Article Text

Abstract
Background There is heterogeneity in the names and anatomical descriptions of regional anesthetic techniques. This may have adverse consequences on education, research, and implementation into clinical practice. We aimed to produce standardized nomenclature for abdominal wall, paraspinal, and chest wall regional anesthetic techniques.
Methods We conducted an international consensus study involving experts using a three-round Delphi method to produce a list of names and corresponding descriptions of anatomical targets. After long-list formulation by a Steering Committee, the first and second rounds involved anonymous electronic voting and commenting, with the third round involving a virtual round table discussion aiming to achieve consensus on items that had yet to achieve it. Novel names were presented where required for anatomical clarity and harmonization. Strong consensus was defined as ≥75% agreement and weak consensus as 50% to 74% agreement.
Results Sixty expert Collaborators participated in this study. After three rounds and clarification, harmonization, and introduction of novel nomenclature, strong consensus was achieved for the names of 16 block names and weak consensus for four names. For anatomical descriptions, strong consensus was achieved for 19 blocks and weak consensus was achieved for one approach. Several areas requiring further research were identified.
Conclusions Harmonization and standardization of nomenclature may improve education, research, and ultimately patient care. We present the first international consensus on nomenclature and anatomical descriptions of blocks of the abdominal wall, chest wall, and paraspinal blocks. We recommend using the consensus results in academic and clinical practice.
- regional anesthesia
- analgesia
- anesthesia
- local
- pain
- postoperative
- acute pain
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Statistics from Altmetric.com
Background
Regional anesthesia continues to define its role as a fundamental component of perioperative care. This has recently been driven by the increased availability, expertise, and understanding of the utility of ultrasound in the safe and effective performance of regional anesthesia.1 As a consequence, ultrasound-guidance has led to the development of innumerable novel approaches to deliver analgesia and surgical anesthesia, including the concept of injecting local anesthesia into a fascial plane to indirectly access target nerves.2
Understanding and application of these novel approaches are hampered by significant heterogeneity in nomenclature and anatomical descriptions of these regional anesthetic techniques. Similar techniques carry different names, and techniques with the same name may represent very different technical approaches and targets.2–11 This inconsistency may prevent clear communication in clinical settings and may lead to confusion in teaching and training in regional anesthesia and related disciplines. Moreover, this absence of consensus in the nomenclature may potentially adversely affect the interpretation and synthesis of data, slowing the progress and standardization of clinical and non-clinical research related to these new techniques. Finally, concerns over this lack of clarity could adversely affect more widespread adoption of regional anesthetic techniques by practitioners who have not received advanced training. This latter concern may have significant implications for improving patient access to regional anesthesia globally.12
There is a need to standardize nomenclature of regional anesthetic techniques for the benefit of trainees, researchers, clinicians, and ultimately patients. We conducted an international study, led by representatives from both the American Society of Regional Anesthesia and Pain Medicine (ASRA) and European Society of Regional Anaesthesia and Pain Therapy (ESRA), aiming to achieve consensus on nomenclature in abdominal wall, paraspinal, and chest wall regional anesthetic techniques. These recommendations regarding names and definitions are intended to have broad applications in regional anesthesia clinical practice, education, and scholarly work in the future.
Methods
We performed an international Delphi consensus study to standardize the names and anatomical definitions of regional anesthetic techniques for (1) abdominal wall blocks; (2) paraspinal blocks; and (3) chest wall blocks. Delphi studies are widely used to obtain input and consensus from a group of experts using an iterative process of multiple rounds, including long-list generation and subsequent feedback and voting.13–17 A modified Delphi method may include at least two rounds of electronic questionnaires, followed by a final round table discussion and ratification round.16 We adhered to the modified Delphi approach in the conduct of this study, with two electronic voting rounds followed by a third round table discussion. The study was conducted by an Executive Committee (KE, EA, NE, SK, ERM, MRW), a Steering Committee (KE, EA, KJC, NE, HE, SK, ERM, AS, MRW, JLX), and an expert panel of Collaborators. This study received Institutional Review Board exemption from Stanford University (ID 58535).
Collaborator selection
Several approaches for the selection of participants for the expert panel can be undertaken, but a pragmatic decision was made to include anesthesiologists who have experience in either performing, researching, or educating on at least one specific regional anesthetic technique. These experts can directly influence patient care and the academic landscape locally, nationally, and internationally. A diverse panel of international collaborators was invited, including academic and private practice anesthesiologists from North America, Europe, Asia, and Australia, aiming to include a broad range of ethnodemographic backgrounds representing varied theoretical and clinical practices. We also invited experts in anatomy relevant to regional anesthesia to participate. Participants were invited on September 8, 2020, and the goals, processes, and timelines of the study were described. Participants who declined or did not respond were no longer included.
Scope
This project aimed to achieve consensus on two characteristics: names and anatomical descriptions for the position of the needle tip for different regional anesthetic techniques. Names were defined as the word or set of words by which each technique is known, addressed, or referred to. Anatomical descriptions were defined as the anatomical location of the needle tip. This meant that non-ultrasound-guided methods of needle tip localization were not considered (eg, field blocks and landmark-based techniques). The type of needle used, needle trajectory, patient position, the position of the ultrasound transducer, use of catheters, or any other technical elements related to the performance of regional anesthetic techniques were not considered. Similarly, efficacy, safety, feasibility, surgical anesthesia, or any other clinical element of each regional anesthetic technique were not considered. After the first round, it was also decided that the vertebral level should be added to the list of technical elements that would not be considered applicable to this project.
Long-list formulation
A long-list of regional anesthetic techniques of the abdominal wall, paraspinal, or chest wall areas was formulated by the Steering Committee through a directed literature review. This involved reviewing the available literature for relevant regional anesthetic techniques, the permutations of names for techniques in similar areas, and anatomical descriptions of regional anesthetic approaches. All regional anesthetic techniques were collated in a Microsoft Excel (Microsoft Inc, Redmond, Washington, USA) spreadsheet that was then reviewed by all members of the Steering Committee. Techniques were excluded if they were unclear, duplicates, or outside the scope of the current project. Responses were then organized according to the anatomical region to which they applied, the language refined and clarified, and appropriate references were cited to each before proceeding with the first round of the Delphi study.
First round
The long-list was distributed electronically to all Collaborators, accompanied by specific instructions on completion of the tool. The long-list contained all relevant names and associated descriptions of the anatomical locations for the three categories of interest. Collaborators were invited to consider each name and anatomical description and state whether they ‘Agree’, ‘Disagree’, or were ‘Unsure’ about the presented nomenclature. Collaborators were advised to vote on each approach independent of others and to consider the voting for the name and its anatomical description independently. As such, it was possible for Collaborators to agree with the name, but disagree with the anatomical description and vice versa, or agree or disagree with both the name and anatomical description. Moreover, uncertainty was accepted. Collaborators were also invited to provide comments for each proposed name and anatomical descriptor. Responses were returned to the project administrator (AS) for anonymization and collation. A fully anonymized spreadsheet containing all comments and votes was then analyzed by the Steering Committee and revisions were made to increase the prospects of achieving consensus in the second round (figure 1). The possible outcomes to the names and or anatomical descriptions were explicitly stated as one of the following:
≥75% agreement: include. Terms proceeded to the next round unchanged.
<75% agreement: revise. Terms were revised for clarity in the absence of multiple names or anatomical descriptions.
<75% agreement: harmonize. If multiple names or anatomical descriptions were deemed to be similar enough to warrant harmonization, this was done using either a novel anatomically descriptive term or an existing name or anatomical description encompassing multiple block descriptions.
<50% agreement: exclude. Terms were excluded if they were outside the scope, were too similar to alternative terms, or were unclear. However, if there were multiple terms for similar blocks with <50% agreement, these were also eligible for considering harmonization.

(A) Flowchart demonstrating Steering Committee decision-making for names between Delphi rounds to achieve consensus. (B) Flowchart demonstrating Steering Committee decision-making for anatomical descriptions between Delphi rounds to achieve consensus.
The Steering Committee then formulated a revised list of approaches, along with explicit justification for the implemented changes.
Second round
All Collaborators who participated in the first round received the results, all associated comments, and a revised list for voting and comments in round two. The process of declaring agreement and commenting in this round adhered to those outlined in the first round. Three clarifying questions were also posed to the participants that arose in the comments during the analysis of first-round results (see online supplemental appendix). Once again, all responses were returned to the project administrator who collated and fully anonymized the results for analysis by the Steering Committee which made revisions based on first-round results to move the group towards achieving consensus in the third round (figure 1). The possible outcomes to the names and or anatomical descriptions were explicitly stated as one of the following:
Supplemental material
Supplemental material
≥75% agreement: accept. Terms accepted in the final list of agreed nomenclature.
50%–74% agreement: discuss. Terms proceeded for discussion in the third round.
<50% agreement: exclude. Terms not discussed further due to similar approaches with different names or anatomical locations achieving higher agreement or remaining an area of future research. An exception was made in the event of a recognized group of blocks or a clarifying question in which none of the options achieved a threshold of >50%, in which case the two highest-scoring names, anatomical descriptions, or responses to clarifying questions proceeded to the third round.
Third round
All Collaborators were invited to attend a virtual round table discussion aiming to achieve consensus for names, anatomical descriptions, and clarifying questions. This was hosted via videoconferencing software (Zoom Video Communications, San Jose, CA, USA) that allowed live online polling. The session was chaired by one member of the Executive Committee (KE) who did not participate in discussions, and two further co-chairs from the Executive Committee (NE and MW). Each name or anatomical description that had yet to achieve consensus but proceeded from the second round was allocated 5 min for discussion, followed by 1 min of anonymous voting. Using an iterative process, areas that warranted revision were modified and subsequent voting was undertaken. The possible outcomes to the names and/or anatomical descriptions were one of the following:
≥75% agreement: accept as strong consensus. Terms accepted in the final list of agreed nomenclature.
50%–74% agreement: accept as weak consensus. Terms accepted but proceeded for discussion in the manuscript.
<50% agreement: exclude. Terms not accepted and considered areas for future research.
Statistical analysis
Consensus was a priori defined as a threshold of 75% Collaborator agreement, which is a threshold that has been used for previous Delphi studies.16 However, there is no broad agreement as to what determines consensus;18 therefore the steering committee iteratively adapted criteria after the third round to define strong consensus (≥75% agreement), weak consensus (50%–74% agreement), and no consensus (<50% agreement). The median (IQR (range)) number of participants invited to Delphi studies is 17 (11–31 (3–418)).18 We, therefore, selected a convenience sample of 78 participants to invite, to account for anticipated dropouts. Data were reported descriptively. When percentages are reported, they refer to the proportion of Collaborators that agreed with a given option, unless otherwise stated (eg, stating ‘50%’ means ‘50% agreement’). All denominators for percentages reported were based on responses, rather than participants.
Results
A total of 78 participants were invited to be Collaborators, of which 60 agreed to participate; 60 (100%), 59 (98%), and 52 (87%) participated in first, second, and third rounds, respectively (online supplemental appendix 2). The flowchart of names of blocks that have been included beyond the first round is shown in figure 2. Further details for all proposed names and anatomical descriptions, including changes made, are shown in online supplemental appendix 1 and further descriptions in online supplemental file 2.

Flowchart of inclusion and agreement (%) for each proposed block approach included beyond the first round. TAP, transversus abdominis plane; TLIP, thoracolumbar interfascial plane.
First round
For abdominal wall blocks, the first round produced no consensus on named variations of the transversus abdominis plane (TAP) block which were therefore excluded.19 Similarly, a range of named variations of the quadratus lumborum blocks were excluded.20–23 There was no consensus on naming quadratus lumborum block types 1, 2, 3 and transmuscular approaches when compared with the lateral, posterior, and anterior quadratus lumborum block approaches (53%, 71%, and 58%, respectively).5 10 24–26
For paraspinal approaches, there was no consensus on named variations of the erector spinae plane (ESP) block based on the vertebral level targeted (eg, lumbar ESP), and it was agreed that this should not be part of the basic nomenclature, but should instead be added as a prefix where appropriate.27 The midpoint transverse process to pleura (MTP), subtransverse process interligamentary plane (STIL), costotransverse foramen plane (CTF), and the multiple injection costotransverse (MIC) blocks achieved weak or no consensus on naming (51%, 18%, 25%, and 26%, respectively).28–31 Comments suggested that they all carried similarities in terms of the anatomical location of injection, and it was therefore proposed that they be harmonized into a single new name, the intertransverse process (ITP) block, for consideration in the second round. The rhomboid intercostal subserratus block had no consensus (46%) and it was suggested that this was better presented as a single-injection approach, with the name reflecting this.32 There was no consensus on the thoracolumbar interfascial plane (TLIP) block (35%) and the modified TLIP (21%) block names,33 34 and new names that were more descriptive of the anatomical site of injection were proposed for consideration; these were the ‘lumbar multifidus’ and ‘lumbar longissimus’ plane blocks, respectively.8 There was also no consensus on the naming of a range of cervical paraspinal plane blocks, and harmonization of these approaches was suggested under the new name ‘cervical paraspinal interfascial’ plane blocks.35 36
For chest wall techniques, variations of the serratus anterior plane block were presented, but there was limited consensus on both the name and the anatomical descriptions, with comments highlighting concerns regarding the lack of specificity of the name and descriptions.37 There was also limited consensus on eight parasternal block approaches (online supplemental appendix 1), which were proposed to be harmonized into the term ‘parasternal intercostal’ plane blocks (deep and superficial).34 38–43 There was weak consensus on the naming of PECS I and II blocks,44 45 and therefore more anatomically descriptive ‘interpectoral’ or ‘superficial pectoralis’ plane blocks were proposed for the former, and the ‘pectoserratus’ or ‘deep pectoralis’ plane blocks for the latter.
Second round
The changes implemented for the second round led to ≥75% agreement being achieved for eight abdominal wall, three paraspinal, but none of the chest wall block names. There was ≥75% agreement in the anatomical descriptions in 11, 3 and 9 block approaches in the same categories, respectively. Full results of the second round are shown in figure 2 and online supplemental appendix 1.
Collaborators were asked three additional clarifying questions in this second round. The first question asked whether the anatomical locations of injection for the posterior TAP, lateral quadratus lumborum, and transversalis fascia plane blocks were similar enough to warrant harmonization. The second question asked whether the anatomical locations of injection for the PECS II and deep SAP blocks were similar enough to warrant harmonization. The third question aimed to clarify whether the term used to describe the connective tissue plane that is targeted in these regional anesthesia techniques (the superficial, deep or muscle-related planes composed of connective tissue) should be ‘fascial plane’, ‘interfascial plane’, or simply ‘plane’. None of the clarifying questions achieved strong consensus in responses (online supplemental appendix 1).
Third round
For abdominal wall blocks, the virtual round table led to strong consensus being achieved for the majority of block approaches. There was weak consensus on harmonizing the posterior TAP and lateral quadratus lumborum blocks (73%) into a single term, with strong consensus for lateral quadratus lumborum block as this unified term (80%). For the paraspinal blocks, there was also strong consensus on harmonizing the STIL, MTP, MIC, and CTF block techniques (84%) and strong consensus for the unified anatomical description (86%). However there was only weak consensus on accepting ITP (58%) rather than MTP (42%) as the unified name. There was weak or no consensus on both the names as well as anatomical descriptions of the lumbar longissimus and multifidus plane block. The rhomboid intercostal plane block achieved weak consensus for the name (69%) but strong consensus for the anatomical description (81%). For chest wall blocks, the deep and superficial SAP blocks achieved strong consensus on the names, with 91% and 80% agreement, respectively. However, the anatomical description for the superficial SAP block only achieved weak consensus (52%). There was only weak consensus on the interpectoral plane block name (73%), although this was higher than the alternative proposal of superficial pectoralis minor block (56%). There was weak consensus on the pectoserratus plane block name (53%), but no consensus on deep pectoralis minor block (46%). Finally, there was strong consensus (78%) that the superficial, deep, or muscle-related planes composed of connective tissue should be called fascial planes rather than interfascial planes (clarifying question three), although this does not apply to names, but only in reference to anatomical descriptions. The final results can be seen in table 1.
Consensus achieved for the block names. Strong consensus (≥75% agreement) was achieved for all block names except for rhomboid intercostal plane block, intertransverse process block, interpectoral plane block, and pectoserratus plane block, that had a weak consensus (50%–74% agreement)
Discussion
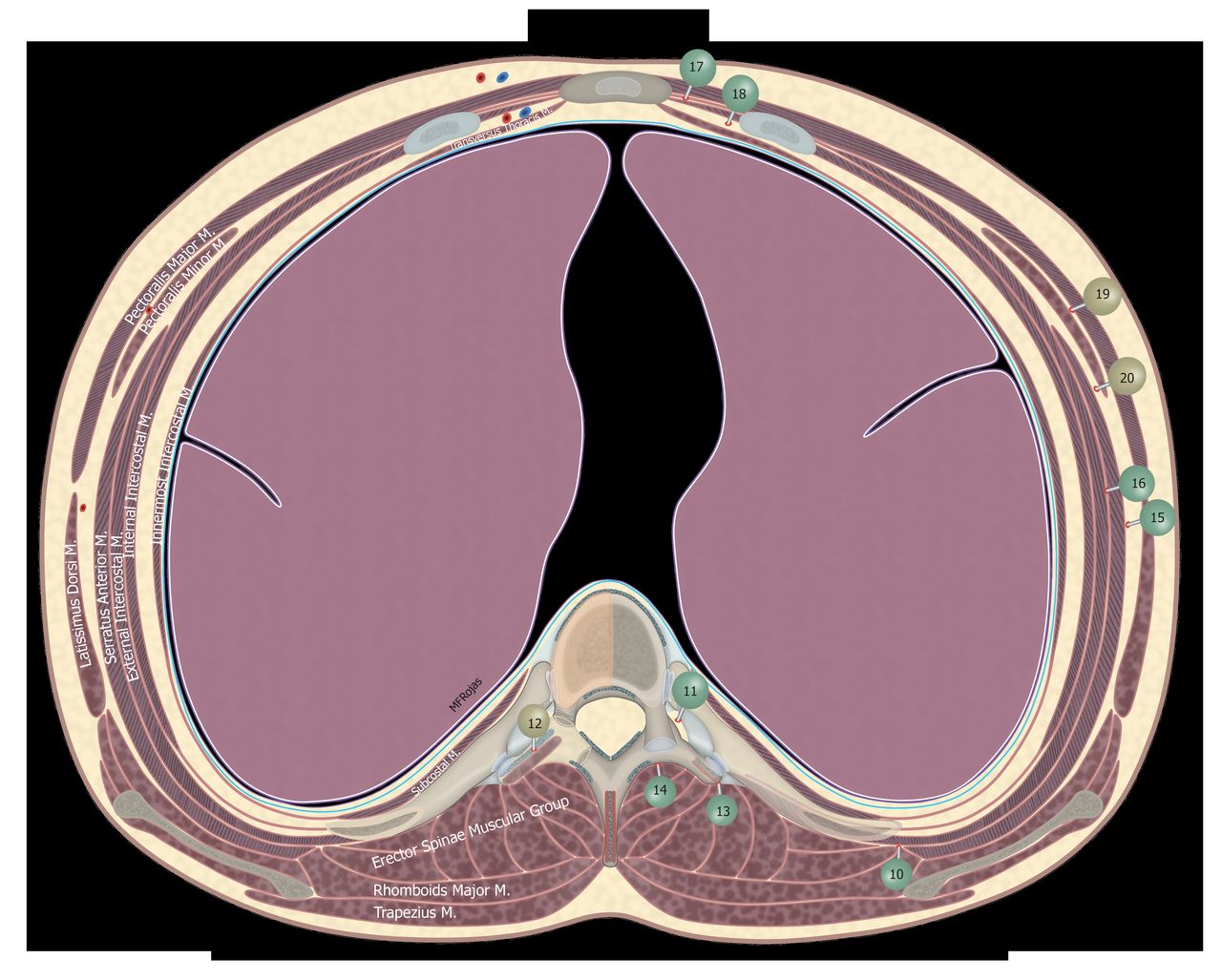
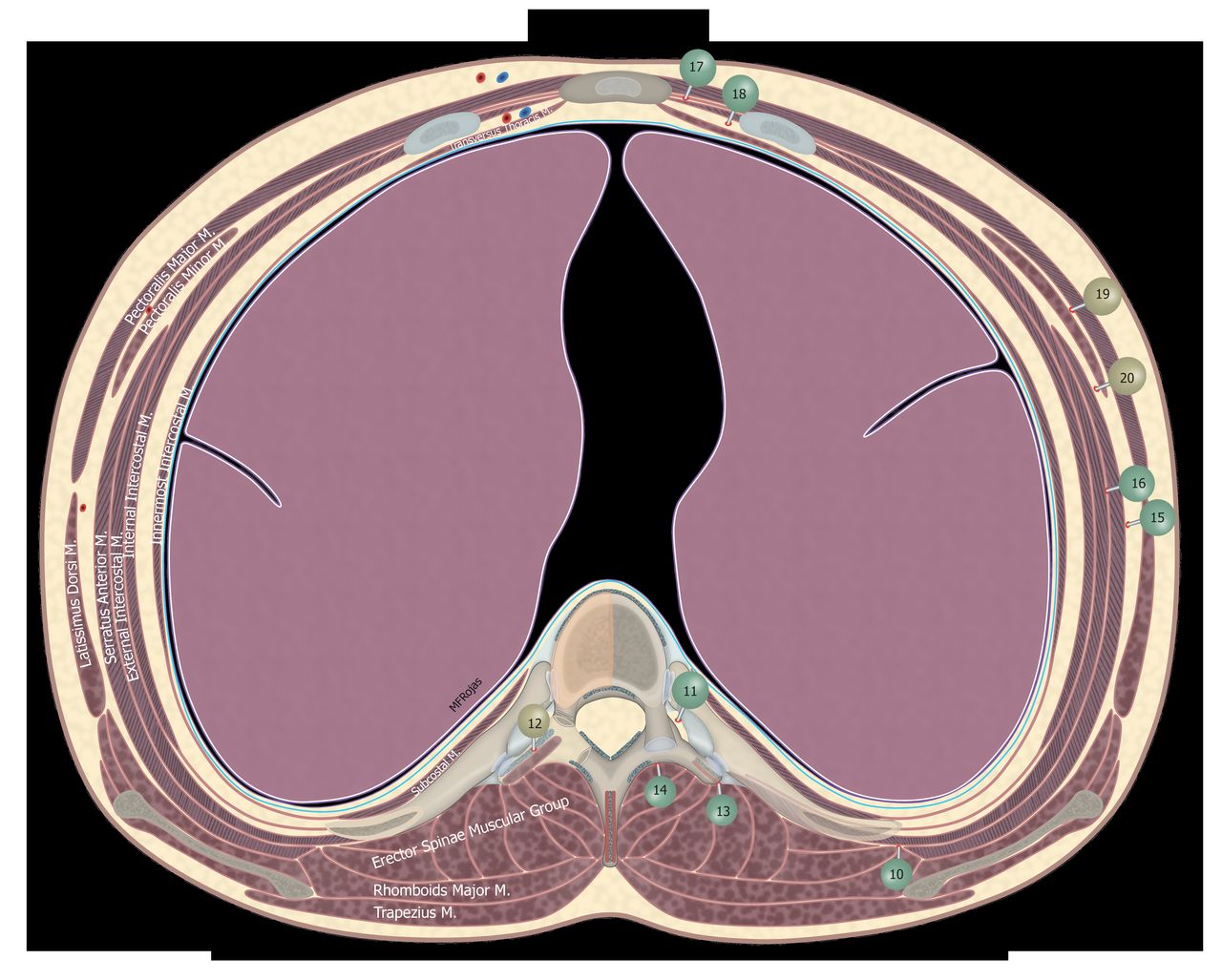
Ultrasound-guided regional anesthesia has widely evolved with the description of a myriad of new blocks. While the authors of the initial descriptions have to be praised for their contribution to the development of the specialty, the absence of consistency in the names given to these novel approaches hinders teaching, academic research, and the dissemination of the regional anesthetic techniques for patient benefit. The aim of this project was to standardize nomenclature of abdominal wall (figure 3), paraspinal (figure 4), and chest wall (figure 4) regional anesthetic techniques. In this first ASRA-ESRA international nomenclature Delphi study involving a collaboration of 60 international experts, the names of blocks of the trunk were condensed from 77 to 20. There was strong consensus from the collaboration on the names of 16 blocks and weak consensus for the remaining 4, these being the rhomboid intercostal plane block, the intertransverse process block, the interpectoral plane block, and the pectoserratus plane block (figure 4). Strong consensus was achieved on the anatomical descriptions of 19 of the included blocks, with weak consensus on the description of the superficial SAP block.
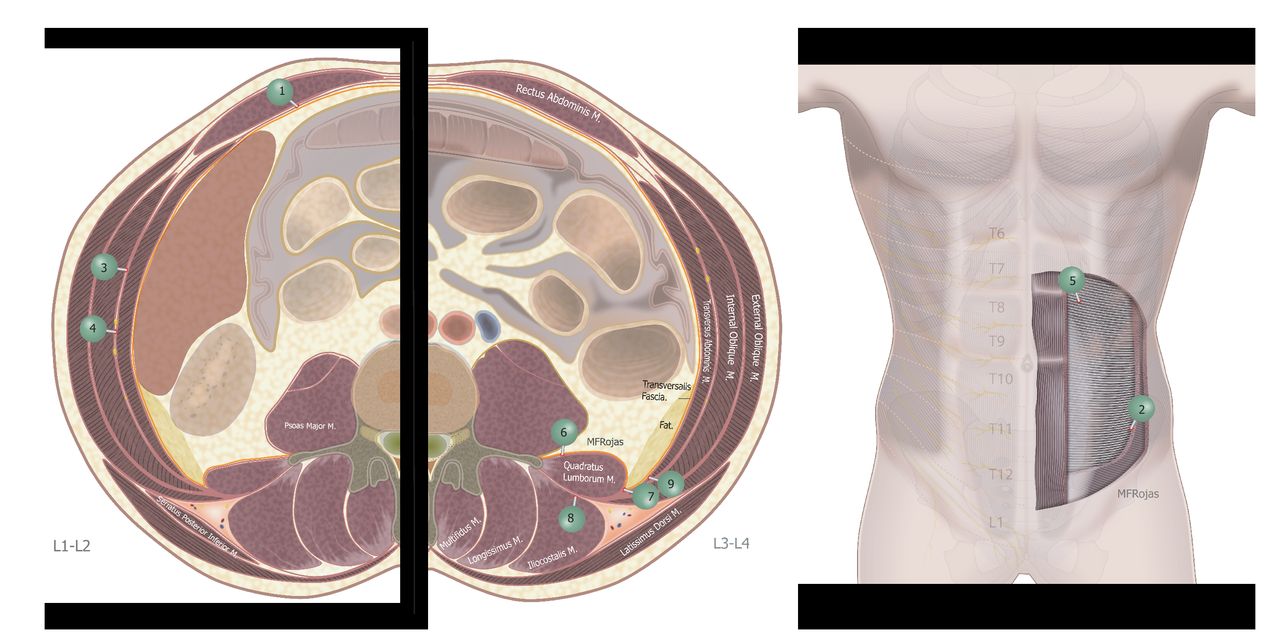
Illustrations of recommended names and anatomical locations of injection for abdominal wall. (1) Rectus sheath block; (2) ilioinguinal iliohypogastric nerves block; (3) transverse abdominis plane (TAP); (4) midaxillary TAP block; (5) subcostal TAP block; (6) anterior quadratus lumborum block (QLB); (7) lateral QLB; (8) posterior QLB; (9) transversalis fascia plane block.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Illustrations of recommended names and anatomical locations of injection for paraspinal and chest wall. Green circles represent strong consensus, yellow circles represent weak consensus. (10) Rhomboid intercostal plane block; (11) paravertebral block; (12) intertransverse process block; (13) erector spinae plane block; (14) retrolaminar block; (15) superficial serratus anterior plane (SAP) block; (16) deep SAP block; (17) superficial parasternal intercostal plane (PIP) block; (18) deep PIP block; (19) interpectoral plane block; (20) pectoserratus plane block.
The guiding principles of the project included not only harmonization of nomenclature, but also a preference for anatomically-descriptive block names wherever possible. In several instances, this prompted the Steering Committee to propose a new unified name for several related techniques. In the first example, the intertransverse process block was proposed as a term to encompass the midpoint transverse process to pleura, and its successors; the rationale being that the new name accurately described the injection site in all the techniques. However, weak consensus was achieved on this new name, with the remaining Collaborators favoring the MTP block. Another notable example pertains to the PECS I and II blocks. These techniques, while established in practice and the literature, nevertheless remain potentially confusing with regard to their name and description. PECS I is a single injection between pectoralis major and minor, and PECS II is a PECS I plus a second injection deep to pectoralis minor; yet many physicians continue to believe that PECS II consists only of a single deep injection.44 45 In the interests of arriving at consistent and anatomically descriptive nomenclature, the names interpectoral plane block and pectoserratus plane block were recommended to replace PECS I and the second injection of PECS II, respectively. There was weak consensus from the collaboration on these new names. Based on these recommendations, the original PECS II block should now be referred to as a combination of interpectoral and pectoserratus plane blocks. A third example is the rhomboid intercostal subserratus plane block,32 which was highlighted as a source of confusion since, like the PECS II block, it involves two separate injections: one into the plane between the rhomboid muscles and either ribs or external intercostal muscles, and a second one between the serratus anterior and either ribs external intercostal muscle. Again, in the interests of consistency, clarity, and harmonization, the name rhomboid intercostal plane block was adopted based on weak consensus by the collaboration, and describes a single injection in the plane between the rhomboid major and intercostal muscles. In following this recommendation, the original rhomboid intercostal subserratus plane block should now be described as a rhomboid intercostal plane block plus a deep SAP block. Finally, with regard to the superficial SAP block, there was strong consensus regarding naming, however there was weaker consensus on its description as an injection into the plane superficial to the serratus anterior muscle, rather than as an injection into the plane separating the serratus anterior muscle and the pectoralis major muscle. However, the collaboration recommends the former description as it is less restrictive, given that the superficial SAP block may be performed in or posterior to the midaxillary line, where this same plane separates the serratus anterior muscle from the latissimus dorsi muscle.
It is important to emphasize that this project does not aim to diminish the academic contributions by the researchers who described and investigated the original techniques. Indeed they must be commended for their contributions to the evolution of the discipline of regional anesthesia, and the impact this has had on advancing patient care. However, the collaboration considers that adoption of a universal nomenclature with harmonized language is essential for clarity in scientific discussion and clinical education, which in turn can only serve to improve the dissemination of these regional anesthetic techniques for patient benefit. We note that consensus from more than 50% of experts in this collaboration was achieved for all of the presented block names and anatomical descriptions, and we therefore believe it would be reasonable for clinicians and investigators to adopt this simplified and unified schema going forward. We aim to reconvene the consensus every 5 to 10 years as the evidence evolves. We would also aim for a similar process to be undertaken to achieve consensus in nomenclature and descriptions for upper and lower extremity regional anesthetic techniques.
There are limitations to this study, many of which relate to the use of the Delphi methodology. First, there are no clear methodological guidelines for the use of the Delphi method in the harmonization of nomenclature, nor evidence of reliability. This could potentially mean that the same questions presented to the same panel of experts may lead to a different consensus if asked at a different time. However, the Delphi technique is a recognized method for achieving consensus, and guidelines exist in the perioperative specialties for agreement of core outcome measures.46 47 Indeed, the Delphi method has been used within regional anesthesia previously48 and is likely to continue to be an important method to obtain consensus in areas that warrant clarity.49–51 A further limitation is that there were some areas in which no consensus was achieved on specific named blocks (box 1), and these remain areas in which further research is required, both to understand the techniques as well as to clarify and harmonize the lexicon. Moreover, we had defined consensus as 75% agreement a priori, but iteratively qualified this after the third round as either weak or strong consensus, which must be considered when interpreting our results. In addition, the anatomical reference points used throughout this nomenclature project had inconsistencies, being muscles, fascial planes, or other anatomical structures for different approaches. This project did not seek to examine clinical utility of any of the included approaches, but we hope this work will aid in standardizing future studies aiming to improve patient outcomes. Finally, this continues to be an evolving field, and as our understanding of regional anesthesia continues to develop, so too must the language that we use. Therefore, this project should not be viewed as definitive, but rather a starting point and template for future developments. Furthermore, this process will require re-evaluation in the future to ensure that the language we use remains current.
Abdominal wall, chest wall, or paraspinal regional anesthetic techniques that have names warranting further research
Thoracoabdominal nerves through perichondral approach
External oblique fascial plane block
Thoracolumbar interfascial plane block
Lateral / modified thoracolumbar interfascial plane block
Cervical interfascial plane block
Multifidus cervicis plane block
Cervical intersemispinalis plane block
Paraspinal interfascial plane blocks
Moving forward, clinicians developing novel regional anesthetic approaches should consider fundamental principles that would benefit readers, clinicians, educators, researchers, and patients. Novel techniques that have minimal or immaterial differences in the position of needle tips when compared with existing techniques should strongly be considered to be subtypes of the existing technique. This will reduce replication of work and maximize harmony. Just as important, any new nomenclature should be simple, clear, anatomically descriptive, and based on the location of the needle tip in relation to key surrounding landmarks, rather than any other details of procedural performance (eg, needle trajectory, ultrasound probe position, vertebral level). It remains unclear whether this should be based on fascial planes, related muscles, other anatomical landmarks, or indeed target neural structures. This should be an area of future investigation.
In conclusion, harmonization and standardization of nomenclature will potentially improve teaching and the research of the regional anesthetic techniques, ultimately resulting in dissemination that will benefit patient care. Therefore, these standards in nomenclature and definitions are recommended for use in clinical and academic practice in the future.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Acknowledgments
We thank Chelsea C Banks and Youxin Guan (New York Medical College, Valhalla, New York, USA) for their assistance in sourcing original papers.
References
Footnotes
Twitter @elboghdadly, @DrEAlbrecht, @kaohesham, @EMARIANOMD, @sanjibadhikary, @CarvalB, @AlwinChuan, @Steve_Coppens, @rljohnsonmd, @claralexlobo, @gamcleod2, @PeterMerjavy, @amit_pawa, @PerlasAnahi, @ESoffin, @Ropivacaine, @nelkassabany
Contributors Study conception and design: KE, EA, NE, SK, ERM, MW. Study conduct: KE, EA, KJC, NE, HE, SK, ERM, AS, JLX. Data analysis: KE, AS. Manuscript preparation: KE, EA. Manuscript revision: KE, NE, AS, ERM, MW, SK, KJC, HE, JLX, EA. Manuscript approval: All authors
Funding This project was supported and approved by both ASRA and ESRA boards of directors. Administrative support for the project was provided by ASRA.
Competing interests IC reports being the first author of original description of the MTP block. PH reports being the original describer of several of the blocks considered. AP receives funding from a Merit Award from the Department of Anesthesiology and Pain Medicine, University of Toronto.
Provenance and peer review Commissioned; externally peer reviewed.