Article Text

Abstract
Background Studies have found that diffuse pain, indicative of central sensitization, portends poor interventional outcomes. Multiple chemical sensitivities are associated with signs of central sensitization. We sought to prospectively determine whether hypersensitivity reactions (HR) were associated with epidural steroid injection (ESI) outcomes.
Methods HR were classified as immune-related or non-immune-related and categorized by number (0=low, 1 or 2=intermediate, ≥3=high). The primary outcome measure was mean reduction in average leg pain score 1 month post-procedure. A positive outcome was defined as a two-point or greater decrease in average leg pain accompanied by satisfaction 1 month post-procedure.
Results The mean number of immune-mediated and non-immune-mediated HR were 0.6±1.2 and 0.8±1.4, respectively. Individuals in the high (n=24) total HR group had a mean reduction in average leg pain of 0.1±2.7, compared with those in the low (n=61; 1.8±2.1, p=0.025) and intermediate groups (n=52; 1.6±3.1, p=0.060). For back pain and categorical successful outcome, those with fewer HR experienced greater benefit. There were no differences in outcomes when patients were stratified by immune-related HR. Among participants in the low, intermediate and high non-immune-mediated HR groups, the mean reductions in average leg pain scores were 1.7±2.5, 1.6±3.0, and −0.2±2.3, respectively (p = 0.002). 51%, 35%, and 12% of people with low, intermediate and high numbers of non-immune-mediated HR experienced a positive categorical outcome, respectively (p=0.007).
Conclusions Non-immune-related HR were inversely correlated with some ESI outcome measures.
- neuraxial blocks: epidural
- interventional pain management
- spinal/epidural injection
- chronic pain: back pain
- chronic pain: central pain syndromes, fibromyalgia
Statistics from Altmetric.com
- neuraxial blocks: epidural
- interventional pain management
- spinal/epidural injection
- chronic pain: back pain
- chronic pain: central pain syndromes, fibromyalgia
Introduction
Fibromyalgia and other nociplastic pain conditions, including some forms of chronic low back pain (LBP),1 have been postulated to result from ‘central sensitisation’.2 3 These conditions, formerly known as functional pain syndromes, are associated with manifestations of a hyperactive nervous system including multisensory hypersensitivity4 and multiple chemical sensitivities.5 6 It is estimated that about 20% of people have multiple chemical sensitivities, which are associated with psychiatric disorders, poor function, and increased use of healthcare resources.7 There is also overlap between true (ie, immune-mediated) medication allergies and non-immune-mediated hypersensitivity reactions (HR), which may have diverse etiologies. The latter includes more severe manifestations of expected side effects, over-reporting of normal side effects, toxicant-induced loss of tolerance, and somatization disorders.8 9
Among chronic pain conditions, LBP is the leading cause of years lost to disability, with a cost exceeding US$100 billion annually in the USA10 11 There are many ways to classify LBP, with perhaps the most useful being into neuropathic and non-neuropathic pain, as this heavily influences treatment decisions. According to one review, among individuals with LBP, 36.6% have primarily neuropathic pain.12
Epidural steroid injections (ESI) are the most frequently performed pain medicine procedure. In recent years, the use of ESI to treat LBP has risen dramatically,13 which has led to increased emphasis on improved selection. There are little data on the use of procedural interventions for nociplastic pain, though they are generally acknowledged to be less effective than for localized pain conditions.1 14 For example, researchers have reported aberrant responses and poor treatment outcomes in patients with fibromyalgia with a primary complaint of LBP.15 16 However, using a concurrent diagnosis to inform treatment decisions is fraught with challenges. These include the subjective nature of syndromes (as opposed to diseases), the expertise required to identify them, and that they represent a spectrum of conditions characterized by different prognoses.17
The use of biomarkers or phenotypic markers and other surrogate measures to objectify diagnosis and guide treatment is considered a top pain research priority. Along these lines, identifying a surrogate marker for central sensitization might be useful in selecting ESI candidates and improve outcomes. One such marker could be HR, which are generally listed as ‘allergies’ in the chart and should be updated on each visit.
There are several reasons that a patient with many drug HR might be more likely to fail treatment. These include the proposed association between HR (ie, chemical sensitivities) and central sensitization, the link between chronic pain and the immune system in people with immune-related drug allergies, the inability of these individuals to tolerate treatments, and the possible association of somatization disorder with aberrant responses to injections and poor treatment outcomes.1 14 18 19 The main objective of this study was to determine whether the number of immune-related and non-immune-mediated HR reported in the medical records of patients who undergo ESI could predict outcome. We hypothesized that patients with a high number of HR would experience poorer ESI results.
Methods
Permission to conduct this pragmatic prospective, observational cohort study was granted by the Institutional Review Boards of Johns Hopkins School of Medicine, Drexel University College of Medicine, Walter Reed National Military Medical Center, Puget Sound Veterans Affairs Hospital, Seattle, WA Landstuhl Regional Medical Center, Landstuhl, Germany, San Diego Naval Hospital and Womack Army Medical Center, Fort Bragg, NC; the latter two institutions did not enroll any participants. This manuscript reports the results of a planned interim analysis for an exploratory study that sought to determine whether the number of documented medication side effects is associated with ESI outcomes for radicular pain, with the larger study examining the effect a multitude of demographic, clinical and technical variables has on LBP injection treatment results. HR were defined a priori and standardized across sites, with the number and type garnered from medical records under ‘allergies’ and patient reports (see below for examples). Per standard of care, these were reconciled in the record before the procedure if there was a discrepancy (ie, added if the patient reported an HR missing from the record or deleted if it was determined that a listed allergy was incorrectly entered, eg, palpitations from local anesthetic with epinephrine injected during a procedure). Thus, the medication HR reported in this manuscript were transcribed directly from electronic records to ensure objectivity, with food allergies excluded. The study was posted on clinicaltrials.gov on 1 January 2015 (ClinicalTrials.gov Identifier: NCT02329951). All participants were treated between January 2015 and September 2018 and provided informed written consent.
Participants and settings
This study was conducted in multidisciplinary pain treatment centers in two civilian and three military treatment facilities, four of which have or are affiliated with accredited pain medicine training programmes. Individuals treated for a primary complaint of lumbosacral radiculopathy were eligible to enroll. Inclusion criteria were age ≥18 years; duration of pain >6 weeks; radicular back pain presumed secondary to herniated disc, spinal stenosis, or other degenerative disc pathology such an annular tear; and leg pain ≥4/10 or comparable to LBP. Excluded from participation were individuals who had received previous injections within the past 2 years; active spondyloarthropathy (eg, symptomatic ankylosing spondylitis); previous low back surgery; allergy to bupivacaine, contrast dye, or corticosteroid; coagulopathy precluding injection treatment; and pregnancy. Because this study was part of a broader endeavor to determine treatment outcomes for back pain injections in general, we did not require specific imaging findings such as a herniated disc for inclusion, though patients with normal MRIs or imaging that did not correlate with symptoms were excluded.
Procedures
Procedures were performed in hospital-based pain clinics using fluoroscopic guidance by or under the supervision of a board-certified pain medicine physician using superficial local anesthetic. Individuals with unilateral symptoms generally underwent transforaminal ESI, while those with bilateral symptoms received interlaminar ESI. Transforaminal ESI were performed with the image intensifier generally angled at least 30 degrees in an oblique fashion to ensure adequate epidural uptake. The 22-gage spinal needles were inserted into the targeted foramen using a coaxial approach with oblique, anteroposterior, and lateral views. Radiopaque contrast injection was used to confirm nerve root and epidural spread. After correct position was confirmed, a 3 mL solution containing 10 mg of dexamethasone, 0.5 mL of saline and 1 mL of 0.25% bupivacaine was administered.
Interlaminar ESI were performed using fluoroscopic guidance in the anteroposterior and lateral views using the loss-of-resistance technique through a Touhy needle directed midline for those with symmetrical pain or slightly to the affected side in people with bilateral radicular symptoms that were more pronounced on one side. Once loss of resistance was obtained and correct position confirmed with contrast, a 4 mL solution containing 40 mg of depomethylprednisolone, 1.0 mL of 0.25% bupivacaine, and 2 mL of normal saline was injected.
Follow-up
No interventions between the procedure and initial follow-up visit were permitted. Rescue medications could include either tramadol, non-steroidal anti-inflammatory drugs, or if the patient was on opioids, a <20% increase in dose (which was not used). The first follow-up visit was 1 month after the ESI. A positive outcome was predefined as a greater than two-point decrease in average leg pain with a positive satisfaction rating (>3 on a five-point scale). Subjects who experienced a positive outcome at their initial 1 month follow-up visit remained in the study and returned for the final 3 month follow-up visit, while those with a negative outcome exited the study to receive other possible treatments. Individuals who obtained a positive outcome at 1 month but experienced a recurrence before their 3 month follow-up visit also exited the study, with their final follow-up data obtained prior to subsequent treatment.
Data collection
Data was obtained by an investigator not involved in the procedure. Baseline data was collected on the first day of treatment and included age, gender, duration of pain, type of ESI, analgesic medication usage (including opioids), active duty status, presence of fibromyalgia or other chronic pain syndrome, Oswestry Disability Index 2.0 (ODI) score, and the number and type of medication HR. A HR was considered to be either an immune-mediated allergic reaction (eg, rash, anaphylaxis, documentation via allergy testing) or a severe side effect (eg, syncope, excessive sedation, vomiting) that warranted documentation under medication ‘allergies’ in the patient’s medical record. Determination of this categorization was made by the physician based on patient report and medical records, which may have included immunological testing. To ensure objectivity, less serious adverse reactions to medications (eg, weight gain or dizziness) that were not listed in the medical record were not considered as HR. For each of the three categories (total, immune-related, and non-immune-related HR), the recorded number of ‘allergies’ was stratified into three separate groupings: 0 (low), 1–2 (intermediate), and ≥3 (high) HR.
The primary procedural outcome measure was mean reduction in average leg pain over the past week 1 month post-treatment. Secondary outcome measures included average and worst leg and back pain scores over the past week, ODI, medication usage, complications, satisfaction graded on a five-point Likert scale ranging from very unsatisfied to very satisfied, and categorical outcome, with a positive outcome defined as a two-point or greater decrease in average leg pain score coupled with a score >3 on the satisfaction scale. Positive medication reduction was predefined as a>20% decrease in opioid use or cessation of a non-opioid analgesic, per previous studies.20 Subjects who failed to achieve a positive outcome at 1 month exited the study to pursue other treatment options, with their negative outcome data carried forward. Those who obtained a positive outcome returned at 3 months for their final follow-up, at which time the same outcome data were retrieved.
Statistical analysis
All statistical analyses were performed in Stata V.14. Although the total number of patients we intend to enroll is based on the principal (ie, outcomes following back pain procedures in general) rather than this exploratory trial, a post hoc power analysis revealed that this study was 76.2% powered to detect the observed difference in the primary outcome measure among the three groups (low, intermediate, and high total HR) at an alpha level of 0.05. Data were analyzed using an intention-to-treat approach, with the last observation carried forward for missing data and patients who exited the study per protocol after the 1 month follow-up due to treatment failure. This approach was felt to be the most conservative analysis of treatment effect for participants who exited at one month, since observations were not missing at random, and those who exited the study per protocol were unlikely to have improvements in outcome measures from the physiological effects of steroids after 1 month. Exits per protocol comprised over 90% of observations carried forward, while missing data from dropouts accounted for less than 10%. A sensitivity analysis of the 3-month outcomes with and without data from the seven dropouts did not alter the overall significant findings of the original analysis.
Study participants were categorized based on total number of HR (low=0, intermediate=1–2, and high ≥3), number of immunological HR, and number of non-immunological HR. For continuous outcomes, group means and SD are reported and analysis of variance was used to compare HR groups. For categorical outcomes, percentages are reported, with χ2 tests used. For comparisons between two groups, a p-value less than alpha of 0.05 was considered statistically significant. For comparisons among three or more groups, post hoc Dunn’s tests were performed, and a Bonferroni-adjusted p-value of n times the p-value of the pairwise comparison (where n is the number of groups) was reported. An adjusted p-value less than an alpha of 0.05 was considered statistically significant.
In order to identify potential differences in baseline characteristics between patients with positive and negative outcomes 1 month following ESI, the two outcome groups were compared. For continuous characteristics, Student’s t-tests were used for parametric and Mann-Whitney U tests for non-parametric data. For binary or categorical characteristics, χ2 tests were used. Variables in the analysis included age, sex, duration of pain, type of ESI, opioid use, active duty status, disability, co-existing chronic pain condition, co-existing fibromyalgia, coexisting psychiatric condition, baseline average and worst Numerical Rating Scale (NRS) low back and leg pain scores, baseline ODI score, and number of immunological, non-immunological, and total HR. To elucidate the potential relationships between selected covariates and ESI outcome at 1 month, a multivariate logistic regression analysis was performed using a backward stepwise approach. Covariates analyzed were age, sex, duration of pain, opioid use, baseline average NRS low back and leg pain scores, and number of non-immunologic HR. A two-sided p-value less than 0.05 was considered statistically significant.
Results
A total of 409 people were screened for eligibility, with 137 who underwent ESI included in the analysis. The most common reason for exclusion was repeat injection (n=209). Table 1 shows baseline demographic and clinical characteristics both overall and by number of total HR. For the cohort, the mean age+SD was 50+14 years, with 57% being female. There was a higher proportion of women in the intermediate HR group (71%), which was significantly greater than the low HR group (43%, p=0.006), but not the high HR group (63%, p=1). There was a statistically significant difference in active duty status and baseline worst leg pain among the three groups, but these differences were non-significant after post hoc pairwise comparisons. There was a higher proportion of patients with fibromyalgia in the high HR group (21%), which was significant compared with the low HR group (2%, p=0.004) and to the intermediate HR group (6%, p=0.037). Similarly, the high HR group had a significantly greater proportion of patients on disability (48%) compared with the low HR group (18%, p=0.022), but not the intermediate HR group (31%, p=0.38). Baseline ODI score was also significantly higher in the high HR group (50±17) compared with the low HR group (38±17, p=0.006), but not the intermediate HR group (43±16, p=0.26). The progression of participants through the study period is depicted in figure 1.
Baseline demographic and clinical characteristics of study subjects
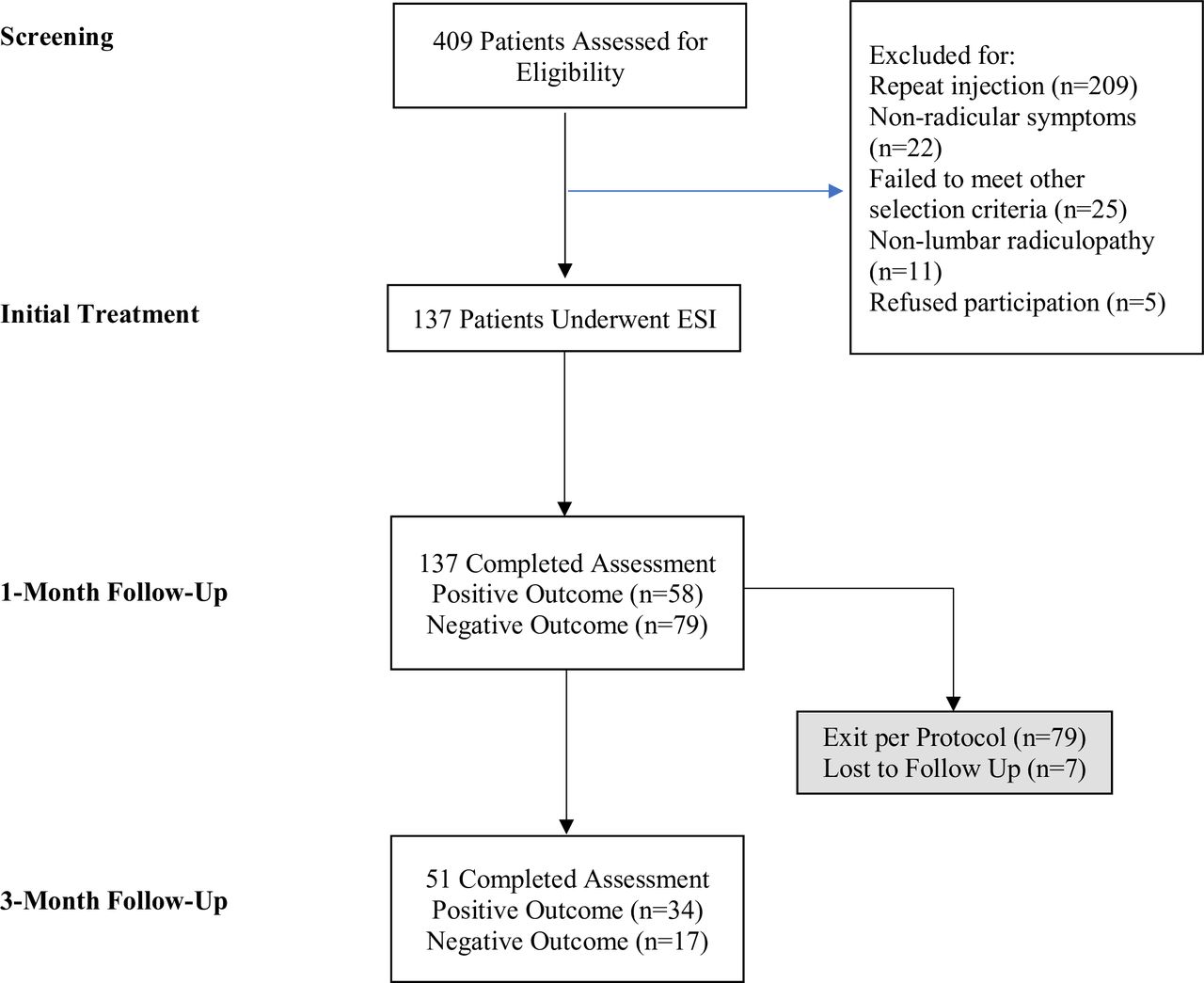
Study flow chart.
Outcomes broken down by total number of HR
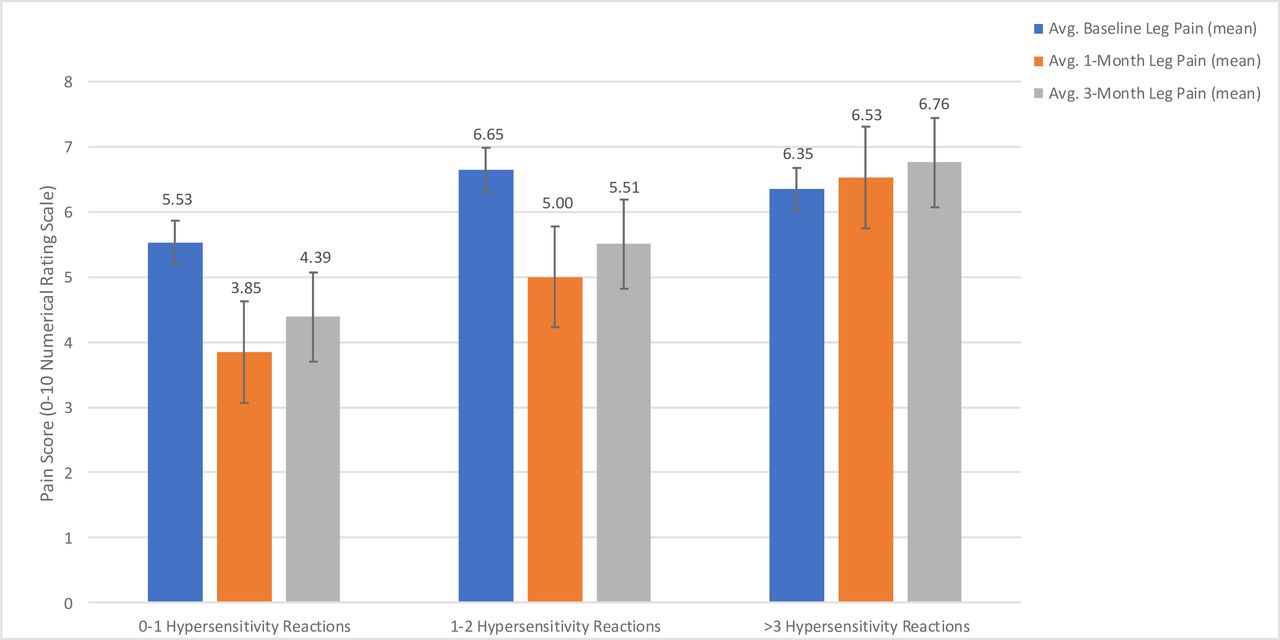
Treatment outcomes at 1 and 3 months following ESI stratified by total number of HR are shown in table 2 and figure 2. For the primary outcome measure of reduction in average NRS leg pain score at 1 month, there was a statistically significant difference among the three groups (p=0.024), with a significant decrease in average leg pain reduction in the group with a high number of HR (0.1±2.7), compared with the low HR group (1.8±2.1, p=0.025), but no significant difference compared with the intermediate HR group (1.6±3.1, p=0.060). The high HR group had significantly lower reductions in average NRS LBP scores at 1 month (−0.4±2.7), compared with the low HR group (1.4±2.0, p=0.004), and the intermediate HR group (1.0±2.3, p=0.033). Similarly, there was a significant difference in reduction in average NRS LBP at 3 months following injection (0.9±1.9 vs 0.7±2.3 vs −0.1±2.4 for low, intermediate, and high HR groups, respectively; p=0.049), with a significant difference between the low and high HR groups (p=0.046), but not between the low and intermediate (p=1) or intermediate and high HR groups (p=0.14). There were no significant differences among groups for reductions in average NRS leg pain at 3 months (p=0.075). The group with a high number of total HR had significantly lower satisfaction scores at 1 month (2.2±1.5) and 3 months (1.8±1.4) compared with the groups with low (3.6±1.3 at 1 month, p<0.001; 3.6±1.3 at 3 months, p<0.001) and intermediate numbers of HR (3.4±1.5 at 1 month, p=0.003, 3.2±1.4 at 3 months, p=0.011). There were no other significant differences in outcomes at one or 3 months among total HR groups.
Treatment outcomes stratified by number of total HR

{kind=link}
{kind=link}
Pain scores over study period stratified by number of hypersensitivity reactions.
Outccomes broken down by types of HR
Table 3 shows treatment outcomes at 1 and 3 months stratified by number of immunological and non-immunological HR. For immunological HR, there were no significant differences in the primary outcome of reduction in average NRS leg pain score at 1 month (1.2±2.0 vs 0.3±2.6 vs 1.2±3.3 between groups with low, intermediate, and high numbers of allergies, respectively; p=0.11). There were also no significant differences among groups for any study outcome at one or 3 months. When broken down by number of non-immunological HR, there was an overall significant difference among groups in the primary outcome of reduction in average NRS leg pain score at 1 month (1.7±2.5 vs 1.6±3.0 vs −0.2±2.3 for low, intermediate, and high numbers of non-immunological allergies, respectively, p=0.002). In pairwise comparisons, there was a significant difference between the high versus low group (p=0.003), but not the high versus intermediate (p=0.26), or intermediate versus low groups (p=0.18). Similarly, the proportion of patients with a positive outcome at 1 month was significantly different for the high non-immunological HR group compared with the low non-immunological HR group (12% vs 51%, p=0.007); the proportion with a positive outcome at 1 month for the intermediate non-immunological HR group was not significantly different from the other two groups (35%, p=0.32 when compared with the low non-immunological HR group, p=0.31 compared with high non-immunological HR group). Satisfaction scores were significantly lower for the group with a high number of non-immunological HR compared with the low non-immunological HR group (2.2±1.4 vs 3.6±1.3, p=0.001 at 1 month; 2.2±1.3 vs 2.9±1.5, p=0.001 at 3 months). Neither group significantly differed from the group with an intermediate number of non-immunological HR at 1 month (3.0±1.6, p=0.16 when compared with the low non-immunological HR group, p=0.17 compared with high non-immunological HR group) or 3 months (2.9±1.5, p=0.12 when compared with the low non-immunological HR group, p=0.21 compared with the high non-immunological HR group).
Treatment outcomes stratified by number and type of HR*
Factors associated with outcome
Differences in baseline demographic and clinical variables between participants with positive versus negative outcomes at 1 month are shown in table 4. Factors that differed significantly between the two groups were duration of pain, disability status, presence of a coexisting psychiatric condition, baseline average and worst NRS low back and leg pain scores, baseline ODI score, and number of non-immunological and total HR. Age, sex, type of ESI, opioid use, active duty status, coexisting chronic pain conditions including fibromyalgia, and number of immunological allergies were not significantly associated with treatment outcome.
Baseline demographic and clinical variables broken down by 1 month treatment outcome
Following multivariate regression analysis, lower baseline average NRS back pain score and less non-immunological HR were the only factors found to be significantly associated with positive treatment outcome (table 5). Age, sex, duration of pain, opioid use, and baseline average NRS leg pain score were not associated with successful outcome. The odds of a positive outcome were 0.66 times lower for each additional non-immunological HR (95% CI 0.47 to 0.94, p=0.022) and 0.81 times lower for each one-point increase in baseline average NRS back pain score (95% CI 0.67 to 0.99, p=0.038).
Odds of positive treatment outcome at 1 month as a function of selected baseline variables
Discussion
The principal finding in this study is that while the total number of HR was not significantly associated with our primary outcome measure, it did predict procedural outcome. Moreover, there was an association between non-immunological medication side effects and ESI, such that a higher number correlated with poor treatment outcome. We hypothesized that individuals with more documented HR would fare worse after ESI for two reasons. First and foremost, individuals with nociplastic pain conditions such as fibromyalgia, who are more likely to fail interventions,15 16 have more ‘chemical sensitivities’, which are often recorded as allergies.5 6 This may reflect central sensitization and other nociplastic mechanisms. Second, individuals with somatization disorder are more likely to experience serious medication side effects that may be reported under ‘allergies’21 and have poor outcomes with pain treatment, as evidenced by higher failure rates for chiropractic manipulation and other treatments for spine pain, a higher failure rate for non-spinal injections, and a higher incidence of persistent pain and false-positive rate with discography.19 22–24
The most likely reason why non-immunological, but not immunological, medication reactions might predict treatment failure is because non-immunological adverse effects are by their very nature more common in people with sensitized nervous systems and/or who are overly focused on their physical state such that they experience physical symptoms in the absence of, or disproportionate to, a physical cause.5–7 21 For adverse medication effects, these non-immune-mediated reactions are often reported as ‘allergies’.25 As alluded to, these types of reactions may also be more common in people with coexisting psychological issues that can predispose patients to ESI treatment failure.14 There are instruments that may be used to gage phenomena such as central sensitization and somatization such as the modified fibromyalgia symptom severity scale,26 but unlike counting allergies, these surveys can be resource intensive. Although chemical sensitivities occur more frequently in nociplastic pain conditions that predispose patients to interventional treatment failure, there is insufficient evidence to support the theory that immune-mediated HR contribute to this phenomenon.27 The reason why HR were grouped together before separating them is because the number of total allergies annotated in medical records is clear-cut and therefore not subject to judgement or bias. Other possible explanations for our findings include an enhanced placebo response in these individuals and alterations in pain processing.
One may question how, or even whether, these findings can be used to guide care. Since the correlation between non-immune-mediated HR and negative outcome is weak, it is not advisable to use allergies as the sole basis for the decision about whether to proceed with a spinal injection. In a similar study that sought to predict ESI outcomes, Schiff and Eisenberg28 reported mixed results for quantitative sensory testing. Compared with quantitative sensory testing which is resource intensive and uncomfortable, the use of a non-invasive, simple and inexpensive predictive tool is preferable. But in conjunction with other negative outcome predictors for back pain in general and ESI in particular such as greater disease burden (eg, longer duration of pain, higher baseline pain and disability, opioid use) and spinal stenosis,14 29 30 these variables may collectively confer high predictive value which can someday form the foundation for treatment decisions. Although many of these predictors are impractical or impossible to treat before an injection (eg, spinal pathology), others such as certain types of central sensitization may be possible to reverse.31
There are several limitations to our study that warrant consideration. First, because we did not refer patients for allergy testing, there may have been misclassifications such that allergies interpreted as immune-mediated were non-immunological-based and vice versa. However, our goal was to find a quick and inexpensive (free) means that could be clinically used to foretell treatment response, and lab testing would be inconsistent with this. Second, because of questions surrounding the diagnosis and treatment effectiveness of facetogenic and sacroiliac joint pain, we elected to examine only ESI as the index procedure, which are performed more frequently. Thus, whether these findings can be generalized to other procedures is unknown. Third, the recording of drug intolerances is highly provider dependent (ie, minor reactions such as dizziness might be listed for some patients but not others), though this confounding factor was somewhat mitigated by standard-of-care allergy reconciliation based on patient report. However, while our methodology addressed potential causes of physician bias, it fails to account for patient bias, such that the HR patients elect to report to physicians may vary. Fourth, since the pre-enrolment power analysis was performed for the primary study, which is examining a host of different back pain injections and therefore employs different outcome measures (eg, average back pain rather than leg pain), this exploratory study may have been underpowered for some measures. Due to the nature of this study, we examined a number of potential factors associated with multiple outcomes. For ease of interpretation, our analyses were performed without adjustment for multiple comparisons, which may have increased the likelihood of false-positive associations that were considered significant. Last, since the objective of the study was to examine outcome predictors for back pain injections in real-world conditions, we employed relatively loose selection criteria, so that these findings may not be applicable to situations where stringent selection criteria are desirable such as for clinical trials.
In summary, we found that individuals with more non-immune-related HR were more likely to experience a negative ESI treatment outcome. In the age of precision medicine, practitioners should take this into account when balancing the risk:benefit ratio of ESI.
Acknowledgments
The authors acknowledge David Reece, DO, and Edward Dolomisiwiecz, MD, for their help in patient recruitment.
References
Footnotes
Contributors SPC contributed to the concept design. TLD contributed to the statistical analysis. SPC, TCD, SD, AJV, SRG, MS and CK contributed to the data collection. SPC and CK did the planning. SPC, TCD, AG, OCC, MBJ and CK contributed to the administrative requirements. SPC, TCD, AG, OCC, MBJ, SD, AJV, SRG, MS and CK were responsible for the patient enrolment and treatment. TCD, AG, OCC, MBJ, SD, AJV, SRG, MS and CK contributed to the critical review of manuscript. SPC and TLD contributed to the interpretation of data. SPC, TLD and TCD drafted the tables and figures. SPC and TLD drafted the manuscript.
Funding Funded in part by a grant from the Centers for Rehabilitation Sciences Research, US Department of Defense.
Competing interests SPC serves as a consultant to Semnur Pharmaceuticals, which is developing a steroid approved by the US FDA for epidural administration.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.