Article Text

Abstract
Background This cadaveric study investigated the innervations of the clavicle and clavicular joints (ie, sternoclavicular and acromioclavicular joints).
Methods Twenty cadavers (40 clavicles) were dissected. A skin incision was made to permit exposure of the posterior cervical triangle and infraclavicular fossa. The platysma, sternocleidomastoid, and trapezius muscles were cleaned in order to identify the supraclavicular nerves. Subsequently, the suprascapular and subclavian nerves were localized after removal of the prevertebral layer of the deep cervical fascia. In the infraclavicular region, the pectoralis major and minor muscles were retracted laterally in order to visualize the lateral pectoral nerve. The contribution of all these nerves to the clavicular bone and joints were recorded.
Results Along their entire length, all clavicular specimens received contributions from the supraclavicular nerves. The latter innervated the cephalad and ventral aspects of the clavicular bone. The caudal and dorsal aspects of the clavicle were innervated by the subclavian nerve (middle and medial thirds). The lateral pectoral nerve supplied the caudad aspect of the clavicle (middle and lateral thirds). The sternoclavicular joint derived its innervation solely from the supraclavicular nerves whereas the acromioclavicular joint was supplied by the supraclavicular and lateral pectoral nerves.
Conclusion The clavicle and clavicular joints are innervated by the subclavian, lateral pectoral, and supraclavicular nerves. Clinical trials are required to determine the relative importance and functional contribution of each nerve.
- upper extremity
- pain management
- nerve block
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Not applicable.
Statistics from Altmetric.com
Introduction
The innervation of the clavicle remains controversial and has been alternately attributed to the long thoracic, suprascapular, subclavian, lateral pectoral, or supraclavicular nerves.1 2 Paradoxically, most descriptions of clavicular innervation can be traced back (with modifications) to a single source: a 1914 French neurology book authored by Jules Dejerine.3 Unfortunately, the latter provided no methodology (cadaveric dissection vs redrawing from previous sources) to support his findings. Thus, a 2013 Daring Discourse recommended further investigation to elucidate the innervation of clavicle.1 In the last 8 years, multiple reports have advocated various combinations of cervical root, cervical plexus, and brachial plexus blocks (eg, interscalene, supraclavicular, upper trunk approach) to provide anesthesia/analgesia for clavicular surgery.4–14 From a methodological standpoint, these reports provide limited insight into the clavicle’s innervation, as cervical root and brachial plexus blocks anesthetize multiple terminal nerves at once. Even PECS block, which target lateral pectoral nerves,2 15 16 may prove beneficial for clavicular surgery through local anesthetic diffusion to the (infraclavicular) brachial plexus.16
Consequently, this cadaveric study investigated the innervation of the clavicle and clavicular joints (ie, sternoclavicular and acromioclavicular joints). Particular attention was paid to the long thoracic, suprascapular, subclavian, lateral pectoral and supraclavicular nerves.1 2
Material and methods
Ethics exemption (Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand) was secured on January 5, 2021 prior to the start of the study. The latter took place over a period of seven and a half months (February 1, 2021 to September 13, 2021). All fresh adult human cadavers were donated to the Department of Anatomy of Chiang Mai University. Cadavers with previous clavicular or shoulder surgery were excluded from the current study. For each cadaver, the two clavicles were treated as separate entities (ie, cadaveric specimens).
Cadaveric dissection
All dissections were carried out by four investigators working conjointly (PL, NM, PK, PN). To permit exposure of the posterior cervical triangle, a skin incision was made along the mandible and anterior borders of the sternocleidomastoid and trapezius muscles. The platysma, sternocleidomastoid, and trapezius muscles were cleaned in order to identify the trapezius branch of the cervical plexus as well as the spinal accessory and supraclavicular nerves. The prevertebral layer of the deep cervical fascia was then removed to visualize the deep structures of the neck. The suprascapular and subclavian nerves were identified and carefully preserved.
In the infraclavicular region, skin incisions were made from the sternal notch the xiphoid process and along the costal margin. The pectoralis major and minor muscles were retracted laterally. The three cords of brachial plexus, the lateral pectoral nerve, and the long thoracic nerve were identified and preserved.
Neural contribution to each third (ie, medial, middle, or lateral third) and aspect (ie, cephalad, caudad, ventral, or dorsal aspect) of the clavicle was recorded. Furthermore, neural contribution to the two clavicular joints (ie, sternoclavicular and acromioclavicular joints) was also documented.
Sample size and statistical analysis
A convenience sample consisting of 20 cadavers (40 clavicles) was selected a priori. Statistical analysis (ie, count and proportion) was purely descriptive in nature.
Results
As planned, 20 cadavers (40 clavicles) were dissected. Demographic data of the cadavers are presented in table 1.
Demographic data of cadavers (N=20)
Innervation of the clavicle
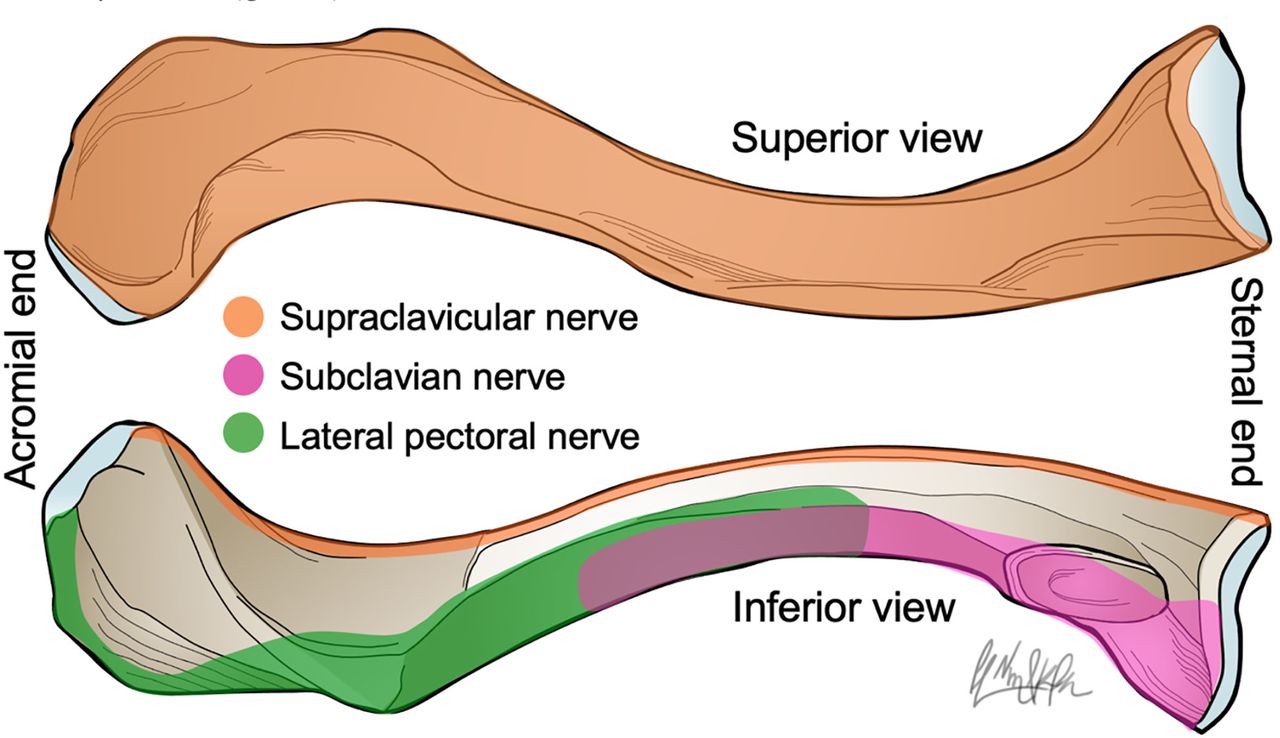
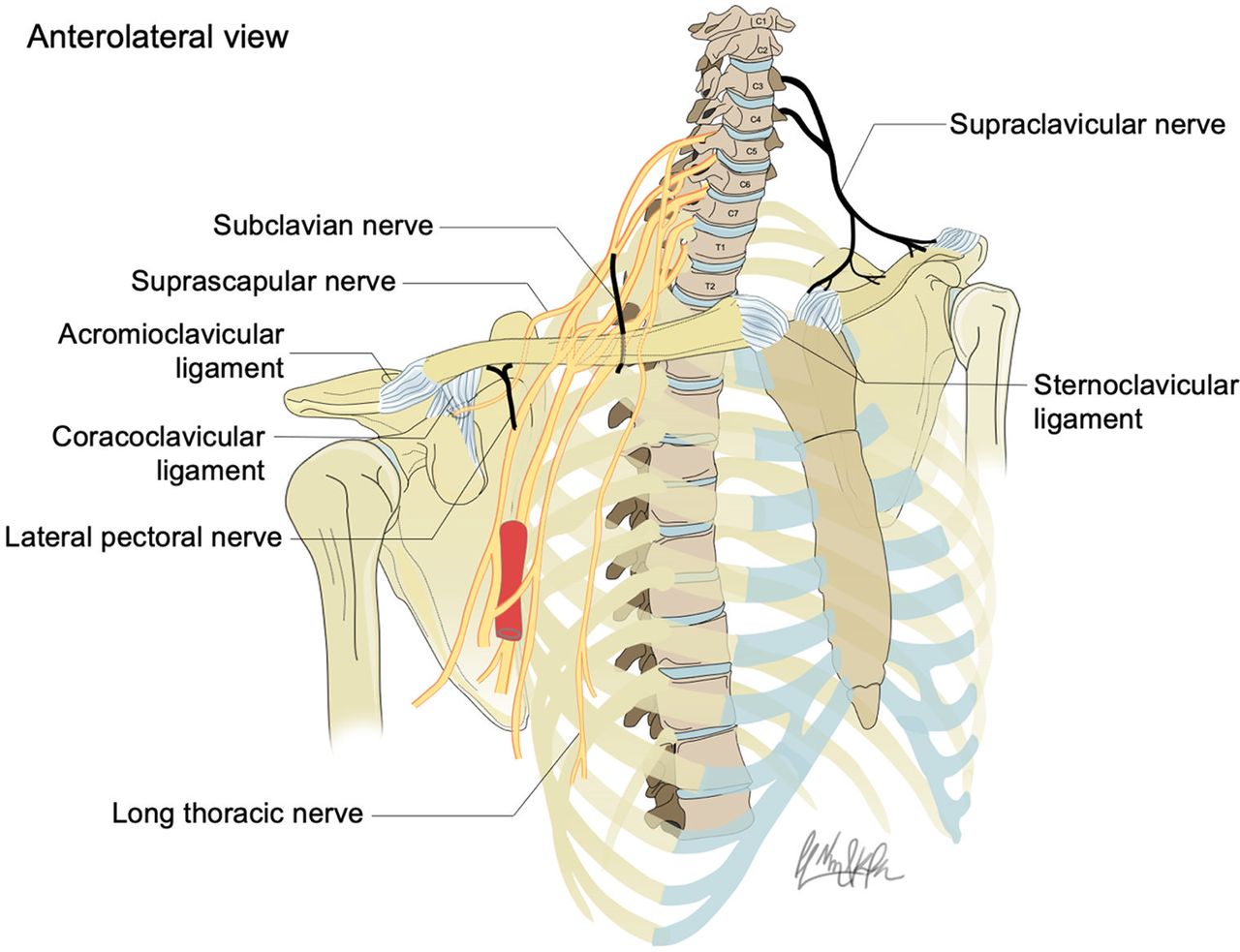
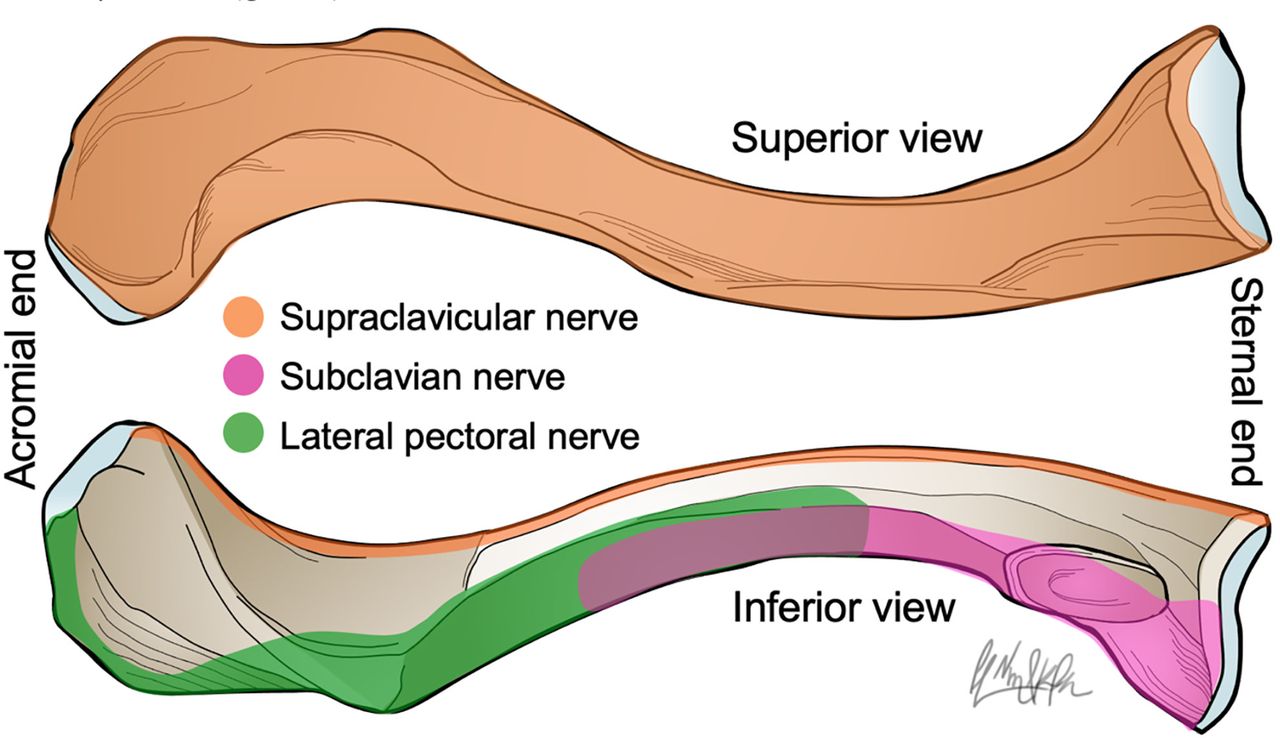
Along their entire length, all clavicular specimens received contributions from the supraclavicular nerves. The latter supplied the cephalad and ventral aspects of the clavicular bone. The caudal and dorsal aspects of the clavicle were innervated by the subclavian nerve (middle and medial thirds). The lateral pectoral nerve supplied the caudal aspect of the clavicle (middle and lateral thirds) (table 2; figures 1–3). A bony strip was found on the caudal aspect of the clavicle where there existed no direct contact between bone and nerves or muscles (figure 3).

Nerves innervating the clavicle and periclavicular joints. (A) Anterior view of the posterior cervical triangle. (B) Lateral view of the infraclavicular region.
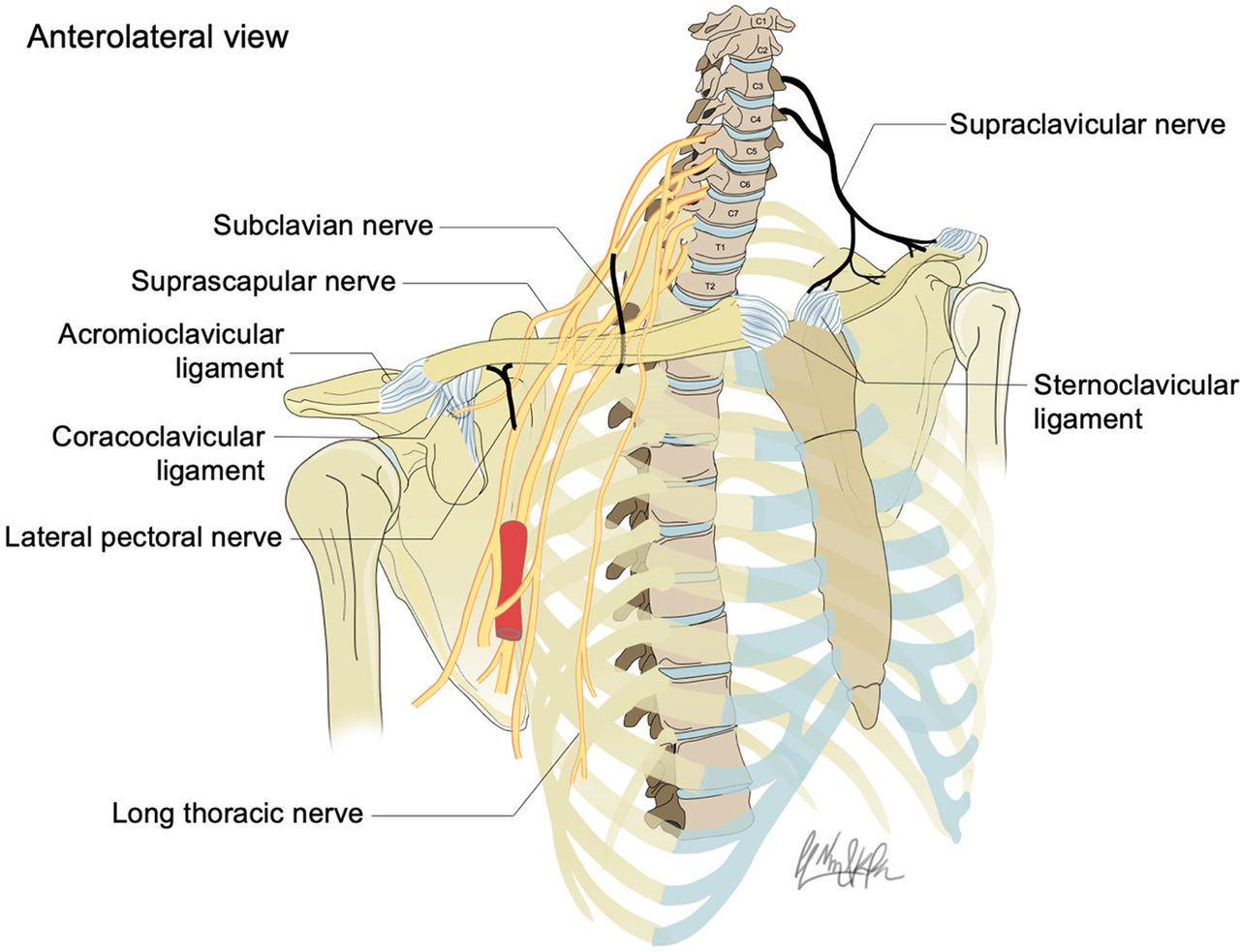
Schematic illustration of nerves supplying the clavicle and periclavicular joints.
{kind=link}
{kind=link}
{kind=link}
Areas of the clavicle innervated by the supraclavicular (orange), subclavian (pink), and lateral pectoral (green) nerves.
Innervation of the clavicle
The trapezius branches of the cervical plexus as well as the spinal accessory, long thoracic, and suprascapular nerves provided no innervation to the clavicle.
Innervation of the sternoclavicular and acromioclavicular joints
The sternoclavicular joint derived its innervation solely from the supraclavicular nerves whereas the acromioclavicular joint was supplied by the supraclavicular and lateral pectoral nerves. We found no significant contribution from the trapezius branch of the cervical plexus nor the spinal accessory, subclavian, long thoracic, and suprascapular nerves (figures 1–3).
Discussion
In this cadaveric study, we found that the subclavian, lateral pectoral, and supraclavicular nerves all contributed to the innervation of the clavicle. Furthermore, the supraclavicular and lateral pectoral nerves supplied the sternoclavicular and/or acromioclavicular joints. Contrary to Dejerine’s claim,3 we detected no significant contribution from the long thoracic nerve. Similarly, we could not validate the hypothetical involvements of the trapezius branches of the cervical plexus, the spinal accessory nerve or the suprascapular nerve.17
The supraclavicular nerves can be easily anesthetized using an ultrasound-guided intermediate cervical plexus block.7 18 Knowledge of the involvement of the subclavian nerve (which originates from the upper trunk) and lateral pectoral nerve (which originates from the lateral cord) could help select the optimal approach for brachial plexus blockade. While cervical root and interscalene blocks remain reliable, they may no longer be required due to the minimal role played by the long thoracic nerve. Instead, more distal approaches (eg, supraclavicular brachial plexus block, upper trunk block) provide possible options that offer potential benefits such a decreased risk of puncturing periforaminal vessels19 and a lower incidence of phrenic nerve block.20 Our results fail to support the use of PECS blocks: even if local anesthetic were to spread to the (infraclavicular) brachial plexus,2 they would spare the upper trunk thereby ignoring the contribution of the subclavian nerve.
The bony strip located on the caudal aspect of the clavicle, which was not attributed to any nerve (figure 3), deserves special mention. In our dissections, in this area of the clavicle, we found no direct contact between bone and muscle or nerve. Thus, we erred on the side of caution and refrained from assigning the territory to a specific nerve. Nonetheless, this dorsal strip of the clavicle may not be entirely devoid of peripheral innervation. For instance, its sensory supply could stem from subperiosteal neural twigs originating from the nerves that supply neighboring areas. This remains speculative and requires confirmation (or infirmation) with neurohistopathology studies.21
The innervation of the sternoclavicular and acromioclavicular joints also require discussion. In our study, in the majority of cases, the supraclavicular and lateral pectoral nerves supplied one or both joints. However, in 13%–15% of cadaveric specimens, we could not locate any neural twigs supplying either joint (table 3). We hypothesize that these small branches could have been inadvertently cut during the dissection process and could have also originated from the supraclavicular or lateral pectoral nerves. Nonetheless, we cannot exclude the possibility that the cut branches could derive from alternate nerves such as the subclavian nerve (sternoclavicular joint)22 or the suprascapular nerve (acromioclavicular joint).23 Fortunately, this residual uncertainty minimally impacts the analgesic management of clavicular fractures since nerve blocks performed to anesthetize the clavicular shaft (ie, intermediate cervical plexus block combined with interscalene, supraclavicular, or upper trunk brachial plexus block) would also anesthetize the clavicular joints irrespective of their innervation (supraclavicular, subclavian, suprascapular, or lateral pectoral nerves).
Innervation of the sternoclavicular and acromioclavicular joints
Our protocol contains some limitations. First, our sample size (40 clavicles) was relatively small: thus, we cannot rule out possible anatomical variations (and contributions from other nerves). Second, an anatomical dissection represents a comprehensive but static survey. It provides minimal insight into the relative importance and the functional contribution of each nerve.1 Thus, clinical trials are required to compare isolated cervical plexus block, isolated brachial plexus block, and combined cervical–brachial plexus block.1 Although a recent study24 has attempted to answer the question, its conclusions were hindered by a lack of research hypothesis and sample size justification as well as discrepancies between the registered and reported protocols (in terms of sample size and primary outcome). Future investigation should also validate the possible benefits of clavipectoral fascial plane block, which purportedly targets terminal neural branches in the periclavicular region.25
In summary, the clavicle and clavicular joints are innervated by the subclavian, lateral pectoral, and supraclavicular nerves, and thus, are amenable to combined (intermediate) cervical plexus block with upper trunk or supraclavicular brachial plexus block. Clinical trials are required to determine the relative importance and functional contribution of each nerve.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Not applicable.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank the Excellence in Osteology Research and Training Center (ORTC), Chiang Mai University, Chiang Mai, Thailand for their support.
References
Footnotes
Contributors PL, NM, PK, PN, and PM participated in the planning, conception, design, conduct, reporting, acquisition of data, data analysis, and interpretation of data. DQT participated in the planning, conception, design, data analysis, and interpretation of data. PL is a guaranter reponsible for the overall content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.