis demonstrated a mean difference of −1.82 cm (95% CI −2.79 to –0.85, p<00.1) between deep vs intermediate block, −2.30 cm (95% CI −3.27 to –1.33, p<0.01 between deep vs superficial block and −0.48 cm (95% CI −1.45 to 0.50, p=0.33) between intermediate versus superficial block.
Secondary outcome measurements
Similarly, to our primary outcome metric, ipsilateral hemi-diaphragmatic movement during normal inspiration did not differ before block placement (1.79±0.75 cm, 2.00±0.72 cm, and 1.84±0.44 cm, for deep, intermediate, and superficial groups, respectively, p=0.66) and showed a significant difference after block placement (1.00±0.93 cm, 1.60±0.75 cm, and 1.62±0.50 cm, for deep, intermediate, and superficial groups, respectively, p=0.047). Contralateral and baseline measurements were included to detect possible changes on diaphragmatic movement after surgery not attributed to regional anesthetic technique. No statistically significant differences between the study groups could be demonstrated in these measurements, except for a probably compensatory contralateral increase of hemi-diaphragmatic movement in the deep, forced inspiration group. Figure 3 summarizes the primary outcome parameters for normal and forced inspiration, while figure 4 demonstrates typical changes in ipsilateral diaphragmatic movement as measured by ultrasound.

Plot of mean diaphragmatic movement for normal and forced inspiration. Results on y-axis in centimeter as measured by transabdominal ultrasound (mean, 95% CI) for normal and forced inspiration as well as corresponding ipsilateral and contralateral measurements.
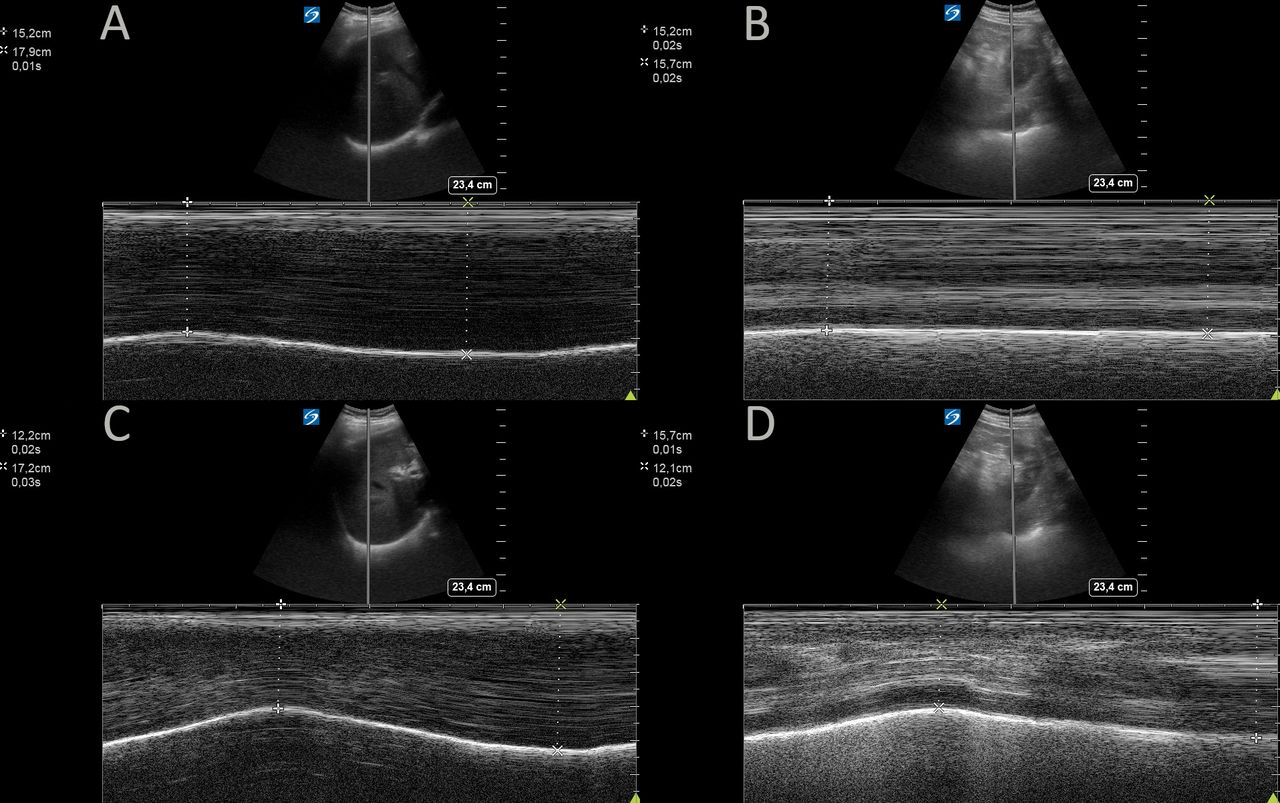
Transabdominal B-mode ultrasound measurement of diaphragmatic movement after left-sided deep cervical plexus blockade. B-mode ultrasound images of normal contralateral (ie, right) diaphragmatic movement visualized through the liver, during normal (A), and forced inspiration (B) versus ipsilateral (ie, left), diaphragmatic movement visualized through the spleen, during normal (C), and forced inspiration (D) demonstrating phrenic nerve blockade.
A higher incidence of postoperative hoarseness (over half the patients at 53%) was observed in the deep cervical plexus block group (p=0.04), but no pairwise significant difference was found (all Fisher’s exact tests, p>0.05). We could not detect a difference in postoperative paresis of the recurrent laryngeal nerve. Lung function parameters and radiographic results are summarized in table 2.
Lung function and radiographic results
In post hoc analysis FEV1 did differ after block versus before block by 0.46 L (95% CI 0.22 to 0.70, p<0.001) in the deep block but not the other groups. Similarly, FVC did only differ to before block placement in the deep block group by 0.66 L (95% CI 0.38 to 0.93, p<0.001) but not the other groups.
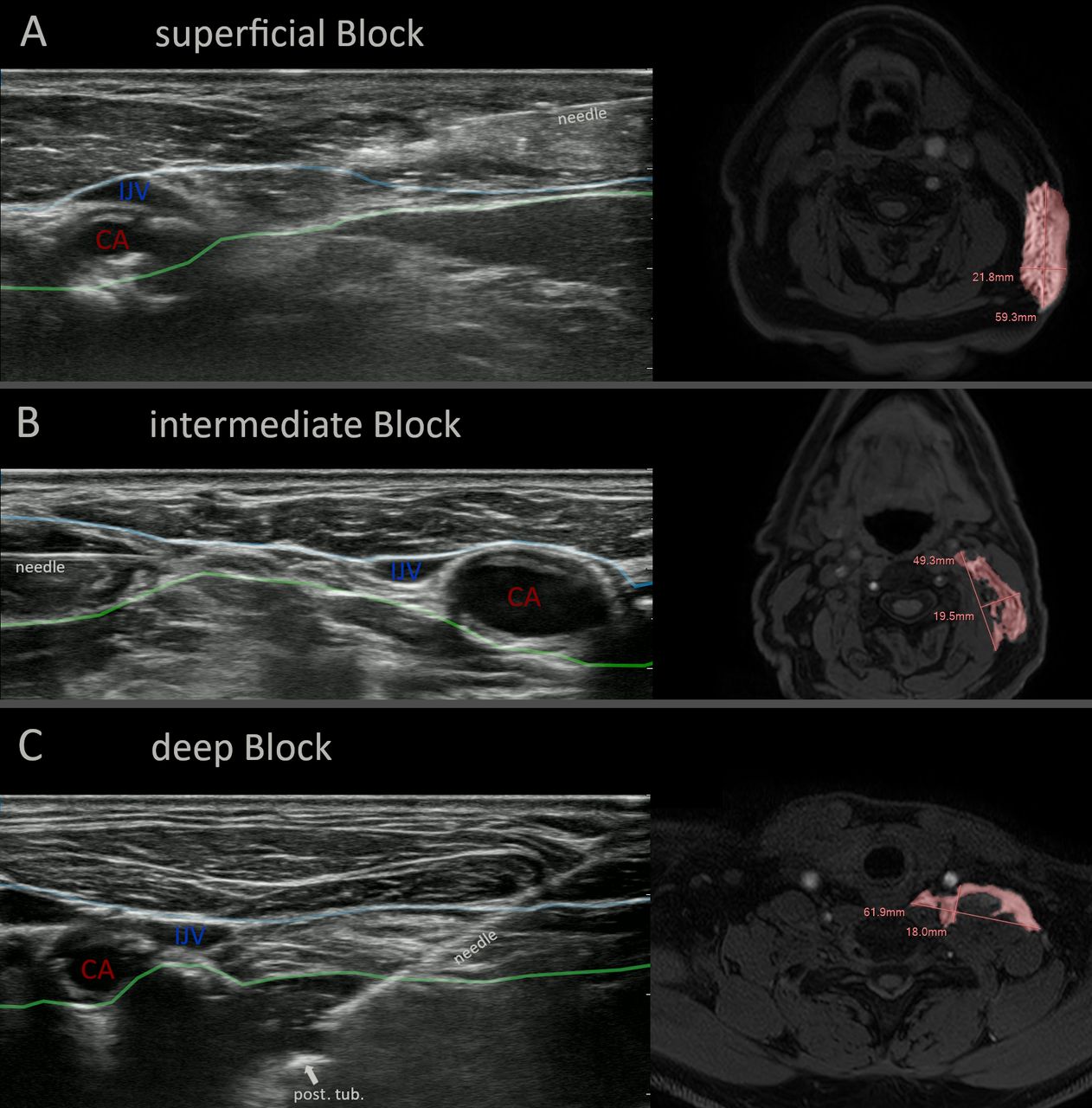
All patients of the superficial group were correctly identified by the radiologists, while four patients were misassigned between the deep and intermediate groups. We could demonstrate a spread of the injectate through the nerve point of the neck in 13 (87%) of superficial blocks. Contrast agent could be visualized below the superficial fascia of the neck in all superficial and intermediate blocks, but none below the deep fascia, while in 14 (93%) of deep blocks contrast agent could be correctly visualized below the deep fascia. Measurements of the longitudinal and transverse diameters demonstrated similar spread, while craniocaudal extent was significantly higher in the intermediate and deep block groups (p<0.01). While functional analysis of the phrenic nerve function, that is, diaphragmatic movement, did not demonstrate a marked decrease in the intermediate block group, radiographic analysis did suggest a vicinity to the phrenic nerve for this group in 14 (93%) of patients. Figure 5 visualizes ultrasound imaging at the time of injection corresponding to acquired MRIs for each study group.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ultrasound imaging at time of injection corresponding to acquired MRIs for each study group. Representative images of superficial (A), intermediate (B) and deep (C) cervical plexus blocks using ultrasound at time of injection (left) and MRI with contrast dye enhancement after injection (right). Blue line represent superficial fascia of the neck and green line represent deep fascia of the neck.CA, carotid artery; IJV, internal jugular vein; post. tub., posterior tubercle of the transverse process of the fourth cervical vertebrae.
Discussion
In this randomized controlled trial, we demonstrated that the depth of cervical plexus block has an impact on the blockade of the phrenic nerve and consequently hemi-diaphragmatic motion. Our study identified more pronounced hemi-diaphragmatic dysfunction after deep cervical plexus block.
This study is the first to explore the relationship between cervical block type and diaphragmatic dysfunction. Although we detected a difference in normal and forced inspiratory diaphragmatic movement, this did not result in significant differences in perioperative lung function between the groups. The observed differences of FEV1 and FVC before and after block in the deep block group may not necessarily be clinically significant. In our population, which excluded patients with severe lung dysfunctions prohibiting prone positioning, we encountered no respiratory complications.
The detailed MRI analysis was novel in that we could observe spread of the local anesthetic injectate in vivo. We could repeatedly demonstrate permeation of the superficial fascia at the point of Erb, even though care was taken to keep injections strictly subcutaneously. This might explain the comparable anesthetic effects of all three block characteristics, with the superficial injection spreading into the intermediate level following the nerve fibers, as has been suggested by previous studies.4 5 Although injection at the intermediate level demonstrated a similar anatomical vicinity to the phrenic nerve as the deep block, its effects were considerably less pronounced. We believe that the location of the phrenic nerve, typically situated ventral of the anterior scalene but beneath the deep prevertebral fascia, may account for this. This would indicate an impediment to diffusion across the deep fascia at this location. Surprisingly only in about half of deep blocks did the injectate reach the nerve roots between C1 and C4. Furthermore, craniocaudal spread was highest at deeper infiltration points, a finding that has been confirmed in earlier case series.8 This perhaps resulted in a more complete blockade compared with the blockade of singular rami at the intermediate level with less pronounced craniocaudal spread. This does not only raise questions concerning the ideal concentration,10 but also volume at this level of block. We deliberately chose the same, although large volume of 20 mL per site of injection, but volume finding studies still need to be performed.
Our study is limited by the possibility that diffusion of the local anesthetic itself might differ from the contrast agent. Strid et al used Dotarem to investigate local anesthetic spread and seemed to confirm diffusion of Dotarem through membranous fasciae, even into the epidural space.17 Dotarem possesses an essentially neutral pH (6–8) in a water-based solution, therefore not interfering with ropivacaine’s capability to diffuse through lipophile membranes. We are confident that this study adds substantial knowledge concerning the spread of local anesthetic solutions, be it by hydrostatic pressure or diffusion through extracellular space. We recorded a higher need of supplemental local anesthetic in the superficial group, but due to cumulative reporting by the surgeon, we cannot attest to the level of depth at which these injections occurred. Further studies might elucidate the role of carotid bifurcation height on block success, as in our practice this, as well as surgical retraction at the gonial angle of the mandible, necessitates frequent supplemental local anesthetic injections.
Another possible, but deliberate weakness of our study, was the delay of sequential measurements of diaphragmatic movement until after surgery. We chose this approach to guarantee block success, full effect on possible neural pathways, and to minimize the further delay of surgery. Care was taken to maintain the same anesthesiologist performing preoperative and postoperative measurements, as well as patient positioning, but residual effects of surgery or sedation may not be discounted. The inclusion of baseline and contralateral measurements did mitigate some possible bias, as we could detect significant differences between the study groups even when changes to the contralateral side and preoperative to postoperative differences were accounted for in post hoc analyses. As our study was severely underpowered to study complication rates, we are not able to give a recommendation on whether the frequent, unilateral blockade of the phrenic nerve warrants special attention or avoidance of deep cervical plexus blockade in patients with precarious respiratory situations. This might indicate that if adopted as standard of care, regional anesthesia for CEA can be a safe and satisfying method for patients, surgeons, and anesthesiologists, if certain exclusion criteria are observed.
Conclusions
We investigated the impact of depth of cervical plexus block on diaphragmatic movement, with the deep plexus block exhibiting the greatest decrease. The clinical significance of our findings is unclear given the minimal changes in pulmonary function. We observed consistent permeation of the superficial fascia of the neck, suggesting this as a possible cause for similar anesthetic properties. Summarizing radiographic spread, lung function, potential for complications, and block effectiveness, the intermediate block does appear to represent the ideal middle ground. Further studies on optimal local anesthetic volume and anatomical variations are needed.
Data availability statement
Data are available upon reasonable request. Study protocols and raw data are available upon reasonable request from the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and the perineural injection of the contrast agent constituted an off-label use. This was approved by the ethics committee of the county of Salzburg, Austria (reference number 415-E/2174/5-2017) and the Federal Office for Safety in Healthcare, Austria (reference number 1157322). Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Twitter @FKenzm
Correction notice This article has been corrected since it was first published. The open access licence has been updated to CC BY.
Contributors MO and AK contributed to planning, designing, and conducting the study, data analysis, drafting, revising, and submitting the manuscript, MO acts as guarantor. RK and MM contributed to designing and conducting the study, data analysis, and drafting the manuscript. FKE and CD contributed to conducting the study, drafting, and revising the manuscript. WH contributed to data analysis, drafting, and revising the manuscript. JN contributed to planning and conducting the study, revising the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.