Article Text

Abstract
Background Evidence-based international expert consensus regarding the impact of peripheral nerve block (PNB) use in total hip/knee arthroplasty surgery.
Methods A systematic review and meta-analysis: randomized controlled and observational studies investigating the impact of PNB utilization on major complications, including mortality, cardiac, pulmonary, gastrointestinal, renal, thromboembolic, neurologic, infectious, and bleeding complications.
Medline, PubMed, Embase, and Cochrane Library including Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, NHS Economic Evaluation Database, were queried from 1946 to August 4, 2020.
The Grading of Recommendations Assessment, Development, and Evaluation approach was used to assess evidence quality and for the development of recommendations.
Results Analysis of 122 studies revealed that PNB use (compared with no use) was associated with lower ORs for (OR with 95% CIs) for numerous complications (total hip and knee arthroplasties (THA/TKA), respectively): cognitive dysfunction (OR 0.30, 95% CI 0.17 to 0.53/OR 0.52, 95% CI 0.34 to 0.80), respiratory failure (OR 0.36, 95% CI 0.17 to 0.74/OR 0.37, 95% CI 0.18 to 0.75), cardiac complications (OR 0.84, 95% CI 0.76 to 0.93/OR 0.83, 95% CI 0.79 to 0.86), surgical site infections (OR 0.55 95% CI 0.47 to 0.64/OR 0.86 95% CI 0.80 to 0.91), thromboembolism (OR 0.74, 95% CI 0.58 to 0.96/OR 0.90, 95% CI 0.84 to 0.96) and blood transfusion (OR 0.84, 95% CI 0.83 to 0.86/OR 0.91, 95% CI 0.90 to 0.92).
Conclusions Based on the current body of evidence, the consensus group recommends PNB use in THA/TKA for improved outcomes.
Recommendation: PNB use is recommended for patients undergoing THA and TKA except when contraindications preclude their use. Furthermore, the alignment of provider skills and practice location resources needs to be ensured. Evidence level: moderate; recommendation: strong.
- nerve block
- regional anesthesia
- acute pain
- treatment outcome
- postoperative complications
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Systematic review and meta-analysis.
Statistics from Altmetric.com
Introduction
Total hip and knee arthroplasties (THA/TKA) are among the most common surgeries in the developed world1 with large increases projected as the population ages.2 Despite representing value-based solutions to end-stage arthritis,3 THA/TKA patients are at risk for serious complications of major organ systems.4 The identification of risk-modifying, perioperative interventions has therefore become a clinical priority.
Besides the well-established intrinsic benefits of regional anesthesia,5 a growing body of evidence has indicated that anesthetic technique and in particular peripheral nerve blockade (PNB) may favorably influence perioperative outcome in terms of serious complications. Here, evidence from randomized controlled trials (RCTs) has been complemented by large population-based data because of the typical lack of precision when investigating the occurrence of harm.6–9
Observational evidence is well established in the context of serious harm because such complications are rare and often not captured during the follow-up of RCTs.10 11 In such settings issues of imprecision, indirectness, or inapplicability may prevent RCT’s from providing high-quality evidence in respect to adverse, unexpected events.12 13
The current analysis is a follow-up of a previous systematic review by the ICAROS group (International Consensus on Anaesthesia-Related Outcomes after Surgery) recommending neuraxial anesthesia for reduced complications in THA/TKA.14
Objective
Recognizing the intrinsic benefits of PNBs, the objective was to address the impact of PNB use on serious perioperative complications.11 The ICAROS group therefore (1) conducted a systematic literature review with meta-analysis, (2) graded the level of evidence quality and (3) developed clinical practice recommendations. Given a relatively low PNB utilization in general,15 findings from this project are likely to profoundly impact on perioperative practice.
Methods
Consensus group
The ICAROS group was comprised 57 individuals with extensive expertise in perioperative research and care of the orthopedic patient. The group was expanded from its original roster to maximize the collective expertise, including anesthetists, orthopedic surgeons, healthcare outcomes and quality researchers, administrators, librarians, and methodologists from North America, Europe, and Oceania representing more than 20 nationalities and practicing in over 10 countries. A 10-member steering committee was tasked with overseeing day-to-day project aspects.
Study plan and healthcare question
According to the prespecified healthcare question, a systematic review and meta-analysis were performed to investigate the impact of PNB utilization on the occurrence of complications in patients undergoing THA/TKA. This is important because clinical recommendations should consider both, benefit and harm.10
As serious complications are relatively rare and are often not captured in RCTs, observational evidence was required to complement randomized evidence.10 12 16
The study protocol was registered on the International Prospective Register of Systematic Reviews PROSPERO (protocol number: CRD42018099935).17
Healthcare questions posed to the consensus group
Does the use of a PNB influence postoperative complications in patients undergoing THA?
Does the use of a PNB influence postoperative complications in patients undergoing TKA?
Outcomes of interest comprised major complications, considered critical to the patients postoperative health condition: inpatient and all-cause mortality, cardiac complications (without myocardial infarction (MI)), MI, pulmonary complications, respiratory failure, gastrointestinal and renal complications, acute renal failure, thromboembolism (deep venous thrombosis and pulmonary embolism), postoperative cognitive dysfunction, delirium, stroke, any systemic infectious complications, surgical site infections, blood loss, and transfusion requirements (both binary and in milliliters). Outcomes accounting for resource utilization included length of hospital stay (LOS), critical care admission, and cost of care. Outcome composition is detailed in online supplemental table A1.
Supplemental material
Study intervention and comparator
The study intervention, anesthesia with PNB use, comprised lumbar plexus block, psoas compartment nerve block, paravertebral block, femoral nerve block, fascia iliaca compartment block, three in one block (including the femoral, obturator, and lateral cutaneous nerves), sciatic nerve block, lateral femoral cutaneous nerve block, and adductor canal block.
The comparator was any anesthesia without PNB use. This involved systemic analgesia, intravenous analgesia, patient-controlled analgesia, intravenous patient-controlled analgesia, local infiltration analgesia (LIA), and periarticular local anesthetic infiltration.
Selection criteria
Based on the defined patient, intervention, comparator, and outcome (PICO) question, eligible studies included RCTs and observational prospective or retrospective studies of adult patients undergoing elective THA and TKA (in English language). Exclusion criteria included patients under 18 years of age and case reports.
Search strategy
A systematic literature search was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
The search strategy, including Medical Subject Headings (MeSH), keywords, and controlled vocabulary terms, was crafted and validated by the expert group in collaboration with two institutional librarians according to the healthcare question. Medline, PubMed, Embase, and the Cochrane Library including Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects, Cochrane Central Register of Controlled Trials, Cochrane Methodology Register, Health Technology Assessment Database, NHS Economic Evaluation Database, were queried from database inception (1946) to May 17, 2018 and subsequently repeated to include August 4, 2020 for a complete and up to date evidence synthesis.
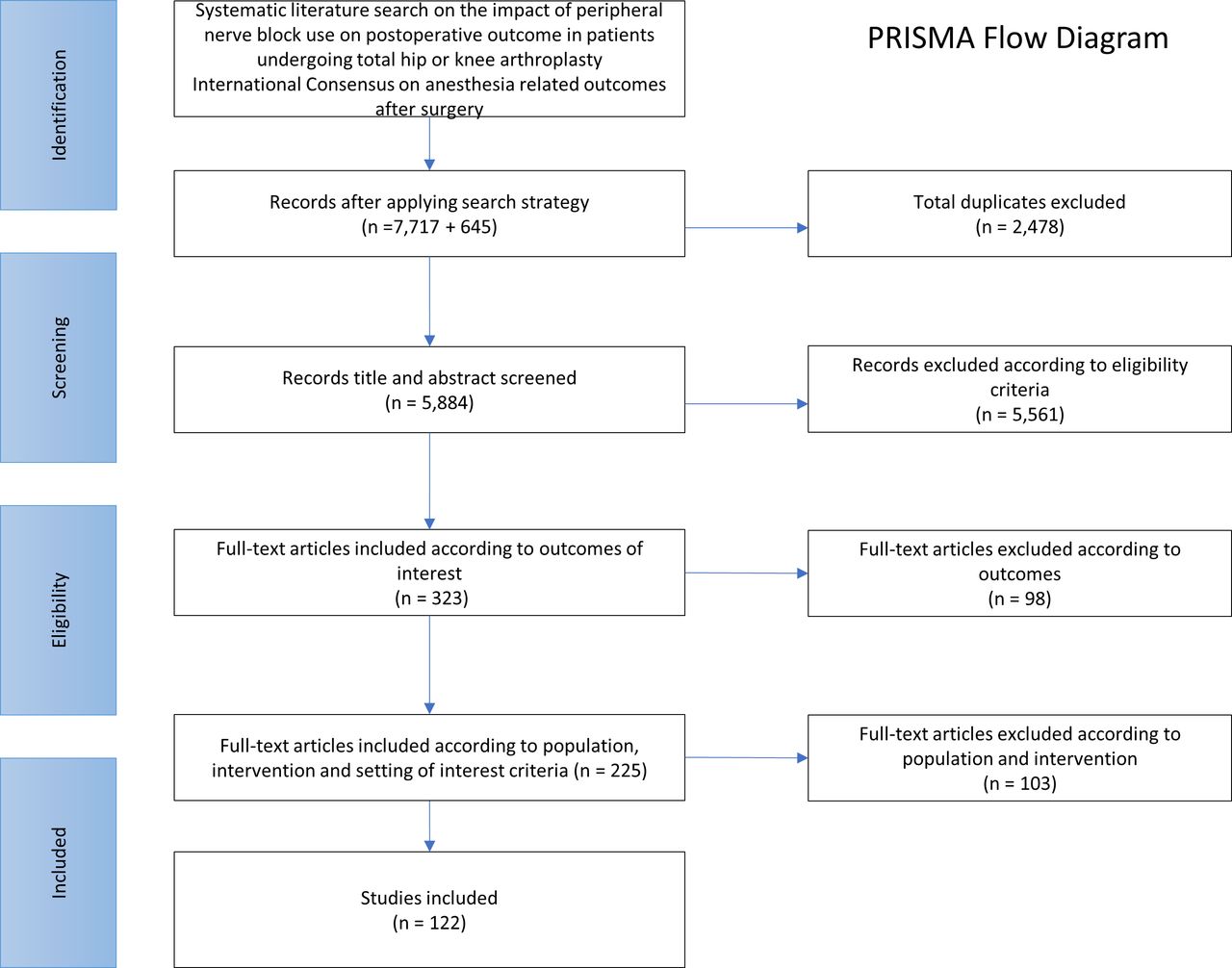
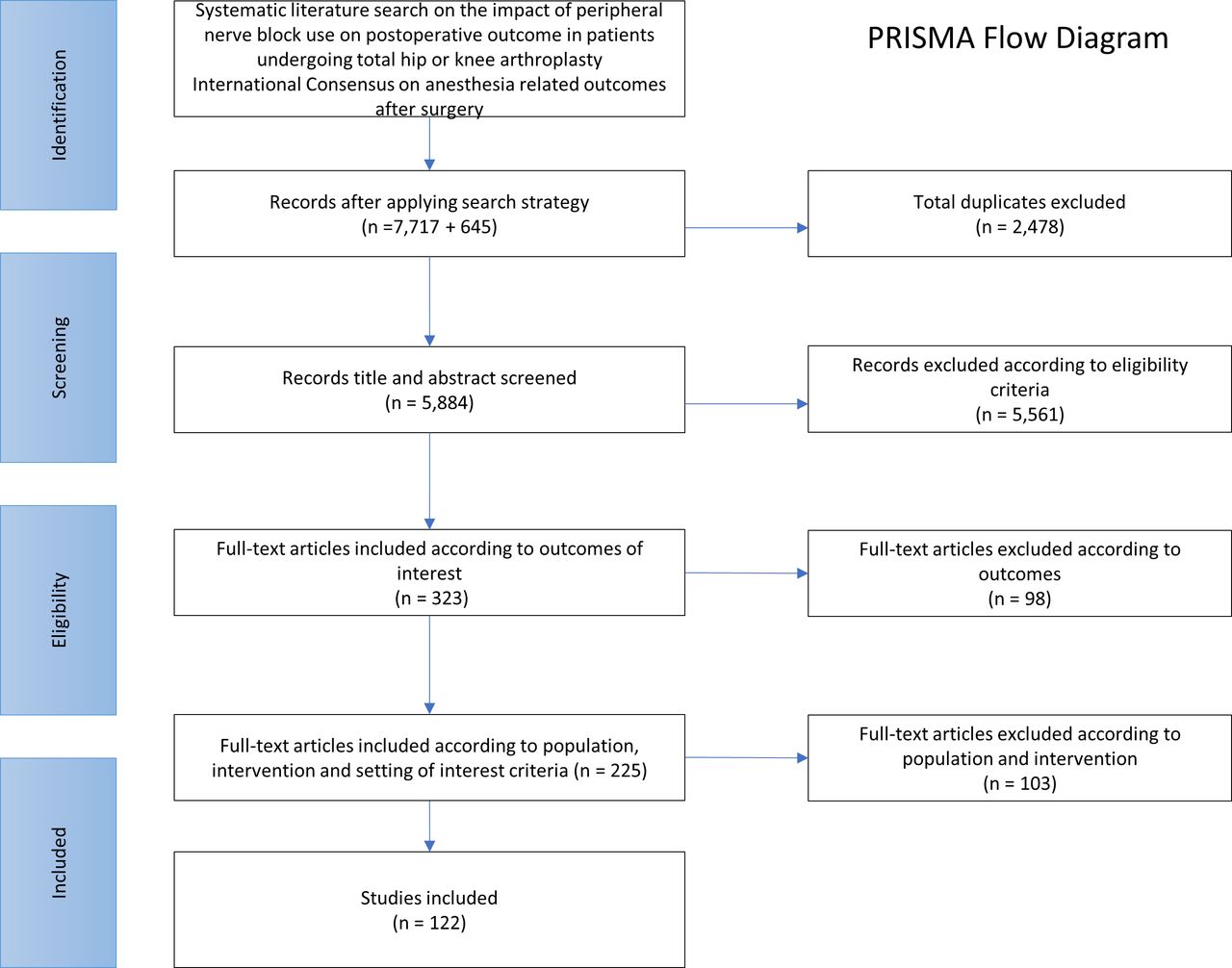
The full search strategy is reported in online supplementarl materials and can be found in online supplemental appendix A1. The search yielded 8326 studies. In addition to the electronic search, a manual search of previously published systematic reviews was performed for the purpose of completeness.
Study identification and data extraction
After removal of duplicates, abstracts of 5884 studies were extracted and imported into the Covidence webtool, a comprehensive framework facilitating abstract screening, full-text review, data extraction, and quality assessment.18 Each step was performed independently by two reviewers, including a third reviewer for disagreements. Extracted data were categorized according to prespecified outcomes and the preliminary risk of bias within individual studies was assessed according to the Cochrane Risk of Bias Tool for RCTs and the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) tool for non-randomized studies of interventions, respectively.19
The flow chart is presented in figure 1.
{kind=link}
Flowchart. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Quantitative analysis
To provide estimates of intervention effects,20 RCT and observational data were pooled by meta-analysis. Review Manager version 5 was used to facilitate data analysis and graphic presentation.21 Summary effect estimates for each outcome (ORs and 95% CIs) with heterogeneity (I2 statistic) were provided. For binary outcomes, group-specific risk was presented in events per 1000 while the relative effect was presented in ORs. For continuous variables, the effect was presented as mean difference.
Primary analysis
Effect estimates for the occurrence of critical complications with and without PNB utilization in THA and TKA, respectively.
Secondary analyses
Subgroup analysis based on study type, stratifying by RCT and observational evidence.
Subgroup analysis based on primary anesthesia technique, investigating potential differences in PNB effects based on the use of general anesthesia (GA), neuraxial anesthesia (NA), or a combination thereof as the primary anesthetic technique. (table 1) For this purpose, THA and TKA populations were merged to assure an adequate sample size. In general, primary anesthetic techniques were matched in the intervention and comparison groups.
Effect estimates comparing outcomes were stratified by the following groups:
GA only with and without PNB use.
GA+NA with and without PNB use.
Any study including GA, regardless of NA (sum of GA only and GA+NA) with and without PNB use.
NA only with and without PNB use.
Sensitivity analysis investigating the potential impact of clinical enhanced recovery after surgery (ERAS) pathways.22 23
Sensitivity analysis accounting for possible prognostic imbalance due to changes in the utilization of perioperative thromboembolic prophylaxis protocols (as performed in the previous project) was not necessary as all included studies were published after the common establishment of respective perioperative measures.23
Subgroup analysis based on primary anesthesia technique
Qualitative analysis
The GRADE system was used with the aim to provide meaningful evidence summaries and recommendations for the practice of evidence-based treatment at the point of care.24 25 This methodology of rating the quality of evidence and grading the strength of recommendations, has been widely adopted for the purpose of providing high-quality summaries of research evidence in systematic reviews and for standardized guideline development.26 GRADE offers a comprehensive framework allowing for a systematic and transparent assessment of the quality of the body of evidence as it relates to each individual outcome. The quality of evidence is specified in four levels of certainty (high, moderate, low, and very low) according to explicit criteria including, the seriousness of risk of bias as it affects an individual outcome across all contributing studies19 the seriousness of heterogeneity, imprecision, indirectness, and publications bias (funnel plots), all analyzed in their bearing and severity on each individual outcome, respectively.25 The rationale for upgrading the quality of evidence included large effect size, a dose–response relationship, or plausible confounders that would decrease an apparent treatment effect.27 Using the GRADEpro software package,28 final results including the pooled estimates of effect and the quality of evidence were presented in the summary of findings tables (tables 2 and 3 for THA and TKA, respectively).
GRADE summary of findings for total hip arthroplasty
The perioperative impact of anesthesia technique with or without peripheral nerve block use in total hip arthroplasty
Recommendations
According to GRADE, critical factors beyond the quality of evidence include the balance between benefit and harm, patient values and preferences, resource considerations, and issues pertaining to feasibility, equity, and acceptability of recommendations.20 29 The balance between desirable and undesirable outcomes and the application of patients’ values determines the direction of the recommendation. These factors, along with the quality of evidence, resource implications, and clinical feasibility considerations determine the strength of recommendations (strong/weak).20 24–26
Modified Delphi process and consensus
After completion of the analyses, two cohorts of participants were tasked with summarizing the evidence, formulating conclusions, and suggesting recommendations. This work was distributed in the form of white papers for THA and TKA, respectively. White papers together with detailed analysis data files and summary tables of results were distributed among the group, requesting anonymous edits and comments according to the modified Delphi process.30 Multiple reviews and revisions were performed to include all participants’ comments.31
Based on the novel coronavirus (COVID-19) outbreak, the in-person meeting scheduled for April 2020 in San Francisco, California, USA, was canceled. Group communication continued via email and conference phone calls. The final consensus decision and approval were assessed in an anonymous online voting process, which was preceded by group discussions and finalized statements.
Disclaimer
Conclusions and recommendations of this consensus are not intended to establish practice guidelines or standards, nor can they—if followed—guarantee successful outcomes. For numerous reasons clinicians or patients may deviate from the current recommendations, including but not limited to medical circumstances, individual patient and clinician preferences, training skills, local resource availability. Conclusions and recommendations are based on current literature at the time of the analysis thus, reassessment and revisions are required as new or differing evidence emerges.
Results
A total of 82 RCTs and 40 observational studies were included in the current analysis comprising more than 1 million patients undergoing THA/TKA. The odds for numerous serious postoperative complications were significantly lower with the use of PNBs.
Summary of findings tables, including pooled estimates of effect and quality of evidence provided in tables 2 and 3 for THA and TKA, respectively. Study characteristics including risk of bias are presented in online supplementary table A2. In-depth analysis including forest plots presented in online supplemental table A3.
Supplemental material
Supplemental material
Primary analysis
Perioperative impact of PNB use in THA
In THA patients, PNB use was associated with significantly reduced complication odds in most outcome categories. For the remaining complication endpoints, no difference in risk was observed. PNB use was not associated with any increase in complication odds (tables 2 and 4).
GRADE summary of findings for total knee arthroplasty
The perioperative impact of anesthesia technique with or without peripheral nerve block use in total knee arthroplasty
Decreased odds were found for cardiac complications (OR 0.84, 95% CI 0.76 to 0.93), pulmonary complications (OR 0.70, 95% CI 0.60 to 0.81), respiratory failure (OR 0.36, 95% CI 0.17 to 0.74), gastrointestinal, (OR 0.55, 95% CI 0.43 to 0.70), and renal complications (OR 0.67, 95% CI 0.59 to 0.76). Furthermore, odds were significantly reduced for postoperative delirium (OR 0.30, 95% CI 0.17 to 0.53), any infectious complications (OR 0.71, 95% CI 0.65 to 0.78), surgical site infections (OR 0.55, 95% CI 0.47 to 0.64), thromboembolic events (OR 0.74, 95% CI 0.58 to 0.96), and blood transfusions (OR 0.84, 95% CI 0.83 to 0.86).
Resource utilization outcomes showed a reduction in critical care admission (OR 0.91, 95% CI 0.86 to 0.95), and LOS with the use of PNBs (OR −0.36, 95% CI −0.42 to −0.31).
No difference in complications odds was found for mortality, perioperative nerve injury, MI, pneumonia, renal failure, stroke, and sepsis. Because of the lack of data, the outcomes readmission and cost could not be investigated in THA.
Perioperative impact of PNB use in TKA
In TKA patients, the utilization of PNBs was associated with significantly improved outcomes in many complication categories (tables 3 and 5).
Reduced odds with PNB use were observed for cardiac complications (OR 0.83, 95% CI 0.79 to 0.86), pulmonary complications (OR 0.84, 95% CI 0.79 to 0.89), respiratory failure (OR 0.37, 95% CI 0.18 to 0.75), and cognitive dysfunction (OR 0.52, 95% CI 0.34 to 0.80).
Furthermore, a significant decrease in any infectious complications (OR 0.77, 95% CI 0.73 to 0.80), surgical site infections (OR 0.86, 95% CI 0.80 to 0.91), thromboembolic complications (OR 0.90, 95% CI 0.84 to 0.96), blood transfusions (OR 0.91, 95% CI 0.90 to 0.92), and blood loss (mean difference −42.53 mL, 95% CI −52.08 to −32.98 mL) was found when PNBs were used.
Outcomes reflecting resource utilization showed an increase in critical care admissions (OR 1.07, 95% CI 1.04 to 1.10), while readmissions were significantly reduced (OR 0.66, 95% CI 0.61,0.70) with PNB use.
No difference in complication odds was found for mortality, MI, pneumonia, gastrointestinal complications, renal complications, renal failure, stroke, and sepsis, and perioperative nerve injury.
Primary analysis results are additionally presented as risk ratios in online supplemental appendix A4.
Pooled results of THA and TKA, rendering a significantly increased study sample, confirmed the individual THA and TKA analysis results, thus strengthening the association of increased perioperative safety with the use of PNBs. Detailed data, including forest plots are found in online supplemental tables A2 and A3.
Supplemental material
Secondary analyses
Subgroup analysis of trial design: RCT versus observational cohort studies
For transparency reasons, subgroup analysis was provided to report results stratified by trial design. As commonly described in current literature, our data demonstrate a lack of sufficient RCT-based evidence for adequate precision.32 Generally, however, RCT-based and observational-based results were compatible (tables 4 and 5).
Subgroup analysis based on primary anesthesia technique
Sample sizes varied substantially among the subgroups with the most homogenous groups of NA only and GA only emerging as rather small. Nevertheless, comparison among these two more stringently stratified groups, revealed some differences. The effect size for the reduction in cognitive dysfunction was greater in the PNB groups receiving GA compared with NA. Moreover, odds for pulmonary complications and respiratory failure were substantially reduced when PNB was used with GA as the primary anesthetic, while this was not observed in the PNB with NA group. Comparison involving the two larger groups (any GA and GA+NA) showed that results were generally consistent with the primary analysis. However, the observed effects appeared to be consistently stronger in groups involving PNB with GA.
Sensitivity analysis investigating a potential impact of ERAS pathways
A post-hoc analysis was performed to investigate whether the effects observed in the context of PNB use could have been driven by emerging clinical ERAS pathways. Studies were therefore stratified into before and after 2017 taking into account the potential impact of ERAS protocols.33 In an alternative approach, studies were also separated into those reporting average LOS<3 versus LOS≥3 days. However, this stratification proved to be unpracticable, because the lack of consistent LOS reporting rendered a loss of 60% of the study sample. In subgroup analysis by publication year, significant PNB effects were only observed in studies before the cut-off of 2017, most likely reflecting the relative scarcity of recent studies published after 2017. Nevertheless, results from the primary analysis indicated very minor differences in LOS with or without PNB use in terms of size of effect, with unlikely clinical significance. This lack of significant reduction in LOS with the use of PNBs does not appear to support the notion that the observed PNB effects may be substantially driven by ERAS measures. Nevertheless, clinical ERAS pathways may contribute to the improvement of outcomes observed with PNB use. As more evidence emerges, ERAS may prove to be significant driver of improved outcomes.
Discussion and recommendations
The current analysis demonstrates that PNB utilization was associated with reduced odds for numerous serious complications with critical impact on perioperative patient health in THA and TKA. The strongest effects were found in reduced odds for respiratory failure and cognitive dysfunction. The confidence in a beneficial impact of PNB use is strengthened by the large consistency of significantly reduced complication, independently observed among THA and TKA patients. Furthermore, the quality of evidence is strengthened considering the potential presence of two factors that would likely decrease the observed PNB effect. First, NA as the primary anesthetic would be expected to obscure an independent PNB effect based on similarities in basic features. Second, patients with a higher comorbidity burden may more readily receive PNBs.34 35 If indeed the case, this may have decreased the observed PNB effect.
From evidence to recommendations
Conclusions were based on the following factors: (1) evidence was largely in favor of the PNB intervention, (2) results were generally consistent among both patient populations and in subgroup analyses, (3) the desirable effects of the intervention significantly outweigh the potentially undesirable ones, (4) the intervention is feasible given that institutional resources and physician training are provided, (5) the intervention is acceptable to stakeholders and clinically feasible and finally (6) the intervention is in alignment with patient preferences based on improved postoperative outcome.20
Does PNB use influence postoperative complications in THA?
The utilization of PNB versus anesthesia without PNB was associated with lower complication odds for most studied outcomes (table 2).
Recommendation
PNB for perioperative pain management should be considered for THA patients when there is no contraindication. Furthermore, the alignment of clinician skills, practice location, and other resources needs to be ensured.
Level of evidence: moderate
Strength of recommendation: strong.
Does PNB use influence postoperative complications in TKA?
The utilization of PNB versus anesthesia without PNB was associated with lower complication odds for most studied outcomes (table 3).
Recommendation
Use of a PNB is recommended for patients undergoing TKA except when contraindications preclude their use. Furthermore, the alignment of clinician skills, practice location, and other resources needs to be ensured.
Level of evidence: moderate.
Strength of recommendation: strong.
Rationale
Based on the current findings and the grading of the level of evidence, the group reached consensus on the recommendations in favor of PNB use as stated above (94% agreed, 4% disagreed, 2% abstained). Considering factors integrated by the GRADE approach for the development of recommendations, the strength of the recommendation was determined as strong.
Several limitations need to be considered. According to the PICO question, the inclusion of observational data was essential because of considerable imprecision in RCT evidence, a typical issue preventing RCTs from providing high-quality evidence on unexpected and rare adverse events.13 Limitations of observational evidence, however, should be viewed in light of the fact that confounding may be less of a threat to validity when researching serious or unexpected events.13 Moreover, confounding by indication primarily influences treatment decisions that relate to expected or intended outcomes of benefit.13
The analysis included unadjusted data because of the lack of consistency in reporting, which also impeded our attempt to apply inverse variance.
Given the primary focus on the impact of PNBs on critical postoperative complications, other outcomes of importance—but not directly critical to the postoperative health condition—such as patient satisfaction, pain perception, opioid consumption, postoperative nausea and vomiting, quality of life, and functional and recovery parameters require separate analyses and were not addressed here.
The investigation of differences in intervention effects based on individual block techniques or specific comparators (including LIA, periarticular infiltration, intrathecal opioid use, intravenous analgesia, and patient controlled intravenous analgesia) was not feasible. Reasons included, the lack of systematic reporting causing inadequate subgroup information size and incomplete evidence synthesis in the context of a systematic literature review. Thus, data analysis providing adequate evidence on the impact of individual block types, LIA, or other comparators requires a customized methodology, targeted towards systematically capturing evidence on these interventions. However, implications of PNB effects in the context of major complications include factors such as mitigation of the surgical stress response, reduced anesthetic, and opioid requirement, as well as improved recovery and mobilization. These represent general features of PNBs and are not necessarily specific to individual block techniques. Furthermore, as a low-risk, high-yield procedure, future studies should investigate the perioperative impact of LIA with and without PNBs. Similarly, as ERAS measures may imply higher levels of care in association with PNBs, more research is needed as these clinical pathways could emerge as significant drivers of postoperative outcomes.
In accordance with GRADE, predefined outcomes were reassessed after the completion of evidence summaries.
In this process, anectodal reporting rather than systematic surveillance of perioperative nerve injury among individual RCTs prevented a complete evidence synthesis. Thus, selective reporting (ie, reporting of nerve injury based on its occurrence in patients receiving PNB) consequentially resulted in serious risk of bias, evident in funnel plots without random distribution. Further, an estimate of effect was falsely shifted in favor of published studies with inconsistent nerve injury surveillance. Substantially differing results between RCT and observational data further affirmed selective reporting. Given the rareness and nature of nerve injury, observational and registry data provide the most robust evidence in this context. For the analysis, the focus was therefore placed on the estimate of effect from observational, rather than RCT data.19 Current literature confirmed this approach, showing equal results for the incidence of nerve injury.36–42 Fortunately, most injuries are transient, subclinical, and may indeed not always be related to PNB43 but potentially linked to surgical and patient-related factors.36–42 44
Nevertheless, for transparency reasons RCT data are reported in online supplemental appendix A2.
Current evidence allows the conclusion that regional anesthesia provides satisfactory anesthesia and analgesia for many procedures, that indications and applications are increasing, and advances in training and techniques continue to emerge.39 Because of the low incidence of block related nerve injury (0.4 per 1000 blocks)42 and the common recovery from these injuries, the group believes that the numerous benefits of PNB outweigh the potential risk for harm.
Outcomes reflecting resource utilization including, critical care admission, and LOS represent rather weak surrogate markers of an independent PNB impact.45 46 The overall reduced complication risk observed with PNB use may indicate a stronger association of LOS and critical care utilization with other factors, including institutional practices and resource availability. These outcomes were therefore considered of limited importance for the development of recommendations.47
Cost of care could not be adequately analyzed due to lack of evidence.
A fixed effects model was used, based on the assumption that the underlying magnitude of treatment effect was considered similar across patients, outcomes, and interventions. As such, the study populations were restricted and largely homogenous and the outcomes of interest were considered largely standardized with limited margin for differential outcome measurement or interpretation. Furthermore, a largely consistent PNB effect was anticipated with regards to serious complications (eg, suppression of the systemic stress response to surgical trauma, reduced need for anesthetic medications and interventions), which should not significantly differ between individual block types. The fixed effect approach is nevertheless limited by the residual risk for between-study clinical heterogeneity.
Finally, despite efforts to investigate and account for possible publication bias in the context of GRADE, residual risk for type-1 error based on heterogeneity and positive publication bias cannot be entirely eliminated in meta-analyses. Nevertheless, this body of work provides a comprehensive and up-to-date synthesis and analysis of the current literature.
In conclusion, the current body of evidence is in favor of PNB utilization for patients undergoing THA and TKA. Quantitative and qualitative analysis demonstrated reduced odds for numerous major postoperative complications. Moreover, the consensus group found that desirable intervention effects outweigh the undesirable effects, that the intervention is acceptable to stakeholders, clinically feasible, and that PNB use is in alignment with patient preferences in terms of improved outcome.
Executive summary
Does the use of a PNB influence postoperative complications in patients undergoing THA?
The utilization of PNBs compared with anesthesia without PNB use was associated with lower odds for numerous major postoperative complications (tables 2 and 4).
Recommendation
PNB for perioperative pain management should be considered for THA when there is no contraindication. Furthermore, the alignment of clinician skills, practice location, and other resources needs to be ensured.
Evidence level: moderate, strong recommendation.
Does the use of a PNB influence postoperative complications in patients undergoing TKA?
In patients undergoing TKA, the use of PNBs was associated with significantly decreased odds for numerous major postoperative complications (tables 3 and 5).
Recommendation
Use of a PNB is recommended for patients undergoing TKA except when contraindications preclude their use. Furthermore, the alignment of clinician skills, practice location, and other resources needs to be ensured.
Evidence level: moderate, strong recommendation.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Systematic review and meta-analysis.
Ethics statements
Patient consent for publication
Ethics approval
Institutional Review Board approval was waived given the nature of previously published, deidentified data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @sgmemtsoudis, @jbLiujb, @ESoffin, @EMARIANOMD, @rljohnsonmd, @barringtonmj, @elboghdadly, @nelkassabany, @jashvant_p, @ESchwenkMD, @@ChrisWuMD
Contributors SGM had the idea for this article and is the guarantor of this project. A steering committee was formed to design, plan and lead and execute the study throughout the project: SGM, NES, CC, JB, JL, EMS, ERM, RLJ and MJH and GG. The literature search was performed by CC, RG, BJ, LP, BHL, PW, MB, GG, SJK, LB, DSW, GH, and BJ. Data extraction was performed by JB, DB, CC, BHL, PW, MB, GG, SJK, LB, DSW, GH, and BJ. Data analysis was performed by CC, SGM, NES, JP, JB, JL, ES, ERM, RLJ,MH and GG.The manuscript was written by CC, SGM, NES, JP, JB, JL, EMS, ERM, RLJ, MJH, and GG. The following participants reviewed and expanded the study plan, reviewed white papers resulting from quantitative analysis, and contributed to the interpretation of results: VA, EA, MJB, AB, JDA, KE-B, NME, PGautier, PGerner, AGDV, EG, ZG, RH, HK, PK, SK, PL’h, CMacLean, CMantilla, DM, AM, JMN, MP, JParvizi, PP, LPichler, JPoeran, LPoultsides, ESS, BDS, OS, ECS, EV, EGV-V, CLW, JY. All participants reviewed, commented on, and approved the study plan.
Funding This work is a result of solely institutional funding by the Department of Anesthesiology, Critical Care, and Pain Management at the Hospital for Special Surgery, 535 East 70th Street, New York, NY 10021, USA.
Competing interests SGM is a director on the boards of the American Society of Regional Anesthesia and Pain Medicine (ASRA) and the Society of Anesthesia and Sleep Medicine (SASM). He is a one-time consultant for Sandoz and the holder of US Patent Multicatheter Infusion System. US-2017-0361063. He is the owner of SGM Consulting, LLC and Centauros Healthcare Analytics and Consulting. SGM is also a shareholder in Parvizi Surgical Innovations LLC and HATH. None of the above relations influenced the conduct of the present project.
Provenance and peer review Not commissioned; externally peer reviewed.