Article Text

Abstract
Introduction Erector spinae plane block has been proposed to reduce opioid use and improve pain relief with controversial results. This randomized clinical study aimed to assess the efficacy of erector spinae plane block in major spine surgery including multimodal and ‘Enhance Recovery After Surgery’ programs.
Method After institutional review board approval, adult patients undergoing elective lumbar spine surgery with standardized general anesthesia, rehabilitation and multimodal analgesia protocols were randomly allocated to receive bilateral ultrasound-guided block with saline versus ropivacaine (3.75 mg/mL). Before surgery, a bilateral erector spinae plane block was performed at lumbar level (third vertebrae) with 20 mL of solution for each side. The primary outcome was morphine consumption after 24 hours. Secondary outcomes included pain scores and side effects, from postanesthesia care unit to discharge, and questionnaires at 3 months on pain and quality of life (EQ-5D).
Results From November 2019 to July 2021, 50 patients were enrolled with similar characteristics and surgery for each group. After the first 24 hours, there was no statistical difference regarding cumulative intravenous morphine consumption between ropivacaine and saline groups: 7.3 mg (3.7–19) vs 12.5 mg (3.5–26) (p=0.51). Over the five postoperative days, opioid sparing, pain scores and side effects were similar between groups. At 3 months, pain relief, incidence of chronic pain and EQ-5D were similar between groups.
Discussion Erector spinae plane block used in conjunction with ‘Enhance Recovery After Surgery’ and multimodal analgesia protocols provides limited reduction in opioid consumption and no long-term benefits.
Trial registration number EudraCT 2019-001678-26.
- analgesia
- anesthesia, local
- analgesics, opioid
- pain, postoperative
Data availability statement
Data are available on reasonable request.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Erector spinae plane block for lumbar spine surgery remains debated regarding pain relief and opioid sparing when combined with ‘Enhance Recovery After Surgery (ERAS)’ programs and multiple drug therapies during the first two to three postoperative days.
WHAT THIS STUDY ADDS
This randomized trial demonstrated that, in conjunction with the ERAS programs, erector spinae plane block (ESPB) provides limited reduction in intravenous opioid consumption (<5 mg vs placebo) and no long-term benefits (chronic pain, quality of life).
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Systematically performing an ESPB is unjustified and should be analyzed on a case-to-case basis according to the perioperative protocol.
Introduction
The number of annual spine surgery procedures worldwide has increased dramatically per year over the period 1999–2017, making spine surgery one of the fastest-growing categories of surgical procedure.1 2 Most of these procedures involve patients with intermediate to severe mechanical and neuropathic pain and psychological frailty.3 4 Moreover, in a large, observational, multicenter study, spine surgery induced severe postoperative pain and was ranked the second (spinal fusion one to two segments) and third (dorsal spinal fusion, three or more segments) most painful surgical act among 179 procedures.5 In this context, a multimodal analgesic approach has recently been recommended to enhance postoperative rehabilitation and pain relief after spine surgery.6–8
For lumbar spine surgery, various perioperative pharmacological and non-pharmacological interventions have been introduced to improve pain relief and outcomes and reduce the length of hospital stays. To enhance the multimodal approach and opioid sparing, several local anesthesia (LA) administration routes have been evaluated: intravenous, infiltration (wound), regional (paravertebral, epidural and spinal).6–9 Recently, lumbar erector spinae plane blocks (ESPB) have been proposed as an alternative to other regional techniques.9–14 Previous cadaveric, CT scan imaging and randomized studies have inconsistently reported clinical efficacy (Numerical Rating Scale (NRS) pain score, opioid sparing) or effective dye diffusion due to the unpredictable injectate spread.10–14 Furthermore, most studies published include various types of spinal surgery (laminectomy, decompression, fusion, discectomy), different levels of injection (thoracic, lumbar), absence of multimodal analgesia and ‘Enhance Recovery After Surgey’ (ERAS) protocols or short-term evaluation without any analysis of chronic pain.10–19 Moreover, there are no randomized trials on the same levels of surgery.10–19
To assess the benefits of a single ESPB injection, we hypothesized that this technique would provide early opioid sparing, thus improving pain relief and quality of life at 3 months. We performed a prospective randomized study using LA (ropivacaine) versus saline on patients scheduled for major lumbar spinal surgery (>2 segments) as part of the ERAS program (multimodal analgesia protocol).19 The primary end point was opioid consumption at 24 hours. Secondary end points were pain levels, morphine consumption in the early postoperative days, quality of life and the occurrence of neuropathic and chronic pain at 3 months.
Methods
This was a prospective, single-center, randomized controlled, 1:1 allocation, parallel-armed, double-blinded, intention-to-treat superiority trial. The study was conducted at a single French tertiary hospital (Nîmes University Hospital, Carémeau, France). The Consolidated Standards of Reporting Trials recommendations were followed to report the trial. The analysis was made once patient enrollment had been completed.
Study design and patients
Eligible patients were adults >18 years scheduled for major lumbar spinal surgery (posterior surgical approach, >2 segments) under standard general anesthesia combined with multimodal analgesia and an ERAS protocol as described by the Enhanced Recovery Spine Surgery committee (ERSS protocol that has been applied and implemented at our institution since its publication). For non-oncological surgery, the ERSS protocol was adapted as described in the ‘General anesthesia, multimodal analgesia and ERAS protocol’ section.19 Exclusion criteria were: refusal to participate, age >80 years, weight <50 or >120 kg, emergency including fracture, any regional anesthesia or analgesia (including wound infiltration, epidural or spinal injection), cognitive disorders (delirium, dementia), pregnancy (beta-human chorionic gonadotropin test performed systematically for women <45 years), patients with alcohol or drug abuse (questionnaire), uncontrolled epilepsy, patients unlikely to be fully cooperative during the study and those who had participated in another study within the previous 30 days. Patients reporting any allergy or contraindication for the drug under study (ropivacaine, non-steroidal anti-inflammatory drugs (NSAIDs), paracetamol, nefopam, morphine), renal failure (creatinine clearance <50 mL/min, Cockroft formula), liver failure (transaminases and/or alkaline phosphatases >3 times the normal upper value and/or prothrombin time <70% of control) and acute or chronic respiratory insufficiency (SpO2 <94% in ambient air) were not included.
Drug under study, randomization and blinding
Patients were randomly assigned either to the saline group or the ropivacaine group using computer-generated random numbers created by the study statistician on a randomization ratio of 1:1. Group allocations were concealed in sequentially numbered opaque envelopes. Patients were randomized into blocks of six patients per block. The solution (saline, ropivacaine) vials were similar. Drug solutions (40 mL) were prepared using 40 mL of saline solution for the saline group and 150 mg of ropivacaine (3.75 mg/mL) for the ropivacaine group. Patients, surgeons, anesthesia staff, surgical ward staff and investigators were blinded to group assignment until data analysis.
Erector spinae plane block and treatment administration
Bilateral ESPB was performed at L3 level before surgery under general anesthesia in a ventral prone position by experienced practitioners (authors). For each procedure, an ultrasound examination of the lumbar area was performed using a low-frequency linear ultrasound probe (5 MHz, Vivid Q, GE Healthcare, USA) covered with a sterile sheath. Briefly, for all blocks, prescanning in both transverse and longitudinal views was performed to identify bone structures, including spinous processes, laminae, transverse processes and the fascial plane of the lumbar erector spinae muscle. This preview was performed from T8 to L5 spine level. Injection was performed through a 22-gage 80 mm needle (Pajunk Sonoplex, PAJUNK Medizintechnologie, Geisingen, Germany) using an in-plane ultrasound technique with the structures visualized in the sagittal plane. The needle was inserted at level L2 and translated in a cephalad-to-caudal direction to reach the transverse process of L3. The needle tip was translated to be placed with the bevel facing upward to reach the tip of the transverse process. Next, 2 mL of saline solution was injected under ultrasound vision to ensure the diffusion in the fascial plane without intramuscular injection. On each side, 20 mL of blinded solution was injected for a total of 40 mL per patient.
General anesthesia, multimodal analgesia and ERAS protocol
The standardized intraoperative protocol was performed in both groups, including intubation and mechanical ventilation. Induction was performed with intravenous propofol (2–3 mg/kg), cisatracurium (0.6–1 mg/kg), sufentanil (0.25 μg/kg) and maintained with sevoflurane 1%–2% and additional intravenous sufentanil (5 μg) every hour or when variations in mean arterial pressure or heart rate >20% from baseline).
For the postoperative nausea and vomiting (PONV) prevention and analgesia protocol, all patients received intravenously:
After induction: dexamethasone (8 mg), ketamine (0.5 mg/kg).
At the end of surgery: paracetamol (1 g), ketoprofene (100 mg), nefopam (20 mg).
From postanesthesia care unit (PACU) to day 2: paracetamol (1 g, at 6-hour intervals), ketoprofene (100 mg at 12-hour intervals and, if necessary, in the event of PONV, ondansetron (8 mg) or droperidol (1.25 mg).
Morphine rescue from PACU to day 2 was the same for all patients:
In the PACU, patients experiencing pain with an NRS >3 (NRS 0–10; from 0=no pain to 10=the worst pain imaginable) were given an intravenous titration of 3 mg of the drug under study (2 mg if body weight <60 kg) at 5 min intervals until an NRS ≤3 was obtained according to the protocol.20
After PACU, for the first 24 hours, intravenous patient-controlled analgesia was given to the patient with morphine (1 mg/mL): postanesthesia care unit (PCA (Gemstar, Abbott Laboratories, Abbott Park, Illinois, USA), boluses of 1 mg, lockout interval of 7 min.
After 24 hours, intravenous PCA was stopped and oral morphine was used as rescue (10 mg of actiskenan every 4 hours if the NRS pain score >3).
The ‘ERAS’ protocol was based on the ERSS protocol, except for oncology-specific preparations.19 This was the same for all patients and ran from the day before surgery up to hospital discharge: preoperative period (patient blood management program with oral iron or subcutaneous erythropoietin administration if hemoglobin (Hb) <13 g/L, no premedication, preoperative fasting: no food restrictions until H6 and no drinking restrictions until 2 hours prior to anesthesia, gabapentin or pregabalin were not introduced but continued if previously used), intraoperative period (intravenous fluid administration restriction <2 mL/kg/h, no intraoperative urinary catheter or gastric tube, central body temperature >36°C using hot air blankets, fluid warmers), postoperative period (early oral intake the day of surgery, no fluid administration, sitting up and walking on day 1). Transfusion was performed only if Hb level was <8 g/dL.
Clinical evaluation
Patients were evaluated by the nurses and anesthesiology care team blinded to the allocated groups. Preoperative evaluations were performed 7 days before surgery including an NRS for pain at rest, a neuropathic pain diagnostic questionnaire (score 0–10) on medical diseases, physiological and biological parameters (Hb, creatinine). Pain intensity and adverse events were assessed at the PACU and every 6 hours throughout the study period on the ward until day 5 (or at home by phone when discharge before day 5). No attempt was made to waken sleeping patients. Total intravenous drug administration at the PACU and over the 48-hour period was recorded. Opioid-related adverse events arising from the analgesic protocol were systematically assessed at the PACU and surgical ward by the nurses in charge of the patient (blinded to group assignment). Presence of nausea, vomiting, respiratory depression, pruritus, urinary retention requiring evacuation, allergy and hallucinations were recorded as binary (yes/no). Arterial oxygen saturation (pulse oximetry), heart and respiratory rates and blood pressure were also recorded every 6 hours.
After 3 months, patients were contacted to record the NRS for pain, neuropathic pain using the DN4 score (0–10 points), satisfaction with postoperative analgesia (0–10), quality of life (EQ-5D health-related quality of life questionnaire) and adverse events (medical or surgical complications).
Objectives
The primary objective was to define morphine consumption at 24 hours (PACU+intravenous PCA period up to 24 hours).
Secondary objectives were to define pain scores, the total amount of morphine consumed during the study period, the number of patients requiring titration at the PACU, the duration of time spent at the PACU and in hospital and, at 3 months, pain relief and patient satisfaction regarding quality of life (EQ-5D).
Sample size calculation
Previous studies had reported that mean morphine consumption was 30 mg (SD: 15 mg) and, using the ERAS program, ranged from 10 to 20 mg on postoperative day 1 including the PACU period: 50% opioid sparing.7 8 19 The power calculation for an expected absolute difference of 50% morphine reduction between the two groups, with a two-tailed α probability level of 0.05 and a power of 0.90 (1–β) yielded a sample size of 23 patients per group. This number was increased to 50 patients (25 per group) to account for 10% of patients lost to follow-up.
Statistical analysis
Statistical analysis was performed using Prism V.9.1.0 software and SAS V.9.4 (SAS, Cary, North Carolina, USA). The analysis was made with no interim analysis and carried out with intention to treat. The Shapiro-Wilk test was used to test for a normal distribution of continuous variables. Statistical results were expressed with means, SD or medians (25–75 IQR) according to distribution. Numbers and associated percentages were given for categorical variables. Quantitative variables were compared between the two study groups using an independent sample t-test or the Wilcoxon-Mann-Whitney test according to variable distribution. Categorical variables were compared using the χ2 test or Fisher’s exact test, as appropriate. The primary outcome (morphine consumption) was evaluated using the t-test due to the normal distribution of the variable. Secondary outcomes were evaluated using the Wilcoxon-Mann-Whitney test for quantitative variables with a non-normal distribution, by the χ2 test or Fisher’s exact test for qualitative variables when applicable. The numerical rating scale for pain was evaluated by a linear mixed model to take repeated measurements in the same patient into account. The NRS was the dependent variable. The randomization group and different measurement times were analyzed as fixed effects, and the patient was the random intercept. The slope, group and time interaction were tested. All statistical tests were conducted as 0.05 two-sided tests.
Results
Study population
From November 2019 to July 2021, 79 patients were screened and 50 patients were randomized (figure 1). One operation was canceled after randomization (the surgical indication was revised to an anterior approach). The final analysis included 49 patients in the intention-to-treat analysis for the primary end point and 49 for the secondary end points at discharge (figure 1).

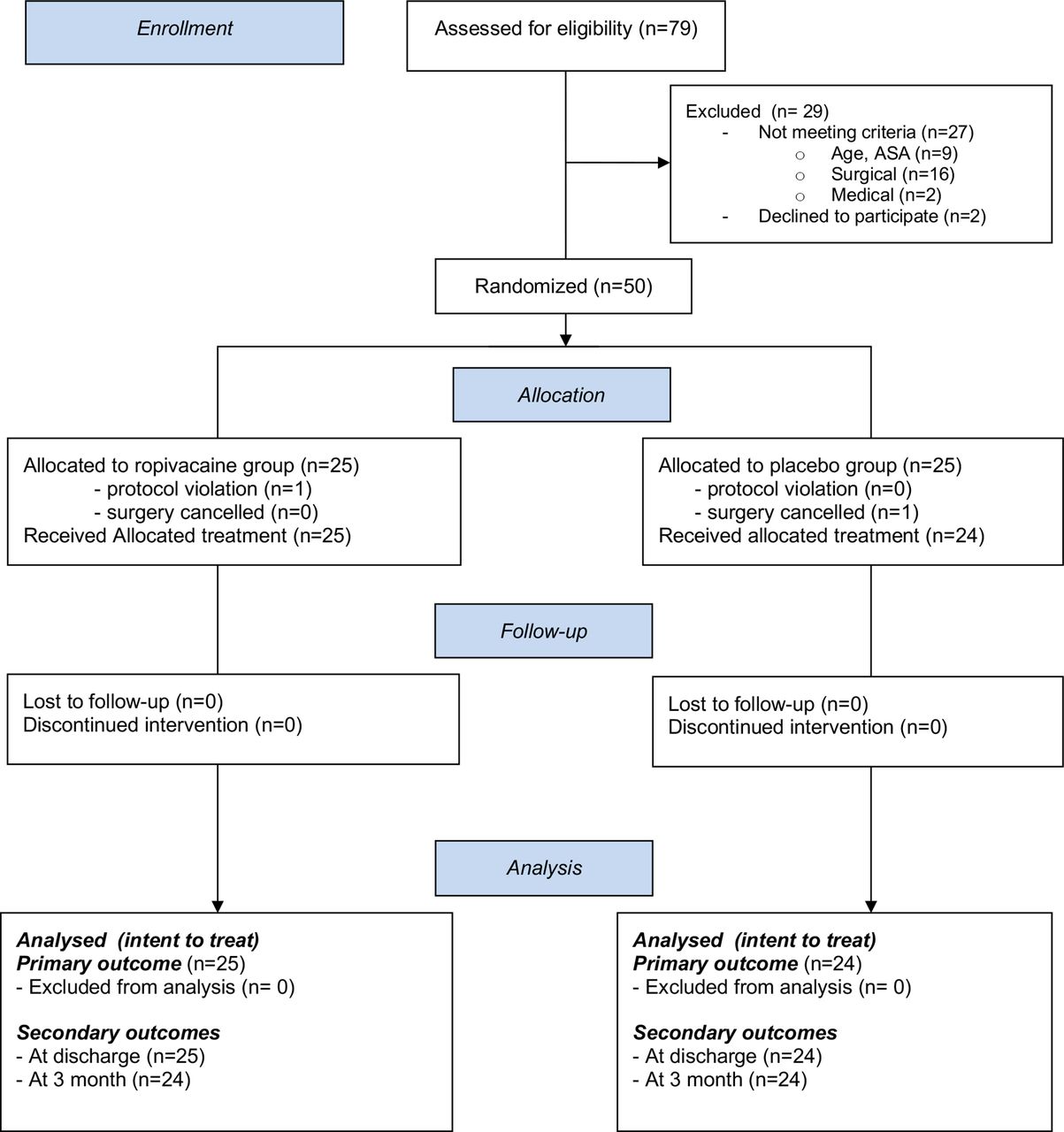{kind=link}
Study flow diagram. ASA, American Society of Anesthesiologists.
Baseline characteristics, preoperative pain, type of surgery and anesthesia are shown in table 1.
Patient, surgery and anesthesia characteristics
Primary outcome
Total morphine consumption during the first 24 hours postoperatively (including PACU) was not significantly lower in the ropivacaine group than in the saline group: 7.3 mg (3.7–19) vs 12.5 mg (3.5–26), respectively, p=0.51 (table 2).
Postoperative morphine consumption, pain score and adverse effects
The numbers of patients requiring morphine titration in the PACU and morphine consumption over the first 72 postoperative hours are given in table 2 with no difference between groups. Morphine-related side effects are also given in table 2 with no difference between groups.
Secondary outcomes
At baseline, pain scores at rest and during mobilization were similar. No difference was observed between either group over time in the PACU, from days 1 to 5, and at 3 months (table 2). Multiple comparison analysis by group and time (fixed model) did not reveal any difference. There was no significant difference between the two groups regarding time spent in the PACU or length of hospital stay (table 1).
At 3 months, there were no serious adverse events apart from one re-intervention on day 7 for hematoma. No surgical site infection was recorded and there was no difference between the two groups in terms of pain, quality of life or satisfaction scores. Details of the scores are given in table 3.
Quality of life at 3 months
At 3 months, the DN4 score was not different between groups. For all patients, the NRS scores for pain at rest or on mobilization were lower than preoperatively (tables 2 and 3).
Discussion
This prospective trial found that lumbar ESPB combined with the ERAS program (ERSS protocol) including multimodal analgesia did not lead to less opioid consumption than with saline within the first 24 hours after major spine surgery. Postoperative pain relief and patient quality of life at 3 months were similar for both groups, clearly demonstrating the limited benefits of this block in an ERAS program.
In this study, using an erector block brought few benefits, both on pain scores and additional morphine consumption. There may be several reasons for this lack of benefits. First, we performed very diversified multimodal analgesia which may have led to clear postoperative morphine sparing.19 This way, several recent reports have highlighted the postive impact of the ERAS program on opioid sparing to significantly reduce intravenous morphine consumption on the first postoperative days.6 19 In a recent network meta-analysis, the authors reported a mean reduction in morphine consumption and a 24-hour postoperative pain score of –26 (95% CI −39 to −12) mg and −2.3 (95% CI −3 to −1) using triple drug therapy.6 In our study, we used multiple drug therapy in the control group (see protocol). Thus, our control group was impacted by this program and consumed a median of only 12.5 mg, which is half the expected dose for calculating the initial sample size. Postoperatively, several patients in the control group did not use any opiates. The high dose of ketamine used (0.5 mg/kg) combined with dexamethasone, NSAIDs and nefopam, probably contributed to this effect. Moreover, this lack of benefit after spine surgery with ESPB was noted in two recently published studies.12 21 22 In a first study, Zhang et al found no difference on morphine rescue consumption in multimodal analgesia without ketamine but had associated dexmedetomidine.22 Later, in a single blind, randomized controlled study with NSAIDs without ketamine, Zhang et al, only found a decrease in morphine consumption and NRS scores at rest in the first 12 hours, with no difference at 24 hours (puncture in L3).12 All in all, the data in the current literature are similar to our results and tend to demonstrate only slight benefits in terms of morphine sparing or pain scores in favor of ESPB at lumbar level.10–18 In our study, we evaluated the long-term benefits in favor of ESPB (at 3 months), because no data were available for this major end point for patients (chronic pain, opioid abuse). Although the number of patients included was limited, we clearly demonstrated the absence of any benefits for these secondary end points. These data now need to be confirmed by a large cohort.
Regarding the efficacy of the erector block, the level of injection and volume injected have been debated. In our study, we performed the block opposite the surgical site (L2 or L3), whereas other authors injected local anesthetics into the low thoracic vertebrae (T10–T12) for lumbar surgery.22 In this study, the advantage of this higher-level injection was not demonstrated. Regarding the volume administered, the anatomical studies seem to favor large volumes so in our study we administered a volume of 40 mL.
Several limitations and biases should be discussed. First, this was a single-center study with patients that received lower consumption of morphine in controls than expected (see above). This strategy (ERAS) leads to an underpowered study due to the drastic reduction of morphine in both groups.19 Underestimated in the recent spinal surgery literature, this rescue reduction will require future studies to include a larger number of patients (large SD). This opioid saving by ERAS should be taken into account in future studies to calculate a number of patients. It should also be noted that saline injection throughout muscle plays a role in the analgesic component. A control group without any injection could have been proposed but we wanted to carry out a study against a real placebo. Second, the heterogeneity of the lumbar surgeries performed should be noted. The number of segments operated on varied from 2 to 4 and the duration of operations ranged from 55 to 371 min, which probably resulted in different degrees of postoperative pain, limited by the randomization. Concerning the site and volume of injection, these are debatable as previously mentioned. Concerning the risk of infection at the surgical site, the administration of LA in contact with surgery deserves discussion between anesthesia and surgical teams to limit the risk of sepsis related to contamination by the block.
To conclude, this study highlighted the absence of any benefits with ESPB when ERAS and multimodal analgesia were used in major lumbar spine surgery.6 18 However, the morphine savings in the ropivacaine group may be of interest in situations with a higher risk of morphine consumption. This clinical impact should be evaluated on a large cohort.
Supplemental material
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
In accordance with French legislation, this randomized study was approved by the institutional human investigation committee (Comité de Protection des Personnes, Kremlin Bicêtre, Paris, France, on September 11, 2019 with corresponding identification number: 19.051) and registered prior to enrollment on EudraCT (number: 2019-001678-26 on 2019-09-16, URL: https://www.clinicaltrialsregister.eu/ctr-search/trial/2019-001678-26/FR). Before inclusion, the investigator had obtained written informed consent from each subject in accordance with the Declaration of Helsinki.
Acknowledgments
The authors wish to thank Teresa Sawyers, English Medical Writer at the BESPIM, Nîmes University Hospital, France, for the final version of this paper.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors GA: designed and analyzed the study and prepared the manuscript; YG: analyzed and revised the manuscript; PBV: was in charge of recruitment and data management; VM: was in charge of recruitment and data management; MP: was in charge of recruitment and data management; NS: was in charge of data and logistics; PGC: analyzed the data and statistics; HE: was in charge of recruitment, data management and study design; YYL: designed the study and analyzed and revised the manuscript; MB: was in charge of anatomical dissection and analysis; PC: designed and analyzed the study, prepared the manuscript and accepts full responsibility for the finished work and/or the conduct of the study. He also had full access to data and controlled the decision to publish.
Funding This work was funded by Nîmes University Hospital, Carémeau, Nîmes, France. Funding was used solely for IRB registration purposes and purchase of drugs under study.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.