Article Text

Abstract
The advent of ultrasound guidance has led to a renewed interest in regional anesthesia of the lower limb. In keeping with the American Society of Regional Anesthesia and Pain Medicine’s ongoing commitment to provide intensive evidence-based education, this article presents a complete update of the 2005 comprehensive review on lower extremity peripheral nerve blocks. The current review article strives to (1) summarize the pertinent anatomy of the lumbar and sacral plexuses, (2) discuss the optimal approaches and techniques for lower limb regional anesthesia, (3) present evidence to guide the selection of pharmacological agents and adjuvants, (4) describe potential complications associated with lower extremity nerve blocks, and (5) identify informational gaps pertaining to outcomes, which warrant further investigation.
Statistics from Altmetric.com
Introduction
Historically, lower extremity nerve blocks have been less widely used than their brachial plexus counterparts.1 Reasons may include the fact that anesthesia of the lower limb requires blockade of several different nerves, whereas neuraxial blocks can provide intraoperative anesthesia and postoperative analgesia with a single puncture site. Furthermore, the depth of many nerves supplying the lower limb also constitutes a physical deterrent. However, since the new millennium, factors such as the increasing use of antithromboembolic prophylaxis and the advent of ultrasound (US) guidance have led to a renewed interest in regional anesthesia of the lower limb. In 2005, Regional Anesthesia and Pain Medicine published a review article that summarized the essentials of the contemporary understanding of lower extremity peripheral nerve blockade.1 In the last 13 years, the field has progressed by leaps and bounds, as novel anatomical concepts (eg, paraneurium and subparaneural compartment), new blocks (ie, femoral triangle and adductor canal blocks), improved descriptions for US-guided techniques (eg, “Shamrock” lumbar plexus block), and novel applications (eg, motor-sparing nerve blocks for total knee arthroplasty) have emerged in the literature. In light of the temporal gap between the current and previous review article, we have elected not to carry out a simple update but to address the topic in its entirety. Although the current review article does not aim to set medico-legal standards, it does strive to (1) summarize the pertinent anatomy of the lumbar and sacral plexuses, (2) discuss the optimal approaches and techniques for lower limb regional anesthesia, (3) present the available evidence to guide the selection of pharmacological agents and adjuvants, (4) describe potential complications associated with lower extremity nerve blocks, and (5) identify informational gaps pertaining to outcomes, which warrant further investigation.
Neuroanatomy of the lower limb
Lower extremity peripheral nerve blocks require a thorough understanding of the neuroanatomy of the lumbosacral plexus (figure 1), which is formed from the ventral primary rami of the 12th thoracic to the fourth sacral spinal nerves (T12–S4)2 and provides sensory as well as motor innervation to the entire lower extremity, including the hip, knee, and ankle joints. The lumbosacral trunk (L4–S1) provides an anatomical communication between the lumbar and sacral plexus. However, for functional purposes, the two plexuses are usually considered distinct clinical entities and will be hereby discussed separately. Branches of the lumbar plexus include the iliohypogastric, ilioinguinal, genitofemoral, lateral femoral cutaneous, femoral, and obturator nerves. Of these, the lateral femoral cutaneous, femoral, and obturator nerves are the most important for lower extremity anesthesia and analgesia. The lumbar plexus usually lies deep within the substance of the psoas major muscle, anterior to the transverse processes of L1-L4 vertebrae whereas the sacral plexus can be found within the pelvis anterior to the piriformis muscle. The sacral plexus gives rise to 12 peripheral nerves, but the sciatic and posterior femoral cutaneous nerves are the most pertinent for lower extremity anesthesia and analgesia.

Idealized lumbar and sacral plexuses. Illustration by Jennifer Gentry. Copyright Jennifer Gentry, American Society of Regional Anesthesia and Pain Medicine.
There exists a multitude of anatomical approaches and nerve localization techniques to anesthetize the lumbar plexus, sacral plexu, and their peripheral branches. Thus, a review of the anatomical course of the two plexuses and their most relevant peripheral nerves is warranted.
Lumbar plexus anatomy
As the L1–L4 spinal nerve roots emerge from their respective intervertebral foramina, they lie anterior to the corresponding transverse processes and are typically embedded within a fascial plane located between the anterior and posterior portions of the psoas major muscle.3–9 The smaller posterior layer of the psoas major originates from the anterior surfaces and lower borders of the L1–L5 transverse processes while the larger anterior layer originates from the lateral surfaces of the respective vertebral bodies and intervertebral discs.3–9 Cadaveric and imaging studies have demonstrated that the lumbar plexus may also be located between the posterior border of the psoas major and the anterior border of the quadratus lumborum muscle in a small percentage of the population.8–10 Within the psoas major, the ventral rami divide into anterior and posterior branches, which subsequently reunite to give rise to the individual peripheral nerves of the lumbar plexus. These nerves descend vertically within the mass of the psoas major. At the level of the L4–L5 transverse processes, the lateral femoral cutaneous nerve is located in the lateral portion of the psoas major, the obturator is situated medially, and the femoral nerve can be found between these two nerves. Although the lateral femoral cutaneous and femoral nerves lie within the same fascial plane, the obturator nerve is often separated (50%–60% of the time) from the other two nerves and contained within its own muscular fold inside the psoas major.3 6 At the L4–L5 level, the anterior-to-posterior distance between the transverse processes and the lumbar plexus is consistently less than 2 cm, and rarely greater than 2.5 cm.5 8 10 11
Femoral nerve
The femoral nerve is formed by the dorsal divisions of the ventral rami of the L2–L4 spinal nerves. The femoral nerve is the largest terminal branch of the lumbar plexus and typically emerges from the posterolateral or posterior surface of the psoas major and courses caudally in a muscular groove between the psoas major and underlying iliacus muscle. Within the pelvis, the femoral nerve supplies muscular branches to the iliacus and pectineus muscles, as well as an articular branch to the hip joint.12 13
The femoral nerve subsequently enters the base of the femoral triangle in the proximal thigh by passing deep (dorsal) to the inguinal ligament. The boundaries of femoral triangle are formed by the following structures (figures 2 and 3):
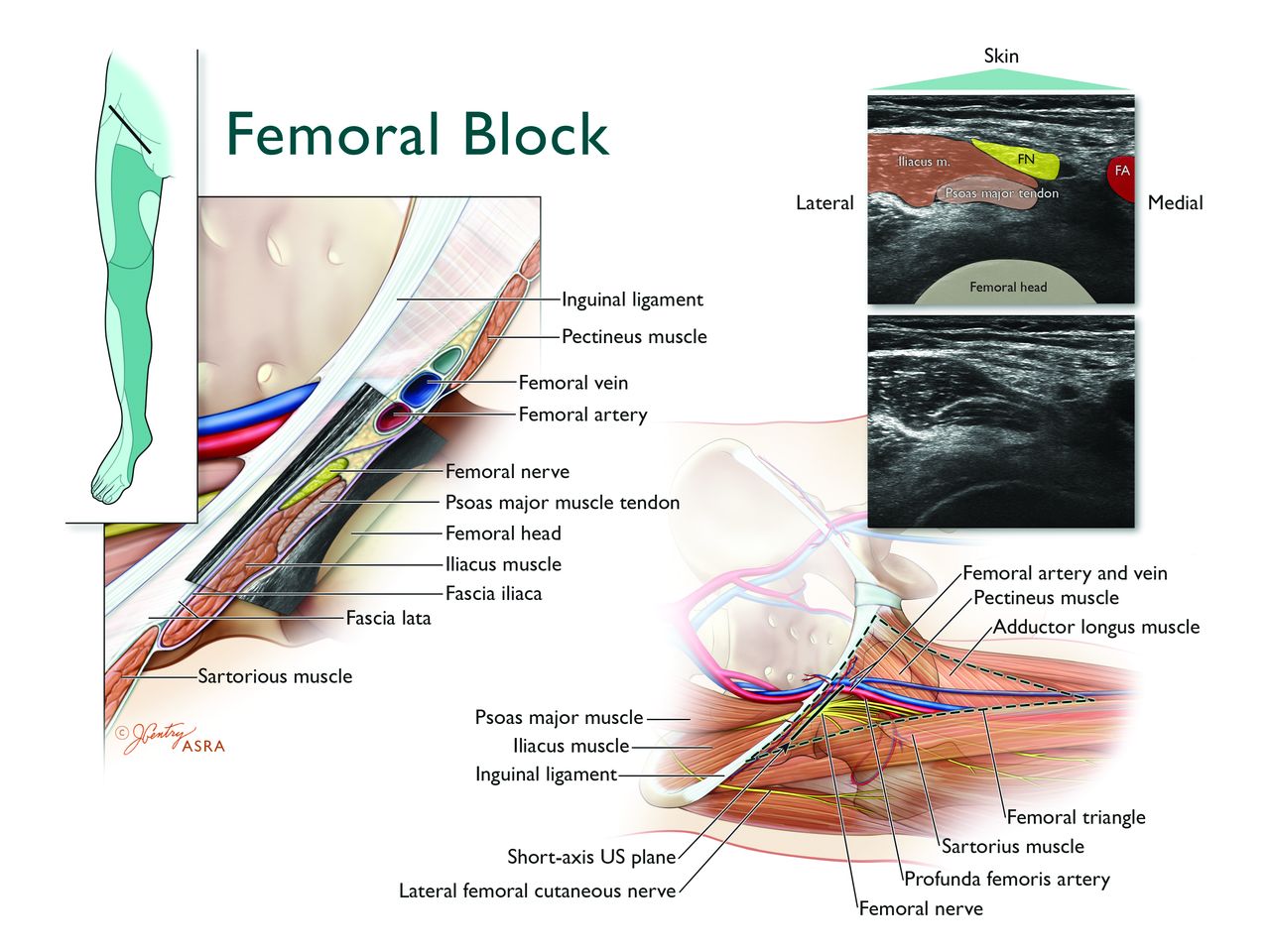
Anatomy of the ultrasound-guided femoral nerve block (FNB). Top left inset depicts the transducer location and expected cutaneous sensory distribution after FNB. The femoral nerve (FN) enters the base of the femoral triangle in the proximal anterior thigh by passing dorsal to the inguinal ligament. The femoral nerve is located within the iliopectineal fossa just lateral or posterolateral to femoral artery (FA) and lies ventral to the iliacus muscle. The magnified axial view illustrates that within the iliopectineal fossa, the FN is located dorsal to the fascia iliaca, while the femoral vessels (located within the femoral sheath) are found ventral to the fascia iliaca. The corresponding short-axis ultrasound image of the FNB is obtained by placing the transducer in an axial oblique position distal to the inguinal ligament. The FN appears as a hyperechoic oval-shaped structure lying directly on the relatively hypoechoic iliacus muscle and just dorsal to the thin hyperechoic linear fascia iliaca. Illustration by Jennifer Gentry. Copyright Jennifer Gentry, American Society of Regional Anesthesia and Pain Medicine.
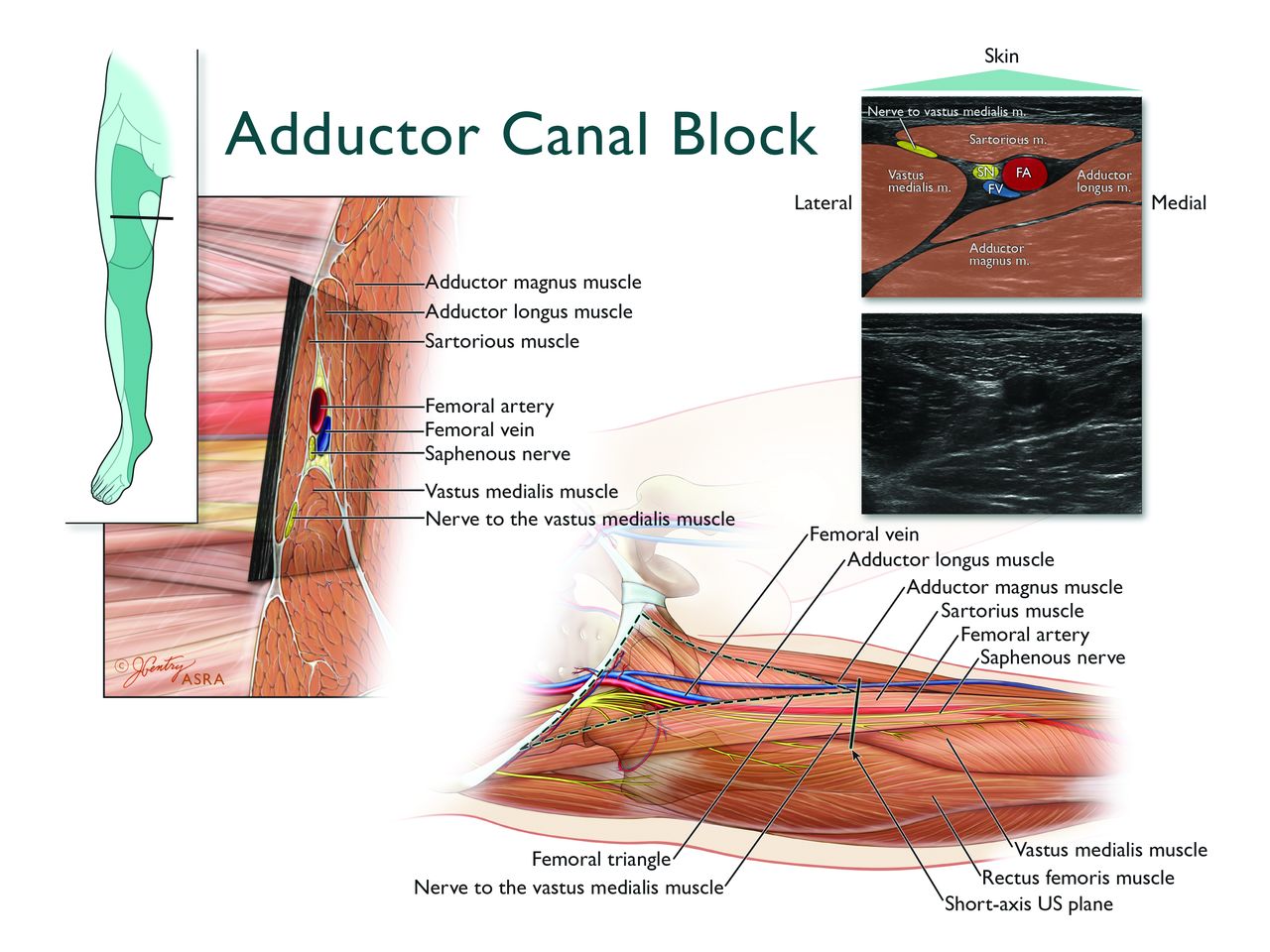
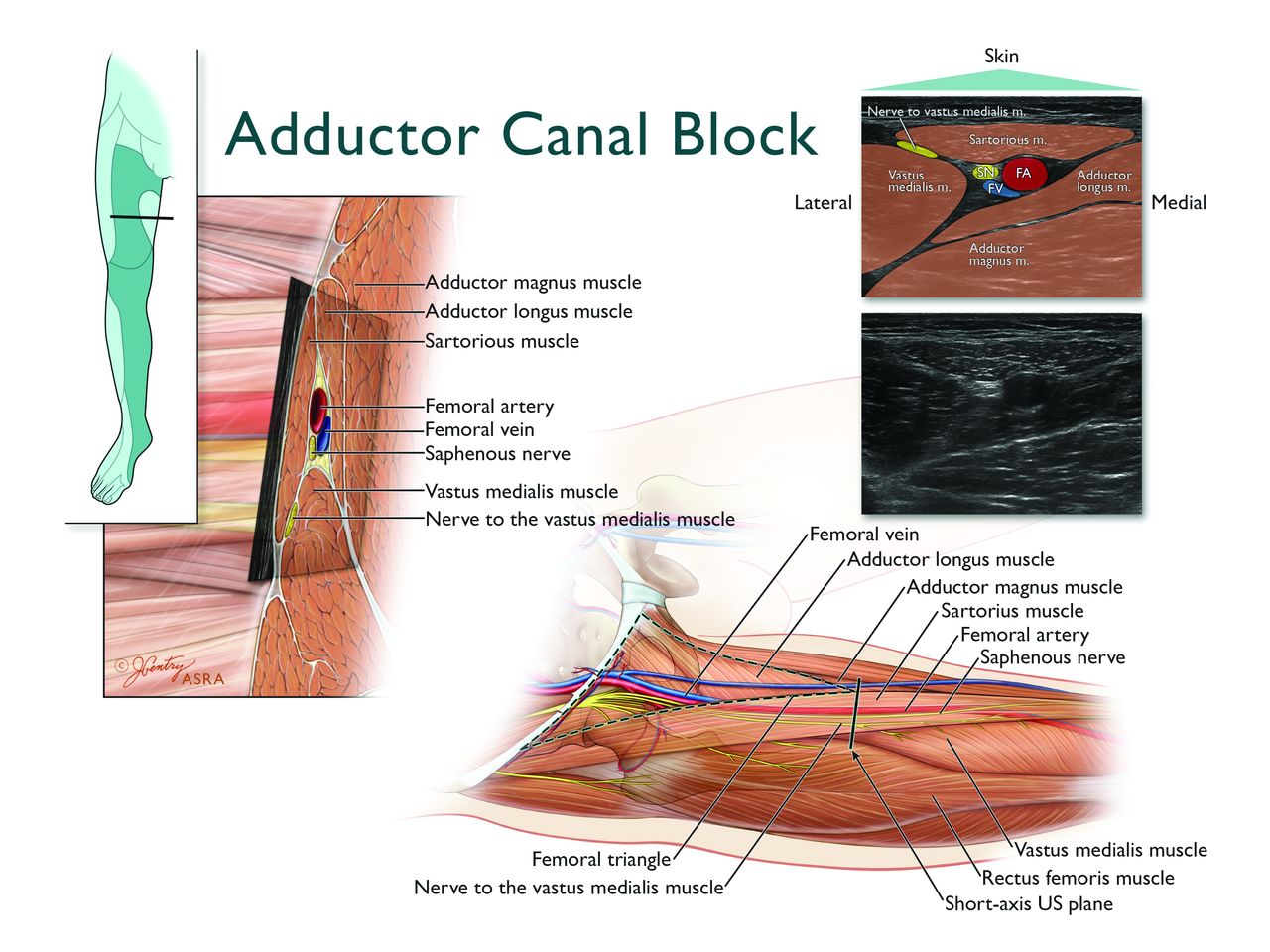
Anatomy of the ultrasound-guided adductor canal block (ACB). Top left inset depicts the transducer location and expected cutaneous sensory distribution after ACB. The magnified axial view just distal to the apex of the femoral triangle illustrates that the adductor canal (AC) is a triangular myofascial structure defined by the sartorius muscle–vasoadductor membrane anteromedially, the vastus medialis muscle anterolaterally, and adductor muscles (adductor longus and magnus) posteromedially. The corresponding short-axis ultrasound image of the AC is obtained by placing the transducer just distal to the apex of the femoral triangle. The apex of the femoral triangle (where the medial border of the sartorius muscle crosses over the medial border of the adductor longus) seamlessly transitions into the proximal aspect of the AC, without a true anatomical boundary. The hyperechoic saphenous nerve (SN) is located lateral to the anechoic femoral artery (FA). The compressible femoral vein (FV) is often located just deep and lateral to the FA. The nerve to the vastus medialis is not located within the AC and travels in a separate myofascial tunnel contiguous but anterior to the AC. Illustration by Jennifer Gentry. Copyright Jennifer Gentry, American Society of Regional Anesthesia and Pain Medicine.
The inguinal ligament (superior border or base).
The medial margin of the sartorius muscle (lateral border).
The medial margin of the adductor longus muscle (medial border).
The apex of the femoral triangle is defined by the intersection of the medial border of the sartorius and the medial border of the adductor longus. In contrast, the intersection of the medial border of the sartorius muscle and the lateral border of the adductor longus muscle corresponds to the apex of the iliopectineal fossa, which constitutes a proximal subset of the femoral triangle.14 15 The lateral and medial floors of the iliopectineal fossa are formed by the iliacus/psoas major and pectineus/adductor longus muscles, respectively. The roof of the iliopectineal fossa is made up by the overlying fascia lata.
At the level of the inguinal ligament, the femoral nerve is located within the iliopectineal fossa and is typically 1 to 2 cm lateral to the femoral artery.16 17 As the femoral nerve courses further caudad to the level of the inguinal crease, it adopts a position just lateral or posterolateral to the femoral artery.16 17 Within the iliopectineal fossa, the femoral nerve can be found dorsal to both the fascia lata and fascia iliaca. In contrast, the femoral vessels (enveloped by the femoral sheath) are located dorsal to the fascia lata but ventral to the fascia iliaca. Thus, the fascia iliaca physically separates the femoral nerve from the femoral vessels.
The femoral nerve demonstrates a relatively flat cross-sectional diameter with a mean medial-to-lateral width of 9 to 11 mm and a mean anterior-to-posterior dimension of 1.3 to 2.3 mm.18 The femoral nerve is composed of multiple “fascicular branches”:
1. Cutaneous branches to the anterior and medial thigh, peripatellar region, medial aspect of the lower leg and foot (figure 4).

Cutaneous and osseous sensory distributions of the lower extremity. Terminal nerves of the lumbar and sacral plexus provide cutaneous sensory innervation to the lower extremity. The sensory distribution of these nerves is variable and overlapping (as depicted by the blended colors as the zones converge). Illustration by Jennifer Gentry. Copyright Jennifer Gentry, American Society of Regional Anesthesia and Pain Medicine.
2. Sensory and motor branches to the hip flexors, quadriceps and sartorius muscles (figure 5).

Muscular sensory distribution. Terminal nerves of the lumbar and sacral plexus provide sensory innervation to the respective muscle groups of the lower extremity. Illustration by Jennifer Gentry. Copyright Jennifer Gentry, American Society of Regional Anesthesia and Pain Medicine.
3. Articular branches to the hip, knee, and ankle joints, as well as contributions to the osseous innervation of the pelvis, femur, and tibia (figure 4).
Fascicular branches innervating the vastus medialis, vastus intermedius, and vastus lateralis are typically found in the central and dorsal portion of the femoral nerve. The fascicular branches innervating the rectus femoris (laterally located), pectineus (medially located), and the cutaneous nerves to the thigh can all be found on the peripheral aspects of the femoral nerve. The fascicular branch supplying the sartorius muscle is usually located on the ventral aspect of the femoral nerve, but can also be found in the lateral, medial, or central portion of the latter.18 19 Anatomical and histological studies demonstrate that the femoral nerve arborizes into separate fascicular branches on average 3 cm distal to the inguinal ligament and consistently proximal to the inguinal (femoral) crease. At the level of the inguinal crease, the fascicular branches become separate nerves with an epineural layer around each individual branch. The branches are tethered together by a common connective tissue sheath, with ample adipose and loose connective tissue between them. Thus, at the level of the inguinal crease, the femoral nerve has already divided into multiple individual branches, which travel in close approximation for some distance before physically separating and heading to their respective destinations.20 Furthermore, at the apex of the iliopectineal fossa, the muscular branches to the rectus femoris, vastus intermedius, and vastus lateralis pierce through and become ventral to the fascia iliaca; they course for several centimeters through loose connective tissue before reaching their respective muscle. In a cadaveric study, US-guided dye injections at the apex of iliopectineal fossa (where the femoral artery has just passed beneath the medial border of the sartorius) consistently stained the nerve to the vastus medialis and the saphenous nerve, but spared the other muscular branches of the quadriceps muscles.21
Within the base of the iliopectineal fossa, the saphenous nerve is located medial to the nerve to the vastus medialis muscle. Together, these two nerves continue distally toward the apex of the femoral triangle in conjunction with the femoral artery and femoral vein thereby forming a neurovascular bundle. In the distal part of the femoral triangle, the nerve to the vastus medialis lies between the sartorius and vastus medialis muscle (figure 3). The medial femoral cutaneous nerve travels along the posterior side of the sartorius muscle and communicates with the saphenous nerve and anterior branch of the obturator nerve thereby forming the subsartorial neural plexus ventral to the vasoadductor membrane.14 These three nerves lie dorsal to the sartorius muscle and lateral to the femoral artery within the subsartorial apex (Scarpa) of the femoral triangle. The saphenous nerve and nerve to the vastus medialis exit the apex of the femoral triangle, but only the saphenous nerve enters the adductor canal in conjunction with the femoral artery and vein. It should be noted that the apex of the femoral triangle seamlessly transitions into the proximal aspect of the adductor canal, without a true anatomical boundary.14 21–24
The adductor canal is defined as the intermuscular compartment that begins proximally at the apex of the femoral triangle and ends distally at the adductor hiatus. The femoral artery exits the adductor canal by passing through the adductor hiatus on its way to the popliteal fossa where it becomes the popliteal artery. Within the adductor canal, the neurovascular bundle is located between the adductor muscles (longus and magnus) posteromedially, the vastus medialis muscle anterolaterally, and the vasoadductor membrane anteromedially (figure 3).14 22–24 Inside the adductor canal, the saphenous nerve can be initially found lateral to the femoral artery. As it continues distally, the saphenous nerve assumes a position anterior and then medial to the femoral artery in the distal adductor canal. Although the anatomical data are conflicting,14 22–25 the nerve to the vastus medialis deviates from the saphenous nerve just proximal to the adductor canal and travels in a separate myofascial tunnel contiguous but ventral to the adductor canal itself.14 22–24 It gives rise to branches that supply the vastus medialis muscle as well as filaments that continue further distally to innervate the anterior and medial capsule of the knee joint and the medial retinaculum.14 24 25 The saphenous nerve and the muscular branches from the nerve to the vastus medialis also give rise to branches that form a deep plexus lying between the femoral artery and the femur. In turn, this deep plexus gives rise to anterior and medial genicular nerves that supply the deep anteromedial aspect of the knee joint.14 24–27
At the distal end of the adductor canal, the saphenous nerve pierces the vasoadductor membrane and emerges subcutaneously between the sartorius and gracilis muscles, where it is located dorsal to the distal aspect of the sartorius muscle.25–29 As it courses further distally toward the joint line of the knee, the saphenous nerve further divides into infrapatellar and sartorial branches.30 The infrapatellar branch provides cutaneous sensory innervation to the anterior aspect of the knee and gives rise to an articular branch that innervates the medial aspect of the knee joint (figure 4).14 25–27
The sartorial branch continues distally along the medial lower leg. Deep branches of the sartorial branch located 4–8 cm proximal to the medial malleolus provide significant innervation to the distal tibia and articular branches to the medial capsule of the ankle joint.31 32 The sartorial branch continues further distally (passing anteromedial to the medial malleolus) to provide cutaneous innervation to the anteromedial lower leg as well as the medial aspect of the proximal and mid-portions of the foot (figure 4). Occasionally, it can contribute sensory innervation to the forefoot or articular innervation to first metatarsophalangeal joint.33–35
Obturator nerve
The obturator nerve is formed within the substance of the psoas major from the anterior divisions of the ventral rami of the L2–L4 spinal nerves. Inside the psoas major, the obturator nerve is the most medially located branch of the lumbar plexus.2 6 8 It emerges from the posterior border of the psoas major and descends along the lateral wall of the pelvis toward the superior part of the obturator foramen. The obturator nerve then enters the adductor compartment of the proximal thigh by passing through the obturator foramen.36 37 After emerging from the latter, just caudad to the superior pubic ramus, the obturator nerve courses distally within an interfascial plane ventral to the obturator externus muscle and dorsal to the pectineus muscle. The obturator nerve and the accessory obturator nerve provide:
Variable cutaneous sensory innervation to the posteromedial distal thigh14 38 (figure 4).
Sensory and muscular branches to adductor muscles of the thigh (figure 5).
Articular branches to the hip joint and posterior capsule of the knee joint.24–27 39 as well as osseous innervation to the pelvis and femur (figure 4).
Anatomical studies have demonstrated a considerable degree of variability in the anatomy of the obturator nerve. It may divide into its respective anterior and posterior branches within the pelvis (23%) as it enters the obturator foramen, or within the obturator foramen itself (52%). It may also emerge from the obturator canal as a singular structure and divide in the proximal medial thigh (25%).36
The anterior division initially courses in the interfascial plane between the pectineus and adductor brevis muscles, but further caudad, travels between the adductor longus and the adductor brevis muscles. The posterior division courses between the adductor brevis and adductor magnus. At the inferior border of the adductor longus within the apex of the femoral triangle, the distal continuation of the anterior division typically communicates with the medial cutaneous and saphenous branches of the femoral nerve to form a subsartorial plexus that supplies the skin on the medial side of the thigh.14 Anatomical dissections have also described occasional communications between the anterior division of the obturator nerve and the articular branch of the saphenous nerve, which contribute to the perigenicular innervation of the medial aspect of the knee.26 27 39
The posterior branch of the obturator nerve descends between the adductor brevis and adductor magnus and enters the popliteal fossa (as the distal genicular branch) from the posterior surface of the adductor magnus muscle, the adductor hiatus, or through the distal 1 cm of the adductor canal. Within the popliteal fossa, the genicular branch anastomoses with branches of the tibial nerve to form the posterior popliteal plexus, which provides sensory innervation to the menisci, perimeniscal and posterior joint capsule, cruciate ligaments, as well as the infrapatellar fat pad.14 27 39
An accessory obturator nerve may be present in 10% to 30% of patients and originates from the ventral rami of the L3–L4 spinal nerves or directly from the obturator nerve itself.40 41 The accessory obturator nerve courses along the posterior aspect of the external iliac artery and descends caudally over the superior pubic ramus giving off branches to the pectineus muscle and the hip joint. The presence of an accessory obturator nerve may carry clinical implications since the obturator and accessory obturator nerves are not adjacent to each other. Consequently, complete obturator nerve block (especially to the hip joint) may require blockade of the accessory obturator nerve as well. Fortunately, US-guided injection of 15 mL of methylene blue in the interfascial plane between the pectineus and obturator externus muscles effectively spreads to the superior ramus of the pubic bone, the obturator foramen, as well as the intrapelvic accessory obturator nerve when present (21% of cases).37
Lateral femoral cutaneous nerve
The lateral femoral cutaneous nerve (LFCN) is a purely sensory nerve originating from the posterior divisions of the ventral rami of the L2–L3 spinal nerves. It emerges from the lateral border of the psoas major muscle and courses obliquely across the iliacus muscle (dorsal to the fascia iliaca) toward the anterior superior iliac spine (ASIS). The LFCN continues caudad dorsal to the inguinal ligament to enter the anterior and lateral compartments of the thigh, where it divides into multiple branches that supply a widely variable cutaneous distribution over the lateral, anterior, and medial thigh as far distal as the knee42 (figure 4). The LFCN’s course on entering the thigh, particularly in relation to the inguinal ligament and ASIS, also demonstrates considerable variability.43–46 It is typically located 1.5 to 2.0 cm medial to the ASIS, although it may travel as far as 7 cm medial or even lateral to the ASIS. The LFCN usually enters the thigh as a single branch passing deep (dorsal) to the inguinal ligament in 70%–90% of cases. Less commonly, it may pass superficial (ventral) or directly through the inguinal ligament, and sometimes even through a bony canaliculus of the ASIS. As the LFCN penetrates the thigh, it is most commonly located ventral to the sartorius muscle and dorsal to the fascia iliaca. It may also pass through the sartorius muscle, and rarely it may even travel ventral to the fascia lata.
Sacral plexus anatomy
The sacral plexus originates within the pelvis from the lumbosacral trunk, the first to third sacral ventral rami, and part of the fourth sacral ventral ramus. The sacral ventral rami enter the pelvis through the anterior sacral foramina and converge to form a flattened band.2 47 The sacral plexus is characterized by a triangular shape with its base along the sacral foramina and its vertex at the greater sciatic foramen. It lies ventral to the piriformis muscle and dorsal to the presacral fascia, which separates it from the intrapelvic viscera. The sacral plexus provides sensory and motor innervation to portions of the lower extremity including the hip, knee, and ankle joints. The most important branches for lower extremity surgery are the sciatic and posterior femoral cutaneous nerves as well as their respective terminal branches. In addition, the nerves to the quadratus femoris and inferior gemellus, the superior gluteal nerve, and a branch originating directly from the proximal sciatic nerve provide sensory innervation to posterior aspects of the hip joint.13 48
Sciatic nerve
The sciatic nerve constitutes the primary terminal branch of the sacral plexus. It is derived from the lumbosacral trunk and ventral rami of the S1–S3 spinal nerves. It is the largest (measuring 10–20 mm in width at its proximal origin) and longest peripheral nerve in the body, extending from the inferior aspect of the piriformis muscle in the gluteal region to the apex of the popliteal fossa in the distal posterior thigh. The sciatic nerve trunk is composed of two major components: the tibial nerve (TN) and common peroneal nerve (CPN). These independent nerves do not mix fibers but share a common trajectory until they physically diverge from each other, typically within the popliteal fossa.49 The lumbosacral trunk and the anterior divisions of the ventral rami give rise to the TN, whereas the posterior divisions give rise to the CPN. The TN is larger, located medial and slightly anterior in relation to the smaller CPN. A common extraneural connective sheath surrounds the TN and CPN to form the main sciatic nerve trunk. The fascicular components of the two nerves are separated by a septum (Compton-Cruveilhier septum) composed of connective and adipose tissue within the main sciatic nerve trunk.50 51
The sciatic nerve exits the pelvis via the greater sciatic foramen, descending caudally in the gluteal region on the ventral surface of the piriformis muscle. The sciatic nerve emerges from the caudal aspect of the piriformis and continues in a caudad direction along the dorsal surface of the external hip rotator muscles (superior gemellus, tendon of the obturator internus, inferior gemellus, and quadratus femoris from a cranial-to-caudal orientation).2 At the caudal end of the quadratus femoris, the sciatic nerve enters the proximal posterior compartment of the thigh as it passes between the lateral border of the ischial tuberosity and the medial border of the posterior surface of the greater trochanter. Within the gluteal region, the gluteus maximus muscle covers the sciatic nerve, which can be found just lateral to both the posterior femoral cutaneous nerve and the inferior gluteal artery. Between the ischial tuberosity and the greater trochanter, the sciatic nerve is located in a well-defined intermuscular compartment (“subgluteal compartment”) dorsal to the quadratus femoris and ventral to the gluteus maximus.52–54 As it emerges from the subgluteal compartment, the sciatic nerve lies on the posterior surface of the adductor magnus muscle and is crossed obliquely by the tendon of the long head of the biceps femoris muscle.55 56 Thus, the sciatic nerve is initially located just lateral to the tendinous origin (ischial tuberosity) of the long head of the biceps femoris before progressing distally deep to the belly of the latter toward the apex of the popliteal fossa.55–58 Within the gluteal region and the proximal-to-midthigh, the most medial aspect of the sciatic nerve provides muscular branches to the semitendinosus, semimembranosus, long head and short head of the biceps femoris, as well as the ischial part of the adductor magnus (figure 5). Further caudad, the sciatic nerve provides articular branches to the knee joint.14 49 59
Within the mid-thigh (approximately halfway between the lateral aspect of the greater trochanter and the popliteal crease), the sciatic nerve is located posterior and medial to the shaft of the femur in a myofascial plane: it can be found dorsal to the adductor magnus and ventral to the belly of the long head of the biceps femoris.57 58 60
The distal sciatic nerve is located in the popliteal fossa. The latter is defined as the diamond-shaped intermuscular space posterior to the knee joint, bordered supero-laterally by the tendon of the long head of the biceps femoris, supero-medially by the tendons of the semimembranosus and overlying semitendinosus, infero-medially by the medial head of the gastrocnemius, and infero-laterally by the lateral head of the gastrocnemius.2 Within the apex of the popliteal fossa, the sciatic nerve is bordered laterally by the long head of the biceps femoris muscle tendon and medially by the semimembranosus–semitendinosus tendons. In the upper part of the popliteal fossa, the sciatic nerve lies posterolateral to the popliteal vessels. The divergence of the sciatic nerve into the anatomically separate TN and CPN usually occurs in the cephalad aspect of the popliteal fossa, but it may also occur at any point between the sacral plexus and the popliteal skin crease.61 62
Tibial nerve
The TN is the larger of the two terminal branches of the sciatic nerve. It continues further caudad within the center-midline of the popliteal fossa toward the popliteal skin crease and lies posterior and lateral to the popliteal vessels. Within the lower aspect of the popliteal fossa, it sends sensory and muscular branches to the major ankle flexors (the gastrocnemius and soleus muscles) (figure 5) as well as articular branches to the knee and ankle joint.59 63 The TN then courses distally with the popliteal vessels deep to the tendinous arch of the soleus and runs along the dorsal surface of the tibialis posterior muscle. At the distal third of the lower leg, the TN emerges from beneath the soleus and courses along the medial aspect of the ankle midway between the dorsal aspect of the medial malleolus and the dorsal portion of the Achilles tendon. Proximal to the medial malleolus, the TN gives off its calcaneal branch, which supplies the heel of the foot.2 52 At the level of the medial malleolus, the TN is only covered by superficial and deep fascia, and is typically found immediately dorsal to the posterior tibial artery. As the TN crosses over to the plantar aspect of the foot, it gives off the medial and lateral plantar nerves, which provide sensory and motor innervation to the foot and ankle. The medial plantar nerve supplies digital nerves to the medial 3 1/2 toes, whereas the lateral plantar nerve sends digital nerves to the lateral 1 1/2 toes.59 63
Common peroneal nerve
The CPN is the lateral terminal branch of the sciatic nerve and travels obliquely along the lateral border of the popliteal fossa just medial to the tendon of the long head of the biceps femoris muscle. Within the popliteal fossa, the CPN provides an articular branch to the lateral aspect of the knee joint. It exits the popliteal fossa by crossing over the lateral head of the gastrocnemius and can be found subcutaneously between the fibular head and the peroneus longus muscle. As it circumvents the neck of the fibula, the CPN divides into its two terminal branches: the superficial and deep peroneal nerve. The superficial peroneal nerve descends in the lateral compartment between the peroneus longus and extensor digitorum muscles to supply the ankle eversion muscles. In the lower third of the leg, it pierces the deep fascia and divides into several branches that provide cutaneous sensory innervation to the dorsal aspect of the ankle and foot. The deep peroneal nerve passes posterior to the extensor digitorum longus and anterior to the interosseous membrane, where it is joined by the anterior tibial artery. It then descends within the distal anterior compartment of the leg and emerges on the dorsum of the foot. The deep peroneal nerve and the contiguous dorsalis pedis artery are located lateral to the extensor hallucis longus tendon. At the level of the malleoli, the deep peroneal nerve can be found lateral to the artery.2 64 Along its course, the deep peroneal nerve supplies the anterior muscle group of the lower leg and provides an articular branch to the ankle joint as well as a cutaneous branch to the first interdigital space.
Sural nerve
The medial (MSCN) and lateral (LSCN) sural cutaneous nerves are purely sensory nerves derived from the TN and CPN, respectively, at the knee joint. In the majority (81%) of cases, the MSCN descends between the two heads of the gastrocnemius muscles where it receives the peroneal communicating branch (LSCN) to form the common sural nerve. Occasionally, the common sural nerve is derived solely from the TN (18% of cases) or the CPN (1% of cases).65 The common sural nerve then continues caudad and courses between the dorsal aspect of the Achilles tendon and the dorsal aspect of the lateral malleolus in close proximity and lateral to the small saphenous vein, before terminating on the lateral side of the foot. The sural nerve provides cutaneous innervation to the posterolateral aspects of the lower leg and ankle as well as the dorsolateral aspect of the foot (figure 4).
Posterior femoral cutaneous nerve
The posterior femoral cutaneous nerve is a purely sensory nerve derived from the ventral rami of the S1–S3 spinal nerves. It exits the pelvis through the greater sciatic foramen, initially medial and then dorsal to the sciatic nerve, while traveling ventral to the gluteus maximus alongside the inferior gluteal vessels. In the gluteal region, the posterior femoral cutaneous nerve is consistently located within the deep investing fascia of the gluteus maximus, while the sciatic nerve is located superficial to this fascial layer.64 While ventral to the gluteus maximus, it gives cutaneous branches to the ipsilateral lower buttock and perineum.2 Caudal to the ischium, the posterior femoral cutaneous nerve can be found lateral and superficial to the long head of the biceps femoris. At this level, it is located in subcutaneous tissues immediately ventral to the inferior margin of the gluteus maximus and fascia lata. In the proximal thigh, a deeper investing fascial layer connects the biceps femoris and vastus lateralis muscles. The sciatic nerve is located under this deeper investing fascial layer, while the posterior femoral cutaneous nerve is located superficial to the latter. Thus, the posterior femoral cutaneous nerve is located in a superficial fascial compartment that is separate from the sciatic nerve. The posterior femoral cutaneous nerve then continues down the posterior aspect of the thigh and leg, giving off, in succession, femoral and sural branches, which provide cutaneous innervation to the back of the thigh, popliteal fossa, and calf2 65 67 (figure 4).
Peripheral nerves: clinical and functional anatomy
A peripheral nerve consists of neural and non-neural components that together create a functional unit. The neural component is formed by axons, which are cytoplasmic neuronal extensions that conduct electrical signals originating from the cell bodies located inside the dorsal root ganglion (for general somatosensory function) or ventral horn of the spinal cord (for general somatic motor function).68 From the inside outward, non-neural protective layers consist of endoneurium, perineurium, and epineurium (figure 6). Individual axons are surrounded by supporting connective tissue called the endoneurium, which consists of fibroblasts and their products (ie, collagen fibers and extracellular matrix). Groups of axons are bundled together into fascicles by the perineurium, which is composed of squamous cells that share tight junctions and are arranged in multiple concentric layers, interspersed by basal lamina. Each fascicle contains multiple axons and capillary blood vessels embedded within the loose connective tissue matrix of the adjacent endoneurium. The perineurium creates both a physical and chemical barrier, and functionally, serves as the “blood–nerve barrier.” The epineurium is the outermost connective tissue layer and encompasses two distinct anatomical components.69 70 The inner (interfascicular) epineurium is composed of fibroadipose connective tissue that surrounds and fills the spaces between neural fascicles. The outer (epifascicular) epineurium encases the peripheral nerve and connects it to the adjacent extraneural tissues.

Peripheral nerve anatomy. Peripheral nerves consist of neural and non-neural connective tissue that together create a functional unit. Peripheral nerves are a collection of individual axons surrounded by supporting connective tissue called the endoneurium. Axons receive nutrition from intrinsic vessels. Extrinsic vessels are under adrenergic control and supply the intrinsic system. Groups of axons are bundled together into fascicles by the perineurium. The epineurium is the outermost connective tissue layer and encompasses both the interfascicular (which surrounds and fills the spaces between fascicles) and epifascicular (which encases the peripheral nerve and connects it to the adjacent extraneural connective tissue) layers. The extraneural connective tissue (paraneurium or paraneural sheath) suspends the peripheral nerve within loose connective tissue that is directly connected to the epineurium. Illustration by Jennifer Gentry. Copyright Jennifer Gentry, American Society of Regional Anesthesia and Pain Medicine.
The extraneural connective (also known as paraneurium or paraneural sheath) suspends large peripheral nerves within a loose connective space that is directly connected to the epifascicular epineurium. In contrast, smaller nerves are surrounded by loose connective tissue originating from intramuscular compartments. The subparaneural space found around larger neural structures provides a path for longitudinal nerve motion, especially around joints thereby functioning as a “gliding layer” for the nerve and offering a layer of protection against neural trauma. In addition, the subparaneural compartment provides a plane of cleavage where the epifascicular epineurium and paraneurium come into contact.71 72 This cleavage plane constitutes a virtual space that runs circumferentially and longitudinally along the course of a peripheral nerve, thus providing a conduit for local anesthetic spread.70–73
Peripheral nerves contain varying proportions of non-neural connective tissue. In general, the number of fascicles or fascicular bundles increases from proximal to distal, whereas the size of the fascicles decreases.49 74 The relative and absolute amount of non-neural tissue also increases from proximal to distal. Thus, fascicles may constitute 25% to 75% of the cross-sectional surface area of a peripheral nerve with the relative amount of neural tissue decreasing from proximal to distal.59 74 Along the path of a peripheral nerve, multiple intricate interconnections exist among fascicles. The latter may divide, regroup, interconnect, and reorganize to form intraneural plexuses.68 75 The vascular supply of a peripheral nerve occurs mainly via longitudinally arranged blood vessels within the endoneurium and epineurium. The endoneural and epineural vessels have interconnecting bridges, and the epineural blood vessels can be directly modulated by the adrenergic system. The endothelial tight junctions of the endoneural capillaries serve as an additional blood–nerve barrier within peripheral nerves.68
Essentials of the evidence pertaining to approaches and techniques
In recent years, the compendium of approaches and techniques for lower limb blocks has increased with the advent of US. In light of the large number of studies published in the English language, an evidenced-based discussion of lower extremity nerve blocks should focus on the best evidence available, ie, randomized controlled trials, published as of April 2018 (see online supplementary appendix 1/Supplemental Digital Content 1) for literature search strategy). Because randomized trials are primarily discussed, all technical recommendations contained in this review article are derived from Oxford Centre for Evidence-Based Medicine level 2 evidence (online supplementary appendix 2/Supplemental Digital Content 2).
Supplemental material
Supplemental material
For the purposes of this review, the term “approach” refers to the anatomical site where a plexus or peripheral nerve is targeted. The term “technique” refers to the modality (loss-of-resistance, paresthesia, neurostimulation, US) or endpoints (type of evoked motor response with neurostimulation, single or multiple injections) needed to identify and anesthetize the nerve for a given approach. While some neural structures (eg, lumbar plexus, saphenous and sciatic nerves) can be blocked with different approaches as well as techniques, the majority of lower limb nerves are targeted using a single approach but multiple techniques.
Nerve blocks of the lumbar plexus
Approaches for lumbar plexus block
Lumbar plexus blocks are usually performed in the setting of hip arthroplasty10 and hip fracture repair76–78 The lumbar plexus can be anesthetized with a posterior approach by depositing local anesthetic (LA) agents within the substance of the psoas muscle10 79–81 Alternatively, Winnie et al 82 suggested that an inguinal injection lateral to the femoral artery, coupled with cephalad angulation of the needle and distal manual compression, would result in cephalad LA diffusion toward the lumbar plexus. Because the three main branches of the lumbar plexus (femoral, lateral femoral cutaneous, and obturator nerves) would be theoretically anesthetized with a single injection, this “anterior” approach to the lumbar plexus has also been called the “3-in-1 block.”
To date, six randomized controlled trials (RCTs) have compared single-injection 3-in-1 blocks and posterior lumbar plexus blocks.81 83–87 Three RCTs reported a higher success rate with the posterior approach (83%–97% vs 16%–53%; p<0.05).83 85 86 Although both methods reliably anesthetized the femoral nerve, obturator motor block was more commonly achieved with the posterior approach (63%–100% vs 0%–30%; p<0.05).81 83 86 Two RCTs (combined n=119) have compared continuous 3-in-1 and lumbar plexus blocks for patients undergoing total knee replacement (TKR).88 89 While one trial observed no differences in onset and sensory block of the obturator nerve,88 the other study noted improved sensory obturator blockade at 24 hours with the posterior approach.89
The unreliable obturator block seen with the 3-in-1 block stems from the fact that, contrary to Winnie’s hypothesis,82 LA anesthetizes the lateral femoral cutaneous and obturator nerves through lateral/medial spread, dorsal to the fascia iliaca and not via proximal diffusion.90 Therefore, with the anterior approach, LA may distribute preferentially in a lateral direction, thus sparing the obturator nerve.85 Some authors have even advocated renaming the anterior approach “2-in-1 block.” 91
In summary, based on an analysis of the clinical evidence available, the posterior approach constitutes the only reliable method to anesthetize the lumbar plexus. The terms “anterior approach” and “3-in-1 block” should no longer be used.
Techniques for (posterior) lumbar plexus block
While early descriptions of lumbar plexus blocks have advocated a loss-of-resistance (LOR) technique,76 80 all subsequent studies have employed peripheral nerve stimulation (PNS).81 92 93 In 2011, one trial comparing both modalities reported similar success rates but a shorter onset time with PNS.94
Four different sets of surface landmarks have been advocated for PNS-guided lumbar plexus blocks.10 79–81 An RCT comparing Winnie’s and Chayen’s landmarks in children reported that, despite similar success rates (88%–92%), Chayen’s landmarks also resulted in a block of the contralateral lower limb in 88% of cases.92 In contrast, in adults, all described landmarks for lumbar plexus block seem to provide similar success rates as well as comparable risks of neuraxial spread (4%–40%).81 93
In a 2008 trial, the relationship between injection pressure and epidural spread has been assessed.95 Compared with a lower injection pressure (<15 psi), an injection pressure>20 psi should be avoided since it significantly increased the incidence of epidural blockade (0% vs 50%; p=0.03).
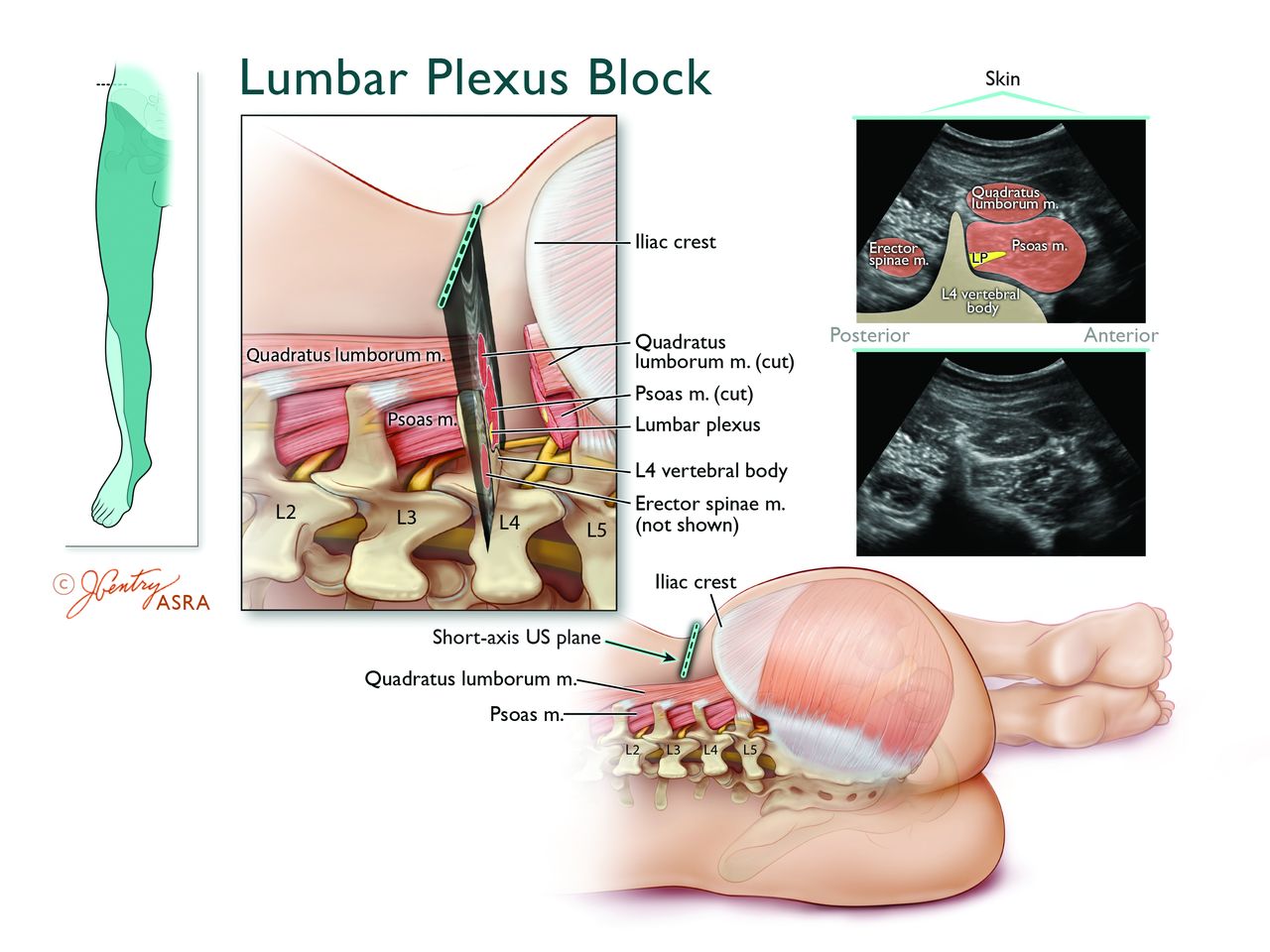
In recent years, US has been increasingly used as an adjunct for lumbar plexus block.96 Because of its depth, the psoas muscle (and lumbar plexus) can be insonated with different US transducer orientations: parasagittal (ie, the “Trident” sign),96 paramedian transverse through the lumbar intertransverse space,97 and axial along the posterior axillary line (ie, the “Shamrock” sign)98 (figure 7). In a small randomized, crossover trial (n=20), Strid et al 99 compared the “Trident” and “Shamrock” methods. These authors found that the latter resulted in a shorter performance time (238±74 vs 334±156 s; p<0.001), fewer needle insertions, and less procedural pain. However, sensorimotor block was similar between the two groups. A recent RCT (n=110) compared combined US–PNS and US alone for lumbar plexus blocks. In the combined group, quadriceps-evoked motor response was sought at a current between 0.2 and 0.8 mA (pulse width=0.1 ms) prior to LA injection. In the US alone group, LA was simply deposited inside the posteromedial quadrant of the psoas muscle. The authors found no intergroup differences in terms of performance time, block success, and postoperative opioid consumption. However, the combined US–PNS resulted in a 34% decrease in onset time compared to US alone.100

Anatomy of the ultrasound-guided Shamrock lumbar plexus block (LPB). Top left inset depicts the transducer location and expected cutaneous sensory distribution after LPB. The magnified axial view illustrates that the lumbar plexus is located within posteromedial aspect of the psoas major muscle (PMM) just anterior to the transverse process (TP). The corresponding short-axis ultrasound view of the lumbar vertebral body, TP, PMM, erector spinae muscles (ESM), and quadratus lumborum muscle (QLM) and lumbar plexus is obtained by placing the transducer in an axial orientation just cranial to the iliac crest approximately along the posterior axillary line. The ultrasound image displays the characteristic view of the TP forming the stem of a Shamrock (three-leaf clover), with the PMM, QLM, and ESM representing the three leaves. The hyperechoic lumbar plexus is contained within the relatively hypoechoic PMM, typically within 2 cm anterior to the intensely hyperechoic TP. Since the segmental lumbar vertebral arteries lie lateral to the vertebral body and medial to the lumbar plexus, the needle tip should be positioned on the lateral side of the lumbar plexus. Illustration by Jennifer Gentry. Copyright Jennifer Gentry, American Society of Regional Anesthesia and Pain Medicine.
In summary, compared to LOR, PNS provides a shorter onset time for lumbar plexus blocks. In adult patients, all described landmarks for the PNS technique result in similar efficacy and adverse events (ie, epidural LA spread). For US-guided lumbar plexus block, compared to a parasagittal probe orientation, the “Shamrock” method results in a shorter performance time and fewer needle redirections. Compared to US alone, combined US–PNS provides a quicker onset for lumbar plexus blocks. However, the decreased onset time may provide minimal benefits if the block is performed mainly for postoperative analgesia and patients undergo concomitant general or neuraxial anesthesia.
Techniques for femoral nerve block
Femoral nerve blocks are commonly used to provide pain control for TKR, anterior cruciate ligament (ACL) reconstruction, total hip arthroplasty as well as femoral fractures.87 101 102
Two RCTs have been carried out to determine the best technique for PNS-guided femoral nerve block.103 104 Compared to a single-injection technique, a three-injection method (with targeted stimulation of the motor branches to the vastus medialis, intermedius, and lateralis muscles) resulted in a decreased total anesthesia-related preoperative time (due to a quicker onset of surgical anesthesia)103 as well as a lower minimum effective anesthetic volume of ropivacaine 0.5% for successful femoral blockade in 50% of subjects (MEV50) (14 vs 23 mL; p=0.001).104
During PNS-guided localization of the femoral nerve, two evoked motor responses (EMRs) are commonly encountered: sartorius muscle contraction (stimulation of the fascicular branch of the sartorius muscle) and quadriceps contraction, ie, “patellar ascension” sign (stimulation of the fascicular branches of the quadriceps muscle). Traditionally, only a quadriceps EMR was deemed acceptable. However, in 64 patients randomized to either sartorius or quadriceps EMR, no differences were noted between the proportions of subjects with complete and partial sensory block or complete motor block of the femoral nerve at 30 min.105 These findings may be explained by the fact that the fascicular branches to the sartorius and quadriceps muscles lie in close proximity to each other dorsal to the fascia iliaca.105
To date, two clinical trials have compared US and PNS for femoral nerve block.106 107 In a dose-finding study, the MEV50 of ropivacaine 0.5% was lower with US compared to PNS (15 vs 26 mL; p=0.002).106 Another RCT, comparing US to combined US-PNS, found similar efficacy; however, the combination of modalities increased both performance time and number of needle passes.108
In three RCTs comparing PNS and US for “3-in-1 blocks,” US was found to provide significant benefits such as a quicker onset and/or a denser combined sensory block of the femoral, lateral femoral cutaneous and obturator nerves.87 109 110
In summary, compared to a single-EMR PNS technique, multiple EMRs shorten the onset time and decrease the LA requirement for femoral nerve block. Based on the limited evidence available, quadriceps and sartorius contraction constitute acceptable EMRs for single-injection femoral nerve block. Ultrasound guidance provides a LA-sparing effect for femoral nerve block. However, if the femoral nerve can be well visualized, the combination of PNS and US confers no additional benefits when compared with US alone. The limited evidence available suggests that US provides a more reliable adjunct for “3-in-1 blocks” than PNS.
Techniques for fascia Iliaca block
In 1989, Dalens et al 111 introduced the fascia iliaca compartment block, an LOR method whereby LA is injected immediately dorsal to the fascia iliaca while firm compression is applied distal to the puncture site. In 120 children randomized to a PNS-guided “3-in-1” or a fascia iliaca compartment block, Dalens et al 111 reported similar rates of complete sensory block for the femoral nerve (100%); however, the fascia iliaca block resulted in improved sensory blockade of the LFCN (92% vs 15%; p<0.05). Subsequently, the same comparison was carried out in 100 adults.112 Again, despite a similar rate of femoral block (88%–90%), the LFCN was more frequently anesthetized in the fascia iliaca group (90% vs 62%; p<0.05). However, motor blockade of the obturator nerve showed no intergroup difference (20%–32%). Thus, compared to its “3-in-1” counterpart, the fascia iliaca block results in more frequent anesthesia of the LFCN. However, obturator block remains elusive in adults.
In 2008, a trial randomized 80 patients to a fascia iliaca block using LOR or US.113 Although similar sensory blocks were observed in the anterior and lateral thighs, US yielded a better sensory block of the medial thigh as well as improved motor block of the obturator and femoral nerves. The authors speculated that subcutaneous fascias might in fact consist of several layers separated by adipose tissue: thus, blind puncture of any of these layers (with subsequent incorrect placement of LA) could have been mistaken for that of the fascia iliaca.
Techniques for LFCN block
Block of the LFCN is commonly performed to anesthetize the skin of the lateral thigh. It can aid in the diagnosis and management of meralgia paresthetica.114
In a randomized crossover study, LFCN block was carried out using fan infiltration or a PNS-guided technique (seeking a paresthesia of the lateral thigh).115 Nerve stimulation achieved a higher success rate, a quicker onset time as well as a decreased rate of incidental femoral nerve block (5% vs 35%; p=0.02). The LFCN can also be anesthetized with US guidance.116 A recent RCT comparing (sensory) neurostimulation and US reported no intergroup differences in terms of success rate, performance time, and onset. However, US guidance conferred a threefold decrease in the number of needle passes (p=0.009).117 Currently, there exist two techniques for US-guided LFCN block. One trial comparing US-guided targeted LFCN block and US-guided infiltration dorsal to the inguinal ligament found that the latter method resulted in a higher success rate (96% vs 75%; p=0.0027).118
Techniques for obturator nerve block
The obturator nerve provides sensory innervation to the medial aspect of the femur as well as articular innervation to the hip and knee. Obturator and femoral nerve blocks can be performed conjointly to provide analgesia for TKR.119
Neurostimulation-guided obturator block can be carried out proximally just caudad to the superior pubic ramus or more distally at the level of the inguinal crease. An RCT comparing these two methods found that, despite a similar efficacy, the distal approach resulted in a shorter performance time (80 vs 120 s; p<0.05), decreased procedural discomfort, and fewer complications such as vascular puncture and groin pain.120
Several reports have advocated US for obturator nerve block.121 122 However, to date, only one RCT (n=50) has compared US and combined US–PNS.123 In the US group, the authors injected LA between the adductor longus and brevis and the adductor brevis and magnus muscles. In contrast, in the US–NS group, EMRs of the adductor magnus (posterior division of the obturator nerve) and the adductor longus or brevis (anterior division of the obturator nerve) were sought. The combination of modalities provided no additional benefits in terms of efficacy (motor block at 15 min) or efficiency (onset/total anesthesia-related times, number of needle passes). Although preliminary studies suggest that obturator block can also be achieved by depositing LA between the pectineus and obturator externus muscles,37 124 further trials are required to validate this technique.
Approaches and techniques for saphenous nerve block
Saphenous nerve blocks are commonly performed to cover the medial leg in the setting of ankle and foot surgery.125 Several approaches have been described to anesthetize the saphenous nerve: perifemoral injection, transsartorial injection, infiltration around the medial femoral condyle, infiltration around the medial tibial tuberosity, paravenous injection distal to the knee joint, and infiltration around the medial malleolus. Techniques include blind LA infiltration, LOR, (sensory) PNS, and US.
In the literature, seven RCTs have compared approaches and techniques for saphenous nerve block.125–131 In terms of approaches, a small volunteer study (n=20) compared blind LA injections around the saphenous vein and distal to the knee (between the tibial tuberosity and the medial head of the gastrocnemius).125 The paravenous approach yielded a higher success rate (100% vs 33.3%; p<0.05). In 2009, Benzon et al 128 compared a PNS-guided perifemoral approach (4 cm distal to the inguinal crease) with a PNS-guided transsartorial approach (3–4 cm superior and 6–8 cm posterior to the supero-medial border of the patella) and three landmark-based field blocks: paracondylar, distal to the knee, and around the medial malleolus. These authors observed the following rates of sensory blockade: 100% for the transsartorial approach, 70% for the perifemoral approach, 10% for paracondylar injection, and 70% for infiltration distal to the knee. Unfortunately, the small number of subjects (n=10) precluded definitive conclusions. However, two subsequent trials did report improved success rate with the transsartorial approach (with LOR or US) compared to blind LA infiltration distal to the knee (80%–100% vs 30%–40%; p<0.05).126 129 In recent years, the US transsartorial approach has also been compared to US-guided LA injection between the sartorius and vastus medialis muscles proximal to the knee joint with mixed results: one trial found no intergroup differences in terms of success rate129 while the other RCT reported a higher success rate (100% vs 86%; p=0.003) and shorter onset time (3 vs 9 min; p<0.001) with the transsartorial approach.130
In an effort to refine the transsartorial technique, LOR, and (sensory) PNS were compared in a group of 25 volunteers.127 Despite an improved success rate (100% vs 72%; p<0.05), the PNS technique was associated with more procedural pain score and a longer performance time. In a recent RCT (n=80), saphenous block 3 to 5 cm proximal to the patella was performed using US or combined US–(sensory) PNS. Adjunctive PNS did not improve block success but only served to lengthen the performance time (314±125 vs 207±76 s; p<0.001).131
In summary, based on the limited evidence available, the transsartorial approach constitutes the optimal approach for saphenous nerve block. Peripheral neurostimulation seems to confer minimal benefits when compared with US.
Techniques for femoral triangle / adductor canal block
In recent years, LA injection next to the neurovascular bundle (around the femoral artery) at the level of the mid-thigh has received considerable interest. In addition to the saphenous nerve, LA injection in this location can also anesthetize the fascicular motor branch (of the femoral nerve) to the vastus medialis.14 While most authors have initially termed this block “adductor canal block,” recent anatomical studies seem to suggest that “femoral triangle block” (FTB) might constitute a more accurate description. Irrespective of the correct denomination, recent RCTs have shown that FTB can decrease pain and/or opioid requirements and preserve quadriceps motor strength (compared to femoral blocks) after TKR.132–134
To date, two RCTs (combined n=122) have investigated the optimal insertion site for FTB perineural catheters in the setting of TKR.135 136 Both trials concluded that proximal insertion sites (ie, where the medial border of the sartorius muscle first covers the femoral artery or where the femoral artery travels dorsal to the medial third of the sartorius muscle) and distal insertion sites (ie, approximately halfway between the anterosuperior iliac spine and the patella or where the femoral artery travels dorsal to the midpoint of the sartorius muscle) resulted in comparable postoperative opioid consumption, quadriceps strength, distance ambulated, and hospital length of stay.135 136
Continuous block of nerves originating from the lumbar plexus
In their simplest permutation, perineural catheters are positioned by advancing the catheter blindly (usually 3–5 cm) past the needle tip (ie, blind catheters). Alternatively, placement of perineural catheters can be accomplished with PNS and preservation of the EMR via the catheter tip as the latter is advanced beyond the needle (ie, stimulating catheters). Increasingly, US is being used to verify the position of perineural catheters (ie, US catheters).
Although one recent trial has reported a 50%-decrease in the MEV50 of mepivacaine 1.5% with stimulating compared with blind lumbar plexus catheters,137 all RCTs comparing the different techniques for catheter insertion have focused exclusively on the femoral nerve.
Techniques for blind femoral catheters
Prior to blind catheter advancement, the femoral nerve can be localized using PNS, US, or LOR (fascia iliaca compartment). Four RCTs have compared these modalities in patients undergoing ACL repair or TKR.138–141 In two trials, PNS and LOR resulted in similar postoperative pain scores and opioid requirements.138 139 However, LOR was associated with a faster performance time and a lower estimated material cost.138 A third RCT compared PNS and US140. Although US resulted in a quicker performance time and less procedural discomfort, postoperative analgesia as well as ropivacaine and opioid requirements were similar between the two groups. In a fourth trial, US was compared to combined US–NS. Again, no differences were found in terms of analgesia and opioid consumption.141 In summary, compared to PNS, LOR and US result in more expedient/less expensive needle placement prior to blind catheter advancement. However, postoperative analgesia is comparable with all three techniques since the catheters are advanced blindly.
Blind versus stimulating femoral catheters
Seven RCTs have compared blind and stimulating femoral catheters in the context of healthy volunteers, TKR, or ACL repair.100 141–146 In 20 volunteers, Salinas et al 142 placed bilateral femoral catheters while randomizing one side to a blind technique and the contralateral side to a stimulating technique. Despite similar success rates, these authors found that limbs anesthetized with stimulating catheters displayed a denser block as evidenced by higher tolerance to transcutaneous electrical stimulation and more pronounced quadriceps motor weakness, when quantitatively assessed with force dynamometry.
Unfortunately, Salinas et al’s results could not be reproduced outside of volunteers. Three RCTs (combined n=204) have compared stimulating and blind femoral catheters in the setting of TKR (n=183) and ACL repair (n=21).143–145 All three trials reported no differences in terms of static/dynamic pain scores, narcotic/LA consumption, physiotherapy performance, and discharge time. In 70 patients undergoing ACL repair, Dauri et al 101 compared blind and stimulating femoral catheters. These authors found that stimulating catheters resulted in a quicker onset of sensory block for the femoral nerve as well as decreased consumption of breakthrough ropivacaine and ketorolac postoperatively. However, there were no intergroup differences in terms of static/dynamic pain scores and incidence of side effects. In two recent trials, 477 patients undergoing TKR were randomized to a stimulating or blind femoral catheter.141 146 In the stimulating catheter group, the femoral nerve was initially localized with combined PNS–US; subsequently, the catheter was positioned with PNS only. In the blind catheter group, the femoral nerve was localized with PNS–US or US alone; subsequently, the catheter was advanced blindly past the needle tip. Both studies found no intergroup differences in terms of postoperative pain scores, physiotherapy performance, and opioid consumption. However, the stimulating catheters resulted in decreased cumulative ropivacaine consumption at 48 hours (181.3±74.1 vs 228.5±49.8 mL; p=0.03).146
In summary, compared to their blind counterparts, stimulating femoral catheters result in decreased in LA consumption. However, they seem to provide minimal clinical benefits in terms of analgesia, physiotherapy performance time, opioid consumption, and discharge time.
Blind versus US-guided femoral catheters
One RCT (n=92) compared blind and US-guided femoral catheters in the setting of TKR.147 For the US group, the femoral nerve was located with combined PNS–US; subsequently, the catheter tip was visualized sonographically to ensure proximity to the femoral nerve. Compared to their blind counterparts, US-guided femoral catheters resulted in decreased LA requirement at 48 hours, static/dynamic pain scores at 12, 24, and 48 hours, and supplemental oral morphine consumption.
Techniques for stimulating femoral catheters
In 120 patients undergoing TKR, PNS was compared to a combination of PNS and US for initial needle placement.148 Subsequently, in both groups, a stimulating catheter was advanced 3 to 5 cm beyond the needle tip with preservation of the quadriceps EMR. The US–PNS group was associated with a decrease in performance time (9.0 vs 13.5 min; p=0.024) and needle passes (p=0.007) as well as a higher rate of complete femoral sensory block at 30 min (63% vs 38%; p=0.01). Since all femoral catheters were placed with PNS, both groups displayed similar postoperative analgesia, knee flexion, and breakthrough opioid consumption.
Stimulating versus US-guided femoral catheters
To date, two trials (combined n=88) have compared PNS and US for placement of the femoral catheter itself.149 150 With PNS, the quadriceps EMR was obtained at a minimal stimulatory threshold of 0.5 mA (pulse width=0.1–0.2 ms). With US, a non-stimulating catheter was advanced under direct vision and its correct position (next to the nerve) inferred by the injection of 1 mL of air or normal saline. Both trials found no differences in postoperative pain scores. However, US resulted in a 24% to 41% decrease in performance time (p<0.03). Furthermore, one trial also reported a decreased incidence of vascular puncture (0% vs 20%; p=0.039) and less procedure-related pain with US.149
Techniques for US-guided femoral catheter
In a total of 97 patients undergoing TKR, two RCTs have compared US-guided femoral catheters inserted parallel (long-axis in-plane technique (LAX-IP)) or perpendicular (short-axis in-plane technique (SAX-IP)) to the long axis of the femoral nerve.151 152 In both groups, the desired position of the catheter tip (within 0.3 cm of the femoral nerve) was inferred by the injection of saline151 or air.152 Catheter placement required significantly less time (45% reduction) in the SAX-IP perpendicular group. There were no differences in the success rate of catheter placement, pain scores, opioid consumption, nausea/vomiting, maximal knee flexion, and length of stay. Thus, compared to a SAX-IP technique, catheter insertion and advancement using a LAX-IP technique confers no clinical benefits. In 16 healthy volunteers, Ilfeld et al 153 placed bilateral US-guided femoral catheters using a SAX-IP technique. Through randomization, the catheter tip was positioned either ventral or dorsal to the femoral nerve on one side. On the contralateral side, the catheter tip was placed in the alternate position. At different time intervals until 22 hours after the start of the LA infusion, the authors assessed sensory and motor blockade using tolerance to transcutaneous electrical stimulation and maximum voluntary isometric quadriceps contraction, respectively. No differences in motor block were found between the two groups. However, at 1, 6, 7, 8, and 9 hours, catheters placed ventral to the nerve provided a denser sensory block.
Summary of femoral perineural catheter techniques
For the placement of blind perineural catheters, the femoral nerve can be identified with PNS, US, or LOR (fascia iliaca compartment). Although LOR and US result in quicker needle placement, postoperative analgesia is comparable since the catheters are advanced blindly beyond the needle tip in all three cases. For the placement of stimulating perineural catheters, the femoral nerve can be identified with PNS alone or combined with US. The combination of modalities yields a shorter block performance time. However, postoperative analgesia is similar, as the catheters are inserted with PNS in both cases. In clinical practice (TKR or ACL repair), compared with their blind counterparts, stimulating femoral catheters seem to provide minimal clinical benefits. Similarly, US-guided and stimulating catheters result in comparable postoperative analgesia after TKR.
Nerve blocks of the sacral plexus
Although the sacral plexus gives rise to multiple branches, only the sciatic nerve is commonly anesthetized for lower extremity surgery. Sciatic nerve blocks can be used as an adjunct to femoral block for TKR154 and to provide anesthesia or analgesia for major ankle155 and foot156 157 surgery. Furthermore, the sciatic nerve, in conjunction with the superior gluteal nerve and the nerve to the quadratus femoris muscle, also provides innervation to the posterior aspect of the hip joint.13 48
Approaches for sacral plexus and proximal sciatic nerve block
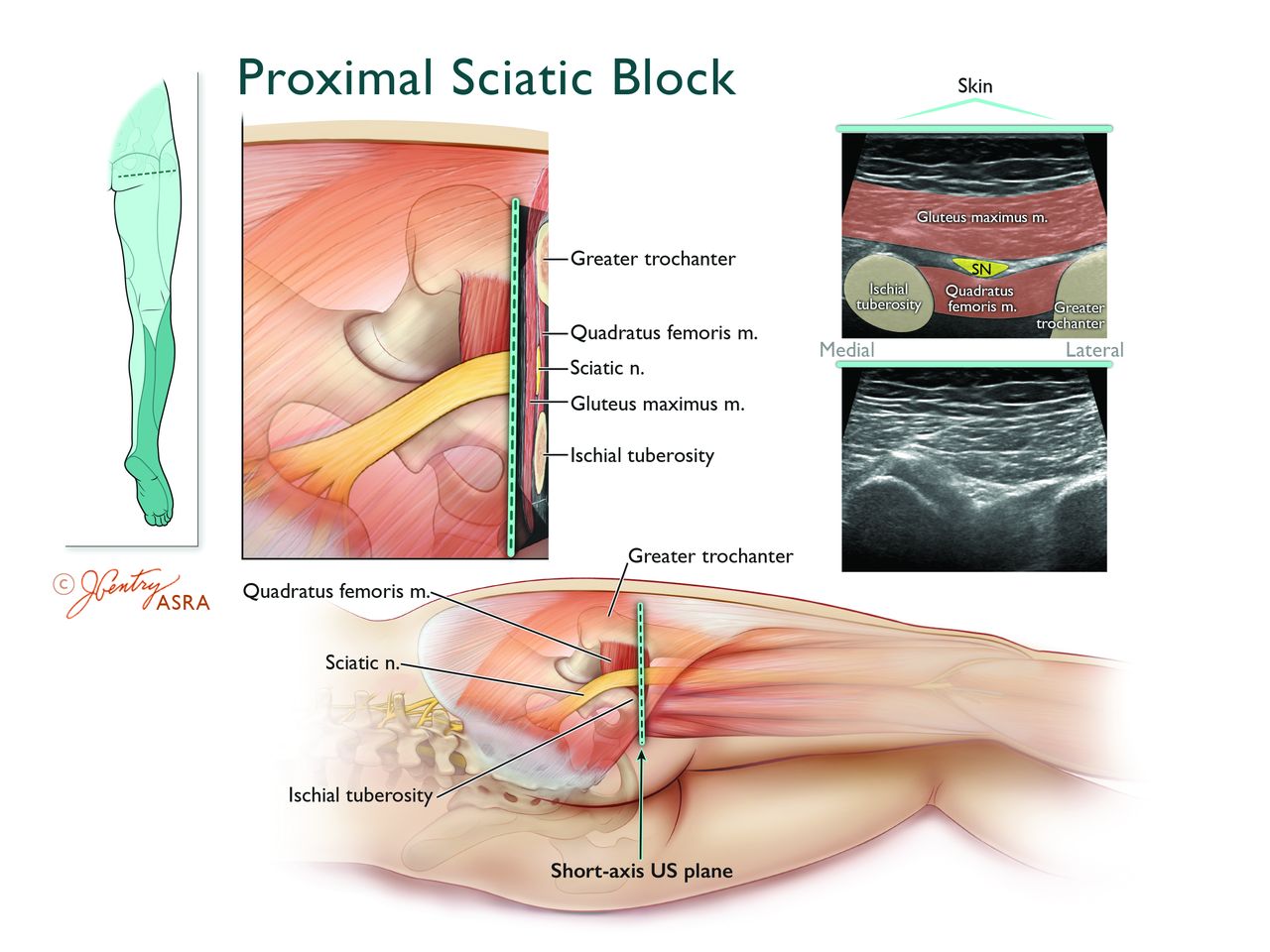
The proximal sciatic nerve can be anesthetized at the level of the sacral plexus (parasacral approach), proximal thigh (transgluteal, subgluteal, and anterior approaches) (figure 8), or mid-thigh (lateral approach). The parasacral approach targets the sacral plexus just caudal to the posterior inferior iliac spine, with a puncture site situated 6 cm inferior to the posterior superior iliac spine (PSIS) on an imaginary line joining the PSIS and the ischial tuberosity.158 In 150 patients, one trial compared parasacral and transgluteal sciatic nerve blocks: although the parasacral approach resulted in a quicker performance time (2.0 vs 5.5 min; p<0.001), total anesthesia-related times and success rates were similar between the two groups.159 Two RCTs (combined n=178) have compared the transgluteal and subgluteal approaches with similar conclusions: while no differences were noted in terms of success rate, onset and offset times, the subgluteal approach was associated with quicker sciatic nerve localization (32 vs 60 s; P<0.001) and less procedural pain.160 161
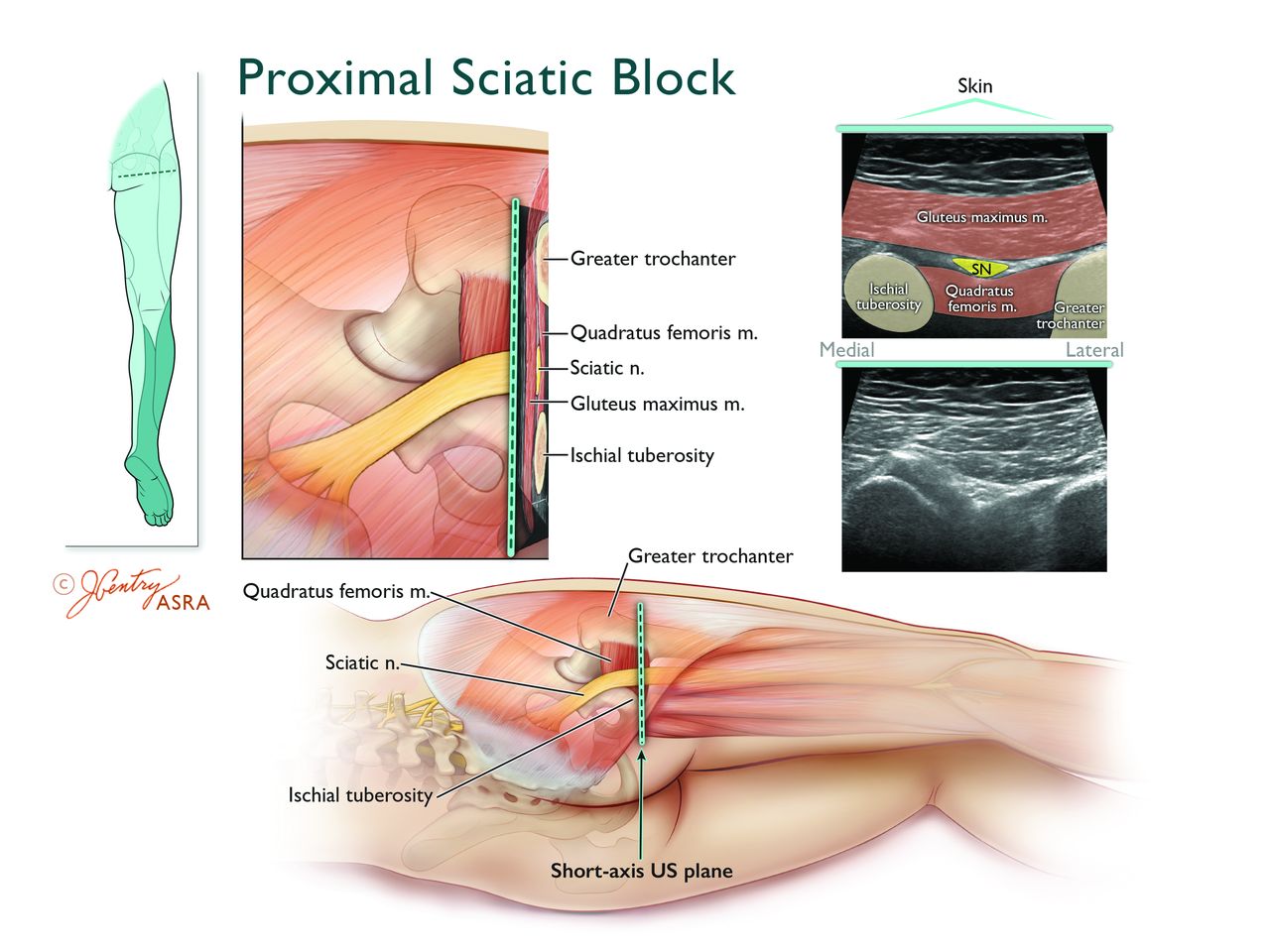
Anatomy of the ultrasound-guided proximal sciatic nerve (SN) block. Top left inset depicts the transducer location and expected cutaneous sensory distribution after proximal SN block. Note that this approach does not provide cutaneous sensory anesthesia to the posterior thigh. The magnified axial view illustrates that the SN is located between the lateral border of the ischial tuberosity (IT) and the medial border of the greater trochanter (GT) within the intermuscular (“subgluteal”) space dorsal to the quadratus femoris (QFM) and the ventral to the gluteus maximus muscle (GMM). The corresponding short-axis ultrasound image of the SN and subgluteal space is obtained the placing the transducer in an axial orientation between the IT and GT. The SN nerve appears as a hyperechoic oval to lip-shaped polyfascicular structure sandwiched ventral to the epimysium of the GMM and dorsal to the epimysium of the QFM. Illustration by Jennifer Gentry. Copyright Jennifer Gentry, American Society of Regional Anesthesia and Pain Medicine.
One RCT (n=59) compared the lateral mid-femoral and anterior approaches and reported similar performance times, success rates (77%–79%), onset times, and block durations.162 In contrast, another trial, which compared the lateral, anterior, and parasacral approaches, found that, despite similar onsets and durations, the anterior approach resulted in a denser block and improved patient satisfaction.163 Finally, one RCT (n=94) compared the anterior and subgluteal approaches using combined PNS and US.164 No differences were found in imaging, performance, onset/offset times, and success rate.
To date, only one trial has assessed proximal approaches in pediatric patients.165 In 180 children undergoing lower extremity surgery, the anterior, posterior transgluteal, and lateral mid-femoral provided similar overall success rates (82%–97%). However, the transgluteal approach was associated with a higher success rate on the first attempt compared to its lateral and anterior counterparts (88% vs 78% and 62%, respectively; both p<0.05).165
In summary, the current evidence suggests that all proximal approaches to the sciatic nerve result in similar success rates. In adults, the subgluteal approach should be preferred to the transgluteal method because of decreased performance time and procedural pain.
Technique for parasacral and proximal sciatic nerve block
Neurostimulation-guided sciatic nerve block can target an EMR of either the TN or CPN. To date, two RCTs have compared the success rates of sciatic nerve block based on elicitation of plantar flexion (TN) or dorsiflexion (CPN) EMR with fairly consistent results (table 1).166 167 For the parasacral and transgluteal approaches, compared to dorsiflexion, plantar flexion resulted in a higher success rate (78%–87.5% vs 16.7%–55.0%; p<0.05)166 167 as well as shorter onset times for complete sensory and motor block.167 These findings could be explained by the fact that the larger TN requires more LA to be deposited in its vicinity. Although preliminary works suggest that inversion and plantar flexion constitute the optimal EMRs for the subgluteal approach (table 1),168 169 these findings require further validation with RCTs.
Evoked motor responses of the sciatic nerve
In an effort to improve the success of proximal sciatic nerve blocks, some authors have proposed a double-injection technique, whereby the TN and CPN are independently localized and anesthetized.159 170 171 For the transgluteal approach, two trials (combined n=150) have compared single-injection to double-injection techniques with similar findings.159 170 A two-injection technique produced a higher success rate at 45 min (75%–100% vs 55%–80%; p<0.05). Furthermore, the longer performance time of the double-injection technique was offset by a decreased onset time.170 For the subgluteal approach, one trial (n=50) compared one-injection and two-injection techniques: despite similar success rates (92%–96%), performance times and block durations, the double-injection technique also provided a faster onset of complete sensory and motor blockade.171
Because of its depth, the proximal sciatic nerve can be difficult to localize. In recent years, new landmarks have attempted to simplify PNS-guided subgluteal, anterior, and lateral mid-femoral approaches. For the subgluteal approach, a new needle insertion site (3 cm medial and 4 cm caudal to the ischial tuberosity),172 based solely on the palpation of the ischial tuberosity (IT), was compared with the conventional one (4 cm caudal to the midpoint between the IT and greater trochanter). The new IT-based approach resulted in a higher rate of successful block placement (100% vs 42%; p<0.001), a shorter performance time, fewer needle passes, as well as a quicker onset of sensory and motor block.172 The results of this trial confirm the fact that, rather than being equidistant between the greater trochanter (GT) and the IT, the sciatic nerve is closer to the latter. For the anterior approach, one RCT (n=20) compared placing the patient’s leg in a neutral position or in external rotation.173 The success rates, distances from skin to nerve, and number of attempts were similar between the two groups. Finally, one trial (n=50) assessed proximal (20 cm distal to the GT) and distal (30 cm distal to the GT) puncture sites for the lateral mid-femoral approach.174 The proximal method resulted in a higher success rate (88% vs 56%; p<0.05) and a faster onset of complete sensorimotor block.
Two RCTs have compared US with PNS for proximal sciatic nerve blocks.175 176 In 2009, 60 patients receiving a subgluteal block were randomized to PNS (TN EMR) or US.175 Ultrasound guidance resulted in lower MEAV50 (12 vs 19 mL; p<0.001) and MEAV95 (14 vs 29 mL; p=0.008) for mepivacaine 1.5%. In the second RCT, PNS was compared to US–PNS for lateral mid-femoral sciatic blocks.176 The combination of modalities resulted in fewer attempts (1 vs 2; p=0.001) and a denser sensory block. However, performance and onset/offset times were similar between the two groups.
Two RCTs have investigated the best technique for US-guided proximal (subgluteal) sciatic blocks.177 178 In 86 patients, circumferential LA injection around the sciatic nerve was compared to a single injection dorsal to the nerve. Although the circumferential group required a longer performance time, it resulted in higher proportions of patients with complete sensory block at 30 min (41.9% vs 16.3%; p=0.018). In the second trial (n=27), in patients with body mass indices >25 kg/m2, Abdallah et al 178 compared US-guided subgluteal sciatic nerve blocks (with perineural LA injection) to US-guided LA injection in the subgluteal space (ie, the intermuscular fascial plane between the gluteus maximus and quadratus femoris muscles). Despite similar success rates, these authors found that the subgluteal space technique resulted in a shorter performance time (4.4 vs 9.0 min; p<0.001) as well as fewer needle passes and less procedural pain.
In summary, for PNS-guided proximal sciatic nerve block, electrostimulation of the TN should be preferred to that of the CPN. Furthermore, compared to its single-injection counterpart, a double-injection (EMR) technique offers significant advantages such as improved success rate and onset time. Compared to PNS, US provides a LA-sparing effect. For US-guided proximal sciatic blocks, circumferential LA injection around the nerve should be preferentially sought. Further trials are required to investigate the subgluteal space technique in patients with normal body mass indices.
Popliteal sciatic nerve block
The lateral and posterior popliteal approaches target the sciatic nerve in the distal thigh at the level of the popliteal fossa (figure 9).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Anatomy of the ultrasound-guided popliteal sciatic nerve (SN) block. Top left inset depicts the two transducer locations and expected cutaneous sensory distribution after popliteal SN block. The magnified axial view illustrates that the SN is located within the apex of the popliteal fossa (bordered laterally by the long and short heads of the biceps femoris muscles and medially by the semimembranosus–semitendinosus muscles) and dorsal (superficial) to the popliteal vein (PV) and artery (PA). The corresponding short-axis ultrasound image of the SN is obtained by placing the transducer in an axial orientation over the apex of popliteal fossa. The SN appears as a round hyperechoic polyfascicular structure dorsal to the PV–PA. The corresponding short axis ultrasound image of the bifurcation of the SN is obtained by moving the transducer distally until the medially located TN and laterally located CPN physically separate from each other. There will be a relatively hypoechoic space located between the hyperechoic TN and CPN that consists of extraneural connective tissue (subparaneural space) located deep to the paraneurium (figure 6), but just superficial to the epineurium of the TN and CPN. Illustration by Jennifer Gentry. Copyright Jennifer Gentry, American Society of Regional Anesthesia and Pain Medicine.
Proximal versus popliteal approaches
Two RCTs (combined n=158) have compared the transgluteal and posterior popliteal approaches for sciatic nerve block and found no differences in onset, offset, and performance times.179 180 While one trial reported a higher success rate with the transgluteal approach (95% vs 45%; p<0.01),179 the other found no difference between the two groups (94%–98%).180 Two RCTs (combined n=100) have compared the transgluteal and lateral popliteal approaches: both studies found a longer onset for sensory and motor block with the latter.161 181 One trial also reported a lower success rate with the lateral popliteal approach (68% vs 96%; p<0.05).181
One trial assessed the subgluteal and posterior popliteal approaches in terms of LA requirement for a complete sensory and motor block at 30 min with 30 mL of mepivacaine.182 The subgluteal approach was associated with a significantly lower minimum effective anesthetic concentration to achieve a successful block in 50% of patients (MEAC50=0.95%±0.014% vs 1.53±0.453%; p=0.026). Using similar methodology, another RCT compared the subgluteal and posterior popliteal approaches in terms of LA requirement for a complete sensory and motor block at 20 min with mepivacaine 1.5%.183 Again, the subgluteal approach was associated with significantly lower LA requirement (MEAV50=12±3 mL vs 20±3 mL; p<0.05). The combined results of these two studies suggest that the subgluteal approach requires approximately 40% less LA than its popliteal counterpart.182 183
One RCT (n=63) comparing the lateral mid-femoral and lateral popliteal approaches reported no differences in performance time, procedural discomfort and quality as well as duration of sensory and motor blockade.184 However, the lateral mid-femoral approach was associated with shorter onset times for sensory block of the TN and for motor block of the TN and CPN.
In summary, the available evidence suggests that, compared to their popliteal counterparts, proximal approaches to sciatic nerve block result in a decreased onset time and lower LA requirements.
Posterior versus lateral popliteal approaches
The lateral and posterior popliteal approaches are similar in terms of PNS EMRs, LA volume, and pharmacodynamics; the main difference resides in the fact that the lateral approach involves needle puncture in the lateral instead of the posterior aspect of the distal thigh. To date, only one RCT (n=50) has compared both popliteal approaches.185 Despite similar success rates (96%–100%), the posterior approach required fewer attempts to localize the sciatic nerve (p<0.001). Nonetheless, the lateral approach may still prove useful when patients cannot be placed in the prone (or lateral decubitus) position.
Techniques for posterior popliteal sciatic nerve block
To date, two RCTs have investigated the optimal landmarks and techniques for PNS-guided posterior popliteal blocks.186 187 One trial (n=109) compared a “modified intertendinous” technique (ie, needle insertion site in the intermuscular groove just distal to the overlap of the lateral and medial hamstring muscles) with a “classic” technique (ie, needle insertion site 1 cm lateral to the midline, 7–8 cm proximal to the popliteal crease).186 No intergroup differences were found in performance times, number of attempts, and success rates (71%–82%). Another RCT (n=60), comparing single-injection and double-injection techniques, reported similar success rates (77%–87%), sensory onset times as well as total anesthesia-related times.187 However, a decreased performance time (4.6±2.8 vs 5.9±3.1 min; p=0.03) and incidence of paresthesia (17% vs 40%; p=0.04) were noted with a single-injection technique. Although observational studies have suggested that foot inversion constitutes the optimal EMR for posterior popliteal sciatic blockade,62 this finding has not been rigorously validated with RCTs (table 1).
Multiple RCTs have compared PNS and US for posterior popliteal blocks.188–193 In 51 patients undergoing a double-injection technique, one study compared PNS to a combination of US and PNS.188 Despite similar performance time, number of needle passes, and procedural pain, patients randomized to PNS–US displayed a higher incidence of complete sensory block (85% vs 32%; p<0.001), complete motor block (65% vs 16%; p<0.001), and success rate (65% vs 16%; p<0.001) at 30 min. In three trials, PNS was compared to US alone.189–191 The first trial used a single-injection technique (accepting any EMR).189 Ultrasonography resulted in a higher success rate (89% vs 61%; p=0.005) as well as a quicker onset of sensory and motor blockade. In contrast, the second study (n=44), which compared US with a two-stimulation/injection technique, observed no differences in the rate of complete sensory and motor blockade, surgical anesthesia (82%–100%), onset time, and patient satisfaction.190 However, US guidance resulted in a shorter performance time (2 vs 5 min; p=0.002), less procedure-related pain (2 vs 4 on a 0–10 scale; p=0.002) as well as fewer needle passes (4 vs 6; p<0.001), paresthesias (0% vs 22%), and vascular punctures (0% vs 22%). In the most recent trial comparing PNS (TN EMR) to US (injection inside the paraneural sheath at the sciatic neural bifurcation), a higher percentage of successful sensory (80% vs 4%; p<0.001) and motor (60% vs 8%; p<0.001) block was observed at 15 min with US guidance.191 In children, one trial compared PNS and US for a combination of sciatic (subgluteal or popliteal approach) and femoral blocks.192 Ultrasound guidance resulted in longer postoperative analgesia (508±178 vs 335±169 min; p<0.001) with levobupivacaine 0.5%. Finally, one trial compared PNS and US for posterior popliteal block performed in Sim’s position.193 Despite comparable rates of surgical anesthesia (83%–100%), US guidance resulted in fewer needle passes and a reduction in the volume of lidocaine 1.5% with epinephrine 5 µg/mL (17 vs 37 mL; p<0.001). Thus, the available evidence suggests that, compared to PNS, US results in higher rates of complete sensory and motor block, quicker performance, shorter onset, and lower LA requirements.
Since anesthesiologists are increasingly relying on US to perform peripheral nerve blocks, recent RCTs have focused exclusively on US guidance for popliteal sciatic blocks. One trial compared LA deposition ventral to the popliteal sciatic nerve and circumferential injection around the latter.194 Despite similar performance times and procedural pain, success rate was expectedly higher with circumferential injection (94% vs 69%; p=0.01). Another study reported a quicker onset for sensory and motor block with separate injections around the TN and CPN compared with a pre-bifurcation injection around the common sciatic trunk.195
From its origin to its division TN and CPN, the sciatic nerve travels inside a common paraneural sheath.50 72 Due to the increased resolution of US machines, LA injection inside this paraneural sheath is now possible. In 2011, Tran et al 196 compared a single LA injection inside the common paraneural sheath at the sciatic nerve bifurcation (ie, the subparaneural technique) with targeted supraparaneural injections around the TN and CPN. These authors observed that the subparaneural technique resulted in a higher success rate (84% vs 56%; p=0.032) as well as improved efficiency (decreased performance/onset/total anesthesia-related times and fewer needle passes). Tran et al’s initial findings were reproduced by Perlas et al. 197 Using a similar research hypothesis, LA mix, injectate volume, and assessment scale for sensorimotor block, these authors found that, compared with separate injections around the TN and CPN, the subparaneural technique resulted in a higher incidence of complete block at 30 min (76% vs 49%; p=0.026) as well as a 30% reduction in onset time for sensory and motor block. A third trial (n=48) compared subparaneural to supraparaneural LA injection at the sciatic neural bifurcation.198 Again, the subparaneural technique yielded a higher success rate (100% vs 73%; p=0.006) and a 35% reduction in onset time. Tran et al 199 then set out to compare subparaneural LA injection at or proximal to the sciatic neural bifurcation: both techniques displayed similar success rates (85%–88%) and onset times. Subsequently, the same investigators compared single-subparaneural to triple-subparaneural injection techniques: again, no intergroup differences were found in terms of success rate (92%). Furthermore, the total anesthesia-related time (defined as the sum of performance and onset times) was also similar between the two groups.200 Consequently, these authors concluded that, as long as LA is deposited inside the paraneural sheath, the actual level and number of injections carry minimal clinical relevance.
In recent years, Cappelleri et al 201 have proposed a deliberate intraneural injection technique of the TN and CPN in the popliteal fossa. These authors demonstrated that, compared to subparaneural injection, intraneural LA injection resulted in a higher success rate (95% vs 63%; p<0.001) and a shorter onset time (10 vs 25 min; p<0.001). Furthermore, no intergroup differences were found in electrophysiological evaluation at 5 weeks. However, Cappelleri et al’s results should be interpreted with caution, as 40% of subjects assigned to the intraneural injection group were lost to follow-up and did not undergo electrophysiological assessment as planned.
In summary, the (robust) available evidence suggests that, for posterior popliteal sciatic nerve block, US should be preferred to PNS in light of demonstrated efficacy and efficiency (ie, decreased onset, performance time, procedure-related discomfort, and number of needle passes). With US guidance, the subparaneural technique constitutes a simple alternative, which results in a high success rate coupled with a short onset time. Further trials are required to investigate the safety of intentional intraneural injection of the TN and CPN.
Technique for lateral popliteal sciatic nerve block
Two RCTs have compared single-injection and double-injection PNS-guided lateral popliteal blocks with conflicting results.202 203 In one trial (n=50), a single-injection technique (using inversion as the preferred EMR) resulted in a lower success rate (54% vs 88%; p=0.007) than targeted localization/injection of the TN and CPN202 In contrast, the other trial observed identical success rates (94%) with single (TN EMR)-injection and double-injection techniques.203
One RCT (n=24) has compared PNS and US guidance for lateral popliteal sciatic nerve blocks in obese patients.204 Despite similar sensorimotor block profiles between the two groups, the authors found that US resulted in decreased performance time (206±40 vs 577±57 s; p<0.001), number of needle redirections, procedural pain and increased patient satisfaction scores.
Two RCTs have investigated the optimal technique for US guidance (SAX-IP technique).205 206 A combined total of 176 patients were randomized to separate injections of the TN or CPN or a single pre-bifurcation injection around the common sciatic trunk. In one trial, separate injections yielded a higher rate of surgical anesthesia (96% vs 51%; p<0.001)205 while similar success rates (97%–100%) occurred in the other one.206 However, both studies found a shorter onset time for complete sensory blockade in the separate-injection group. In recent years, there has been considerable interest in LA injection inside the paraneural compartment of the sciatic nerve. Missair et al 207 compared the subparaneural technique to an US-guided supraparaneural LA injection for lateral popliteal sciatic nerve blocks. These authors reported a higher rate of complete sensory block at 30 min (90% vs 63%; p=0.03) as well as a quicker onset and a 39%-longer block duration in the subparaneural group.
In summary, for lateral popliteal sciatic blocks, the current evidence suggests that, with either PNS or US guidance, separate injections around the TN and CPN provide a higher success rate or shorter onset time than a single LA injection around the common trunk. Expectedly, US provides superior efficiency to PNS in obese patients. As is the case with US-guided posterior popliteal sciatic blocks, the subparaneural technique results in an improved success rate and onset time compared toLA injection outside the paraneural sheath.
Sciatic perineural catheters
Continuous sciatic perineural infusion may be used to extend the duration of postoperative analgesia for procedures such as lower limb amputations, ankle arthroplasty as well as repair of tibial, fibular, and calcaneal fractures.
Blind subgluteal versus posterior popliteal catheters
In 60 patients undergoing elective foot surgery, one trial compared blind subgluteal and posterior popliteal catheters.208 For both approaches, either plantar or dorsiflexion were accepted as EMRs via the stimulating needle. Subsequently, the operator advanced the catheter blindly 3 to 4 cm beyond the needle tip. The authors found no differences in terms of intraoperative fentanyl supplementation, postoperative pain scores, patient satisfaction, ropivacaine use, and breakthrough morphine consumption.
Techniques for blind posterior popliteal catheters
Two recent RCTs have compared PNS and US for needle placement prior to blind catheter advancement (3–4 cm) of posterior popliteal catheters.209 210 In the first trial (n=98), in addition to fewer needle passes and improved patient satisfaction, US resulted in a higher rate of sensory block at 1, 6, 24, and 48 hours (94% vs 79%; p=0.03) and decreased morphine consumption during the first 48 hours (18 vs 34 mg; p=0.02).209 However, no differences were noted in terms of pain scores, LA consumption, and postoperative nausea. Nonetheless, using a cost-effectiveness analysis, the authors estimated that there was an 85% likelihood that US is cheaper and more effective than PNS.211 In the second trial (n=45), no differences were found in terms of static or dynamic pain scores, breakthrough opioid consumption, side effects, and length of stay. However, during the study period (approximately 48 hours), the US group consumed less ropivacaine (cumulative total=50 vs 197 mL; p<0.001).210 In an effort to define the optimal length for blind catheter insertion, Ilfeld et al 212 randomized 100 patients to a blind advancement of 0 to 1 or 5 to 6 cm beyond the needle tip. The authors found no intergroup differences in pain the day after surgery, breakthrough opioid consumption, catheter dislodgement/leakage, and incidence of insensate lower limb.212
Blind versus stimulating posterior popliteal catheters
Four RCTs have compared stimulating and blind posterior popliteal sciatic catheters in the setting of hallux valgus surgery.213–216 In 98 subjects, one trial observed that stimulating catheters were associated with a shorter onset of sensory and motor blockade as well as decreases in ropivacaine consumption and rescue (tramadol) analgesia (25% vs 58% of patients; p=0.002).213 However, this did not translate into a difference in static and dynamic pain scores, patient satisfaction or side effects. The following year, the authors repeated the same protocol in another 76 patients with similar findings.214 Again, during the study period (24 hours), stimulating catheters were associated with a decrease in ropivacaine (120 vs 153 mL; p=0.04) and tramadol consumption but not in pain scores or side effects. However, the authors were able to calculate that the reduction in ropivacaine resulted in a decrease in LA-related costs (21 vs 42 euros; p<0.001) if 100 mL bags of ropivacaine were used. The decreased cost was able to cover the additional expense of the stimulating catheter so that, in the end, there were no differences in analgesia-related expenditures between the two groups. When using 200 mL bags, the LA-sparing effect did not occur: thus, a 40% increase in analgesia-related costs was seen with stimulating catheters (€75 vs €55; p<0.001). Another study randomized 48 patients to blind posterior popliteal sciatic catheters using levobupivacaine 0.125% infusion, stimulating catheters using levobupivacaine 0.0625% infusion and stimulating catheters using levobupivacaine 0.125% infusion.215 The stimulating catheter/levobupivacaine 0.125% group consistently displayed lower pain scores at 6 to 8 hours (5 vs 60–70 on a 0–100 scale; p<0.05) and required less rescue analgesia at 24 hours (0% vs 31%–44% of patients; p<0.05). In 2009, a fourth RCT randomized 48 patients to either a blind or a stimulating posterior popliteal sciatic catheter.216 Despite similar onset times for sensory and motor block, stimulating catheters resulted in lower median volumes of 1.5% mepivacaine to achieve surgical anesthesia in 50% of subjects (2.6 vs 16.6 mL; p<0.05). In summary, the available evidence suggests that, compared to their blind counterparts, stimulating popliteal catheters provide similar pain control but result in decreased postoperative LA and opioid consumption. However, this sparing effect may not translate into a reduction in expenditures or adverse events.
Subgluteal versus posterior popliteal stimulating sciatic catheters
In 56 patients undergoing hallux valgus repair, one RCT compared stimulating sciatic perineural catheters placed using a subgluteal or a posterior popliteal approach.217 No differences in pain scores were observed during the study period (24 hours). However, subgluteal catheters were associated with fewer attempts for placement and decreased ropivacaine consumption (84±22 vs 106±30 mL; p<0.05).
Stimulating versus US-guided popliteal sciatic catheters
In two RCTs (combined n=120), Mariano et al 218 219 compared PNS and US guidance for posterior popliteal catheters in patients undergoing foot or ankle surgery. Both trials found a shorter performance time with US (5.0–7.0 vs 10.0–11.0 min; p<0.034). However, findings pertaining to procedural pain and vascular puncture were mixed: one study found improvement with US guidance218 while the other reported no differences between the two groups.219 Interestingly, the trial powered to detect a difference in postoperative analgesia (n=80) reported lower average pain scores at 24 hours with PNS (3.0 vs 5.0 on a 0–10 scale; p=0.032).219 Thus, the available evidence suggests that, compared to PNS, US guidance decreases the insertion time of posterior popliteal catheters. However, pain control may be superior at 24 hours with PNS.
Techniques for US-guided posterior popliteal catheters
In recent years, four RCTs have attempted to elucidate the optimal insertion technique for US-guided posterior popliteal catheters.220–223 In 128 patients undergoing foot or ankle surgery, one RCT compared suprapaneural and subparaneural positions of the catheter tip at the neural bifurcation of the sciatic nerve. Patients assigned to the subparaneural group reported lower average and worst pain scores the morning after surgery. However, no intergroup differences were found in terms of opioid consumption.220
Supraparaneural popliteal catheters can be performed by insonating the sciatic nerve in long or short axis. In 46 patients undergoing foot or ankle surgery, one RCT (n=46) compared both methods and found similar success rates (ie, complete sensory block at 30 min), onset times, numbers of needle passes, procedural pain, intraoperative/postoperative opioid consumption, and patient satisfaction. However, the long axis technique required a markedly longer performance time (9.5 vs 6.5 min; p<0.001).221
Subparaneural popliteal catheters can be inserted using an IP or OOP needling technique (prior to catheter advancement). Hauritz et al 222 found that, compared to its out-of-plane (OOP) counterpart, the IP technique was associated with a fourfold increase in catheter dislodgement and 150% greater opioid (morphine) requirements. A recent trial (n=82) compared positioning the catheter tip between the tibial and peroneal nerves or medial to the tibial nerve in the subparaneural space.223 Catheter tip placement medial to the tibial nerve resulted in lower incidences of foot drop (p=0.012) and insensate limb (p<0.001) without impacting overall analgesia and LA consumption.223
Summary of continuous sciatic perineural catheters
Continuous sciatic blocks can be performed with proximal (subgluteal) or distal (popliteal) approaches. The current evidence suggests that both methods provide comparable postoperative analgesia. However, LA consumption may be decreased with the subgluteal approach. For the placement of blind popliteal catheters, the sciatic nerve can be identified with PNS or US. Although the use of US requires fewer passes for needle placement, postoperative pain scores are comparable since the catheters are advanced blindly beyond the needle tip in both cases. For foot/ankle surgery, compared to their blind counterparts, stimulating popliteal catheters provide similar pain control but result in decreased postoperative LA and opioid consumption. Compared with PNS, US guidance requires a shorter performance time for the placement of posterior popliteal catheters. However, pain control may be superior at 24 hours with PNS. For US-guided popliteal catheters, an OOP needling technique should be used and the tip should be preferentially positioned inside the paraneurial compartment, medial to the tibial nerve.
Ankle block
Ankle block is commonly performed for midfoot and forefoot surgery.224 In 71 patients, one trial compared the conventional infiltrative method (using 30 mL of ropivacaine 0.5%) with an US-guided technique.225 Both methods provided similar success rates (80%-89%). However, during the first 24 hours, the proportion of patients requiring breakthrough opioids was lower with the conventional technique (20% vs 50%; p=0.01).225 An US-guided localization technique with concomitant PNS has been proposed for anesthesia of the deep peroneal nerve at the level of the distal malleolus.226 However, in 18 volunteers randomized to a landmark-based technique on one side and US on the other, no differences in sensory and motor block were noted between 20 and 60 min.227 In contrast, two other volunteer studies reported a higher success rate of tibial and sural blockade with US guidance.228 229 Thus, although US seems to provide minimal benefits for ankle blocks, it may improve the block success of individual nerves such as the tibial and sural nerves.
Gaps in technical knowledge
A critical survey of available RCTs can provide an effective tool to determine the most effective approaches and techniques for lower limb anesthesia. Despite current best evidence, many important technical issues regarding lower extremity nerve blocks remain unresolved and require further elucidation through well-designed and meticulously conducted RCTs. The authors’ opinion related to technical questions warranting further investigation is presented in table 2.
Important technical areas pertaining to lower extremity nerve blocks warranting further investigation with randomized controlled trials
Local anesthetics and adjuvants
Desirable LA properties for lower extremity nerve blocks may differ from those pertaining to brachial plexus blockade. For instance, upper limb surgery is often carried out under regional anesthesia. In contrast, surgical anesthesia for lower extremity surgery is most often accomplished using neuraxial or general anesthetic techniques, and lower extremity nerve blocks are used most often to extend postoperative analgesia rather than as the primary anesthetic. This carries implications for LA and adjuvant selection in that rapid block onset becomes less important while analgesic duration assumes a higher priority.
Local anesthetic selection
When single injection anesthesia is used, LA choice is dictated primarily by the desired block duration (box 1). 2-Chloroprocaine 3% is effective when rapid block onset and resolution are required for ambulatory surgery.230 Longer duration lower extremity analgesia follows the pattern bupivacaine>ropivacaine>mepivacaine.231 232 Thus, single-injection bupivacaine (0.25% to 0.5%) or ropivacaine (0.5%–0.75%) blocks are indicated for prolonged surgical anesthesia/analgesia, while intermediate-acting lidocaine and mepivacaine (1%–1.5%) are appropriate for 1-hour to 3-hour surgeries of mild-to-moderate discomfort, or to serve as the primary block when postoperative continuous infusion is planned. Liposomal bupivacaine, used off-label in a single volunteer crossover study of femoral nerve block, resulted in partial sensory and motor block for over 24 hours, but with high inter-subject variability of block magnitude. Moreover, an inverse relationship was seen between the dose of liposomal bupivacaine and the magnitude of the block.233
Evidence-based recommendations for local anesthetic and adjuvant selection for lower extremity peripheral nerve blocks
Local anesthetics
Local anesthetic selection
2-Chloroprocaine 3% is useful when rapid block onset and resolution are desired (2).
Lidocaine or mepivacaine 1% to 1.5% are indicated for surgical anesthesia of 1–3 hours’ duration or as primary block when a continuous postoperative technique is used (2).
For surgical anesthesia, equipotent bupivacaine 0.5% or ropivacaine 0.75% are indicated. For analgesia, bupivacaine 0.25% or ropivacaine 0.5% are adequate (2).
Liposomal bupivacaine is off-label and limited study is inadequate for recommendations at this time (4).
Local anesthetic mixing modestly reduces block onset time, but at the expense of block duration (2).
Local anesthetic dose, concentration, and volume
Dose, volume, and concentration of local anesthetics for lower extremity blockade tend toward higher-than-necessary parameters, especially when ultrasound guidance is used (2).
Patient weight–based dosing is fallacious and may be dangerous in children or adults with low muscle mass (3).
For continuous perineural techniques, drug mass appears to be more important than concentration or volume. Lower local anesthetic concentration may not result in less motor block (2).
Adjuvants
Epinephrine
Prolongs intermediate-acting local anesthetic agents (~50%) to a greater extent than long-acting agents (<20%).
Possesses the unique advantage of a marker of intravascular injection (2).
Clonidine
Prolongs intermediate-acting local anesthetic agents to a greater extent than long-acting agents (20% to 30%).
Does not improve continuous infusion techniques (2).
Buprenorphine
Mild to modest prolongation of blockade with increase in nausea and vomiting (2).
Dexamethasone
8 mg and higher perineural doses prolong analgesia modestly, but are not different than equivalent intravenous doses (1).
4 mg or less is recommended for perineural dosing (4, 5).
Dexmedetomidine
Most effective adjuvant for prolonging long-acting local anesthetic blocks (1).
Recommendations based on Oxford Centre for Evidence-Based Medicine 2011 Levels of Evidence (available at: http://www.cebm.net/index.aspx?o=565 (Level 1 = systematic review of randomized trials or n-of 1 trials; Level 2 = randomized trial or observational study with dramatic effect; Level 3 = non-randomized controlled cohort/follow-up study; Level 4 = case-series or case-control studies, or historically controlled studies; Level 5 = mechanism-based reasoning).
Local anesthetic mixing
The practice of mixing LAs to achieve faster block onset combined with prolonged duration has not been extensively investigated in the setting of lower extremity blockade. In a study of femoral–sciatic nerve block, mixing bupivacaine 0.5% or ropivacaine 0.7% with lidocaine 2% resulted in modestly faster block onset (7 to 12 min), but shorter block duration, as compared with using either long-acting LA alone. Furthermore, there were no inter-group differences in terms of pain scores and morphine use.234 A faster block onset coupled with a shorter duration could be considered inconsequential and detrimental, respectively, if the block is intended solely for analgesia.
Local anesthetic mass, concentration, and volume
The amount of LA used for nerve blocks is often greater than the dose required for adequate blockade. Intuitively, increasing LA concentration, volume, and/or mass should result in improved block characteristics (ie, quicker, denser, and longer-acting block). With rare exceptions, this has not proven true and may in fact increase the risk of local anesthetic systemic toxicity (LAST, from higher-than-necessary LA doses) or neurotoxicity (should the nerve’s protective perineurium be breached and the fascicles become exposed to higher LA concentrations). Dosing based on patient weight is fallacious because nerve size is independent of a patient’s morphometric parameters. Over-reliance on weight-based dosing can be particularly dangerous in children, whose smaller size places them at risk for LAST.235 For example, several children (36±10 kg) given 3.5 mg/kg of ropivacaine for fascia iliaca block attained high plasma concentrations that exceeded the recommended range.236 Experimentally, nerve cross-sectional area can predict LA dosing. For instance, complete sensory and motor blockade of the common sciatic nerve was achieved using only 0.15 mL/mm2 of ropivacaine 0.75%.237
Local anesthetic concentration
For surgical anesthesia, higher LA concentrations are often necessary; here, the comparative potency of LAs takes on importance. For large nerves, such as the proximal sciatic nerve, ropivacaine 0.75% is equipotent to bupivacaine 0.5% in terms of surgical anesthesia.238 While l-bupivacaine and ropivacaine share characteristics more similar to each other than to racemic bupivacaine, the former is more potent and consistently results in longer duration blocks than ropivacaine.239–241
Successful neural blockade is attainable despite low LA concentration. Using US guidance for femoral nerve blockade, ropivacaine in concentrations as low as 0.167% weight/volume (95% CI 0.14 to 0.184) resulted in surgical anesthesia.242 Lower concentrations are particularly adequate for analgesia: bupivacaine 0.25% or ropivacaine 0.2% resulted in 24-hour pain scores after ACL repair that were no different from those obtained using ropivacaine 0.75%.243 For US-guided transgluteal sciatic nerve blocks, mepivacaine 1% rendered block onset and duration equivalent to mepivacaine 2%.244 Conversely, when PNS was used to localize the sciatic nerve for the same approach, mepivacaine 1.5% resulted in faster block onset and higher success as compared with mepivacaine 1% in equal drug mass. This difference may be due to the block needle being farther away from the nerve using PNS compared with US.245
Local anesthetic volume
There exists little evidence to suggest that LA volumes in excess of 20 mL (administered via a perineural catheter) result in longer block duration.246 247 Nevertheless, LA volume does vary among block approaches. For instance, the MEV50 of mepivacaine 1.5% is nearly 50% less for a subgluteal sciatic nerve block than for its popliteal counterpart.183 The MEV50 for US-guided subparaneural popliteal sciatic nerve block was determined to be only 6.1 mL (95% CI 4.3 to 7.9) for ropivacaine 0.75%, but 40 min was required to achieve full sensorimotor blockade.248 Compared to PNS, US guidance decreases the MEV50 by~40% for subgluteal sciatic,175 ankle,225 and femoral106 nerve blocks.
Continuous perineural techniques
The role of volume, concentration, and dose is not well studied for lower extremity continuous perineural blocks. Using a continuous popliteal sciatic nerve block model, Ilfeld et al 249 reported that analgesia and patient satisfaction did not differ when ropivacaine was administered at 16 mg/h in either a 0.2% or 0.4% concentration. However, the more concentrated/lower basal rate infusion (0.4% at 4 mL/h) resulted in fewer insensate limbs (a desirable outcome). Conversely, neither concentration nor volume of ropivacaine affected continuous lumbar plexus block characteristics, which led the authors to conclude that LA mass constitutes the most important factor for lumbar plexus blocks. In this study, lower ropivacaine concentration (0.2%) did not impart the advantage of decreased motor blockade.250
Adjuvant selection
When continuous perineural techniques are not feasible, prolongation of analgesia beyond the expected duration of plain LA is accomplished through the use of adjuvant drugs (box 1). Classic adjuvants such as epinephrine and clonidine prolong intermediate-acting LA duration by approximately 50%, but have much less effect on long-acting LAs, in which only dexmedetomidine and perhaps dexamethasone exert an impactful effect. Pure opioid agonists and other adjuvants251 such as magnesium,252 tramadol, or midazolam253 have no significant effect on LA duration and/or display neurotoxicity concerns. The addition of sodium bicarbonate to bupivacaine for combined lumbar plexus and sciatic nerve block does not result in faster block onset.254 Alkalinization of intermediate-acting LAs has not been studied specifically for lower extremity block, but the evidence from upper extremity studies suggests that it does not result in a significantly faster onset of anesthesia.251
With the exception of epinephrine, all adjuvants discussed hereafter should be considered “off-label” with regard to their perineural use as per the US Food and Drug Administration.
Epinephrine
Epinephrine remains a useful addition to intermediate-acting LAs and possesses the unique characteristic of being an intravascular marker, which is important when potentially toxic doses of LA are used.255 Epinephrine’s attributes of intravascular marker and increased LA duration are similar whether 5 µg/mL (1:200 000 dilution) or 2.5 µg/mL (1:400 000) dilution is used, but the latter has less detrimental impact on tachycardia or peripheral nerve blood flow. The vasoconstrictive effects of epinephrine lead to reduced LA clearance and thus prolong block duration, but also cause concern over its use in patients with abnormal peripheral nerves. Thus, epinephrine is relatively contraindicated in patients at risk for peripheral nerve injury, such as those with diabetes mellitus, hypertension, or tobacco use.255 Even in healthy patients, concern for the integrity of peripheral nerve blood flow to the proximal sciatic nerve has led some experts to advocate avoiding epinephrine when using this approach, but there is no consistent evidence to support this advice.
Clonidine
The non-neurotoxic alpha-2 adrenoceptor agonist clonidine prolongs analgesic duration by inhibiting cation current across the cell membrane. Prolongation is more effective with intermediate-acting than with long-acting LAs253 where prolongation of anesthesia is only about 30% when added to ropivacaine 0.75% for femoral-sciatic nerve block256 or 20% when added to bupivacaine 0.375% with epinephrine for popliteal sciatic nerve block. In the latter study, clonidine did not affect overall pain scores and supplementary analgesic use.257 Bradycardia, hypotension, and drowsiness are linked to perineural clonidine doses greater than 100 µg. Based on data from upper extremity studies, clonidine is unlikely to add value to continuous infusion techniques and may (undesirably) enhance motor block.251
Buprenorphine
Discovery of opiate receptors on primary afferent neural fibers suggests a possible adjuvant role for opioids.258 The mu-agonist, kappa-antagonist buprenorphine is not neurotoxic when admixed with ropivacaine in cell cultures.253 Unfortunately, its benefit for lower extremity blockade remains unclear. Candido et al 258 found that perineural buprenorphine 0.3 mg added to bupivacaine 0.5% with epinephrine for infragluteal sciatic nerve block enhanced and prolonged analgesia to a minor degree as compared with intramuscular (IM) administration, but was linked to increased nausea and vomiting. When admixed with dexamethasone 4 mg and bupivacaine 0.25%, perineural administration of buprenorphine 150 µg resulted in 16 hours longer average sciatic nerve block duration, but no difference in pain on movement at 24 hours.259
Dexamethasone
Perineural and intravenous dexamethasone have been the subject of substantial investigation for prolonging neural blockade. Postulated mechanisms of action include inhibition of nociceptive C fibers, upregulation of potassium channels, and vasoconstriction.260 261 At doses of 8 mg and higher, the existing literature suggests that perineural dexamethasone is not different from intravenous or IM administration in terms of clinically meaningful block quality or duration when using infragluteal sciatic nerve block,260 popliteal sciatic nerve block, or ankle block.261 262 As noted previously, perineural dexamethasone 4 mg combined with buprenorphine 150 µg and 0.25% bupivacaine resulted in prolonged sciatic nerve block duration and lower worst pain scores after ankle surgery, but did not affect pain with movement at 24 hours. Moreover, the study’s multimodal analgesic approach using oxycodone/acetaminophen, meloxicam, pregabalin, and ondansetron resulted in low pain scores overall, making it difficult to assess the true contribution of dexamethasone. If dexamethasone is used, toxicity studies suggest limiting perineural dose to 1 to 2 mg.263 264 A recent Cochrane review concluded that current evidence is insufficient to determine the effectiveness of dexamethasone as an adjuvant for lower extremity regional anesthesia.265 As with epinephrine, the use of dexamethasone around diabetic peripheral nerves remains controversial.
Dexmedetomidine
Perineural dexmedetomidine is non-neurotoxic and appears to be an effective adjuvant for prolonging lower extremity sensory and motor blockade when using long-acting LAs. Similar to clonidine, dexmedetomidine’s purported mechanism of action stems from its alpha-2 adrenoceptor agonist properties. However, it displays an alpha-2/alpha-1 selectivity eight times that of clonidine.266 In a volunteer crossover study of US-guided posterior tibial nerve block, perineural dexmedetomidine 1 µg/kg admixed with ropivacaine 0.5% increased sensory block by an average 5.3 hours (about 25%).266 For femoral nerve block, increasing the dose to 2 µg/kg resulted in only one additional hour of analgesia.267
Complications of lower extremity nerve blocks
Complications common to all nerve blocks
The lack of RCTs investigating complications (and their treatments) related to lower extremity nerve blocks can be attributed to ethical reasons, as Institutional Review Boards are unlikely to approve proposals comparing active treatment versus placebo. Thus, in the following section, much of the discussion and recommendations are based on registries, quality assurance publications, prospective and retrospective observational studies, case series, animal trials, and practice advisories.
Local anesthetic systemic toxicity
Because the lower extremity receives innervation from the lumbar and sacral plexuses, regional anesthesia of the lower limb often requires two or more nerve blocks. The resultant cumulative dose of LA can predispose to LAST. To complicate matters further, the manifestations of LAST after lower extremity blocks may be delayed because of the increased circulation time and the concomitant use of sedation or general anesthesia. Furthermore, perineural LA infusion constitutes another source of delayed LAST and hepatic/renal failure can increase the inherent risk. Fortunately, in clinical practice, the incidence of seizures after lower limb regional anesthesia seems relatively low. For instance, Auroy et al reported only three seizures out of 20 162 lower extremity nerve blocks (incidence=0.98/1000).268 Similarly, in a prospective audit of 4522 lower limb blocks, Barrington et al 269 observed only two episodes of LAST (ie, overall incidence=0.44 per 1000 blocks). Two recent large retrospective (n=6678) and prospective (n=8101) studies detected only one episode of seizure each after lower limb regional anesthesia (incidence=0.12–0.215/1000).270 271 The incidence of cardiovascular arrest from LAST also constitutes a rare occurrence, as none occurred in published studies by Auroy et al, Barrington et al, Orebaugh et al, and Sites et al.268–271 When present, clinical manifestations of LAST should be managed according to the (recently updated) ASRA recommendations (box 2).235
Summary statements and recommendations on complications after lower extremity peripheral nerve blocks
Local anesthetic systemic toxicity (LAST)
Symptoms of LAST can be delayed from slow absorption of the local anesthetic (3). The clinician should be aware of total local anesthetic dose and the delayed symptoms with LE blocks (4).
The risk factors for LAST include extremes of age, low muscle mass, female gender, and patients with cardiac, liver, and metabolic comorbidities (3).
ASRA recommendations for preventing LAST include the use of ultrasound (3), use of lowest effective dose (4), incremental injections (5), aspiration before each injection (5), and addition of epinephrine when employing potentially toxic doses (4).
There is considerable variation in the presentation of LAST and the symptoms can be delayed up to 30–60 min (4).
Postoperative neurologic symptoms (PONS)
There are no clinical data to support the superiority of one nerve localization technique over another in terms of reducing PNI (3).
High injection pressures have been related to fascicular injury in animal studies, but no human data have shown the effectiveness of monitoring the injection pressure in reducing PNI (3). Subjectively assessing injection pressure is not reliable (2).
While US can detect intraneural injection, it does not have adequate resolution to distinguish between intrafascicular and interfascicular injection (5).
Infectious complications
Patients who are immunocompromised or have diabetes appear to be at greater risk (3).
The risk of infection is higher with continuous compared with single-injection PNBs (3).
There is higher incidence of colonization with LE block, especially blocks in the inguinal area (4). However, most colonizations do not result in clinical infection (3).
Chlorhexidine-based solutions appear to be more effective than povidone-iodine in decreasing potential infectious complications (2).
Hemorrhagic complications
The elderly, subjects with low body weight, females , and patients with liver or kidney problems have exaggerated response to the effect of anticoagulant drugs (3).
Blood loss can be a serious sequela of bleeding after LE peripheral nerve blocks (4).
Deep plexus blocks (lumbar plexus blocks) have been associated with post-block hematomas (4). Extra vigilance should be observed with these injections (5).
Role of ultrasound in complications
US decreases the incidence of LAST across its clinical continuum of symptoms, from minor symptoms to seizure and cardiac arrest (3).
There is no difference in the incidence of peripheral nerve injury between USG and other localization techniques (3).
Blocks while patient is awake versus sleep
Adults should not routinely receive regional anesthesia while they are anesthetized or deeply sedated (5).
Multi-institutional prospective studies documented the safety of neuraxial and regional anesthesia in children (3). For pediatric patients, nerve blocks can be done under general anesthesia (3).
Local anesthetic-induced myotoxicity
Clinically evident local anesthetic myotoxicity is rare, but cases have been reported after adductor canal block (4).
Muscle weakness is the usual symptom of local anesthetic myotoxicity (4).
Most patients recover although it may take several months for complete recovery (4).
Falls and lower extremity nerve blocks
Risk factors associated with falls in patients who had peripheral nerve blocks include patients’ age greater than 65 years, prolonged admission, primary total knee replacement surgery, obesity, use of femoral nerve catheter, male sex, and presence of comorbidities (fluid and electrolyte abnormalities, sleep apnea, psychosis, obesity, coagulopathy, and blood loss anemia) (3).
Most of the falls after orthopedic surgery are due to unassisted mobilization, occur during the night or evening shift, and elimination (bathroom)-related (3).
Patients who have a continuous LE peripheral nerve block have increased risk of falling compared with patients who did not have a nerve block (4).
The decrease in strength of the quadriceps muscles is less with adductor canal block compared with a femoral nerve block (2). The incidence of “near falls” is less with adductor canal block (3).
Periarticular local anesthetic injection, compared with femoral nerve block, results in a lower incidence of falls (3).
Measures to reduce inpatient falls include educational programs, fall prevention protocols, and use of walkers, crutches, or a wheelchair until the block has resolved (3). Knee immobilizers improve lower extremity stability (3).
Peripheral nerve catheter–related complications
The incidence of infections from a peripheral nerve catheter is rare (3).
Risk factors for catheter colonization include duration of catheter placement exceeding 24 hours, diabetes, and antibiotic administration the month before the surgery (3).
Peripheral nerve catheters are safe in children in terms in terms of infection, LAST, or PONS (3). The most common adverse events are malfunction and dislodgement (3).
The number of disconnection and reconnection should be limited (5). Unwitnessed disconnections should be removed (5).
Tourniquet-related complications
The application of a tourniquet during surgery reduces minor complications such as wound oozing, necrosis of wound margins, dehiscence, superficial infection, and leg swelling (3). However, it increases the risk of thrombotic events (3).
Tourniquet use should be limited to 2 hours as nerve recovery is delayed with prolonged inflation (3).
Venous emboli occurs in patients who have total knee arthroplasty, and the incidence is markedly increased after tourniquet deflation (3).
Compartment syndrome
Cases of compartment syndrome have been reported in patients who had LE nerve blocks; cardinal symptom is pain that is out of proportion to the injury and worsened by passive movement (stretching) of the affected muscles (4).
The signs and symptoms include pain, edema of the affected extremity, pallor, stiffness of the involved muscles, paresthesia, and diminished or absent peripheral pulse (4).
A high index of suspicion should be observed in patients with accelerating pain or increasing analgesic needs after surgery (5).
Damage to muscle and nerves occur within 4 to 8 hours of the initial symptoms of compartment syndrome (3). Surgery should be conducted within 4–12 hours after the onset of symptoms (3).
Based on the Oxford Levels of Evidence (Level 1 = systematic review of randomized trials or n-of 1 trials; Level 2 = randomized trial or observational study with dramatic effect; Level 3 = non-randomized controlled cohort/follow-up study; Level 4 = case-series or case-control studies, or historically controlled studies; Level 5 = mechanism-based reasoning).
ASRA, American Society of Regional Anesthesia; LAST, local anesthetic systemic toxicity; LE, lower extremity; PNB, peripheral nerve block; PNI, peripheral nerve injury; PONS, postoperative neurological symptoms; US, ultrasound.
By decreasing the risk of vascular puncture during nerve blocks, US has been shown to curb the incidence of LAST across its clinical continuum, from minor symptoms to seizure and cardiac arrest.235 270 272–276 In fact, the combined estimate of vascular puncture reveals a significant difference between US and PNS (Relative Risk = 0.16, 95% CI 0.05 to 0.47, p=0.001).277 Furthermore, propensity analysis also confirms that US can lower the risk of LAST by 65%.273 However, US cannot completely eradicate LAST276 278; thus, continued vigilance is paramount to ensure timely diagnosis and treatment.
Perioperative neurologic symptoms (PONs)
In regional anesthesia, one of the most feared complications is the unintentional intrafascicular injection of LA (box 2).279 280 In animal (rat) models, intrafascicular injections of bupivacaine, lidocaine, or ropivacaine into the sciatic nerve result in significant neuronal loss, with the most severe changes occurring closest to the injection point.281 In clinical practice, PONS occurs infrequently after lower extremity nerve blocks (table 3).268 281–284 Furthermore, deficits seldom persist and most symptoms resolve within a few months (table 3).268–270 , 282–287 In fact, The American Society of Anesthesiologists (ASA) Closed Claims Study Group reported that litigation involving lower limb nerve injuries occur less commonly than that involving the brachial plexus.285 In previous decades (1980s and 1990s), femoral and sciatic nerve injury accounted for 1% of the (non-obstetric) claims involving permanent neural deficit.285 However, contemporary data reveal that injuries to other nerves (eg, popliteal sciatic, peroneal, and nerves of the ankle) are starting to occur more frequently due to the increasing popularity of these blocks (table 3).
Nerve injuries after lower extremity nerve blocks
The use of adjunctive PNS may provide a specific albeit non-sensitive method to detect an intraneural position of the needle tip. For example, in 4 of 24 patients who underwent popliteal sciatic nerve blocks, no EMR was obtained with stimulating currents of 1.5 mA (pulse width=0.1 ms) even when the needle was found to be intraneural.288 However, intraneural injection occurred in all the patients with EMRs between 0.2 and 0.4 mA. Similarly, the presence of paresthesia constitutes an unreliable marker of neural penetration by the needle tip, as PONS have been reported despite the absence of sentinel paresthesia. Nonetheless, severe paresthesia on needle advancement or LA injection should alert to the possibility of intraneural needle position. Injection pressure has also been advocated as a possible monitor of intraneural placement.289 For instance, pressures<15 psi are usually recorded when the needle tip is located 1 mm away from the nerve.290 In contrast, pressures≥15 psi suggest possible intraneural injection.
Ultrasound guidance ensures proximity between the needle tip and the nerve while avoiding neural penetration. In turn, this could (theoretically) decrease the incidence of PONS.276 However, quality assurance and registry studies have found no difference in the prevalence of PONS between US and other localization techniques.270 276 291 Fortunately, the occurrence of long-term PONS (ie, symptoms exceeding 6–12 months) is rare (incidence=2 to 4 per 10 000 nerve blocks). However, this also signifies that 70 000 patients per group would be required to demonstrate an US-related decrease from 4 to 2 injuries per 10 000 nerve blocks (alpha=0.05, beta=0.8).276
At present time, because the optimal method to detect intraneural injection remains elusive, the second ASRA practice advisory on neurologic complications has recommended that adult patients not routinely receive regional anesthesia while under general anesthesia or deep sedation.292 Similarly, lower extremity nerve blocks should only be performed with extreme caution if the patient has a concomitant neuraxial block. In contrast, both the ASRA and the European Society of Regional Anesthesia and Pain Therapy support the performance of nerve blocks under general anesthesia in pediatric patients,293 as multi-institutional prospective studies have demonstrated the safety of peripheral nerve blocks in children who are asleep.294–297
In summary, until the advent of definitive proof, the benefits of injection pressure measurement, adjunctive PNS, US guidance, and avoiding the performance of nerve blocks under general anesthesia remain theoretical and driven by expert opinion. However, in light of the significant sequelae associated with inadvertent intrafascicular injection, the prudent anesthesiologist may elect to incorporate some (or all) of these strategies into his/her clinical practice.
Hemorrhage
Bleeding accompanied by retroperitoneal, psoas, and renal subscapsular hematoma has been reported after lumbar plexus blocks, attesting to the difficulty in diagnosing and halting hemorrhage occurring in deep and non-compressible areas.298–302 In the case report authored by Klein et al,299 the large psoas hematoma resulted in a 4-month lumbar plexopathy with weakness of the quadriceps, adductors, and hip flexor muscles.
The recent ASRA guidelines for regional anesthesia in patients receiving anticoagulation have attempted to stratify the hemorrhagic risk after peripheral nerve blocks. Superficial plexus/nerve blocks (eg, femoral block) are considered low risk, while their deep and non-compressible counterparts (eg, lumbar plexus and parasacral blocks) should be approached with extreme caution (if at all) in patients receiving anticoagulation. Intermediate-risk peripheral nerve blocks should be assessed on a case basis according to site compressibility, body habitus, comorbidities as well as the degree of anticoagulation.303 Studies on anticoagulants have demonstrated that patients who are elderly, female, afflicted with hepatorenal dysfunction, or have a low body weight can display an exaggerated response to the effect of these drugs.304 Moreover, in the literature, reports of bleeding have occurred with the combination of anticoagulants possessing different mechanisms of action (eg, enoxaparin and aspirin,299 warfarin and aspirin301) or drugs with the same antiplatelet action (eg, dipyridamole and aspirin).305 Thus, the performance of nerve blocks in patients receiving more than one anticoagulant is strongly discouraged.304
Infection
The prevalence of bacterial colonization associated with lower extremity perineural catheters is high (especially in the inguinal area) (29%–57%). Independent risk factors for catheter colonization include duration of catheter placement (>24 hours), diabetes, and antibiotic administration the month before surgery.306 Fortunately, the incidence of true infection requiring antibiotic or surgical therapy is much lower (0%–3%) and, expectedly, increases with the duration of catheter placement (table 4).286 306–312 In a prospective study of 20 174 perineural catheters,313 patients who developed an infection displayed a longer median (IQR) duration of catheter placement than those who did not (4.5 (3–7) vs 3 (1–3); p<0.001). Although infection following perineural catheter placement usually occurs at the insertion site, cases of bacteremic seeding resulting in psoas abscess (after a continuous femoral catheter),314 315 or thigh abscess (after a continuous popliteal sciatic catheter)312 have been reported.
Rate of infectious complications after lower extremity perineural catheters
Both the ASRA and the ASA have issued practice advisories to curtail the risk of infectious complications: their recommendations are virtually identical (ie, thorough hand washing, skin disinfection with chlorhexidine, use of surgical gloves as well as mask) (box 2).316 317 Additionally, disinfection of the US machine is recommended, as this practice has been shown to reduce bacterial colonization of the equipment.318 Although chlorhexidine-based solutions are most effective for skin disinfection,319 320 chlorhexidine-impregnated patches do not appear to decrease the risk of bacterial colonization for perineural catheters.311
Premature disconnection occasionally occurs with perineural catheters. Although no recommendation exists for witnessed catheter disconnection, the prudent anesthesiologist can employ the ASA practice advisory issued for neuraxial catheters317: in the event of witnessed disconnection, one should limit the time between disconnection and reconnection. However, in cases of unwitnessed disconnection, perineural catheters should be immediately removed.
Local anesthetic-related myotoxicity
All LAs are inherently myotoxic.321–323 However, clinically evident myotoxicity is rare and has been mostly confined to retrobulbar and peribulbar blocks until now.324–331 In recent years, sentinel cases have been reported after femoral triangle/adductor canal blocks.323 Signs and symptoms of LA-related myotoxicity include swelling, paresis, and pain that is typically aggravated by stretch and relieved by shortening of the muscle.321 However, in recent reports,323 swelling and pain were not always manifest, and flaccid quadriceps paralysis constituted the more consistent finding. MRI can reveal edema, localized swelling as well as inflammatory changes. Diminished action potentials, consistent with myopathy, appear on electromyography. Muscle biopsy confirms the diagnosis of muscle injury (ie, degenerating and regenerating muscle fibers, fiber splitting, and inflammatory infiltrates).322 Treatment remains conservative and includes non-steroidal anti-inflammatory drugs, non-opioid analgesics, and physical therapy. Although most patients recover, the process may take several months.
Complications specific to lower extremity nerve blocks
Patient fall
One of the most prevalent concerns after lower extremity nerve blocks is patient fall. In 2010, Ilfeld et al 332 pooled data from three published RCTs involving continuous femoral nerve blocks for hip and knee arthroplasty. These authors detected no fall in 86 patients who received perineural saline infusion compared with 7 falls in 85 subjects who were administered perineural ropivacaine (p=0.013). In 2013, Johnson et al 333 also concluded that continuous lumbar plexus blockade was associated with a fourfold greater risk of fall when compared with single-injection or no blockade. The association between lower extremity nerve blocks and inpatient falls was further investigated by Crumley-Aybar et al,334 who pooled data from 13 separate articles that met their inclusion criteria. These authors reported that a patient who had a peripheral nerve block incurred an eight times greater risk of fall and that the number (of blocks)-needed-to-harm was 50.334 However, the association between nerve blocks and falls has been recently challenged by Memtsoudis et al.335 Using a national Premier Perspective database of 191 570 patients, these authors found no link between peripheral nerve blocks and inpatient falls.335 Furthermore, from a mechanistic standpoint, it is possible that sensorimotor blockade does not constitute the primary etiology for falls, as Turbitt et al 336 have detected no difference in the rate of falls between patients with femoral catheters in situ, subjects who fell less than 12 hours after catheter removal, and those who incurred a fall more than 12 hours after catheter removal. Other important contributory factors could include medication side effects, delirium, reduced vigilance, decreased strength in the surgical limb, and non-adherence to the fall-prevention protocol. Nonetheless, as a preventive measure, Ilfeld et al 332 have recommended minimizing the LA dose and employing limited-volume patient-controlled bolus doses for perineural catheters. Other measures include the adoption of a specific protocol to prevent falls and the use of assistive devices (eg, walker, crutches, knee immobilizer, wheelchair) until the block recedes. Unfortunately, beneficial effects stemming from these programs remain ambiguous.337 338
Local anesthetic spread to adjacent structures
During the performance of lumbar plexus blocks, LA can diffuse to the epidural space thereby resulting in total spinal anesthesia and circulatory collapse.95 286 339 340 Femoral triangle blocks may result in quadriceps weakness due to retrograde LA spread to the muscular branches of the femoral nerve.341 342 Voiding difficulties requiring bladder catheterization (or urinary incontinence) can occur after parasacral blocks due to the proximity of the injection site and the autonomic nerves supplying the bladder.343 344
Needle trauma to adjacent structures
Cases of rectal perforation and hematoma have been described with parasacral blocks.345
Complications related to lower extremity surgery
Tourniquet-related complications
Although arterial tourniquets shorten surgical time, they do not prevent blood loss or blood transfusion but, in fact, can increase the risk of thromboembolic events.346–348 As a general rule, tourniquet time should be limited to 2 hours, as inflation periods exceeding 100 min are associated with an increased risk of infections, deep vein thrombosis, compartment syndrome, and nerve injury.349
Neural damage after tourniquet inflation ranges from paresthesia to paralysis350–352 and can be attributed to mechanical pressure as well as ischemia. Transient tourniquet release followed by re-inflation has been advocated to alleviate neural impairment. Unfortunately, this maneuver only modestly decreases the risk of neural injury.353 Strategies to prevent tourniquet-related complications include proper maintenance of the cuff and rubber tubing, positioning the tourniquet at the maximal circumference of the lower limb, confirmation of the manometer’s accuracy, ensuring that the padding placed underneath the tourniquet is free of folds, and alerting the surgeon at frequent and agreed-upon temporal intervals (box 2).351
Compartment syndrome
The etiology of compartment syndrome is multifactorial and includes tight dressings/casts, malposition of the lower limb during a long surgery, and trauma. The increased pressure within the compartment decreases vascular flow in arterioles, leading to neuromuscular infarction and necrosis. Damage to muscle and nerves usually occurs within 4 to 8 hours.354 Thus, early diagnosis and surgical decompression (within 4–12 hours) is paramount to prevent permanent deficits.354–356 The cardinal symptom of compartment syndrome is pain that is out of proportion with the injury and worsened by passive movement (stretching) of the affected muscle. Objective signs include edema, pallor, stiffness, diminished peripheral pulses, and muscle paresis.356–358 Unfortunately, these clinical findings can be unreliable; furthermore, pulselessness and paralysis usually occur late in the evolution of compartment syndrome.359
One of the greatest controversies in regional anesthesia revolves around the (safe) performance of peripheral nerve blocks in patients who are at risk for compartment syndrome. Because the latter has been reported in subjects who had received lower extremity nerve blocks,354 356 360–364 some experts have questioned whether lower limb regional anesthesia can delay the diagnosis by masking the pain of compartment syndrome. In contrast, others have argued that occurrence of “breakthrough pain” despite an effective sensorimotor block constitutes a reliable manifestation of compartment syndrome.356 363 Furthermore, pain in neural territories not anesthetized by the nerve block can offer another important diagnostic clue.354 Until the conundrum can be solved, communication between anesthesiologists and surgeons is paramount when/if carrying out regional anesthesia in patients at risk for compartment syndrome. Furthermore, if nerve blocks are performed, a dilute LA concentration should be selected in order to provide adequate analgesia while avoiding profound sensorimotor blockade354
Neural injury related to lower extremity surgery
Lower extremity surgery can lead to multiple neural injuries. For instance, total hip arthroplasty (THA) may result in injury to the common peroneal nerve (due its subcutaneous location) and to the femoral nerve (due to compression from an improperly placed retractor).365 Furthermore, the superior gluteal and lateral femoral cutaneous nerves can be damaged with the lateral and anterior surgical approaches, respectively. During hip arthroscopy, the perineal post may cause traction injury to the pudendal nerve. Total knee arthroplasty can result in impairment of the common peroneal nerve due to traction or compressive hematoma . Damage to the saphenous nerve may occur during arthroscopic meniscal repair and the infrapatellar branch can be harmed during ACL reconstruction.365 Because ankle arthroscopy is performed via anterior and posterior approaches, damage to cutaneous nerves may result from the placement of arthroscopic portals. The tibial nerve can be particularly vulnerable during posteromedial portal insertion.366 An anterior approach for total ankle replacement can lead to injury of the peroneal nerve. The superficial peroneal and sural nerves may be traumatized by the lateral cutaneous incision commonly used in ankle arthrodesis. Therefore, in light of the potential neural injury associated with surgery itself, nerve blocks should not be automatically assumed to be the cause of PONS. Instead, the prudent anesthesiologist should seek a neurologic consultation and conduct a thorough investigation to establish the topography of the deficit and the likely etiologic factors. The results of these investigations will inform the prognosis and optimal management strategy.
Controversial areas related to outcomes
Over the last 20 years, the advent of prophylactic anticoagulation, the increasing popularity of US for lower extremity nerve blocks,367 and the rehabilitative benefits associated with continuous femoral and femoral triangle blockade for TKR368–370 have ushered in a new standard of care. In contemporary practice, single-injection and continuous lower extremity nerve blocks are routinely employed to provide postoperative analgesia for TKR, ACL repair, THA, and hip fracture surgery. While an in-depth discussion of the evidence supporting the many different nerve blocks for these surgical procedures exceeds the scope of the current review article, a brief overview of controversial areas may be warranted (table 5).
Important issues pertaining to lower extremity surgery and peripheral nerve blocks warranting further investigation with randomized controlled trials
Total knee arthroplasty
The anterior, medial, and posterior aspects of the knee joint are primarily innervated by the femoral, obturator, and sciatic nerve, respectively (figure 4). Because continuous femoral blocks provide comparable analgesia and fewer side effects (eg, hypotension, urinary retention) than lumbar epidural analgesia, they have been routinely used in the setting of TKR since 1998.368 369 371 However, in the last 5 years, their hegemony has been challenged by so-called adductor canal blocks. The latter aim to spare the main femoral nerve therby preserving quadriceps motor function. Randomized trials comparing single-injection and continuous adductor canal to femoral blocks have all confirmed that the former result in improved postoperative quadriceps strength with minimal impact on the quality of pain control after TKR.370 372–374 However, whether the improved motor function of the quadriceps muscle results in better patient mobilization and a decreased risk of fall remains debatable.374–377 Future investigation is required to elucidate the matter. Furthermore, since the introduction of adductor canal blocks into clinical practice, some authors have employed single-injection blocks374 while others have advocated continuous blockade.370 373 376 377 Thus, randomized trials are required to compare single-injection and continuous adductor canal blocks for TKR. More importantly, the optimal injection site requires clinical elucidation: recent anatomical studies suggest that LA injection at the midpoint between the anterosuperior iliac spine and the patella, a technique favored by most authors, targets in fact the femoral triangle (which contains the saphenous nerve and the nerve to the vastus medialis muscle) and not the adductor canal per se (which contains the saphenous nerve).14 22 378 Therefore, future trials are required to determine if femoral triangle blocks may be superior to their adductor canal counterparts because of concomitant anesthesia of the saphenous nerve and the nerve to the vastus medialis muscle.
In addition to femoral (or femoral triangle) blockade, supplemental obturator nerve blocks have been advocated for TKR by some authors. Compared with femoral nerve blocks (with or without concomitant sciatic nerve blocks), the addition of obturator blocks has been demonstrated to improve pain control and decrease consumption of breakthrough opioids.119 379 Furthermore, the benefits stemming from obturator blockade also seems to extend to postoperative analgesic regimens using femoral triangle blocks. In 2016, Runge et al 380 compared femoral triangle blocks to combined femoral triangle-obturator blocks in patients undergoing TKR. These authors reported that the addition of obturator blockade resulted in decreased opioid consumption, pain scores and side effects (ie, nausea and vomiting). Although patients randomized to femoral triangle-obturator blocks (expectedly) displayed decreased motor strength, this did not impact ambulation. To date, RCTs have only investigated obturator blocks in the setting of single-injection femoral and femoral triangle blocks. Thus, future studies should determine if the benefits associated with obturator blocks would still persist in the setting of continuous femoral/femoral triangle blocks. Furthermore, continuous obturator blocks should also be investigated for TKR.
The issue of supplemental sciatic nerve block remains controversial. Although the combination of femoral and sciatic blocks seem to provide optimal analgesia for TKR,381–383 the impact of calf and foot motor paralysis on physiotherapy and ambulation remains a concern for many practitioners.154 Proposed alternatives to sciatic nerve block include LA infiltration of the posterior capsule of the knee joint, selective tibial nerve block,384 and sensory posterior articular nerve of the knee (ie, SPANK) block.385 Posterior capsular infiltration remains controversial, as Gi et al 386 found it to a be viable alternative to sciatic nerve block whereas Safa et al 387 and Pinsornak et al 388 concluded that it confers no additional analgesia when combined with femoral nerve block or standard LA infiltration of the knee, respectively. Although selective tibial nerve block spares the peroneal nerve (and prevents the occurrence of foot drop), its impact on ambulation and rehabilitation remains unknown. Further trials are required to investigate SPANK blocks.
ACL reconstruction
In contemporary practice, ACL repair is usually carried out with an arthroscopic surgical technique. Femoral nerve block remains the most common choice for postoperative analgesia. In the most recent meta-analysis (11 trials; 628 patients), Kirkham et al 389 concluded that, compared to intra-articular LA infiltration, femoral blockade results in superior analgesia in the immediate (0–2 hours), intermediate (3–12 hours), and late (13–24 hours) postoperative periods. Unfortunately, the meta-analysis could not draw definitive conclusions pertaining to functional outcomes (eg, quadriceps motor strength, range motion) and complications (eg, fall), as these parameters were not recorded by the original trials. Currently, the most controversial issue surrounding femoral blocks for ACL repair revolves around femoral nerve injury and quadriceps motor dysfunction. In 2017, Stebler et al 390 randomized 74 patients undergoing ACL reconstruction to 48 hours of continuous femoral nerve block or intravenous opioids. At 4 weeks, all patients underwent electrophysiological studies: no patient in either group met the electrophysiolocal criteria for femoral nerve injury. In contrast, in a recent systematic review article, Swank et al 391 pooled the findings of six studies that assessed quadriceps strength between 7 days and 6 months postoperatively. Swank et al 391 reported that, at 6 months, two out of four studies detected greater deficits in isokinetic testing in patients who had received femoral blocks for ACL reconstruction. In another study, the deficit persisted at 6 weeks but had subsided by 6 months. The clinical implication of these findings remains uncertain, as no differences were observed in terms of functional outcomes and patient return to sports at 6 months after ACL reconstruction.391
In recent years, El Ahl392 and Abdallah et al 393 set out to investigate the benefits of quadriceps-sparing femoral triangle/adductor canal blocks compared with femoral blocks for ACL reconstruction. Expectedly, in both studies, patients randomized to the former displayed superior quadriceps strength as assessed by straight leg raise during the first 24 hours392 or maximal voluntary isometric contraction at 45 min.393 However, the findings pertaining to pain control differed between the two trials. Whereas Abdallah et al 393 found that femoral triangle/adductor canal blocks resulted in non-inferior analgesia and opioid consumption compared to femoral blocks, El Ahl392 reported lower pain scores (at 18 and 24 hours) as well as decreased morphine consumption in patients receiving femoral blocks. This discrepancy could be attributed to the nature of the graft: patellar392 versus hamstring or bone–tendon–bone.393 Nonetheless, in light of these contradictory results, additional trials are needed to compare femoral triangle/adductor canal and femoral blocks for the different types (grafts) of ACL repair. Furthermore, future studies should investigate long-term (6 months) muscle strength in patients receiving femoral triangle/adductor canal blocks for ACL repair.
Total hip arthroplasty
The hip joint receives sensory innervation from both the lumbar and sacral plexuses (figure 4). However, the contribution of the former may be more important31 and as a result, most randomized trials have focused on lumbar plexus, femoral, and fascia iliaca blocks. The contemporary literature displays remarkably consistent results: compared with sham/no blocks, lower extremity nerve blocks result in significant benefits (eg, decreased postoperative pain and opioid consumption) for patients undergoing THA.394–399
Lumbar plexus, femoral, and fascia iliaca blocks have been compared with one another with mixed results. For instance, Biboulet et al 87 reported that during the first 4 hours after THA, pain scores and morphine consumption were lower with single-injection lumbar plexus blocks than single-injection femoral blocks. However, after 4 hours, no significant differences could be detected between the two groups. In contrast, Marino et al 400 observed that, compared to their continuous femoral counterparts, continuous lumbar plexus blocks consistently provided lower pain scores during the first two postoperative days. Furthermore, the use of continuous lumbar plexus blocks was associated with a decreased incidence of opioid-related side effects, greater distances walked, and improved patient satisfaction.400 Ilfeld et al 401 have also compared continuous lumbar plexus and femoral blocks in patients undergoing THA. Although they did find greater ambulation distances with lumbar plexus catheters, unlike Marino et al,400 they could not detect intergroup differences in terms of pain, breakthrough analgesic consumption, and patient satisfaction.401 In a recent meta-analysis (five trials; 308 patients), Wang et al 402 set out to compare fascia iliaca and femoral blocks for THA: these authors concluded that fascia iliaca and femoral blocks result in equivalent analgesia. However, their findings should be interpreted wit caution, as all pooled trials have employed the conventional infrainguinal technique for fascia iliaca blocks. In 2015, Kumar et al 403 demonstrated that, compared with its infrainguinal counterpart, a suprainguinal technique results in improved analgesia (at 6 hours) and decreased opioid consumption (at 24 hours) for patients undergoing THA. These authors speculated that the suprainguinal method promote cephalad diffusion of LA, resulting in a more reliable spread toward the lumbar plexus.403 Thus, additional trials are required to compare suprainguinal fascia iliaca and femoral blocks in patients undergoing THA. Moreover, future studies are also required to compare suprainguinal fascia iliaca and lumbar plexus blocks.
In addition to elucidating the optimal nerve block for THA, future investigation should also confirm the benefits of continuous over single-injection lower extremity nerve blocks. In 2008, Ilfeld et al 404 reported that, for lumbar plexus blocks, compared with an overnight LA (ropivacaine 0.2%) infusion, a 4-day infusion regimen attained three discharge criteria (ie, adequate analgesia, independence from intravenous analgesics, and ambulation distance ≥30 m) more swiftly. However, health-related quality of life, measured using the Western Ontario and McMaster Universities Osteoarthritis (WOMAC) index, was comparable between the two groups from 7 days to 1 year after surgery.405 Similar trials are required for femoral and fascia iliaca blocks. More importantly, future investigation should attempt to determine if regional anesthesia is truly necessary for THA. There exists some evidence to suggest that intrathecal morphine may provide similar (or superior) efficacy to fascia iliaca blocks406 and lumbar plexus blocks.407 Furthermore, in a recent network meta-analysis (35 trials, 2296 patients), Jiménez-Almonte et al 408 found no differences between LA infiltration and peripheral nerve blocks in terms of analgesia or opioid consumption 24 hours after THA. In fact, in a recent trial, Kuchálik et al 409 observed that, compared to femoral blocks, LA infiltration resulted in decreased pain during mobilization and lower morphine consumption at 24 hours.
Hip fracture surgery
Hip fracture commonly occurs in an at-risk (elderly) patient population that is often afflicted with multiple comorbidities (eg, osteoporosis). Peripheral nerve blocks have been traditionally employed to optimize postoperative analgesia and curtail the consumption of breakthrough opioids. In the most recent Cochrane Database systematic review (31 trials; 1760 patients), Guay et al 410 concluded that regional anesthesia decreases pain on movement within 30 min after block placement. Furthermore, moderate-quality evidence suggests that lower extremity nerve blocks also reduce the risk of pneumonia as well as the time to first mobilization.410 Possible nerve blocks for hip fracture include lumbar plexus, femoral, lateral femoral cutaneous, and fascia iliaca compartment blocks. Expectedly, LFCN blocks confer minimal benefits411 because they anesthetize the skin of the lateral thigh but not the fractured bone (figure 4). To date, most randomized trials have compared single-injection femoral and fascia iliaca blocks with mixed results.412 413 While Reavley et al 412 observed no significant differences between the two blocks, Newman et al 413 reported that patients receiving fascia iliaca blocks required significantly more morphine than those receiving femoral nerve blocks. This discrepancy could be attributed to the fact that the “blind” fascia iliaca technique, favored by both Reavley et al and Newman et al, can be notoriously unreliable, as fascias consist of several layers separated by adipose tissue; thus, blind puncture of any of these layers could have been mistaken for the second “pop.”113 Thus, future trials should endeavor to compare lumbar plexus, femoral, and fascia iliaca blocks using optimal techniques (eg, US guidance for fascia iliaca blocks). Furthermore, the benefits of continuous nerve blocks should be investigated for patients with hip fractures.
The research arena surrounding hip fracture surgery can be deceptively complex, as it encompasses multiple surgical interventions (eg, insertion of pins and screws or hemiarthroplasty). In a previous cohort study, Foss et al 414 have observed higher postoperative pain levels in subjects receiving dynamic or intramedullary hip screws than those undergoing hemiarthroplasty. Thus, future trials should carefully define their study population a priori; furthermore, researchers should be cognizant of the fact that their results may not be translated to a different type of hip fracture or another surgical intervention. Because nerve blocks can be performed in three different settings (ambulance, emergency department, and operating room), the situation becomes even more intricate from a technical and safety standpoint. For instance, while most emergency and operating rooms benefit from ready access to US machines, ambulances may not be outfitted with the latter; thus, despite its documented shortcomings, “blind” fascia iliaca blocks may constitute the only option.415 Moreover, lumbar plexus block carry an inherent risk of LA spread to the epidural space.95 Therefore, although they are routinely (and safely) performed in operating room settings, the prudent emergency physician may opt for more conservative options like femoral (or fascia iliaca) blocks.
Future research directions
Thirteen years have elapsed since the publication of the first review article on lower extremity regional anesthesia.1 During this time, lower limb nerve blocks have enjoyed renewed popularity due to the implementation of US guidance and its conferred ability to visualize the needle, nerve, and LA spread. In parallel to the clinical resurgence of lower extremity blocks, our collective understanding of lower limb anatomy has also progressed by leaps and bounds. For instance, although not novel per se, certain anatomical concepts (such as the subparaneural compartment) have crossed over into the clinical realm and led to the development of new techniques (eg, subparaneural sciatic blocks). However, much work is still required, as other anatomical concepts (eg, contents of the femoral triangle and adductor canal) remain hotly debated. Furthermore, the understanding of “new” anatomical notions, like the relative contributions of the sciatic and obturator nerves to the popliteal neural plexus, remains embryonic and requires further research in years to come.
Despite current best evidence, many important technical issues regarding lower extremity nerve blocks remain unresolved and mandate investigation with well-designed and adequately powered trials (table 2). Most importantly, despite Cappelleri et al’s promising initial results,201 the risk:benefit ratio of intentional tibial and peroneal intraneural injection necessitates further validation. Until the time when the safety and maximal LA volume/concentration for intraneural injection are elucidated beyond a reasonable doubt, the authors advise extreme caution when breaching (if at all) the epineurium of small peripheral nerves, as current US technology cannot distinguish between intraneural extrafascicular and intrafascicular positions of the needle tip.
Local anesthetic pharmacology benefits from a substantial amount of research cumulated throughout the years. Results acquired using traditional nerve localization modalities (eg, PNS) can and will apply to lower extremity nerve bocks performed with US. However, future research is still very much needed to investigate the optimal doses of novel adjuncts such as dexamethasone and dexmedetomedine. Moreover, investigators should remember to compare the clinical effects of these molecules to each other.
Since lower extremity regional anesthesia is (axiomatically) performed for lower extremity surgery, future trials must determine the optimal blocks for the different types of surgical intervention (eg, femoral vs femoral triangle blocks for ACL repair, optimal analgesic modality for posterior knee pain after TKR). Although postoperative pain should never be neglected, future studies should also investigate “big” outcomes. For example, femoral triangle/adductor canal blocks are currently widely used for knee surgery. Considering the fact these blocks are not devoid of complications (eg, local anesthesia–related myotoxicity), large prospective studies are required to determine if, beyond preservation of quadriceps strength, they can actually translate into concrete benefits such as a decreased incidence of patient fall or improved rehabilitation. Similarly, the contributive and mechanistic roles of femoral blockade in long-term quadriceps dysfunction after ACL repair require further investigation.
In conclusion, the last 13 years could be construed as the beginning of a “Golden Age” for lower extremity regional anesthesia. Multiple well-conducted studies have appeared in the literature, broadening our collective understanding of the anatomy, methods/techniques, pharmacology, and outcomes pertaining to lower extremity nerve blocks. More importantly, these trials have also highlighted areas in dire need of further investigation. The authors are convinced that, with the (future) third iteration of this review article, multiple questions raised in the preceding pages will have found answers and multiple new queries will see the light of day.
Acknowledgments
The first author would like to thank Dr Daniela Bravo (University of Chile) for her invaluable assistance with the literature search pertaining to the Outcomes section.
References
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
Footnotes
Competing interests None declared.