Article Text

Abstract
Background and objectives Perineural dexamethasone or dexmedetomidine prolongs the duration of single-injection peripheral nerve block when added to the local anesthetic solution. In a randomized, controlled, double-blinded study in patients undergoing thoracoscopic pneumonectomy, we tested the hypothesis that combined perineural dexamethasone and dexmedetomidine prolonged the duration of analgesia as compared with either perineural dexamethasone or perineural dexmedetomidine after intercostal nerve block (INB).
Methods Eighty patients were randomized to receive INB using 28 mL 0.5% ropivacaine, with 2 mL normal saline (R group), with 10 mg dexamethasone in 2 mL (RS group) or 1 µg/kg dexmedetomidine in 2 mL (RM group), or with 1 µg/kg dexmedetomidine and 10 mg dexamethasone in 2 mL (RSM group) administrated perineurally. The INB was performed by the surgeon under thoracoscopic direct vision; a total of six intercostal spaces were involved, each with an injection of 5 mL. The primary outcome was the duration of analgesia. Secondary outcomes included total postoperative fentanyl consumption, visual analog scale pain score and safety assessment (adverse effects).
Results The duration of analgesia in RSM (824.2±105.1 min) was longer than that in RS (611.5±133.0 min), RM (602.5±108.5 min) and R (440.0±109.6 min) (p<0.001). Total postoperative fentanyl consumption was lower in RSM (106.0±84.0 µg) compared with RS (243.0±175.2 µg), RM (237.0±98.7 µg) and R (369.0±134.2 µg) (p<0.001). No significant difference was observed in the incidences of adverse effects between the four groups.
Conclusion The addition of combined perineural dexmedetomidine and dexamethasone to ropivacaine for INB seemed to be an attractive method for prolonged analgesia with almost no adverse effects.
Trial registration number ChiCTR-IOR-17012183.
- dexamethasone
- dexmedetomidine
- intercostal nerve block
- thoracoscopic pneumonectomy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Single-injection peripheral nerve block (PNB) is commonly used for perioperative analgesia and anesthesia.1 Although PNB are beneficial for improved early postoperative pain management, it is often insufficient, as postoperative pain can persist for several days. The aim of prolonging the duration of PNB to treat postoperative pain is a key issue in regional anesthesia. Three approaches for extending the duration of PNB include continuous PNB with catheter-based techniques, novel local anesthetics delivery systems and addition of novel adjuvants to local anesthetics.2
Adjuvants that are frequently added to local anesthetics to prolong analgesia following single-injection PNB include epinephrine, opioids, tramadol, ketamine, midazolam, magnesium, clonidine, dexmedetomidine and dexamethasone, but often with limited success and unproven safety.3–6 Studies of perineural buprenorphine, dexamethasone and dexmedetomidine have most consistently demonstrated prolongation of PNB.5
Dexamethasone is a potent long-acting steroid that has shown efficacy as an adjuvant to local anesthetics in various studies.7 8 Dexmedetomidine enhances PNB when added to local anesthetics, providing better quality of anesthesia as well as postoperative analgesia.9 10 The mechanism by which dexamethasone and dexmedetomidine prolong the duration of local anesthetics are not completely understood and may arise from various factors. Both dexamethasone and dexmedetomidine can reduce local inflammation and prolong the duration of nerve block through vasoconstriction by maintaining the local concentration of the local anesthetic.11–14 Vasoconstriction also inhibits the nociceptive impulse transmission along myelinated C fibers.15 Possible mechanisms of dexmedetomidine in prolonging the duration of nerve blocks may also include the inhibition of the hyperpolarization-activated cation current (Ih current).16 Some research suggests that dexmedetomidine may provide local anesthetic action that blocks the conduction of nerve signals through C and Aδ fibers, not through α2 action, and may stimulate the release of enkephalin-like substances at peripheral sites.17
Due to the different mechanisms of action, we hypothesized that ropivacaine combined with both perineural dexamethasone and dexmedetomidine could further prolong the duration of PNB. Therefore, we performed a prospective, randomized, double-blinded, controlled trial to investigate whether the addition of two adjuvants (dexmedetomidine and dexamethasone) to ropivacaine for INB prolongs block duration and therefore improves postoperative analgesia, as compared with each adjuvant alone with ropivacaine.
Methods
Trial design and participants
After providing written informed consent, patients with American Society of Anesthesiologists (ASA) physical status classes I and II, aged 28–68 years and scheduled for thoracoscopic pneumonectomy between September 2017 and April 2018 were considered eligible to participate in this prospective, randomized, double-blinded clinical trial. Major exclusion criteria were: hypertension; ischemic heart disease; psychiatric disorders; preoperative heart rate (HR) less than 50 beats/min with/without cardiac conduction or rhythm abnormalities; diabetes mellitus; neuromuscular and endocrine diseases; coagulation disorders; adrenoreceptor agonist or antagonist therapy; chronic pain treatment or chronic steroid therapy; allergy to the study drugs and refusal to participate in the study. Individuals who had an estimated intraoperative blood loss of more than 500 mL were subsequently excluded from the study. Those who were transferred to an open chest operation, those who required a second operation for postoperative hemorrhage and those who presented severe postoperative infection were also subsequently excluded from the study.
Randomization and blinding
A computer-generated random numbers list was used to randomize consented study participants on a 1:1:1:1 ratio to receive INB with trial medication.
Group R (control): 28 mL of ropivacaine 0.5%+2 mL normal saline.
Group RS: 28 mL of ropivacaine 0.5%+perineural dexamethasone 10 mg in 2 mL.
Group RM: 28 mL of ropivacaine 0.5%+perineural dexmedetomidine 1 µg/kg in 2 mL.
Group RSM: 28 mL of ropivacaine 0.5%+perineural dexamethasone 10 mg and perineural dexmedetomidine 1 µg/kg in 2 mL.
The volume of study drug was always 30 mL. All patients were not administered intravenous dexmedetomidine or dexamethasone perioperatively. Their patient-controlled intravenous analgesia (PCIA) protocol was programmed with 1 mg fentanyl diluted to 100 mL (3 mL bolus, lockout time interval of 8 min and 1 hour limit of 15 mL without any baseline infusion). The randomization table was kept in the hospital pharmacy. The study medication and PCIA solutions were prepared by a nurse who did not participate in the study. The patients, surgeon and research staff who enrolled patients and collected study data were blinded to group assignment.
Interventions
Before the study procedure, all the patients were trained how to use the PCIA pump and also instructed on using a 10 cm visual analog scale (VAS; with 0: no pain, to 10: the worst imaginable pain).
On arrival in the operating room, an 18-gage intravenous cannula was inserted into a peripheral vein on the arm, and an infusion of lactated Ringer’s solution was started. Five-lead ECG, HR, invasive blood pressure, respiratory rate (RR) and pulse oxygen saturation (SpO2) were continuously monitored. General anesthesia was induced with 0.08–0.10 mg/kg of midazolam, 0.15–0.30 mg/kg of etomidate, 2–4 µg/kg of fentanyl and 0.12 mg/kg of cisatracurium. Maintenance of anesthesia was achieved with propofol, sevoflurane, remifentanil and atracurium.
At the end of the surgery, the INB was performed by the surgeon under thoracoscopic direct vision. At the site of the surgical incision (generally three incisions, usually between ribs 4–8) and including the adjacent upper and lower two intercostal spaces, a total of six intercostal spaces were involved, each with an injection of 5 mL. All patients received PCIA for postoperative analgesia. PCIA was administered for VAS ≥4 or on patient request.
Outcomes
Duration of analgesia, defined as time in minutes to the first request for analgesic, was designated as the primary outcome. Total postoperative fentanyl consumption was also recorded within the 48-hour period. In the postanesthesia care unit, time of tracheal extubation was recorded. The patients’ HR, mean arterial pressure (MAP), VAS at rest and Ramsay Sedation Score (RSS) (1: anxious patient; 2: cooperative and tranquil; 3: responding to command; 4: brisk response to stimulus; 5: sluggish response to stimulus; 6: no response to stimulus) were assessed before surgery (baseline) and at 6 hours, 12 hours, 24 hours, 36 hours and 48 hours after surgery.
Side effects such as bradycardia (HR <50 beats/min), hypoxemia (SpO2 <90%), hypotension (systolic blood pressure <90 mmHg or more than 20% decline from the baseline), respiratory depression (RR <10beats/min lasting for more than 10 min), headache, pruritus, nausea, vomiting and neurotoxicity were recorded after surgery, whereas hypotension was treated with fluid loading, intravenous ephedrine or phenylephrine. In addition, bradycardia was treated with atropine. Respiratory depression was treated with oxygen or naloxone until RR ≥15 beats/min.
Statistical analysis
Duration of analgesia was the primary outcome. We hypothesized that perineural dexamethasone and dexmedetomidine combined (RSM group) prolonged the duration of analgesia compared with single adjuvant groups of perineural dexamethasone (RS group) or perineural dexmedetomidine (RM group) after INB. In our preliminary study conducted with eight patients (two in each group), the mean duration of analgesia was 500±160 min, 570±226 min, 550±147 min, 767±184 min in groups R, RS, RM and RSM. Sample size calculation was performed with PASS V.11.0 (PASS, NCSS, USA) for Windows. One-way analysis of variance (ANOVA) was selected and grouped into four groups, group allocation ratios were equal, hypothesized means were 570, 550 and 767 and SD were 226, 147 and 184, respectively. At a power of 0.80 and an alpha error of 0.05, the required sample size for each group was calculated to be 15. Considering the dropouts and incomplete follow-up, suggested 20 patients per group and a total of 80 patients for this study.
Statistical analysis was performed with SPSS V.24.0 for Windows and GraphPad Prism 6 (GraphPad Software, La Jolla, California, USA). For duration of analgesia, total postoperative fentanyl consumption and VAS data, ANOVA followed by the Bonferroni post hoc test was used. For time-to-event outcomes, we analyzed data using the Kaplan-Meier survival method and compared groups using the log-rank test, with adjustment for multiple comparisons. Repeated measures ANOVA with Bonferroni correction was used for MAP and HR data. Categorical data (the incidence of side effects) were presented as frequencies (%) and analyzed using Fisher’s exact test. P<0.05 value was considered to be statistically significant.
Results
A total of 151 patients were approached to participate in this study from September 2017 to April 2018; 54 patients were ineligible due to not meeting inclusion criteria or refusal to participate; 17 patients were excluded because of non-adherence to the protocol (three patients refused to participate in the study after surgery; two patients converted to open surgery; three patients hemorrhage need transfusion; four patients lost to follow-up; one patient underwent second surgery in 48 hours; two patients refused to use PICA after surgery; and two patients developed actelectasis in 24 hours); and finally, 80 patients were randomized and completed the study protocol (R group: n=20; RS group: n=20; RM group: n=20; and RSM group: n=20). Figure 1 represents the Consolidated Standards of Reporting Trials flow diagram depicting patient progress through the study phases.

Patient enrollment, inclusion and exclusion process. PICA, patient-controlled intravenous analgesia.
A total of 80 patients were included for analysis in the study. No significant differences in patient characteristics were evident between each group (table 1).
Demographic data and surgical characteristics
The duration of analgesia was significantly longer in group RSM compared with the other three groups (p<0.001). Compared with group RS and group RM, the duration of analgesia was significantly shorter in group R (p<0.001). There was no significant difference between group RS and group RM (p=1.000) (table 2). The Kaplan-Meier survival analysis of the time to the first analgesic request was shown in figure 2. The log-rank test also suggested prolongation of the first analgesic request for group RSM compared with the other three groups (p<0.001). Compared with group RS and group RM, the first analgesic request was significantly shorter in group R (p<0.001). There was no significant difference between group RS and group RM (p=1.000).

Kaplan-Meier survival plot representing the first analgesic request in the four groups. *P<0.001 between RSM and other groups. #P<0.001 between RS, RM and R group. R, ropivacaine; RM, ropivacaine+dexmedetomidine; RS, ropivacaine+dexamethasone; RSM, ropivacaine+dexamethasone+dexmedetomidine.
Duration of analgesia and total postoperative fentanyl consumption
Total postoperative fentanyl consumption in group RSM was lower than that the other three groups (p<0.001). Compared with group RS and group RM, total postoperative fentanyl consumption was significantly higher in group R (p=0.016 and p=0.010, respectively). There was no significant difference between group RS and group RM (p=1.000) (table 2).
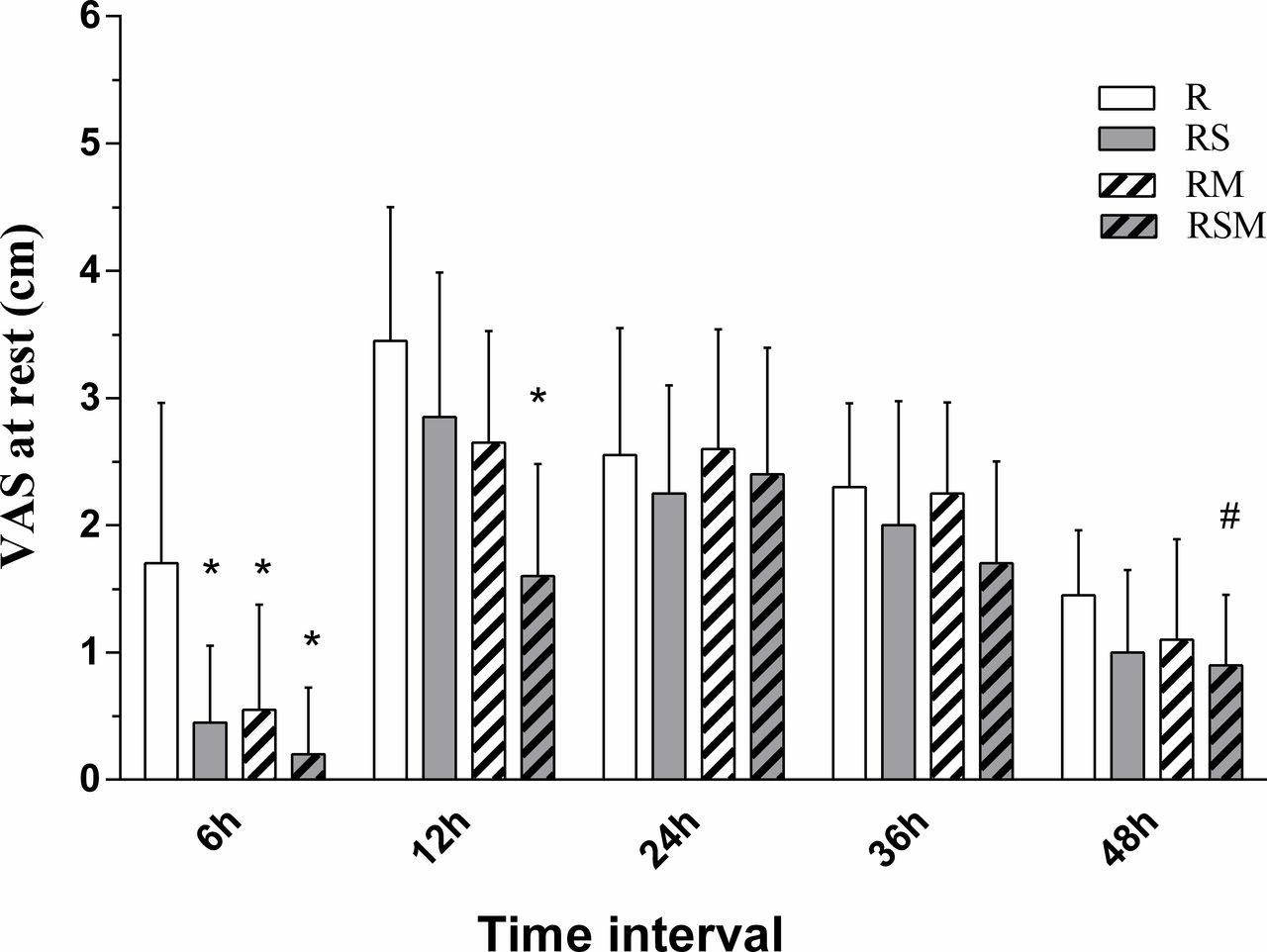
At 6 hours postoperatively, VAS in group R was higher than those in the other three groups (p<0.001). At 12 hours postoperatively, VAS in group RSM was lower compared with group RS, group RM and group R (p<0.001). At 48 hours postoperatively, VAS was lower in group RSM compared with group R (p=0.043). There were no significant differences in VAS among the four groups at 24 hours and 36 hours postoperatively (p=0.645 and p=0.076, respectively) (figure 3).

Postoperative pain severity VAS score at rest (in cm) at 6, 12, 24, 36 and 48 hours postoperatively. At 6 hours postoperatively, *p<0.001 group R compared with groups RS, RM and RSM. At 12 hours postoperatively, *p<0.001 group RSM compared with groups RS, RM and R. At 48 hours postoperatively, #p=0.043 between groups RSM and R. R, ropivacaine; RM, ropivacaine+dexmedetomidine; RS, ropivacaine+dexamethasone; RSM, ropivacaine+dexamethasone+dexmedetomidine; VAS, visual analog scale.
The discrepancies of MAP and HR acquired at different time points were statistically significant (P<0.001). No significant differences were observed between the study groups (P=0.242 and P=0.792, respectively) (figures 4 and 5).

MAP changes at different times in each group. In all groups, the changes in MAP showed a significant difference in relation to time with *p<0.001. MAP, mean arterial blood pressure; R, ropivacaine; RM, ropivacaine+dexmedetomidine; RS, ropivacaine+dexamethasone; RSM, ropivacaine+dexamethasone+dexmedetomidine.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Heart rate changes at different times in each group. In all groups, the changes in HR showed a significant difference in relation to time with *p<0.001. HR, heart rate; R, ropivacaine; RM, ropivacaine+dexmedetomidine; RS, ropivacaine+dexamethasone; RSM, ropivacaine+dexamethasone+dexmedetomidine.
The number of patients experiencing side effects was reported in table 3. No significant differences were observed in the incidences of hypotension, hypoxemia, respiratory depression, vomiting, nausea, pruritus or dizziness among the four groups. The RSS was two in all patients.
Incidence of side effects
Discussion
In this study, we demonstrated that ropivacaine combined with two perineural adjuvants (dexamethasone and dexmedetomidine) can further prolong the duration of analgesia and reduce the consumption of fentanyl compared with ropivacaine combined with a single perineural adjuvant (dexamethasone or dexmedetomidine) or ropivacaine alone in patients undergoing thoracoscopic pneumonectomy with almost no adverse effects.
Although there are multiple adjuvants that could extend the duration of local anesthetics, it was worth noting that the ability of adjuvants to prolong nerve block may have a ceiling.18 Similar effect might not have been achieved by simply increasing the dosage of dexamethasone or dexmedetomidine. In the context of that knowledge, we raised the question: could the combination of two adjuvants further prolong the duration of nerve block? From this study, we found that dual agent combination perineural adjuvant drugs increased the duration of effect of ropivacaine almost twofold. This interesting observation was in accordance with the work of Hassan and colleagues,19 who observed that the combination of both dexamethasone and dexmedetomidine could further prolonged the sensory block of the caudal block. As local anesthetic adjuvants, dexamethasone and dexmedetomidine might have synergistic or additive effects. Unfortunately, our study has the same flaws as the above study (no intravenous control group), which made it impossible to determine whether the effect was due to systemic or local effects.
Thakur et al 20 reported that 1 µg/kg dexmedetomidine was nearly the ideal dose as an adjuvant in axillary blocks and that this dose increases the duration of postoperative analgesia and delays the requirement of the first dose of analgesic. Although dexamethasone was widely used clinically, the optimal dose of dexamethasone as a local anesthetic adjuvant was inconsistent. Previous studies have shown that dexamethasone demonstrated significant beneficial dose-dependent effects as an adjuvant for local anesthetic.21 Recent studies have shown that perineural high doses of dexamethasone have no advantage, and low doses of dexamethasone are advocated.22 A recent meta-analysis showed very low quality evidence that there was a ceiling effect of dexamethasone at 4 mg.23 However, the latest research findings that both intravenous and perineural administered dexamethasone 4 mg has no clinically relevant effect on the duration of sensory block provided by ropivacaine applied to the ulnar nerve in volunteers.24 In addition, in the current study, we used a higher dose of dexamethasone than other experts have recommended. Although no permanent complications associated with nerve block could be attributed to the use of dexamethasone, considering that high doses of dexamethasone may increase potential risks, we no longer recommend high doses of dexamethasone administered perineurally.25 Therefore, the effective dose of dexamethasone as an adjuvant for local anesthesia needs further study.
There are a number of limitations associated with the present study. First, this study lacks an intravenous control. It would have required more than four groups by adding the intravenous group, making calculations and statistical analysis of the sample size more difficult. However, without intravenous control, we cannot ascertain whether the addition of either dexamethasone or dexmedetomidine was via systemic absorption or through perineural action. Second, we used a higher dose of dexamethasone than other experts have recommended. Third, VAS scores were measured only at rest, thus this reduces the usefulness of the results provided. Fourth, we did not assess the duration of the sensory block in patients using repeated neurological examinations. Considering that frequent testing of sensory block after surgery can affect patients’ rest, the time from the end of INB to the first use of fentanyl after operation indicates the duration of analgesia. Fifth, dexamethasone and dexmedetomidine are used off-label. Even though it is widely used on an international level and has been investigated in many scientific trials, the US Food and Drug Administration does not approve dexamethasone or dexmedetomidine for perineural administration. Regarding the inconclusive data on the safety of perineural dexamethasone and dexmedetomidine, we would like to remind clinicians that this ‘off-label’ use needs approval of the appropriate regulatory health institutions. Finally, our calculation of the number of patients who were needed in our study might not adequate, so the study power cannot differentiate statistically significant differences between the dexamethasone and dexmedetomidine. Of course, further research is needed to confirm this.
Conclusions
We demonstrated that patients undergoing thoracoscopic pneumonectomy with the addition of perineural 10 mg dexamethasone and 1 µg/kg dexmedetomidine to 0.5% ropivacaine for INB had further increases in the duration of analgesia and decreases in postoperative fentanyl consumption compared with patients who did not receive this combination of drugs.
Acknowledgments
The authors thank Min Yu, PhD, and Youli Hu, PhD (Department of Anesthesiology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu Province, China) for their critical review of the manuscript. The authors would like to thank all the members of Thoracic Surgery Department (The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu Province, China) for their great help and support.
References
Footnotes
PZ and SL contributed equally.
ZR and CL contributed equally.
Contributors All authors helped design the study. PZ, ZR and CL helped conduct of the study. PZ, SL, ZR and CL helped recruit the patients. JZ, ZR and CL helped collect the data. PZ, SL, ZR and CL helped analyze the data. PZ, SL and CL was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study protocol was approved by the Ethics Committee of The First Affiliated Hospital of Nanjing Medical University (Nanjing, Jiangsu Province, China) and was prospectively registered on Chinese Clinical Trial Registry (registration number ChiCTR-IOR-17012183).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.