Article Text

Abstract
Background When combined with adductor canal block (ACB), local anesthetic infiltration between popliteal artery and capsule of knee (iPACK) is purported to improve pain following total knee arthroplasty (TKA). However, the analgesic benefits of adding iPACK to ACB in the setting of surgeon-administered periarticular local infiltration analgesia (LIA) are unclear.
Objectives To evaluate the analgesic benefits of adding iPACK to ACB, compared with ACB alone, in the setting of LIA following TKA.
Evidence review We conducted a meta-analysis of randomized trials comparing the effects of adding iPACK block to ACB versus ACB alone on pain severity at 6 hours postoperatively in adult patients undergoing TKA. We a priori planned to stratify analysis for use of LIA. Opioid consumption at 24 hours, functional recovery, and iPACK-related complications were secondary outcomes.
Findings Fourteen trials (1044 patients) were analyzed. For the primary outcome comparison in the presence of LIA (four trials, 273 patients), adding iPACK to ACB did not improve postoperative pain at 6 hours. However, in the absence of LIA (eight trials, 631 patients), adding iPACK to ACB reduced pain by a weighted mean difference (WMD) (95% CI) of −1.33 cm (−1.57 to –1.09) (p<0.00001). For the secondary outcome comparisons in the presence of LIA, adding iPACK to ACB did not improve postoperative pain at all other time points, opioid consumption or functional recovery. In contrast, in the absence of LIA, adding iPACK to ACB reduced pain at 12 hours, and 24 hours by a WMD (95% CI) of −0.98 (−1.79 to –0.17) (p=0.02) and −0.69 (−1.18 to –0.20) (p=0.006), respectively, when compared with ACB alone, but did not reduce opioid consumption. Functional recovery was also improved by a log(odds ratio) (95% CI) of 1.28 (0.45 to 2.11) (p=0.003). No iPACK-related complications were reported.
Conclusion Adding iPACK to ACB in the setting of periarticular LIA does not improve analgesic outcomes following TKA. In the absence of LIA, adding iPACK to ACB reduces pain up to 24 hours and enhances functional recovery. Our findings do not support the addition of iPACK to ACB when LIA is routinely administered.
- regional anesthesia
- nerve block
- lower extremity
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
Statistics from Altmetric.com
Background
Managing postoperative pain following total knee arthroplasty (TKA) continues to be challenging. Despite the relatively recent advent of the adductor canal block (ACB) and surgeon-administered periarticular local infiltration analgesia (LIA) for TKA, moderate-to-severe pain1 localized to the posterior knee remains commonplace during the first 24 hours postoperatively.2 Such pain interferes with early functional recovery,3 particularly within the context of clinical pathways4 featuring outpatient models of care.5 The infiltration between popliteal artery and capsule of knee (iPACK) block, an acronym for local anesthetic infiltration between the popliteal artery and capsule of the knee, is a relatively novel ultrasound (US)-guided technique purported to improve posterior knee pain post-TKA.6 However, US-guided iPACK may be redundant, and its incremental benefit limited, when local anesthetic is routinely administered intraoperatively by surgeons as part of periarticular LIA. Furthermore, the potential for foot-drop associated with iPACK, stemming from local anesthetic spread to the peroneal branch of the sciatic nerve, can impede early physiotherapy.7 Importantly, evidence on the topic is conflicting, with some trials suggesting that adding iPACK to ACB improves patient outcomes,8 9 while others failed to detect any benefit.10–12
This systematic review and meta-analysis seeks to evaluate the analgesic benefits of adding iPACK block to ACB, compared with ACB alone, in the setting of LIA for patients undergoing TKA. The primary outcome of this review was rest pain at 6 hours. Analgesic consumption, rest pain scores at other time points, functional recovery and iPACK-related complications were set as secondary outcomes.
Methods
This manuscript was written in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement guidelines.13 We sought randomized controlled trials that evaluated the benefits of adding iPACK to ACB compared with ACB alone in the setting of LIA for postoperative pain management following TKA. The study protocol was registered with the international prospective register of systematic reviews (PROSPERO): CRD42020210773.
Eligibility criteria
Randomized trials of adult patients undergoing unilateral or bilateral knee arthroplasty allocated to receive either iPACK in combination with ACB compared with ACB alone in the setting of LIA were considered for inclusion. Studies were eligible if ACB was performed in both groups. Surgeries completed under neuraxial or general anesthesia were accepted. No restrictions were imposed on language, and non-English studies were translated using the assistance of online translation.
Search methods
A search strategy was developed by an evidence-based medicine librarian (T.S.) for the US Library of Medicine (MEDLINE) database, the Cochrane Database of Systematic Reviews, and the Excerpta Medica (EMBASE) database. The databases were searched from July 2012 (first description of iPACK block) to March 1, 2021. The full search strategy for the MEDLINE database can be viewed in online supplemental appendix A. We also electronically searched the following clinical trial registries for additional citations: www.clinicaltrials.gov (US Clinical Trials Registry); https://apps.who.int (International Clinical Trials Registry Platform); https://dkrs.de (DRKS-German Clinical Trials Register); www.ctri.nic.in (Indian Clinical Trials Registry); https://www.irct.ir (Iranian Clinical Trials Registry); http://www.chictr.org.cn (Chinese Clinical Trials Registry); and http://www.clinicaltrials.in.th (Thai Clinical Trials Registry). Published abstracts of the following international conferences were also searched: American Society of Anesthesiologist (ASA) 2013–2020, American Society of Regional Anesthesia and Pain Medicine (ASRA) 2013–2020, International Anesthesia Research Society (IARS) 2013–2020, and the European Society of Anesthesiology (ESA) 2015–2020. Finally, the citation lists of all included studies were closely examined to identify any other potentially relevant trials.
Supplemental material
Selection of included studies
The title and abstracts obtained from the search strategy were reviewed independently by two reviewers (NH and BS). All potentially eligible citations had their full-text versions retrieved for additional consideration by the same two reviewers. In the case of disagreement on full-text inclusion, a discussion was initiated until a consensus was reached. If a final decision could not be reached by discussion, a third reviewer assessed the article in question (FWA) and made the final decision.
Although LIA is currently the care standard in many centers, a preliminary search of the literature revealed that many trials8 10 11 14–20 excluded this analgesic component when evaluating the benefits of adding iPACK to ACB. We therefore decided to dichotomize (subdivide) the patient population and evaluation of outcomes based on presence or absence of LIA.
Data extraction
A reviewer (NH) created a standardized data extraction form. Data extraction was then carried out in duplicate independently by two reviewers (NH and BS). Any disagreements in data extraction between the two reviewers was discussed until a consensus was reached. If a final decision could not be reached by discussion, a third reviewer assessed the article in question (FWA) and made the final decision. The data extraction form collected information regarding: publication year; type of surgery; primary outcome of study; iPACK technique (including dose and volume of local anesthetic); ACB technique (including dose, volume, and use of catheter); LIA technique; preoperative, intraoperative and postoperative analgesic regimen; rest pain scores at all time points; analgesic consumption at all reported time intervals; postoperative function and the tool used for measurement; opioid related side effects; and iPACK-related complications. Data presented in graphical format was extracted using a graph digitizing software (GraphClick, Arizona Software, USA). When needed, authors of included studies were contacted for additional methodological trial information and outcome data.
Assessment of methodological quality
The methodological quality of each included trial was assessed using the Cochrane Collaboration Risk of Bias tool. Specifically, each study was evaluated for random sequence generation; allocation concealment; level of blinding of study personnel and outcome assessors; loss to follow-up and selective outcome reporting.21 The overall methodological quality of evidence across statistically pooled outcomes was assessed using the guidelines created by the Grades of Recommendation, Assessment, Development and Evaluation (GRADE) working group.22 23 Pooled outcomes were classified as being of high quality (⊕⊕⊕⊕), moderate quality (⊕⊕⊕⊝), low quality (⊕⊕⊝⊝), or very low quality (⊕⊝⊝⊝) evidence.
Primary and secondary outcomes
We designated knee pain at rest reported at 6 hours postoperatively, as measured on a numerical rating scale (NRS), as the primary outcome. The 6-hour time point enables assessment of the analgesic effectiveness of iPACK during its peak effect, based on the duration of local anesthetics used.
Secondary outcomes of this review included postoperative opioid consumption in milligrams of oral morphine equivalents at postanesthesia care unit (PACU) and 24 hours; acute postoperative rest pain severity in the PACU (1 hour), and at 12 and 24 hours; opioid related side effects (postoperative nausea and vomiting, excessive sedation, respiratory depression, pruritus, urinary retention, or constipation); functional recovery; and iPACK-related complications (foot drop (sciatic nerve block), hematoma, nerve injury or local anesthetic systemic toxicity).
Measurement of outcome data
All postoperative pain scores were converted to an equivalent score on the 0–10 cm NRS pain score, with 0 corresponding to no pain and 10 corresponding to worst pain imaginable. All analgesic consumption data were converted to milligrams of oral morphine equivalents.
Statistical analysis
The mean and SD were extracted for all continuous outcome data. If not available, approximations were made using reported data. Specifically, the median and IQR, median and range, or mean and 95% CI were used to approximate these values, based on whichever was available.24 If needed, dichotomous outcome data were converted to continuous form represented by a mean and SD.25 Finally, the median was used to approximate the mean in situations when statistical conversions could not be made.26 Dichotomous outcome data related to adverse events was converted to overall incidence numbers.
For postoperative functional recovery, we anticipated that authors may use various tools and scales. Therefore, we a priori planned to report the (1) weighted mean difference (WMD) of all studies if the same continuous scale was used; (2) standardized mean difference (SMD) and corresponding log(OR) if different scales that measured the same theme were used; and (3) OR if all functional recovery was reported in a binary format. Conversion from SMD to log(OR) was done using the formula log(OR)=SMD (π/√3).27 28
Meta-analysis
Statistical pooling was performed for all outcomes when data were available from at least three studies. For continuous outcome data, we used the inverse variance method with random-effects modeling in anticipation of the presence of clinical difference among trials. For dichotomous outcome data, we used the Mantel-Haenszel random-effects method.29 For the primary outcome of this review, rest knee pain at 6 hours, a WMD with a 95% CI was calculated. A two tailed p value of <0.05 was designated as the threshold of statistical significance.
A WMD with a 95% CI and a OR with 95% CI were calculated for continuous and dichotomous secondary outcomes, respectively. We a priori adjusted the threshold of statistical significance for the pooled secondary outcomes in each comparison using the Bonferroni-Holm correction (Pc, corrected threshold of statistical significance) to account for the secondary outcomes analyzed.30 A 95% CI was also used for all secondary outcomes.
Interpretation
The minimal clinically important difference (MCID) was used for interpretation of all pain scores presented in this review.31 For a single time-point, the MCID of NRS acute postoperative pain has been reported to be 1.0 cm.32
Exploring heterogeneity
The degree of heterogeneity was evaluated for all statistically pooled outcomes by calculation of an I2 statistic. Significant heterogeneity was considered to be present with I2 values >50%.24 When significant heterogeneity was present in the primary outcome of this review, sensitivity analysis was performed based on preidentified clinical factors that may affect this outcome, namely, (1) ACB technique (single shot vs catheter based) and (2) postoperative analgesic regimen (unimodal opioid-based vs multimodal analgesia).
Assessment of publication bias
The risk of publication bias assessed using the Egger’s Regression test33 for all outcomes examined, and a funnel plot for risk of bias was constructed for the primary outcome.
Data management
Sensitivity analysis was performed using Comprehensive Meta-Analysis V.3.0 (Engelwood, USA). Review Manager Software (RevMan V.5.2; Nordic Cochrane Centre, Cochrane Collaboration) was used to create forest and funnel plots.
Results
Study characteristics
The initial search strategy identified 30 unique citations; 19 were excluded due to being an ineligible study design (n=16) or ineligible comparator (n=3). Of the remaining 11 citations, 634–39 were excluded (ineligible study design (n=2)37 38 ; ineligible comparator (n=3)34–36 ; and ineligible study population (n=1)39) and 5 trials8–12 were included. Hand searching of conference proceedings, trial registries, and Gray literature identified an additional nine14–20 40 41 trials that satisfied the eligibility criteria. Thus, a total of 14 trials8–12 14–20 40 41 were included in this review; 108–12 15 16 18 40 41 of these were prospectively registered with clinical trial registries, 120 was started prior to 2019, and we could not ascertain the registration status for the remaining 3 due to language barriers14 17 or inability to communicate with the authors.14 17 19 The authors of four12 15 40 41 trials provided supplementary methodological details facilitating this review. A full flow diagram of study inclusion can be viewed in online supplemental appendix B.
Supplemental material
The clinically relevant outcomes and trial characteristics are summarized in table 1. The 14 trials8–12 14–20 40 41 encompassed a total of 1044 patients. The comparisons included 49 12 40 41 conducted in the presence of periarticular LIA, and another 108 10 11 14–20 conducted in the absence of LIA. Unilateral TKA was performed in all studies under spinal anesthesia in eight trials8 11 12 15 19 20 40 41 or general anesthesia in four trials.9 14 16 17 One study10 permitted both spinal and general anesthesia, and another18 did not specify the nature of surgical anesthetic used. All included trials assessed postoperative pain severity scores at rest8–12 14–20 40 41 in the first 24 hours, and eight studies assessed postoperative opioid consumption in the same time frame.8–10 12 15 18 19 40 41 Finally, it was noted that the results reported in one study11 were conflicting, with results reported in text and conclusions being different from those reported in the accompanying tables.
Study characteristics and outcomes of interest assessed in included studies
The iPACK and ACB techniques and analgesic regimens are presented in table 2. The iPACK blocks were performed preoperatively in 11 studies,8–12 14–17 20 40 postoperatively in 1,41 and intraoperatively in 119; 1 study did not specify the timing of iPACK block performance.18
Local anesthetic techniques for iPACK and analgesic regiments of included studies
The risk of bias assessment for all included studies can be viewed in online supplemental appendix C.
Supplemental material
Primary outcome
Rest pain at 6 hours
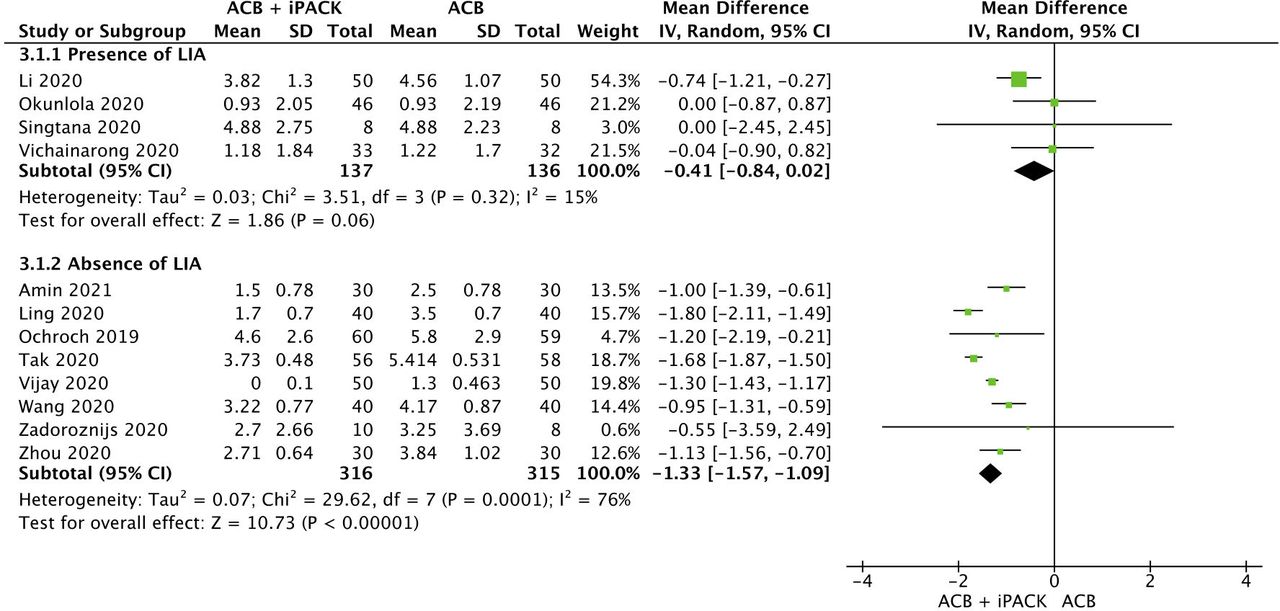
A total of four studies9 12 40 41 (273 patients; ACB + iPACK: 137, ACB: 136) evaluated the benefits of adding iPACK block to ACB in the presence of periarticular LIA. Adding iPACK block did not improve postoperative pain severity at 6 hours, with a WMD (95% CI) of −0.41 cm (−0.84 to 0.02) (p=0.06, I2=15%) (figure 1A). This analysis was characterized by a low heterogeneity (I2=15%). Although visual inspection of the funnel plot suggested that smaller studies reported greater treatment effects, Egger’s test indicated the absence of publication bias (p=0.27) (online supplemental appendix D). The GRADE of evidence was rated as moderate due to imprecision in the pooled estimate.
Supplemental material

{kind=link}
Forest plot of rest pain scores at 6 hours postoperatively for (A) ACB versus ACB with infiltration in the iPACK in the presence of LIA) and (B) ACB versus ACB with iPACK in the absence of LIA. Pooled estimates of the weighted mean difference are shown with 95% CIs. Pooled estimates are represented as diamonds and lines represent the 95% CIs. ACB, adductor canal block; iPACK, interspace between the popliteal artery and capsule of the knee; LIA, local infiltration analgesia.
In contrast, eight studies8 11 14–17 19 20 (631 patients; ACB + iPACK: 316, ACB: 315) evaluated the effect of adding iPACK to ACB on postoperative rest pain at 6 hours in the absence of periarticular LIA. Adding iPACK reduced rest pain at 6 hours by a WMD (95% CI) of −1.33 cm (−1.57 to –1.09) (p<0.00001, I2=76%) (figure 1B). This difference surpassed the predesignated threshold for clinical importance of 1.0 cm. Results for this outcome were characterized by high heterogeneity (I2=77%). Sensitivity analysis by excluding studies that used continuous (catheter based) ACB8 19 did not decrease heterogeneity. However, the heterogeneity was resolved (I2=2%) by excluding studies that used unimodal opioid-based analgesic regimens14 17 20 and the one study11 with conflicting results. Although visual inspection of the funnel plot suggested that smaller studies reported greater treatment effects, Egger’s test indicated the absence of publication bias (p=0.56) (online supplemental appendix D). The GRADE of evidence was rated as moderate due to significant heterogeneity in the overall pooled estimate.
To ensure adherence to the journal’s policy42 regarding prospective trial registration, we also conducted an additional post-hoc sensitivity analysis on the primary outcome by excluding all four trials14 17 19 20 for which we could not confirm prospective registration. The new WMD (95% CI) was −1.29 (−1.85 to –0.72), indicating that the results were robust to this sensitivity analysis.
Secondary outcomes
Rest pain in PACU, 12 hours and 24 hours
A total of four studies9 12 40 41 (n=273; ACB + iPACK: 137, ACB: 136) evaluated the effect of adding iPACK block to ACB in the presence of periarticular LIA on postoperative pain in the PACU and at the 12-hour and 24-hour time points. Adding iPACK did not improve pain severity at any of these time points (table 3). All p values were robust in directionality to the Bonferroni-Holm correction (PACU, p>Pc=0.05; 12 hours, p>Pc=0.01; and 24 hours, p>Pc=0.017). The GRADE of evidence was rated as moderate for the measurements in PACU and 12 hours, and high for 24 hours (online supplemental appendix E).
Supplemental material
Secondary endpoint results
In contrast, adding iPACK block to ACB in the absence of periarticular LIA was evaluated by 510 14 16 18 20 (n=345; ACB + iPACK: 173, ACB: 172), 68 14 16 17 19 20 (n=499; ACB + iPACK: 250, ACB: 249), and 108 10 11 14–20 (n=757; ACB+iPACK: 380, ACB: 377) trials at the PACU, 12-hour, and 24-hour time points, respectively. In the absence of LIA, the addition of iPACK to ACB reduced rest pain at 12 and 24 hours by a WMD (95% CI) of −0.98 (−1.79 to –0.17) (p=0.02, I2=97%) and −0.69 (−1.18 to –0.20) (p=0.006, I2=94%), respectively; however, these differences did not surpass predesignated threshold for clinical importance of 1.0 cm on a NRS. No differences in rest pain scores were observed between the two groups in the PACU (table 3). The p values were robust in directionality to Bonferroni-Holm correction at PACU (p>Pc=0.025) and 24 hours (p<Pc=0.01); however non-significance was obtained at 12 hours (p>Pc=0.012). The GRADE of evidence was rated as low at PACU and moderate for all other time points (online supplemental appendix E).
Postoperative opioid consumption in PACU
No trials assessed PACU opioid consumption in the presence of periarticular LIA.
Two studies10 18 wherein iPACK was added to ACB in the absence of periarticular LIA evaluated opioid consumption in the PACU. Results for this outcome were not pooled; but qualitatively, both studies10 18 failed to detect a benefit when iPACK was added.
Cumulative 24-hour postoperative opioid consumption
The effect of adding iPACK block to ACB in the presence of periarticular LIA on cumulative 24-hour postoperative opioid consumption was evaluated by four9 12 40 41 studies (n=273; ACB + iPACK: 137, ACB: 136). The addition of iPACK failed to reduce 24-hour postoperative opioid requirements. (table 3) The p value remained robust in directionality to Bonferroni-Holm correction (p>Pc=0.012) and the GRADE of evidence was rated low (online supplemental appendix E).
Similarly, the effect of adding iPACK block to ACB in the absence of periarticular LIA on cumulative 24-hour postoperative opioid consumption was assessed by three studies8 10 18 (n=246; ACB + iPACK: 124, ACB: 122). The addition of iPACK did not improve this outcome (table 3). The p value remained robust in directionality to Bonferroni-Holm correction (p>Pc=0.05) and the GRADE of evidence was rated as moderate (online supplemental appendix E).
Functional recovery
The effect of adding iPACK block to ACB in the presence of periarticular LIA on functional recovery was evaluated by three9 12 41 studies (n=257; ACB + iPACK: 129, ACB: 128). The addition of iPACK did not improve functional recovery (table 3). The p value remained robust in directionality to Bonferroni-Holm correction (p>Pc=0.025) and the GRADE of evidence was rated low (online supplemental appendix E).
In contrast, the effect of adding iPACK block to ACB on postoperative function in the absence of periarticular LIA was evaluated by nine studies8 10 11 14–19 (n=696; ACB + iPACK: 349, ACB: 347). Adding iPACK improved the log(OR) (95% CI) of functional recovery by 1.28 (0.45 to 2.11) (p=0.003, I2=87%) (table 3); The p value remained robust in directionality to Bonferroni-Holm correction (p<Pc=0.008) and the GRADE of evidence was rated moderate (online supplemental appendix E).
Opioid-related side effects
Evaluating the effect of adding iPACK block to ACB on opioid-related side effects in the presence of periarticular LIA was performed in two studies9 40 (n=116; ACB + iPACK: 58, ACB: 58). Data were not pooled for this outcome; but qualitatively, both studies did not detect a difference between the two groups.
Evaluating the effect of adding iPACK block to ACB on opioid-related side effects in the absence of periarticular LIA was performed in six studies14–17 19 20 (n=398; ACB + iPACK: 200, ACB: 198). Adding iPACK seemed to reduce the OR (95% CI) of opioid related side effects by 0.43 (0.21 to 0.91) (p=0.03, I2=7%) (table 3); however, correction for multiple testing using the Bonferroni-Holm correction rendered this difference non-significant (p>Pc=0.017). The GRADE of evidence was rated as high (online supplemental appendix E).
iPACK complications
No block-related complications were reported in any of the studies included in this review.8–12 14 16 20 The quality of evidence for this outcome was rated as high.
Discussion
This systematic review and meta-analysis indicates that the addition of iPACK to ACB in the setting of periarticular LIA for postoperative pain management following TKA does not confer any clinically important analgesic benefits. However, in the absence of periarticular LIA, moderate quality evidence suggests improvement in pain severity between 6 and 24 hours postoperatively and enhanced functional recovery when iPACK is added to ACB. These improvements in pain severity appear to be clinically meaningful at 6 hours but not at the remaining time points.
First described by Sinha et al,6 the theoretical benefits of iPACK stem from anesthetizing the articular branches originating from main trunks of tibial and obturator nerves, which contribute to posterior knee pain following TKA.6 43 Unlike the sciatic nerve block, the US-guided iPACK block is arguably easier to perform and aims to spare the main trunks of the tibial and common peroneal nerves and maintains sensorimotor function below the knee,6 which is paramount to promoting early functional recovery and participation in physical therapy.38 44 The results of our review are largely consistent with these proposed benefits as iPACK was found to improve pain scores after surgery when LIA is not used. However, our review found no important benefits when iPACK was added to ACB in the presence of LIA, which is most likely explained by redundancy in local anesthetic coverage and effect between iPACK and LIA. While the trials included in this review did not describe the LIA technique in full detail, the benefits observed herein suggest that the posterior knee capsule was among the tissues routinely targeted by LIA.
Our systematic review and meta-analysis has multiple strengths. First our literature search was comprehensive enabling us to generate meaningful estimates of effects for clinically important outcomes. Second, we successfully resolved heterogeneity in our primary outcome using sensitivity analysis according to prespecified clinically relevant covariates (use of multimodal analgesia). This generated an estimate of effect that was more generalizable to modern clinical practice, where a multimodal postoperative analgesia is routinely used. Third, we were able to highlight the relative effectiveness of iPACK by stratifying our analysis by the use of LIA, reflecting contemporary multimodal practices. Fourth, results for analgesic and functional outcomes were consistent across the stratified analysis, which corroborates our findings. Fifth, our use of conservative thresholds for statistical significance in our secondary outcomes by using the Bonferroni-Holm correction limited the risk of multiple testing bias.
However, limitations of this systematic review exist. This review included a limited number of relatively small clinical trials, which may predispose to bias and limit external validity. This was most notable for the comparison conducted in the presence of periarticular LIA, which was limited to four studies.9 12 40 41 Furthermore, because of lack of systematic assessment, we were unable to provide estimates of effect for important outcomes, such as postoperative pain localized to the posterior knee. Finally, some outcomes8 10 18 20 required using the median to approximate the mean; this approximation is true only if the distribution of data is symmetrical. This assumption may not necessarily be true, in which case the validity of the estimate becomes questionable.
Conclusions
The addition iPACK to ACB in the setting of periarticular LIA does not improve post-TKA analgesic outcomes. In contrast, moderate-quality evidence suggests that adding iPACK to ACB in the absence of LIA reduces pain severity up to 24 hours and enhances functional recovery, but without a corresponding reduction in opioid consumption. This appears to be most pronounced at 6 hours, where the improvement in pain is clinically meaningful (based on a MCID of 1 cm on a NRS). Our findings do not support the addition of iPACK to ACB when periarticular LIA is routinely administered as part of a multimodal analgesic pain management strategy.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Acknowledgments
The authors would like to thank Dr Poonam Pai, Dr Sergejs Zadoroznijs, Dr Wirinaree Kampitak, and Dr Kanokphol Singtana for providing data and information for this review. We would also like to thank Tamara Sawyer for her assistance in the development of the search strategy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Faraj_RegAnesth
Contributors All authors provided equal contribution.
Funding Dr Brull receives research time support from the Evelyn Bateman Cara Operations Endowed Chair in Ambulatory Anesthesia and Women’s Health, Women’s College Hospital, and Merit Award Program, Department of Anesthesia and Pain Medicine, Toronto, Ontario, Canada.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.