Article Text

Abstract
Background and objectives As a follow-up to the 6-month report,12 this study investigated the analgesic effect of cooled radiofrequency ablation (CRFA) in patients with knee osteoarthritis (OA) 12 months postintervention and its ability to provide pain relief in patients who experienced unsatisfactory effects of intra-articular steroid injection (IAS).
Methods Seventy-eight per cent (52/67) of patients originally treated with CRFA were evaluated at 12 months, while at 6 months post-IAS, 82% (58/71) of those patients crossed over to CRFA and assessed 6 months later.
Results At 12 months, 65% of the original CRFA group had pain reduction ≥50%, and the mean overall drop was 4.3 points (p<0.0001) on the numeric rating scale. Seventy-five per cent reported ‘improved’ effects. The cross-over group demonstrated improvements in pain and functional capacity (p<0.0001). No unanticipated adverse events occurred.
Conclusions This study demonstrates that analgesia following CRFA for OA knee pain could last for at least 12 months and could rescue patients who continue to experience intolerable discomfort following IAS.
Clinical trial registration The ClinicalTrials.gov registration number for this study is NCT02343003.
- chronic pain
- radiofrequency ablation
- clinical pain
- interventional pain management
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Total knee arthroplasty (TKA) is an effective therapeutic option of last resort for individuals afflicted with significant osteoarthritis (OA)-related knee pain and dysfunction. While the outcomes of TKA are consistent and well established,1 2 the procedure may not be indicated in patients who have comorbidities,3 or those who otherwise may not be appropriate candidates for TKA.4 Therefore, providing a therapeutic option with long-term duration of effect may enable such patients to have a more satisfactory quality-of-life.
The minimally invasive, outpatient nature of radiofrequency ablation (RFA) of targeted nociceptive nerves is becoming an increasingly well known and timely option for patients in whom conservative therapies have failed and/or those who are not candidates for TKA.5–8 In particular, the ‘cooled’ form of RFA (CRFA) has afforded patients with knee OA with pain relief9–12 and functional improvement.9 11 12 Most recently, we reported that 74% of patients treated with CRFA had pain reduction of 50% or more compared with 16% of demographically matched patients who received an intra-articular steroid injection (IAS) at 6 months postintervention.12 In addition, through secondary measures, significantly more patients at 6 months reported ‘satisfactory joint function’ via the Oxford Knee Score and a perception that their treatment effect had ‘improved’ their condition than those who received an IAS per the Patient Global Perceived Effect. Although the beneficial effectiveness of CRFA for treating OA of the knee was evident from the 6-month analyses of this study,12 a paucity of data has been published regarding longer term durability of these effects.
This analysis explored the sustainability of analgesic effects realized at 6 months in patients with knee OA who were treated with CRFA. We hypothesized that significant (≥50%) analgesia would remain among the majority (>50%) of patients in the original CRFA group 12 months postintervention and that patients who still had intolerable discomfort 6 months following IAS would experience significant (≥50%) pain relief after CRFA. As such, this current study primarily evaluated the proportion of patients whose knee pain was reduced by ≥50% from baseline 12 months post-treatment within the initial cohort of patients with OA who were enrolled in the 6-month clinical trial at 11 different sites.12 Additionally, clinical features of subjects who elected to cross-over to receive CRFA after 6 months (‘cross-over’ (XO) group) were evaluated.
Methods
All patients were properly consented prior to initiating screening activities. The study is registered in ClinicalTrials.gov: registration number, NCT02343003; initial release date, 15 January 2015.
Study design
This prospective, randomized, open-label, multicenter (11 sites) clinical study with a parallel-group design initially included the test treatment, CRFA (N=76), utilizing the Coolief System (Halyard Health, Alpharetta, Georgia, USA), or IAS (N=75), in a 1:1 randomization scheme. The methodological differences between the active treatment comparators in this study did not permit blinding of investigators or patients to the interventions. The initial results from this study presented data through study follow-up visits at 1, 3, and 6 months compared with the two study groups primarily by the proportion of subjects whose knee pain was reduced by ≥50% from baseline at 6 months post-treatment. Additional secondary measures noted improvements in function, and nearly all patients in the CRFA group (91%) reported perceptions of ‘improvement’ regarding their knee pain.12 The focus of this report is to describe the patient’s experience through 12 months. Additionally, to further evaluate CRFA, patients who were dissatisfied with their IAS treatment after 6 months could cross-over to the ablation treatment. The substantial migration of original IAS study group members to the XO group left only four patients in the former cohort, which was considered too small to conduct any meaningful analytical statistical comparisons between CRFA and IAS treatments at 12 months post-interventions. Patients in the IAS cohort who elected to receive CRFA treatment at the 6-month follow-up visit were followed for an additional 6 months and are herein referred to as XO group members. Methodology, patient demographics, and 6-month results for the original CRFA and IAS study groups have been published.12
Study population
Patients who had radiographic evidence of OA within 12 months prior to study screening, with no other etiology demonstrated as the source of knee pain, were eligible for the study. While individuals with bilateral knee OA were not excluded; only one knee was screened and enrolled as the ‘index knee’ for treatment. Management of contralateral knee pain in bilateral patients was left up to the discretion of the investigators and patients as part of standard of care. Selection criteria included: knee pain ≥6 months that was unresponsive to conservative treatments (physical therapy, oral analgesics: ≤60 mg morphine equivalence, stable for 2 months; intra-articular injections with steroids and/or viscosupplementation), body mass index (BMI) <40, and reporting ≥50% response to blocks as described previously12 and below. On confirmation that a patient was eligible, randomization was completed utilizing prepopulated, sequentially numbered, sealed envelopes generated by the statistician using a computerized randomization programme. Sites opened a single envelope per patient and chose the lowest available number to maintain sequential ordering of randomization. Additional treatments for the index knee were prohibited during the study.
The block paradigm was as follows: patients who indicated a score reduction on the numeric rating scale (NRS) ≥50%5 at least 15 min following fluoroscopically guided blockade of the superomedial and inferomedial branches of the saphenous nerve and the superolateral branch of the femoral nerve13 using 0.60–0.75 mL/site of local anesthetic (preferably Marcaine (bupivacaine) Hospira, Lake Forest, Illinois, USA, 0.5% or similar) at each site were eligible for the study.12
Study intervention
Cooled RFA of the index knee was administered to patients in the CRFA study cohort, as facilitated by fluoroscopic visualization of anatomical landmarks.13 A 75 or 100 mm 17-gage CRF introducer was placed at the appropriate locations after 1–3 mL of 1% lidocaine was infiltrated. An 18-gage internally cooled 4 mm active tip electrode was placed into the introducer needle, and 50 Hz sensory stimulation at <0.5 V in all three locations reproduced concordant knee pain that ensured proximity of the probe to each of the target nerves (superomedial and inferomedial branches of the saphenous nerve and the superolateral branch of the femoral nerve)13 prior to lesioning. Next, motor stimulation at 2 Hz was carried on up to 1 V without muscular contractions to ensure proper distance of final radiofrequency (RF) needle active tip position from any motor nerve fibers.
The CRFA intervention produces thermal energy with average maximum tissue temperatures greater than 80°C,14 while the probe tip temperature is maintained at 60°C by the cooling water circulating within the probe. Each lesion was created over 150 s. Following the procedure and patient recovery, each patient was discharged to home with instructions to limit strenuous activity for at least 24 hours postprocedure.
Study outcomes
The proportion of subjects whose knee pain was reduced by ≥50% compared with baseline was calculated at 12 months post-treatment,15 as measured by the NRS. Secondary endpoints included: (1) change in knee function detected by the Oxford Knee Score (OKS)—a validated outcomes instrument that is routinely used to evaluate the overall condition of subjects with knee OA,16 (2) subjects’ perception of treatment effect as reflected by the Global Perceived Effect score, and (3) opioid analgesic use, as measured by subject self-reported average daily dosage used. Reported assessments of these study endpoints were based on patients’ impressions made during the week preceding data collection at each study visit for the original CRFA group (baseline and 12 months) and XO group (baseline and 6 months). The baseline values utilized for XO analysis were those at the time of cross-over for all outcome measures. All subjects were evaluated for adverse events (AEs) and serious AEs (SAEs) at each visit.
To investigate a theoretical concern that CRFA could inadvertently progress knee OA relative to evidence provided at study baseline, an amendment was created late in the study to allow for the collection of radiographs at 12 months. Fifty-one images were considered, and the disease state displayed by each was quantified by independent radiologists (generally) per the Kellergan-Lawrence Scale. Twenty-four images were from the originally treated CRFA group and 27 were from the XO group.
Statistical analysis
A non-inferiority evaluation was used to estimate the study sample size. The sample size was based on the estimated success rates of 59%8 (success ≥50% NRS score reduction) and 47%17 (success ≥30% NRS score reduction) in the CRFA and standard groups, respectively, and a non-inferiority margin of 15%. Assuming an attrition rate of 20% and a two-sided significance level of 5%, 144 subjects enrolled into the study would yield 114 subjects at the primary endpoint.
As was previously reported on 6-month outcomes of this study,12 the 12-month data are derived from the full-analysis study population set, while the XO results are from the per-protocol set. The protocol defined the full analysis set as: all randomized subjects will be analyzed following the principle of intention-to-treat (ITT) provided they received Coolief or corticosteroid injection treatment and had at least one effectiveness observation, thereby, the results presented can be considered a modified ITT. Percentages are reported with 95% CI. Within-group comparisons were expressed as mean and an associated SD, with significant differences indicated by p≤0.05. Such analyses were not prespecified, and so no type I error adjustment for multiplicity was made to preserve the overall 5% level of significance. Assessment determinations were made from aggregates of data collections from all available patients at each study time point.
Results
Disposition of study patients
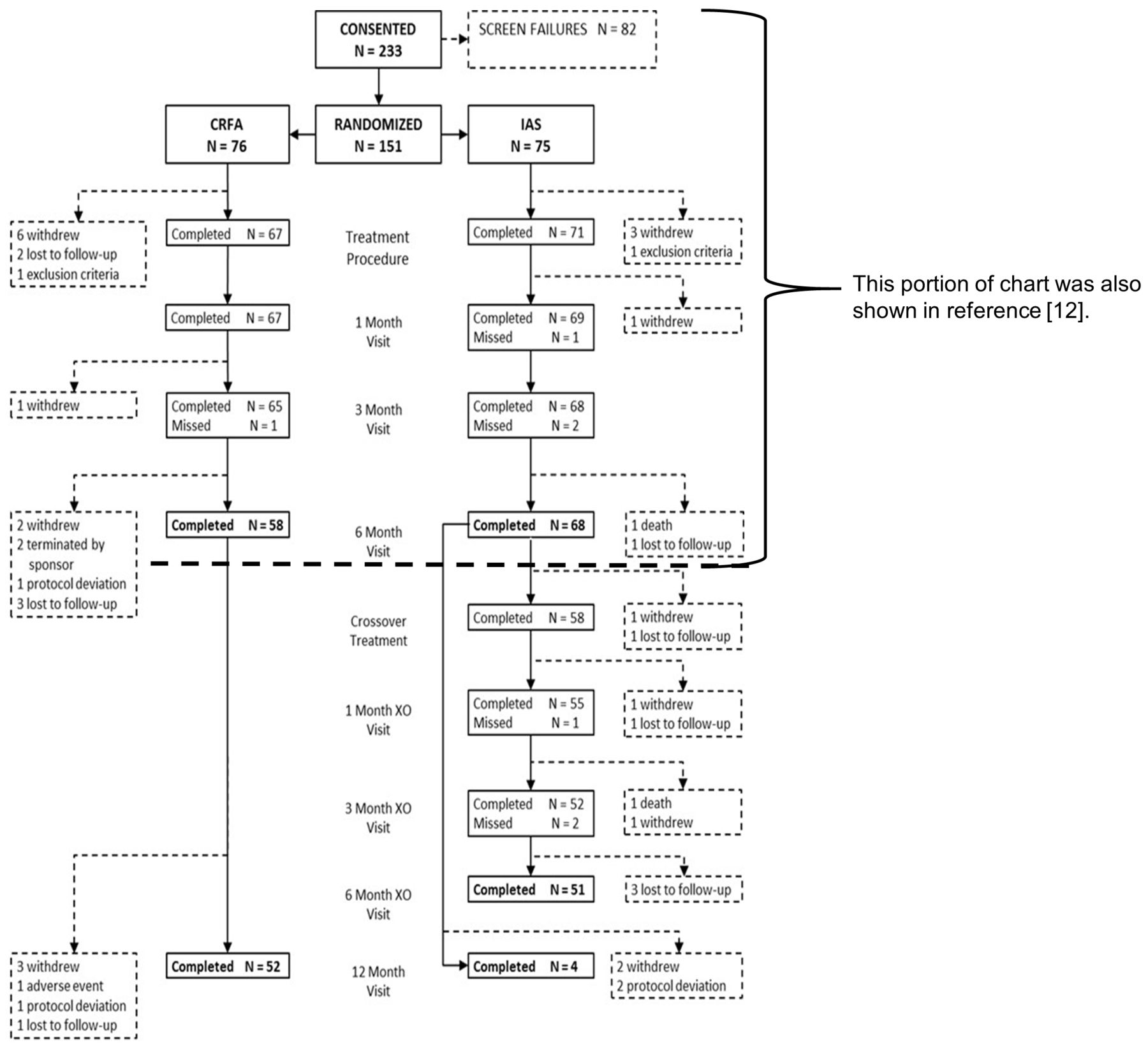
Out of the 233 patients screened, 151 were enrolled into the initial study,12 with 76 and 75 randomized to the CRFA and IAS study groups, respectively12 (figure 1). Of those randomized, 67 patients in the CRFA and 71 patients in the IAS group were treated.12 At 6 months, 58 (87%) and 68 (96%) of treated patients in the CRFA and IAS cohorts contributed data to the primary endpoint,12 and 58 (82%) patients of the IAS group crossed over to receive CRFA. At 12 months, 52 (78%) patients in the originally treated CRFA group contributed data to the primary endpoint, while at 6 months post-CRFA, 51 (88%) patients in the XO group did the same. Four patients (6%) of the IAS group completed the 12-month visit. At the time of cross-over eligibility, three of these four patients were not in severe enough pain to warrant intervention and one did not want the procedure due to comorbid conditions.

Consolidated Standards of Reporting Trials diagram displaying patients through study stages. *Two subjects were terminated by the sponsor, because the principal investigator changed jobs and a suitable replacement could not be identified. The site was closed, and subjects were dropped. **Adverse event—subject had return of index knee pain and chose a surgical alternative.
Study population
Baseline demographic variables, including age, gender and race distributions, mean BMI, mean duration of knee pain, analgesic medication utilization, knee OA severity, mean index knee pain levels (NRS scores) before diagnostic block, and the extent of index knee pain reduction postdiagnostic block were made available previously.12
Pain assessment in the original CRFA group at 12 months
Raw data are presented in table 1. The mean 4.3±2.7 (SD)-point decrease in NRS from baseline at 12 months in the original CRFA group was statistically significant (N=52, p<0.0001, paired Student’s t-test). The mean alteration in the NRS score at the 12-month time point was similar with that reported at 6 months, where a mean improvement of 4.9±2.4 points was identified.12 Further evidence for this sustained response to CRFA is shown in figure 2, where the mean NRS scores following CRFA are similar from 1 to 12 months. And whereas 70% (47/67) (95% CI 59.2 to 81.1), 72% (47/65) (95% CI 61.4 to 83.2) and 74% (43/58) (95% CI 62.9 to 85.4) of the CRFA group experienced diminished pain relative to baseline that was ≥50% at 1, 3, and 6 months, respectively12; 65% (34/52) (95% CI 52.5 to 78.3) of the group reported this clinically relevant15 outcome at 12 months.
Study outcomes: original CRFA group versus IAS group up to 12 months†

Mean pain scores (Numerical Rating Scale) in the cooled radiofrequency ablation cohort over time. SD are indicated in parentheses. Baseline, N=76; 1 month, N=67; 3 months, N=65; 6 months, N=58; 12 months, N=52. Baseline through 6-month values were previously reported.12
Secondary study outcomes in the original CRFA group at 12 months
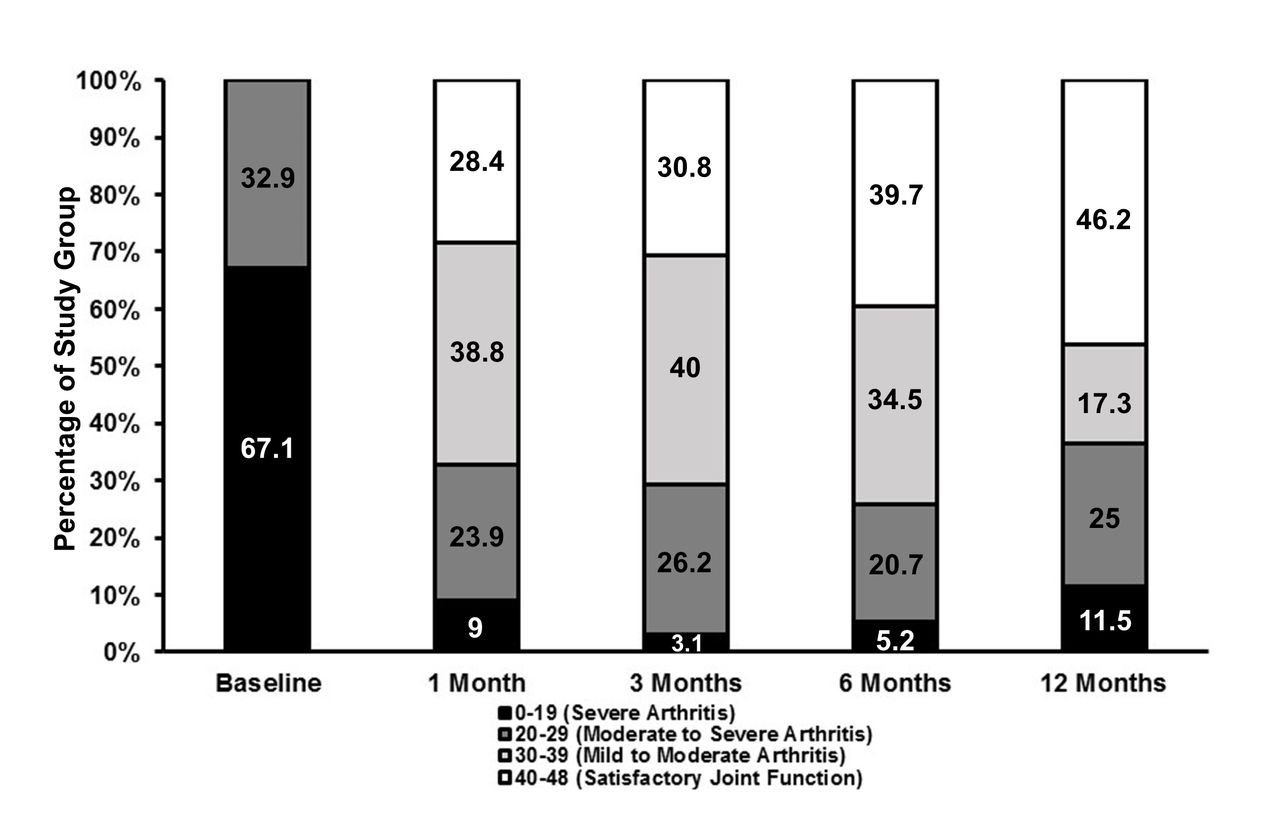
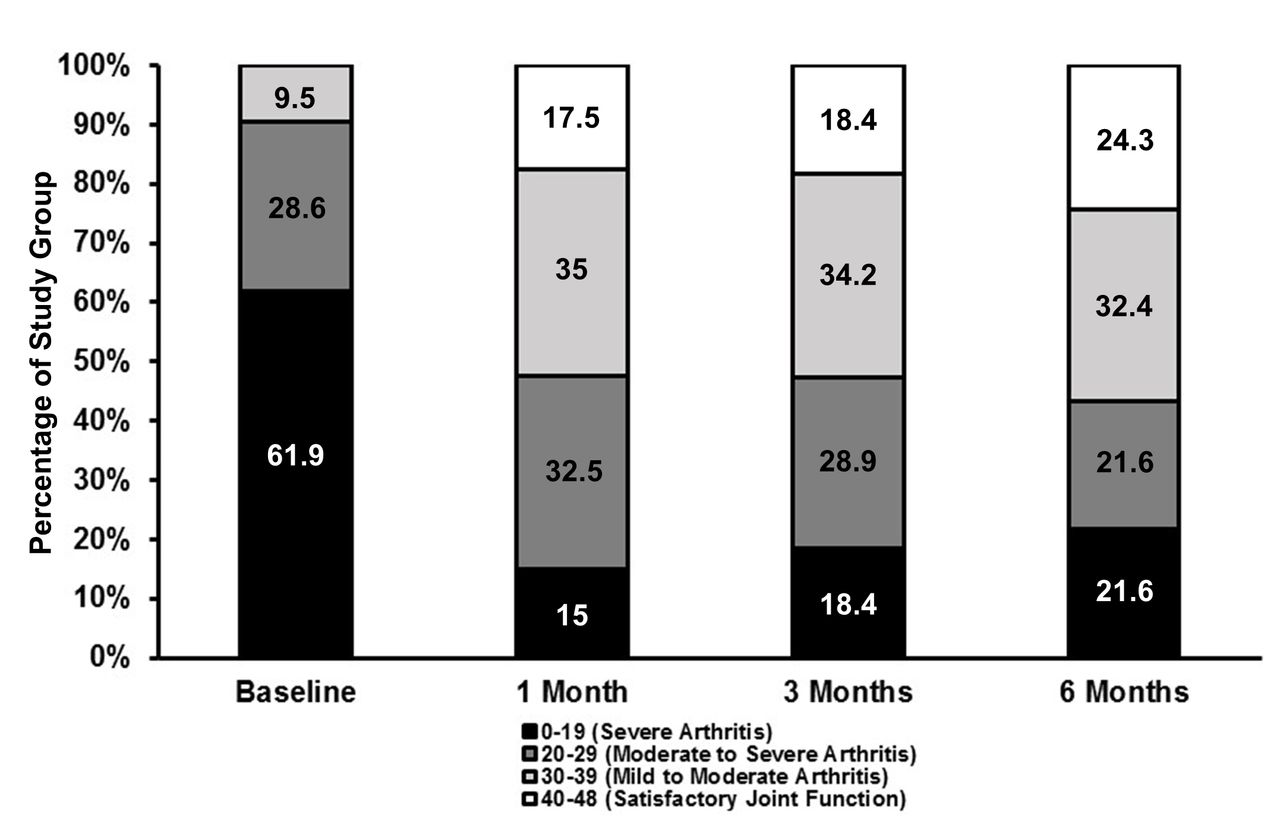
At 12 months, the OKS increase from baseline in the original CRFA cohort was 17.3±12 points (N=52, p<0.0001, Student’s paired t-test), with an absolute mean of 34.3±11.1 points. The fraction of patients in the CRFA group experiencing ‘severe arthritis’ and ‘satisfactory knee function’ (as defined by the OKS scale) with time post-treatment was inversely distributed (figure 3). Indeed, the percentage of patients reporting OKS ‘severe arthritis’ was progressively reduced from baseline to 6 months and was nearly sevenfold less at 12 months compared with baseline. In contrast, while there were no patients with OKS ‘satisfactory joint function’ in the CRFA group at baseline, the proportion of CRFA patients in this group consistently increased throughout the study, with nearly half reporting this outcome at 12 months. Patients who claimed ‘moderate to severe arthritis’ were approximately 25% at all time points, while those reporting ‘mild to moderate’ OKS were approximately 40% through 6 months, but then dropped to 17% at 12 months.
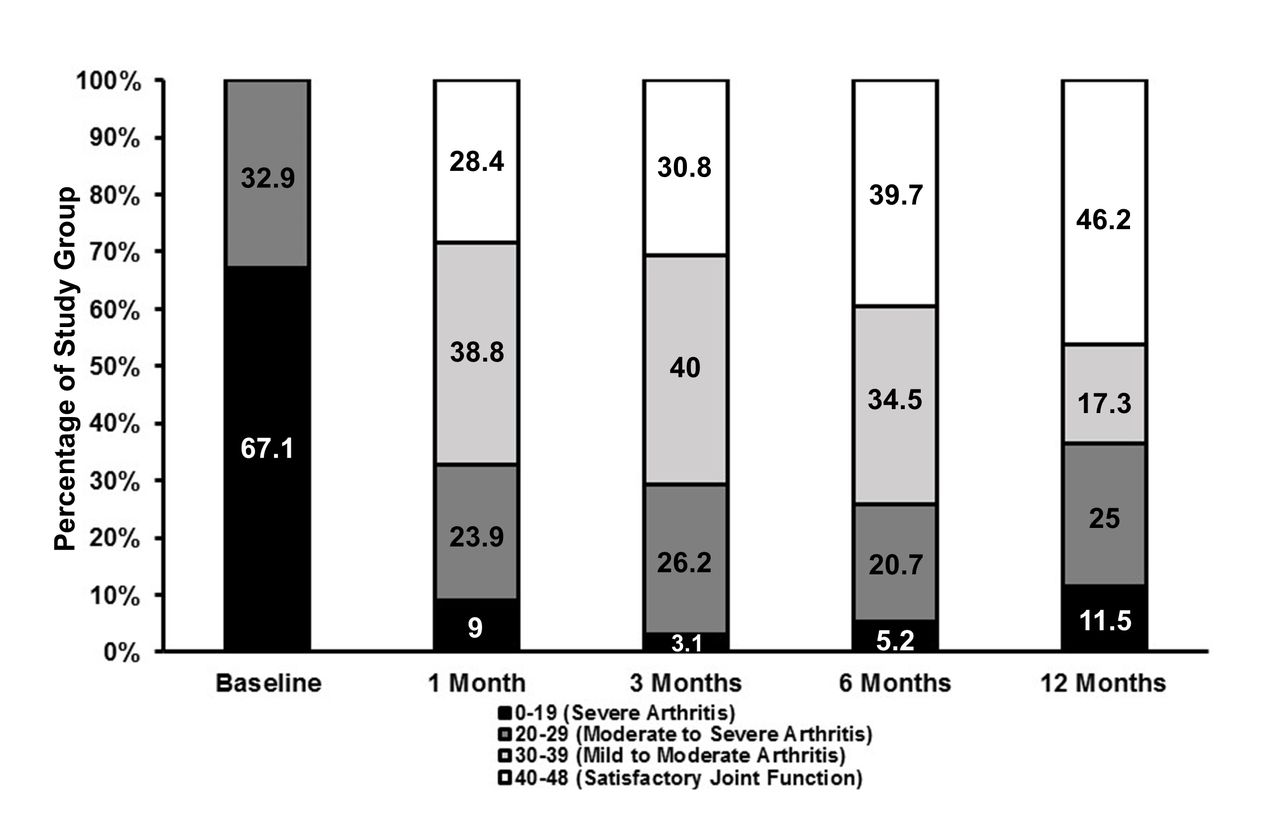
Knee function (Oxford Knee Scale) in the cooled radiofrequency ablation group over time. Baseline, N=76; 1 month, N=67; 3 months, N=65; 6 months, N=58; 12 months, N=52.
The proportion of patients in the CRFA group who had a perception of the treatment effect on their health as being ‘improved’ at 12 months was 75% (39/52) (95% CI 63.2 to 86.8), which was similar to values at 1 (79%, 53/67) (95% CI 69.4 to 88.8) and 3 months (80%, 52/65) (95% CI 70.3 to 89.7) post-treatment and substantially different than the baseline value of 17% (12/72) (95% CI 8.1 to 25.3).12 Proportions for all of the aforementioned time points are less than that observed at 6 months (91%, 53/58) (95% CI 84.2 to 98.6).12
The mean total daily dose in opioid analgesic medication (morphine equivalents in mg) in the CRFA group at 12 months was 30.3±27.4 mg (N=17), which was similar to the baseline value (delta=−1±10.3 mg, N=17, p=0.68, paired Student’s t-test). As noted in the previous publication, 43% of patients in the CRFA group who were taking opioids as of the study’s baseline assessment were using such medication for medical indications beyond OA related knee pain (ie, knee and back pain, back pain, etc). Additionally, a subgroup analysis was undertaken examining response to treatment of patients from the original CRFA group who were not taking opioids to manage their pain at study baseline. Fourteen of 67 (21%) patients fell into this category and of those, 11 (79%) patients indicated ≥50% relief of their baseline reported index knee pain at 6 months. This subgroup reported greater pain relief (mean NRS point reduction=6.1 at 6 months) than what was observed for the entire originally treated CRFA group at 6 (mean improvement=4.9 points) or 12 months (mean improvement=4.3 points).12
Pain assessment in the XO group at 6 months
The XO group had significant reductions from baseline, reporting mean changes of 3.1±2.5 points (N=40), 3.6±2.4 points (N=38), and 3.2±2.7 points (N=37) in the NRS at 1, 3, and 6 months, respectively (p<0.0001, paired Student’s t-test). These similar point reductions are reflected by the consistent NRS score means observed across the follow-up time points in this group (figure 4). Forty-nine per cent (18/37) (95% CI 32.5 to 64.8) of the XO group experienced clinically relevant15 pain relief compared with baseline that was ≥50% at 6 months.

Mean pain scores (Numerical Rating Scale) in the cross-over group over time. SD are indicated in parentheses. Baseline, N=66; 1 month, N=40; 3 months, N=38; 6 months, N=37.
Secondary study outcomes in the XO group at 6 months
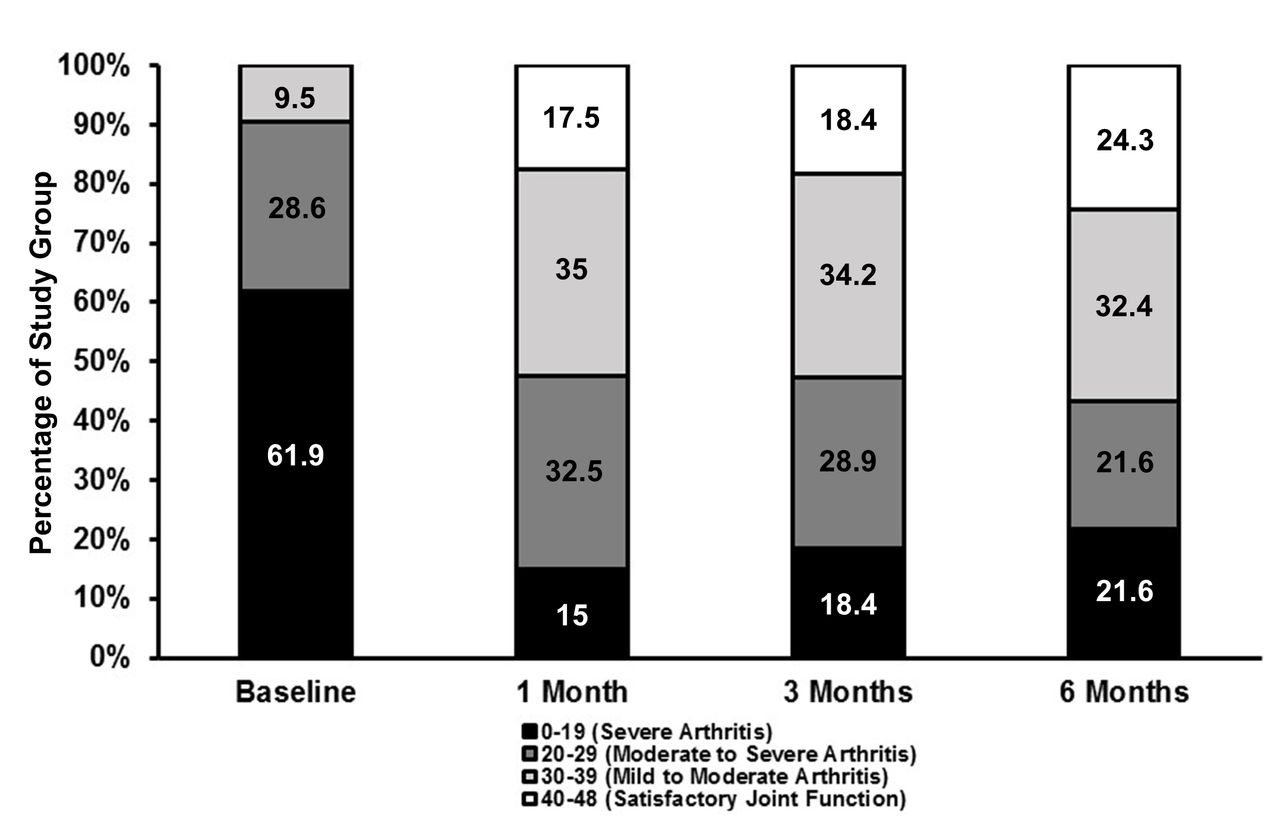
Improvements in function were also noted in the XO group, and the mean increase in the OKS from baseline in the XO group at 6 months was 11.6±9.8 points (N=36, p<0.0001, Student’s paired t-test). The mean OKS at each study time point was 18.6±6.6 (N=42), 30±9.4 (N=40), 30.3±10 (N=38), 29.8±10.6 (N=37), at baseline, 1, 3, and 6 months, respectively. While none of the XO patients reported OKS ‘satisfactory joint function’ at baseline (6 months post-IAS), approximately two-thirds of XO cohort members reported OKS ‘severe arthritis’ at this time point (figure 5). However, nearly one-fifth of the XO group reported OKS ‘satisfactory joint function’ 1 month after CRFA, and this condition progressively increased to include approximately one-quarter of the cohort by 6 months. In contrast, the incidence of OKS ‘severe arthritis’ in the XO group fell more than fourfold at 1 month and included approximately one-fifth of the cohort at 6 months. The frequency of OKS ‘moderate to severe arthritis’ fell by more than 10% from 1 to 6 months post-CRFA, while the proportion of patients having OKS ‘mild to moderate arthritis’ consistently remained at approximately 34% during this time frame.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Knee function (Oxford Knee Score) in the cross-over group over time. Baseline, N=42; 1 month, N=40; 3 months, N=38; 6 months, N=37.
While at the baseline (6 months post-IAS), 7.1% (3/42) (95% CI 0.0 to 14.9) of XO group members described the effect of CRFA on their health as ‘improved’, 65% (26/40) (95% CI 50.2 to 79.8), 79% (30/38) (95% CI 66.0 to 91.9), and 57% (21/37) (95% CI 40.8 to 72.7) of the group reported this outcome at 1, 3, and 6 months post-CRFA, respectively.
Radiographic evidence of knee OA
To understand the state of knee OA following CRFA, an amendment was added late in the study to collect x-rays at each subject’s final visit allowing for comparison to baseline OA status. Fifty-one radiographs were collected, 24 of which were from patients originally treated with CRFA. While most of these patients (58.3%;14/24) (95% CI 38.6 to 78.1) had no change in knee OA grade through 12 months, a worsening by one grade was detected in 8.3% (2/24) (95% CI 0.0 to 19.4) of the cohort. In the XO group, 27 radiographs were collected 6 months post-CRFA. These images revealed that 81.5% (22/27) (95% CI 66.8 to 96.1) of grades remained the same as reported at study entry, and worsening by one grade was identified in 7.4% (2/27) (95% CI 0.0 to 17.3) of this group. No patients worsened by more than one grade during the study.
Adverse events
There were 81 AEs that occurred among 42 CRFA patients between 6 and 12 months of the study. Non-SAEs included pain in the index knee (nine events—one of which led to subject discontinuation), with a decision to pursue a surgical alternative (1; figure 1**), pain in the non-index knee (3), musculoskeletal pain (9), and falls (5). SAEs occurred among four patients in the CRFA cohort from 6 to 12 months and included blood/lymphatic (3) and musculoskeletal (1) infections, cardiovascular (1), respiratory (3), gastrointestinal (1), and skin (1) events, and a non-CRFA procedure-related event that involved a musculoskeletal component. None of the SAEs were related to CRFA.
Discussion
The effect of CRFA to reduce index knee pain by at least 50% in the majority of the originally treated CRFA study group was sustained at 12 months and validated a portion of the study hypothesis, as 65% of this cohort experienced this benefit. The mean 4.3-point decrease on the NRS at 12 months compared well with 4.9-point drop that was observed at 6 months.12 Patients who elected to have CRFA after originally being treated with an IAS also reported analgesia, as the mean NRS pain score in the XO group fell at least 3.1 points up to 6 months postprocedure, and 49% of this population had at least 50% pain relief at 6 months, which confirmed the other portion of the study hypothesis. It is unknown why a difference in response was seen between the originally treated group and the XO group; however, the study was not powered or designed to draw specific conclusions from the XO group and this group should be considered observational given their participation and pathway in the trial. From a functional perspective, after CRFA, the incidence of patients having ‘satisfactory joint function’ was established and increased throughout the study in both cohorts, while the incidence of patients having ‘severe arthritis’ diminished with time in both groups. The majority of the originally treated and XO CRFA groups reported ‘improved’ perceptions of treatment effect on their health at 12 months and across all follow-up visits, respectively. Mean analgesic medication use was similar to baseline at 12 months in the originally treated CRFA group, and no unanticipated AEs occurred as a result of CRFA.
An effect of CRFA on opioid use in this investigation was not detected. As noted in the previous publication,12 multiple factors affected our ability to detect a difference in this area, including the duration at which subjects were on opioids prior to the trial, the addictive nature of opioids and the fact that nearly half of the subjects in the CRFA group were taking opioids for reasons beyond their knee pain. However, opioid use stayed consistent with baseline during the trial; therefore, the trial results noted are unlikely to be confounded by these medications.
Interestingly, for the patients described above who were not taking opioids to manage their pain at study baseline ((14/67) of the original CRFA group), 11 (79%) patients indicated ≥50% relief of their baseline reported index knee pain at 6 months and their 6.1 mean NRS point reduction was larger than the study wide 4.9-point decrease. Adequately powered studies are warranted to explore the suggestion that CRFA treatment prior to opioid use may be most beneficial to mitigate OA-related knee pain.
As radiographic analysis was not completed through a central lab, assessment variability is to be expected. However, given that less than 9% of subjects in both CRFA groups experienced OA grade worsening during the study (in similar ratios), a concern that CRFA unreasonably accelerates joint degeneration seems unfounded.
The current treatment algorithm for knee OA has limited effectiveness, and patients often suffer for extended periods before they qualify for TKA. Chronic use of non-steroidal anti-inflammatory drugs can introduce gastrointestinal, cardiovascular, and renal complications18; opioids present the risk of tolerance and addiction with escalating dosage over time19; physical therapy requires routine visits that increase healthcare expenditures; corticosteroid injections have limited duration of efficacy20 21; viscosupplementation efficacy is equivocal,22 23 as is platelet-rich plasma compared with viscosupplementation,24 25 and bracing may not be cost-effective.26 A TKA is a well-established and successful procedure,1 2 but there are certain populations where one could argue for a more conservative option,27 such as when patients are not yet considered ‘operative’, or have comorbid health issues that would preclude them from surgery or increase the risk profile for undergoing a TKA. A large subgroup of patients who may be not be considered for TKA, such as those with poor glucose control and/or obesity, may become candidates following 6 months to 1 year of mobilization and weight loss afforded by undergoing CRFA first.
This study indicates that large percentages of patients can receive a durable analgesic effect from CRFA, which contrasts with other non-operative treatment options for patients with knee OA.20–25 Additionally, at the time of this publication, Santana et al produced the only standard RF knee OA series in the literature providing information to 12 months,7 with a mean NRS score reported of 5.8, compared with the mean NRS score of 3.1 in the current CRFA series. While few head-to-head studies exist comparing standard versus cooled radiofrequency directly, such observations are consistent with previous suggestions that the cooling characteristic of CRFA facilitates a larger lesion size than standard RF,28 thus, making it more likely that target nerves will be ablated by the CRFA, and perhaps prolonging the time required to complete nerve regeneration.29 Further study is needed to examine potential differences between the two technologies.
The beneficial outcomes observed in this current report with respect to CRFA treatment of knee OA extend the bibliography of publications having similar results using CRFA.9–11 Our study is the largest prospective randomized comparison to date observing the changes in pain and disability in patients undergoing CRFA. Within this context, the results show that CRFA is safe and durable, thus providing patients who are ineligible for TKA with a seemingly more effective option than IAS,12 and perhaps other conservative therapies, to gain relief from OA-related knee pain and disability. For those who are TKA candidates, but wish to postpone such a relatively more invasive intervention in favor of CRFA first, evidence suggests benefits of RF-facilitated denervation in this scenario. Taverner et al demonstrated that pulsed RF, but not sham treatment, of patients with painful knees afforded them with a significant pain relief at rest and during exercise prior to total knee joint replacement.30 Carli and co-workers used pulsed and thermal RFA to denervate nociceptive nerves of the knee13 of a 79-year-old woman with severe knee OA that required TKA.31 The patient had significant knee pain that was unrelieved by opioids, and severely impaired functional activity. The authors attributed significant improvement in the objective and self-reported outcome measures recorded during the 6 weeks of prehabilitation before surgery to the patient’s denervation-facilitated preoperative analgesia. The successful prehabilitation was hypothesized to enable rehabilitation implementation post-TKA. The significant gains in functional improvement identified during this study warrant further exploration into this patient population, and large, adequately powered studies (ClinicalTrials.gov identifiers: NCT02746874 and NCT02925442) are in progress to investigate this seemingly purposeful synergistic clinical approach to knee OA between RF-mediated denervation and TKA.
A limitation of this study is the one-way XO option, from IAS to CRFA, but not vice versa. This paradigm is consistent with the intention of the study to test CRFA as a rescue intervention for knee OA, rather than long-standing, conservative IAS. The limitations of this portion of the study are that the remaining IAS group sample size was not large enough to perform statistical test-based comparisons between the originally treated CRFA patients and the IAS group members at 12 months, outcomes of the originally treated CRFA group and those of the XO cohort could not be directly compared at 6 months, because the groups were derived from two different study populations, and an effect of CRFA on opioid use could not be detected, perhaps due to alternate patient conditions that also utilized opioids as therapy. Further, the late addition of the amendment to collect X-rays at the final visit limited our ability to capture data on a large portion of the patients enrolled.
Statistically significant and clinically relevant pain relief and functional improvements were sustained 12 months following CRFA treatment of OA-related knee pain and dysfunction. These effects were reflected by patients’ perceptions of their ‘improved‘ health 12 months following CRFA. Moreover, CRFA may rescue patients who have been dissatisfied with results of prior IAS for OA knee pain and who are not candidates for TKA.
References
Footnotes
Contributors All authors equally contributed in completing this manuscript.
Funding Financial support was provided to each of the investigator’s institutions by Halyard Health to cover the budgeted costs necessary to conduct this study protocol. Data management, study site monitoring and statistics services were performed by a third party, independently of Halyard Health.
Disclaimer This study and its 6-month results were presented as poster and platform abstracts at the American Society of Regional Anesthesia and Pain Medicine (ASRA) 2016 (November) Meeting in San Diego, California, USA, and the American Academy of Pain Medicine (AAPM) 2017 (March) Meeting in Orlando, Florida, USA, and have been published in manuscript form in Regional Anesthesia and Pain Medicine. The 12-month data in this report were presented at the European Society of Regional Anesthesia (ESRA) Congress 2017 in Lugano, Switzerland.
Competing interests TD, DePalma, MD, and LK are paid consultants (clinicaladvisory board) for Halyard Health.
Patient consent for publication Obtained.
Ethics approval This study was approved for engagement by the Western Institutional Review Board (IRB; Puyallup, Washington, USA) and Rush University Medical Center IRB (Chicago, Illinois, USA).
Provenance and peer review Not commissioned; externally peer reviewed.