Article Text

Statistics from Altmetric.com
Introduction
Lumbar medial branch blocks (LMBBs) are a prognostic tool for lumbar medial branch radiofrequency ablation (LMBRFA). The number of blocks and percent pain relief necessary for progression to LMBRFA are debated. Consensus practice guidelines have made a clinical practice recommendation that ≥50% pain relief following an LMBB serve as the threshold for a positive prognostic block for progression to LMBRFA.1 Previous research has demonstrated variable results in LMBRFA outcomes with utilization of higher LMBB pain relief thresholds exceeding 50%. For example, Cohen et al 2 found no significant difference in LMBRFA outcomes on any LMBB pain relief threshold above 50%. Even in studies that have reported better outcomes with higher cutoffs, the results indicate that using higher cutoffs would result in a substantial proportion of LMBRFA responders being denied treatment.3 However, as of March 2021, Medicare Administrative Contractors (MACs) require two preceding LMBBs with ≥80% pain relief before progression to LMBRFA.4 The principal objective of this study was to understand the influence of the second block on progression to LMBRFA under pain relief thresholds of either 50% (ie, ≥50%) or 80% (ie, ≥80%). Secondary objectives were to determine the potential impact of the new MAC requirements on LMBRFA utilization and the associated economic consequences of a second block.
Methods
Following institutional review board approval, a single-center retrospective review was performed on 224 patients with two consecutive local anesthetic-only LMBBs with ≥50% pain relief on the first block from September 2013 to June 2019 in an ambulatory surgical center (ASC). Patient-reported percentage improvement in pain scores were obtained. Data were analyzed using the consensus practice guideline and the MAC coverage determination criteria.
The associated 2022 Medicare ASC and physician fee costs for the one-block and two-block paradigms at the 50% and 80% thresholds for the accompanying bilateral two facet level LMBBs and LMBRFA procedures were calculated.5 The results were then extrapolated to the latest available procedure data (2020) for traditional Medicare beneficiaries to estimate costs for the Medicare population.6
Statistical analyses were performed with Python V.3.6.9.7–9 CIs for proportions used the Clopper-Pearson method.
Results
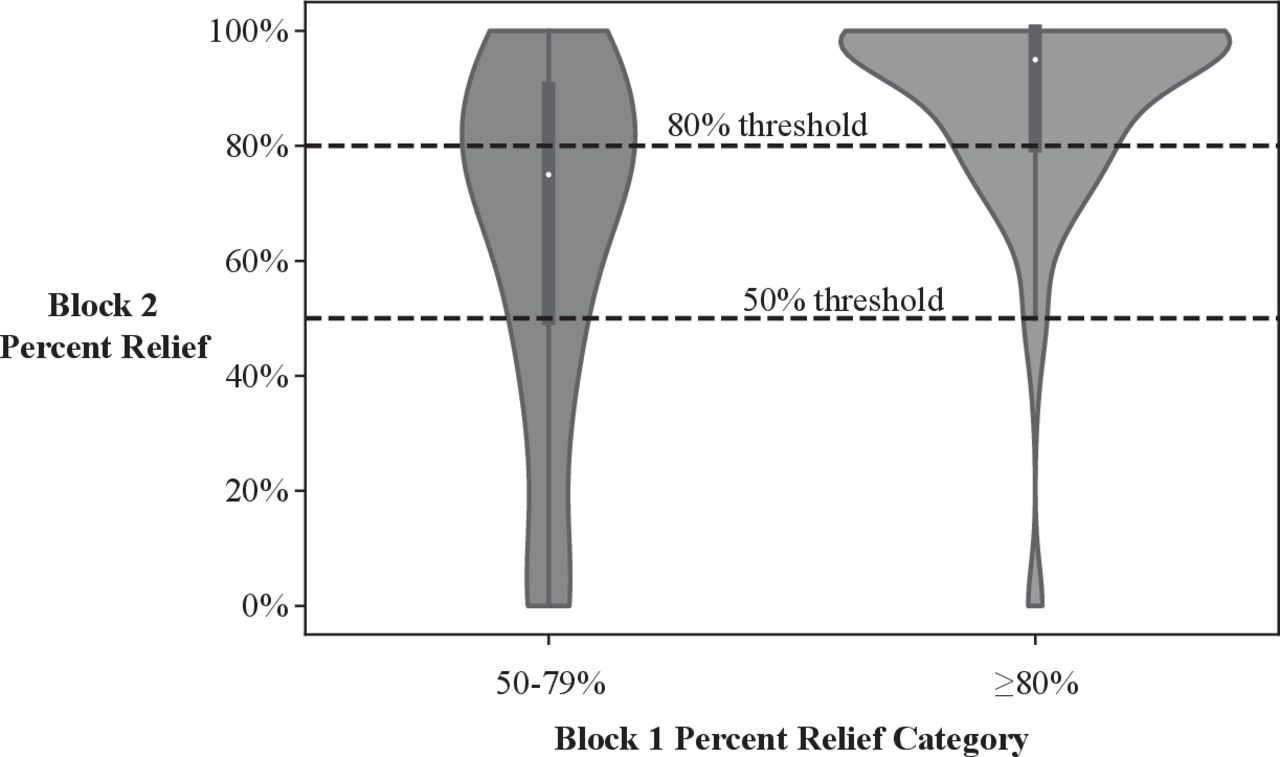
Two hundred and twenty four patients (table 1) had two local anesthetic-only blocks with ≥50% pain relief on the first block. Although percent pain relief on the two blocks was only moderately correlated (Spearman r=0.45; p<0.001), we observed significant differences on block 2 for patients in the different block 1 categories of 50%–79% pain relief and ≥80% pain relief (figure 1).
Demographic information for patients in this study, stratified by percent relief category on the first block. The breakdown of block 2 results into percent relief categories of <50%, 50%–79%, and ≥80%, with 95% CIs for each proportion.

{kind=link}
Violin plots showing the distribution of percent relief on the second block, stratified by relief category on the first block. Silhouette of violin represents smoothed histograms of block 2 percent relief from the 224 patients in the study. Inner boxplots represent the IQR (first quartile, third quartile; thick gray bar) with the median represented by a white dot: 75% (95% CI 70.0 to 80.0) for patients with 50%–79% relief on block 1 and 95% (95% CI 90.0 to 100.0) for patients with ≥80% relief on block 1; and with an effect size of 20% (95% CI 12.0 to 29.0). CIs are based on 10,000 bootstrap samples. Horizontal dotted lines indicate 50% and 80% thresholds.
Most patients achieved the same or better pain relief block category with the second block (table 1 and figure 1). When considering patients with 50%–79% and ≥80% pain relief on block 1, only 22.4% and 18.7% of patients, respectively, fell into a lower category on block 2. Furthermore, when comparing patients who had ≥80% relief versus 50%–79% relief on block 1, the proportion who had ≥50% relief on block 2 was 97.1% (95% CI 92.8 to 99.2) versus 77.6% (95% CI 67.3 to 86.0), respectively, representing a relative risk (RR) of 1.25 (95% CI 1.11 to 1.41). For the same comparison, the proportion who had ≥80% relief on block 2 was 81.3% (95% CI 73.8 to 87.4) versus 43.5% (95% CI 32.8 to 54.7), representing an RR of 1.87 (95% CI 1.45 to 2.41), indicating that an individual with ≥80% relief on block 1 is 87% more likely to achieve that same threshold on block 2 relative to an individual with 50%–79% relief on block 1.
The introduction of the MAC requirements of ≥80% for 2 blocks would result in a 43.8% (95% CI 36.8 to 50.9) LMBRFA procedural volume reduction when compared with the 50% threshold for 2 blocks.
Table 2 depicts the 2022 Medicare costs and associated calculation assumptions for the single- and double-block paradigms at the 50% and 80% thresholds. One-block paradigms for the 50% and 80% thresholds for this study population would result in a 21.8% ($111,599.00) and 15.6% ($57,578.00) cost reduction when compared with their respective 2-block paradigms. When extrapolated to 2020 Medicare initial LMBRFA procedure data, these percentages correspond to $176,768,433.00 and $88,045,374.00 cost savings for the 50% and 80% thresholds, respectively.
Cost analysis of medial branch block paradigms
Cost data are based on 2022 Medicare reimbursement payments, including ASC and physician fees. All cost data were based on two level lumbar bilateral procedures, including LMBBs (current procedural terminology CPT) codes: 64493 and 64494) and lumbar RFA (CPT codes: 64635 and 64636). The total number of initial lumbar RFAs performed in 2020 (most current available date) for traditional Medicare beneficiaries was 307,360.6 Estimates based on the frequency data for this study for the 50% and 80% thresholds were used to calculate the number of Medicare beneficiaries in each threshold category. The estimates were based on performing these procedures in an ASC. Calculations would differ based on reimbursement values for the office and the hospital outpatient department.
Discussion
A second prognostic LMBB could be valuable if it significantly alters patient selection for RFA, but the benefits would have to be weighed against additional healthcare cost, added humanistic burden, and associated second-block procedural risk. In this study, approximately 80% of patients under each selection criteria obtained the same or better category result on the second block. Furthermore, for the study population presented here, a one-block paradigm resulted in a >15% cost reduction. The data presented here can help clinicians, patients, and payers determine whether a second block is worth pursuing in individual cases and brings into question the utility of a mandatory second block. Furthermore, the introduction of the new MAC coverage determination policies would result in an approximate 40% initial LMBRFA procedure volume reduction and the possibility of withholding a beneficial procedure from a substantial number of individuals.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Robert Morris University's institutional review board (201906032098). Design was a single-center retrospective review.
Acknowledgments
We would like to acknowledge Noah Hoffman for his assistance in data collection.
Footnotes
Twitter @DProvenzanoMD, @Zef_Leech
Presented at Presented at American Society of Regional Anesthesia and Pain Medicine 18th Annual Meeting. New Orleans, Louisiana, November 2019. Abstract ID #276.
Correction notice This article has been corrected since it published Online First. Typographical errors in the table 1 heading have been corrected.
Contributors DAP and JEL were involved with study inception, data collection, data analysis, and manuscript preparation. JSK was involved with study inception, data analysis, and manuscript preparation. LAS was involved in data analysis and manuscript preparation. All authors approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.